
Abstract
Introduction
Home blood pressure monitoring is often considered less reliable than conventional blood pressure monitoring due to different factors.
Aim
To investigate variations in home blood pressure monitoring and associated factors, differences in measured blood pressure under varying conditions such as postural changes from sitting to standing, among adults with hypertension.
Methods
A systematic review of studies was conducted on adults (≥18 years) with hypertension. Peer-reviewed studies published between 1992 and 2025 were searched in the Web of Science, PubMed, MEDLINE, and CINAHL databases in August 2023 and September 2025. The review included studies on home blood pressure monitoring, the associated factors, and reported in systolic and/or diastolic values. The main outcome was variations in home blood pressure monitoring categorized as small (<5 mmHg), moderate (5–15 mmHg), or large (>15 mmHg). Associated factors were also identified and the findings were analyzed using narrative synthesis.
Results
A total of 2,843 peer-reviewed articles were identified across four databases, of which 33 met the inclusion criteria. Generally, variations in home blood pressure monitoring ranged from −21.8 to +9.5 mmHg for systolic blood pressure and from −5.0 to +5.5 mmHg for diastolic blood pressure, where the + and − signs indicate the direction of changes. Fifteen factors associated with variations in home blood pressure monitoring were identified and broadly categorized into patient, device, procedural, protocol, and observer factors with related subcategories.
Conclusions
There were variations in home blood pressure monitoring and were associated with the factors, ranging from large decreases to large increases in both systolic and diastolic blood pressures, among adults with hypertension. Therefore, when measuring and interpreting blood pressure at home, it is essential to consider the factors associated with the variations. Furthermore, this study serves as a baseline for future research. This review is registered in PROSPERO.
Plain language summary
This review examined global evidence on variations in home blood pressure monitoring and factors associated with it among adults with hypertension. Identifying these variations and their associated factors is essential for obtaining more reliable readings and for improving hypertension management at home.
Introduction
Hypertension (HTN) is a significant risk factor for cardiovascular disease globally and requires urgent attention to prevent, diagnose, treat, and control it (Ferdinand et al., 2021). Home blood pressure monitoring (HBPM) refers to the self-measurement of blood pressure (BP) outside a clinical setting using BP devices, occasionally with the help of family members or others (health care providers, research assistants in cases of physical and cognitive limitations, or children) (Parati et al., 2021). Self-measured BP is more effective than office BP in predicting organ damage and cardiovascular outcomes including left ventricular hypertrophy (Shimbo et al., 2020).
Blood pressure is a dynamic physiological indicator that fluctuates with environmental, physical, emotional, and behavioral factors (e.g., stress, sleep, diet, alcohol, smoking, caffeine) (Parati et al., 2013; Shahoud et al., 2025), and understanding these variations can improve HTN management (Kawano, 2011). Several factors influence BP readings, including device accuracy, measurement techniques, patient preparation and positioning, monitoring schedules, device validation, and adherence to protocols. Errors in BP measurements can result in misdiagnosis or inappropriate management of HTN, thereby compromising the care of patients with HTN (Kallioinen et al., 2017). Even small deviations in BP (≥5 mmHg SBP) can misclassify HTN (Padwal et al., 2019), while larger deviations (≥20 mmHg SBP, ≥10 mmHg DBP) increase cardiovascular risk (Fuchs & Whelton, 2020), highlighting that reliance on single or recent readings is insufficient and may lead to misclassification, irregular reporting, and inadequate monitoring, thus requiring repeated assessments (Powers et al., 2011). In this review, HBPM variations refer to differences in home BP measurements across conditions or times, such as morning versus evening, before versus after eating, or sitting versus standing.
For accurate HBPM interpretation, healthcare professionals (e.g., nurses, doctors) and hypertensive patients must understand the factors influencing BP measurement accuracy (Kallioinen et al., 2017). Although HBPM can improve treatment adherence, healthcare providers are concerned about patients’ ability to measure correctly, device accuracy, and long-term commitment (Hiremath et al., 2024; Muntner et al., 2020). Home BP monitoring is an important aspect of HTN management, empowering patients to actively participate in their care and allowing for more accurate diagnosis and monitoring of BP at home (Ihm et al., 2022). Direct healthcare providers, especially nurses, play a vital role in supporting HBPM by educating patients on proper techniques, ensuring accurate readings, and integrating data into comprehensive care plans (Barkauskas et al., 2011; Himmelfarb et al., 2016).
This review hypothesizes that different factors contribute to HBPM variations in adults with HTN, and understanding them can improve measurement reliability, support self-management, enhance detection of white-coat HTN, reduce cardiovascular risks, and lower healthcare burdens by decreasing clinic visits. It offers valuable insights for direct healthcare providers, patients, and families on the sources and implications on variations in HBPM and the factors associated.
Methods
Design
A systematic literature review was conducted to evaluate the variations in HBPM and potentially associated factors in adults with HTN. The findings were reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher et al., 2009) (Figure 1). The review protocol was registered in PROSPERO.

Systematic Reviews and Meta-Analyses (PRISMA) flowchart showing study selection from the databases. HBPM: home blood pressure monitoring; ABPM: ambulatory blood pressure monitoring.
Exploratory Searches
Peer-reviewed articles were searched using Web of Science, PubMed, MEDLINE, and CINAHL databases. The search was limited to English-language articles published between January 1, 1992, and September 1, 2025. Furthermore, considering the last reviewed, we added September 1, 2024, to September 1, 2025, related studies from the same databases. The protocol for validating automated BP monitoring was established in July 1987 (Association for the Advancement of Medical Instrumentation, 1987; Stergiou et al., 2018a). For this review, peer-reviewed articles focusing on searches were conducted from 1992 to allow protocol adaptation and study initiation. Key search terms, including HBPM, measurement, self-measurement of BP, practice, accuracy, adults, and HTN, were developed in collaboration with an expert librarian and reviewers (Supplementary Table 2).
Selection Criteria
The inclusion criteria were studies, such as (a) on HBPM conducted in adults with HTN, (b) where BP was measured at home by adult hypertensive patients, their relatives, or researchers, (c) identified one or more factors associated with HBPM, (d) quantified the systolic and/or diastolic BP, and (e) only studies published in English were considered.
The exclusion criteria included: (a) studies conducted outside the home, such as in clinics, hospitals, pharmacies, or other institutions, (b) excluded if BP was measured only by health professionals without comparison to hypertensive patients in the context of HBPM, (c) if HBPM was conducted in nonhypertensive adults, (d) studies involving hypertensive patients under 18 years of age, (e) systematic reviews, meta-analyses, qualitative studies, or (f) those with low-quality appraisal assessment scores were excluded.
Search Outcome
Web of Science, PubMed, Medline, and CINAHL database searches revealed 2,843 studies. After removing duplicates and screening for eligibility, 33 identified studies were included in the review (Figure 1). Data from the eligible studies were independently extracted by two reviewers, and any discrepancies were resolved by a third reviewer. Study selection was performed using Rayyan software, where articles were classified as excluded or potentially included. The abstracts and full texts of the potentially included studies were then discussed in detail, and disagreements were resolved by a third reviewer. The final set of included studies was exported to Excel for synthesis and analysis in line with the review objectives.
Quality Appraisal Assessment
Quality assessment of the included studies was performed using a standardized scoring system. For Quality appraisal assessment, the Quality Assessment Criteria for Evaluating Primary Research Papers for of Variety Fields (Kmet et al., 2004) were utilized in this review. Each study was evaluated across multiple criteria, including objectives, study design, participant selection, measurement methods, sample size, statistical analysis, control for confounding factors, and whether the results supported the conclusions. The quality of the studies was summarized by assigning scores to each indicator, which guided the interpretation of the findings, although the scores were not directly comparable (Supplementary Table 1). Items were scored as “Yes” (2 points), “Partial” (1 point), or “No” (0 points), with “Not Applicable” excluded. Fourteen items were assessed in quantitative studies, giving a maximum score of 20. The summary score was calculated by dividing the total by the maximum possible score, and studies score of 55% was used as cut line (Kmet et al., 2004).
Data Extraction
The checklist was developed based on inclusion and exclusion criteria and broadly categorized as patients, procedures, devices, protocols, and observers’ related factors. The extracted data included the first author, publication year, country, study setting, design, measured outcome, purpose of study, sample size, and study quality (Supplementary Table 1 and 3). Data extraction was independently performed by two reviewers and a third author to resolve any discrepancies.
Data Synthesis
This review analyzed variations in HBPM and the associated factors. The results of the studies are summarized in tables, and similarities and differences within and between the studies were narrative synthesized. Meta-analysis was deemed a method for analyzing pooled data from each study due to inconsistencies in the design used, differences in the questions asked, and variations in the target populations across studies. If a consensus could not be reached between the two reviewers, a third reviewer was consulted to make the final decision. This approach ensured consistency and minimized bias in the selection of studies. For ease of interpretation, we adopted conventional methods, and variations were categorized into three levels: small (<5 mmHg), moderate (5–15 mmHg), and large (>15 mmHg) (Kallioinen et al., 2017). Furthermore, the (−) and (+) signs indicate decreases and increases in SBP and DBP, respectively. Moreover, factors associated with variations in HBPM were extracted. The selected studies were exported to Endnote and Microsoft Excel for narrative syntheses.
Analysis of Subgroups
Pregnant women, patients with arrhythmia (atrial fibrillation), patients with large arm circumferences (>42 cm), and older adults (≥65 years) were analyzed separately for the subgroup analysis.
Results
Description of Studies
Collectively, 15 potential factors associated with HBPM variations were identified in the 33 included studies (Supplementary Table 1). These factors associated with HBPM variation were categorized into five major categories, similar to a previous study, including patient-related, device-related, procedure-related, protocol-related, and observer-related factors (Kallioinen et al., 2017). Patient-related factors were categorized into six subcategories that include educational level, variation in temperature, causal effect, seasonal variation, fruit intake, and tobacco intake. Procedure-related factors affecting HBPM consist hand positioning, sleep pattern, measurement time, and cuff inflation. Furthermore, BP device-related factors, protocol-related factors, and observer-related factors were included (Supplementary Table 1).
Variations in HBPM
This systematic review included 33 studies that focused on variations and factors associated with them focusing on HBPM in adults with HTN. The variations ranged from −21.8 to 9.5 mmHg for SBP and −5.0 to 5.5 mmHg for DBP, where positive values indicate increases and negative values indicate decreases (Supplementary Table 1 and Table 1).
Summary of Variation Ranges and Categories of Potentially Associated Factors.
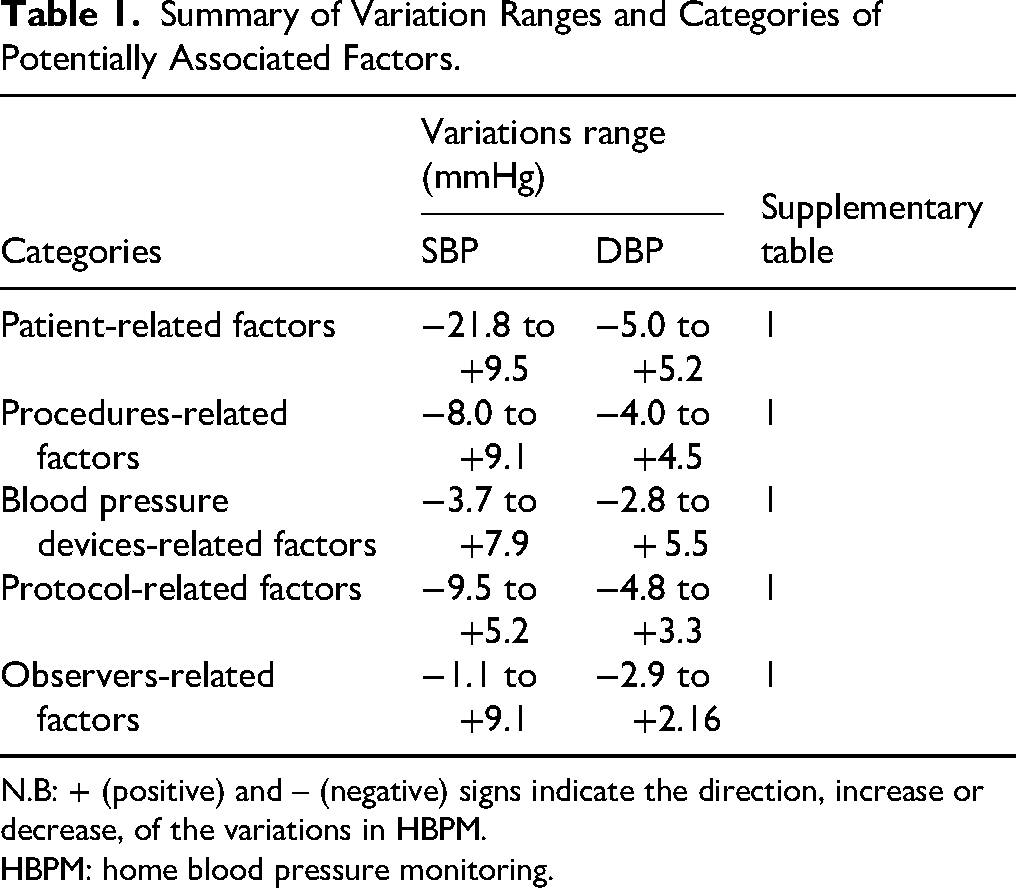
N.B: + (positive) and – (negative) signs indicate the direction, increase or decrease, of the variations in HBPM.
HBPM: home blood pressure monitoring.
Patient-Related Factors
This review identified 11 studies that investigated patient-related factors affecting HBPM variations (Avegno et al., 2023; Barroso et al., 2019; Groenland et al., 2022; Iwahori et al., 2018; Margolius et al., 2012; Seki et al., 2010; Sirin et al., 2024; Strom et al., 2022; Stryker et al., 2004; Umishio et al., 2019; Umishio et al., 2021). Patient-related factors associated with variations in HBPM were further classified into effects of educational interventions, causal effects, Exposure to Temperature, exposure to seasonal variations, frequency of fruit intake, and exposure to tobacco smoke (Supplementary Table 1). Home BP monitoring differences before and after simple educational intervention were compared, with variations ranging from small increase to small decrease (SBP: +1.3 mmHg and DBP: −1.3 mmHg) (Stryker et al., 2004). Weekly telephone counseling also reduces home SBP and DBP to −13 mmHg and −5 mmHg, respectively (Avegno et al., 2023). SBP after coaching compared to combined with home titration of antihypertensive medications showed a large decrease in variation at home (SBP: −21.8 mmHg) (Margolius et al., 2012). Moreover, training on adherence to instruction on guidelines decreased HBPM (SBP: −1.8 mmHg and DBP: −3.1 mmHg) (Sirin et al., 2024) (Supplementary Table 1).
Furthermore, exposure to indoor temperature throughout the day varied from small to moderate increases in SBP, +3.9 to +9.5 mmHg (Umishio et al., 2019; Umishio et al., 2021) (Supplementary Table 1). The morning SBP is more sensitive to indoor temperature changes, increasing by 8.2 mmHg for every 10°C decrease (Umishio et al., 2019). Evening SBP was also increased (8.6 mmHg) in older adults (Umishio et al., 2021). In contrast, two studies found HBPM diurnal differences in SBP, ranged from small decrease to small increases (SBP: −2.0 to 2.2 mmHg) (Groenland et al., 2022; Iwahori et al., 2018). Morning SBP was significantly lower than the evening SBP (−2 mmHg) (Groenland et al., 2022). Morning–evening summer–winter differences showed small increases in SBP (0.7–0.8 mmHg), and SBP was lower from February to July than from August to December (−1.5 mmHg) (Iwahori et al., 2018) (Supplementary Table 1).
Frequent fruit consumption compared to least eating intake such as bananas, apples/pears, and oranges/citrus fruits, at home showed small decrease in SBP ranged from −3.9 to −2.7 mmHg (Strom et al., 2022). Additionally, without antihypertensive treatment, home tobacco smoke was 4 mmHg higher than nonexposure. With antihypertensive treatment, home and work/other tobacco smoke exposure was 3 mmHg higher than in the nonexposure group. This was a small increase in SBP associated with tobacco smoke exposure (3–4 mmHg) (Seki et al., 2010). Casual BP (white-coat and masked HTN) compared to home BP (HBP) showed differences of 7.6 mmHg in SBP and 5.2 mmHg in DBP, respectively (Barroso et al., 2019) (Supplementary Table 1).
Procedure-Related Factors
Sixteen studies reported variations in HBPM among different procedure-related factors (Campbell et al., 2001; Costa Borges et al., 2025; Dourmap et al., 2010; Gazzola et al., 2018; Hofstede et al., 2022; Johansson et al., 2010; Kawabe & Saito, 2008; Kjeldsen et al., 2002; Kyriakoulis et al., 2022; Liu et al., 2024; Morris et al., 2025; Mullen et al., 2023; Okada et al., 2019; Stergiou et al., 2008; Stergiou et al., 2010; Stryker et al., 2004) (Supplementary Table 1). This included hand position, sleep pattern, point of time of measurement, after 5-min rest, cuff inflation related, and place of BP measurement. The variations in SBP and DBP between one arm and the opposite arm were 5.3 mmHg SBP and 3.4 mmHg DBP (Stryker et al., 2004). Arm-HBP was higher compared to Wrist HBP (SBP: 5.2 mmHg and DBP: 2.2 mmHg) (Stergiou et al., 2008). Wrist BP was 8/1 mmHg lower (SBP/DBP) with the hand on the opposite shoulder, and 2 mmHg lower SBP but 1 mmHg higher DBP with the hand on the opposite elbow, compared to arm BP (Dourmap et al., 2010). Poor sleep moderately increased SBP (7.1 mmHg) and decreased DBP (3 mmHg) compared to good sleep (Okada et al., 2019). Morning short sleep increased SBP by 0.8 mmHg with no change in DBP compared to proper sleep (Kawabe & Saito, 2008). Before sleep, SBP was only 0.2 mmHg higher than after sleep, with DBP not applicable (Kario, 2021) (Supplementary Table 1). The time of day had only a minimal effect, with SBP and DBP being slightly higher during the daytime compared to evening or night measurements (≤0.5 mmHg) (Costa Borges et al., 2025). The first and second readings showed a consistent pattern, with the first measurement yielding higher values (2–3 mmHg for SBP and 1–2 mmHg for DBP) (Hofstede et al., 2022; Stergiou et al., 2010). Across days, day 1 HBP were generally higher than on subsequent days, with small increase to +3.5 mmHg for SBP, although in SBP and DBP were lower by day 7 (−3.2 and −1.5 mmHg, respectively) (Kyriakoulis et al., 2022; Morris et al., 2025). Furthermore, the last 7 days (7 days backward) had small decrease in SBP and DBP values (−2.8 and −1.7 mmHg, respectively) compared to the first 7 days (day 1–7) (Johansson et al., 2010; Morris et al., 2025; Mullen et al., 2023).
When comparing patient and trained nurse HBP taken before the 5-min rest, patient readings were 9.1 mmHg higher for SBP and 1.5 mmHg higher for DBP. After the 5-min rest, the difference decreased, with patient readings being 3.8 mmHg higher for SBP and 1.1 mmHg higher for DBP compared to the nurse's measurements (Campbell et al., 2001) (Supplementary Table 1).
This systematic review also found that, the first cuff inflation produced higher readings than the second after a 10-min rest, with increases of +6.9 mmHg SBP and +4.5 mmHg DBP using the 10/5 mmHg adjustment, and +4.4 mmHg SBP and +2.7 mmHg DBP without the adjustment (Gazzola et al., 2018). Using a wide-range cuff compared to a normal cuff demonstrated small decrease in both SBP (−0.8 mmHg) and DBP (−2.2 mmHg), while an extra-large cuff compared to a normal cuff also has small decrease for both (SBP −0.4 mmHg and DBP −2.9 mmHg) (Liu et al., 2024). On the other hand, HBPM was lower than office BP, with small variations of −4 mmHg in SBP and −3.1 mmHg in DBP (Kjeldsen et al., 2002). In contrast, hospital self-measured BP compared to self-measured HBP demonstrated a small difference, with SBP being 0.7 mmHg decrease and DBP 0.9 mmHg increase in the hospital setting (Hofstede et al., 2022) (Supplementary Table 1).
Blood Pressure Devices-Related Factors
Six studies evaluated the effects of different BP devices on HBPM (Akpolat et al., 2018; Hofstede et al., 2022; Jung et al., 2015; Ringrose et al., 2017; Schaefer et al., 2021; Tremonti et al., 2017) (Supplementary Table1). Home BP devices, compared to the auscultation standard, showed a small decrease in SBP (−3.3 mmHg) but a small increase in DBP (+0.9 mmHg) (Ringrose et al., 2017). The Omron BP654 wrist cuff recorded higher values than the aneroid sphygmomanometer (+4.8 mmHg SBP, +3.6 mmHg DBP), whereas the Omron BP786 arm cuff showed lower SBP (−1.5 mmHg) but higher DBP (+2.5 mmHg) than the aneroid device (Schaefer et al., 2021). Individuals owning a BP monitor compared to nonowners had lower readings (−3.7 mmHg SBP, −2.8 mmHg DBP) (Akpolat et al., 2018). The pulse wave wrist cuff (CDXP) measured a slightly lower SBP (−0.7 mmHg) and slightly higher DBP (+0.4 mmHg) relative to the aneroid standard. Similarly, the Omron M6 produced higher SBP (+1.5 mmHg) but lower DBP (−2.8 mmHg) (Hofstede et al., 2022). Similarly, comparing validated and nonvalidated devices, both SBP and DBP remained within ±5 mmHg (Tremonti et al., 2017). Different model of BP devices showed variable differences relative to the sphygmomanometer: Omron BP5450 (+0.5 SBP, +2.5 DBP), UA-8000WM (+1.9 SBP, +3.6 DBP), WGNBPA-240BT (+2.5 SBP, +5.5 DBP), and BP3MW1–4YC (+7.9 SBP, +5.5 DBP) (Jung et al., 2015) (Supplementary Table1).
Protocol-Related Factors
Two studies compared HBPM with other protocols (Chung et al., 2009; Groenland et al., 2022) (SupplementaryTable1). The mean differences in Home Microlife watch in pregnant women compared with the British Hypertension Society (BHS) protocol showed small variations with SBP (0.4 mmHg) DBP (−0.4 mmHg). In preeclampsia, the Home Microlife watch has small decrease in SBP by −2.6 mmHg and small increase in DBP by 0.8 mmHg relative to the BHS protocol (Chung et al., 2009). The 7-day, twice-daily European protocol showed lower values than true home BP (−9.5 mmHg SBP, −4.8 mmHg DBP) but higher values than the Microlife Average Mode (MAM) (+5.2 mmHg SBP, +3.3 mmHg DBP), whereas the 3-day protocol was more closely aligned with true home BP (+1.5 mmHg SBP, +1.0 mmHg DBP) and the MAM (+4.8 mmHg SBP, +2.3 mmHg DBP) (Groenland et al., 2022) (Supplementary Table1).
Observer-Related Factors
Three studies explored variations in HBPM among observer-related factors (Campbell et al., 2001; Liu et al., 2024; Nessler et al., 2023) (Supplementary Table 1). Patient-measured BP readings were higher than researcher measurements, with a moderate increase of 8.36 mmHg for SBP and small increase of 2.16 mmHg for DBP (Nessler et al., 2023). Patient readings were higher than nurse measurements at 5 min (+9.1 mmHg SBP, +1.5 mmHg DBP) but decreased after 5 min (+3.8 mmHg SBP, +1.1 mmHg DBP) (Campbell et al., 2001). Compared with nurse measurements, patient self-measurement showed slightly lower values with a standard cuff (−1.1 mmHg SBP, −0.9 mmHg DBP) and with an extralarge cuff (−2.9 mmHg DBP) (Liu et al., 2024) (Supplementary Table1).
Discussion
The variations found in this systematic review raise concerns about the reliability of HBPM for HTN management in adults. Such variations can affect the diagnosis, treatment, monitoring, cardiovascular risk prediction, and advice given to patients. Large increases in the variation raise cardiovascular risk, while large decreases may cause dizziness or fainting in hypertensive patients. These variations are clinically important for outpatient monitoring (e.g., BP, heart rate, pulse), diagnosis, and follow-up of HTN. Similarly, a study found that BP is not constant; it fluctuates daily due to factors such as stress, activity, diet, and medication (Kawano, 2011). In addition, there is a significant difference between “true” resting BP and measured BP, impacting decisions for patient monitoring, diagnosis, and HTN management (Kallioinen et al., 2017). Therefore, understanding these variations is essential to improve clinical decision-making and ensure accurate HBPM assessment for hypertensive patient better outcomes.
This review also revealed that HBPM combined with weekly counseling and health coaching significantly reduced SBP, including BP device ownership. SBP was more unstable before the educational intervention. Similarly, a study revealed that self-monitoring of BP with moderate to high educational interventions support significantly reduced HBPM (Rahimi et al., 2017). Counseling and health coaching reduce BP by promoting self-care, medication adherence, lifestyle changes, and patient engagement, while supporting better communication with healthcare providers (Margolius et al., 2012). Furthermore, temperature changes are associated with BP fluctuations, with cool indoor temperatures increasing SBP and exposure to low temperatures increasing BP at home (Huang et al., 2019; Saeki et al., 2014; Wang et al., 2017). Cold indoor and outdoor temperatures increase SBP by causing blood vessel constriction and increasing cardiovascular strain, especially in elderly individuals, hypertensive individuals, and women (Janssen et al., 2023). These findings underscore combining HBPM with regular counseling and health coaching, consider device ownership, and temperature effects to improve BP control in hypertensive adults.
In this review, it was found that incorrect cuff size use has effect on BP readings; too small leads to overestimation (false HTN), and too large results in underestimation (missed HTN). A similar previous study also found that incorrect cuff size use can fluctuate systolic BP readings by approximately ±5 mmHg, which may misclassify HTN (Padwal et al., 2019). Furthermore, cuff inflation effect persists during continuous HBPM is also found in this review (Gazzola et al., 2018). Self-initiated BP measurement using a fully automated BP device provides more reliable readings than a semiautomated method by reducing autocuff-related inflation effects (Berkhof et al., 2020). Hence, it is recommended to use properly sized, fully automated BP cuffs for HBPM to reduce measurement variations and improve accuracy. Furthermore, this review revealed that morning BP tended to be lower than evening BP and larger fluctuations were observed in older adults. Different fruit consumption has been associated with small reductions in BP (Fujiwara et al., 2018). Morning BP readings are more reliable for monitoring trends, guiding treatment, and predicting cardiovascular risks because they establish a consistent baseline before daily activities, stress, and food intake can influence the results (Fujiwara et al., 2018). Blood pressure tends to rise with age, mainly due to arterial anatomical and physiological changes, particularly increased stiffness of the large arteries (Singh et al., 2025). Eating fruits and vegetables rich in nutrients such as potassium, nitrates, and fiber helps lower BP by improving blood vessel function, reducing inflammation, and supporting healthy weight (Altawili et al., 2023). In contrast, this review found that exposure to tobacco smoke increased BP in patients not treated with antihypertensive medication, but had less impact on BP than those on antihypertensive medication. Tobacco smoke, including secondhand smoke exposure, increases BP by stimulating vasoconstrictive hormones and damaging arteries (plaque buildup), leading to narrowed blood vessels and increased pressure (Leone, 2005). This highlights to measure BP in the morning for accurate HBPM, encourage fruit and vegetable intake, and minimize exposure to tobacco smoke, especially in older adults, while considering seasonal and lifestyle influences.
In addition, this review found that validated BP monitors were more reliable than invalidated devices in HBPM. Observer-related factors also contributed to variations, with patients frequently recording higher BP readings than those who measured their BP (e.g., researchers and healthcare providers), particularly before rest periods. Previous studies have also indicated that patients may show higher BP readings than professionals due to anxiety (white-coat effect), poor positioning, talking during measurement, or a less standardized technique (Padwal et al., 2019). Studies have also shown that many invalidated BP devices lead to wide variations in the HBPM (Picone et al., 2020). Upper-arm BP measurements are more accurate than wrist BP measurements (Zweiker et al., 2000). Arm cuffs measure BP at the brachial artery, while wrist cuffs measure it at the radial artery, and arm position affects readings because placing the cuff above heart level lowers them and placing it below heart level raises them due to gravity (Gavish & Gavish, 2011; Mukkamala et al., 2022). Incorrect arm positioning, such as an unsupported arm on the lap or hanging by the side during BP measurement, can falsely raise readings by increasing the distance from the heart or causing muscle strain (Netea et al., 2003). These show the use of validated upper-arm BP devices for HBPM, ensure correct arm positioning at heart level, and follow standardized measurement techniques to reduce observer- and device-related variations.
Protocol-related factors in the 7-day HBPM protocol provided more reliable BP readings than shorter durations (1–2 days). Hence, it is recommended that HBPM be initially recorded for 3 days and extended to 7 days if the average BP is close to the diagnostic or treatment threshold (Hodgkinson et al., 2019; Niiranen et al., 2011). Home BP monitoring should be taken using multiple readings via validated devices for at least 3 days, preferably 6–7 days, in the morning and evening (Lurbe et al., 2016). A 7-day HBPM protocol offers more accurate and reliable readings by averaging daily variations, reducing white-coat or masked effects, and capturing true BP trends, which improves the diagnosis and prediction of outcomes (Groenland et al., 2022; Morris et al., 2025). Hence, it is recommended to use a 7-day HBPM protocol with two consecutive readings taken twice daily, discard the first day's measurements, and average the remaining readings to improve diagnostic accuracy and capture true BP trends.
In this review, studies comparing HBP with office BP found that HBP measurements were generally lower than office BP measurements (Verberk et al., 2005). Home BP measurements are generally lower than office readings because they avoid the stress-induced “white coat effect” and allow for multiple readings in a calm environment (Little et al., 2002). Studies show that patients with cardiovascular conditions often have higher BP due to changes such as heart muscle thickening and stiff arteries, which increase heart workload and reduce blood flow regulation (Messerli et al., 2017; Shams et al., 2025). Therefore, these findings are underscoring the use of validated upper-arm BP devices, ensure patients rest at least 5 min before measurement, perform HBPM 3–7 days, provide tailored monitoring and treatment for patients with cardiovascular comorbidities, and educate patients on proper techniques and lifestyle changes to improve BP control.
Subgroups Analysis
Pregnant women with poor sleep quality in the first trimester experience increased morning SBP as pregnancy progresses. Most BP devices used during pregnancy are accurate (within 5 mmHg) according to the BHS protocol. Poor sleep quality in the first trimester can raise morning BP, as hormonal changes, stress, and early pregnancy adaptations (e.g., increased blood volume and heart rate) trigger responses that elevate SBP (Okun et al., 2009; Remien & Majmundar, 2025). A study on pregnant women also found that the CDXP measured BP accurately, performing better than the Omron M6 in hospitals, and found that the CDXP is easy to use for HBPM (Supplementary Table 1) (Hofstede et al., 2022). Furthermore, automated oscillometric devices may not provide reliable results during pregnancy or preeclampsia, which necessitates further research (Nathan et al., 2015; Stergiou et al., 2018b). The CDXP device may be a preferred option for HBPM in pregnant women due to its accuracy and ease of use; however, clinicians and researchers should use caution with automated oscillometric devices during pregnancy and preeclampsia.
Strengths and Limitations of the Study
This systematic review provides a clear and comprehensive summary of evidence on variations in HBPM among adults with HTN. It combines findings from multiple reputable databases, uses well-defined categories to describe BP variations, and systematically identifies factors associated with these variations. Overall, the review establishes a strong foundation for improving the accuracy of HBPM, measurement, guiding clinical practice, and supporting future research on HTN management at home.
To our knowledge, this review did not identify factors associated with HBPM variations in patients with arrhythmia, those with large arm circumferences, or older adults, likely because of the challenges of conducting such studies at home. Due to the nature of studies design, scope and analysis methods used, a meta-analysis was deemed, and findings were synthesized narratively. Restricting inclusion to English-language, peer-reviewed studies may have introduced publication selection bias. Furthermore, all selected studies were conducted in adult populations (≥18 years), limiting its generalizability.
Implications for Practice
The findings underscore the importance of cautious interpretation of home BP readings and adherence to standardized monitoring protocols to enhance reliability. In addition, this systematic review highlights the vital role of nurses in ensuring accurate and consistent HBPM among adults with HTN. Nurses should promote the use of validated devices, standardized measurement protocols, and proper techniques, such as correct posture, cuff placement, and timing of readings at home. Awareness of factors that associated with variations in HBPM, such as device type, measurement procedures, observers’ differences, and patient adherence, is essential for accurate interpretation of BP. By providing education and emphasizing repeated, reliable BP measurements, nurses can enhance diagnostic accuracy, support effective HTN management, empower adults with HTN self-care, and ultimately reduce cardiovascular risk.
Conclusion
This systematic review found variations and factors associated with HBPM among adults with HTN. Although HBPM remains essential for diagnosis, management, and cardiovascular risk prediction, it is affected by both internal and external factors. SBP readings, which generally show greater fluctuations than DBP readings, present challenges for a consistent assessment.
Future research should explore the long-term effects of HBPM variations, evaluate interventions to improve HBPM reliability (education, standardized protocols, and digital tools), assess cost-effectiveness of validated devices, examine patient factors and cultural differences, and develop innovative HBPM technologies.
Supplemental Material
sj-docx-1-son-10.1177_23779608251403037 - Supplemental material for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review
Supplemental material, sj-docx-1-son-10.1177_23779608251403037 for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review by Tecleab Okubai, Desale Tewelde Kahsay, Tesfit Brhane Netsereab and Melat Adugna Asnake in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251403037 - Supplemental material for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review
Supplemental material, sj-docx-2-son-10.1177_23779608251403037 for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review by Tecleab Okubai, Desale Tewelde Kahsay, Tesfit Brhane Netsereab and Melat Adugna Asnake in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608251403037 - Supplemental material for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review
Supplemental material, sj-docx-3-son-10.1177_23779608251403037 for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review by Tecleab Okubai, Desale Tewelde Kahsay, Tesfit Brhane Netsereab and Melat Adugna Asnake in SAGE Open Nursing
Supplemental Material
sj-docx-4-son-10.1177_23779608251403037 - Supplemental material for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review
Supplemental material, sj-docx-4-son-10.1177_23779608251403037 for Factors Associated with Variations in Home Blood Pressure Monitoring among Adults with Hypertension: Systematic Review by Tecleab Okubai, Desale Tewelde Kahsay, Tesfit Brhane Netsereab and Melat Adugna Asnake in SAGE Open Nursing
Footnotes
Acknowledgments
The authors sincerely thank Associate Professor Rumei Yang for her valuable contribution in enhancing the quality of this manuscript.
Consent for Publication
The authors declare that all data are open to publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing was not applicable to this study because no datasets were generated or analyzed. Therefore, no data were available.
Supplemental Material
Supplemental material for this article is available online.
Authors’ Statement
Desale Tewelde Kahsay and Tecleab Okubai: Conceptualization, original draft preparation, methodology visualization, data extraction, and interpretation. Tesfit Brhane Netsereab: writing, reviewing, editing, and resolving any discrepancies. Melate Adugna Asnake: writing and reviewing. All the authors have read and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.