
Abstract
Background
White coat hypertension (WCH) is characterized by elevated clinic blood pressure (BP) measurements and normal out-of-clinic readings. Once considered benign, emerging evidence suggests WCH is associated with increased cardiovascular risk and mortality.
Methods
This feasibility study was conducted at a primary care clinic in Singapore between November 2019 and October 2023. Individuals with elevated clinic BP were recruited through convenience sampling. Data was collected across two visits via an interviewer-administered questionnaire and a weeklong self-measured BP monitoring program. Home BP readings were interpreted utilizing three methods: (1) average of all readings, (2) 2018 ESH/ESC guidelines, and (3) clinician “eyeball method”. WCH was diagnosed in individuals with elevated clinic BP readings and normal home BP readings.
Results
Sixty individuals were recruited, with a mean age of 61.8 ± 9.6 years, most were Chinese (90%) and married (63%). Nearly half the participants had hyperlipidemia with 56.7% overweight or obese. WCH was diagnosed in 23.3% of participants, while 35% were newly diagnosed with hypertension. None of the individuals with WCH reported significant anxiety as assessed using the GAD-7 scale. The clinician “eyeball method” resulted in five more individuals being diagnosed with hypertension compared to the 2018 ESH/ESC method.
Conclusion
Over half of individuals with elevated clinic BP had WCH or undiagnosed hypertension. Primary care physicians should promote home BP self-monitoring and adopt standardized guideline-based methods for home BP interpretation. Future research should explore practical strategies to assimilate guidelines to real-world practice, improving diagnostic accuracy and treatment.
Keywords
Introduction
White coat hypertension (WCH) is defined as an elevated blood pressure (BP) measurement in a healthcare setting with normal ambulatory readings. 1 Historically, WCH was considered a benign condition not associated with increased cardiovascular disease risk.2,3 Consequently, individuals with WCH are often not prescribed anti-hypertensives due to the potential risk of postural hypotension, falls, and increased pill burden. 4 However, recent studies suggest that individuals with WCH could have an increased risk of cardiovascular disease and mortality compared to their normotensive counterparts.5,6
Primary care serves as the ideal setting for the timely diagnosis and management of WCH. As the first point of contact to healthcare for most adults, primary care providers are well-positioned to identify individuals with elevated clinic BP readings. 7 Prior studies found that 15% to 30% of individuals presenting with an elevated clinic reading have underlying WCH.8,9 If the local population reflects a similar proportion, more resources should be dedicated to developing evidence-based strategies to manage WCH in primary care.
Despite its importance, WCH diagnosis in primary care is challenging as it relies heavily on individuals consistently and accurately monitoring their home BP. While global BP machine ownership is high, ranging between 50% and 60%, only half regularly monitor their home BP.10–12 Individuals often do not monitor their home readings citing a lack of time or motivation, failing to understand its significance. 13 Additionally, individuals who monitor their home BP often do so with wide variation in practices and inconsistencies in documentation thereby limiting its usability. 13 The lack of reliable home BP monitoring readings hamper accurate WCH diagnosis and limits our understanding of WCH prevalence in the local setting.
Presently, there is limited local data on the proportion of individuals with WCH in the primary care setting. Ascertaining this proportion and potential associated factors could inform the development of local WCH clinical guidelines. Uncovering the associated factors could enable the early identification of individuals at higher risk so that appropriate interventions can be administered expediently. These findings could reduce the incidence of adverse cardiovascular outcomes among individuals with WCH.
This study aims to assess the feasibility of using self-measured blood pressure monitoring to assess for white coat hypertension among individuals with an elevated clinic BP reading in the local primary care setting.
Material and methods
Study design and setting
This single-center feasibility study was conducted in one primary care clinic in Singapore between 1st November 2019 to 18th October 2023.
Participants
Singaporean and Singaporean permanent residents aged between 40 and 80 who presented to Outram Polyclinic with an elevated blood pressure (BP) measurement of systolic or diastolic readings of >140 mmHg or >90 mmHg respectively were included in the study. Individuals with known hypertension or who are pregnant, hearing, visually, cognitively impaired, and acutely unwell were excluded from the study.
Subject recruitment
Subjects were recruited through convenience sampling. Treating physicians referred individuals with an elevated clinic BP reading to the study team for possible recruitment. The study team screened referred individuals for eligibility before obtaining informed consent.
Visit schedule
This was a two-visit study with eligible and agreeable individuals recruited into the study. At the first visit, they completed a questionnaire and were enrolled in a week-long self-measured home BP monitoring program. They were loaned a BP machine and provided a diary detailing the recommended monitoring time points.
Three days post-study enrolment, the study team contacted individuals to enquire if they had started monitoring their BP and if they encountered any issues.
At the second visit, participants had their second clinic BP reading measured, returned the BP device and submitted their diary.
The study team ensured that individuals with newly diagnosed hypertension or possible anxiety had a doctor’s appointment to review their condition.
Variables
Clinic blood pressure
The clinic BP measurement was performed using a regularly calibrated automated BP device (OmronTM HEM-7280T) by trained healthcare staff. Readings were considered abnormal should the systolic BP ≥140 mmHg or the diastolic BP ≥90 mmHg.
Home blood pressure measurement
The home BP readings were performed by study participants across seven days and captured in the study diary provided using a regularly calibrated study-issued device. All participants were loaned a BP machine, regardless of ownership, to ensure standardized home BP readings. BP measurements were taken twice daily, once in the morning and once in the evening, with two measurements taken at each session one to two minutes apart.
Home blood pressure interpretation
Three methods were used for home BP interpretation: 1. Method 1: The mean of all BP readings collected over seven days was calculated. 2. Method 2: Per the ESH/ESC 2018 guidelines, at least 16 out of 28 readings were required, with the first day’s readings excluded, ensuring at least 12 readings for analysis.
14
3. Method 3: A clinician reviewed all BP readings and diagnosed hypertension if more than half the readings over seven days were elevated.
The mean BP readings were considered elevated if the systolic BP ≥135mmHg or the diastolic BP ≥85 mmHg. 14
Definition of white coat hypertension
Definition of White coat hypertension.

Generalized Anxiety Disorder (GAD-7) Scale
The GAD-7 scale was implemented as anxiety is associated with white coat hypertension. 15 A cut-off of 10 points was used to identify individuals requiring doctor’s review as it corresponded with moderate anxiety. 15
Data collection
Study questionnaire
The data was collected via an interviewer-administered questionnaire that underwent content and face validation. The questionnaire collected demographic, medical information and the Generalized Anxiety Disorder (GAD-7) scale.
Home blood pressure diary
The diary was developed and adapted from the existing clinic BP diary, incorporating instructions from the 2018 ESH/ESC guidelines and can be found in Appendix 1. 14 The diary underwent content validation through consultation with senior Family Physicians, who assessed its relevance, comprehensiveness and alignment with practice guidelines. Thereafter, face validation was performed through input from practicing physicians to ensure clarity and usability in practice before being used in the study.
Sample size calculation
To identify the potential problems for pilot studies, at least 30 subjects are sufficient to estimate a parameter. 16 The final sample size was 60 subjects, with a buffer of 50% for dropouts and missing data.
Statistical analysis
Demographics were summarized for participants with continuous variables presented in mean and standard deviation, while categorical data are presented as frequency counts and percentages. All analyses were performed with SPSS version 25.0.
Results
Baseline characteristics (N = 60).

Comparison of methods for blood pressure interpretation.
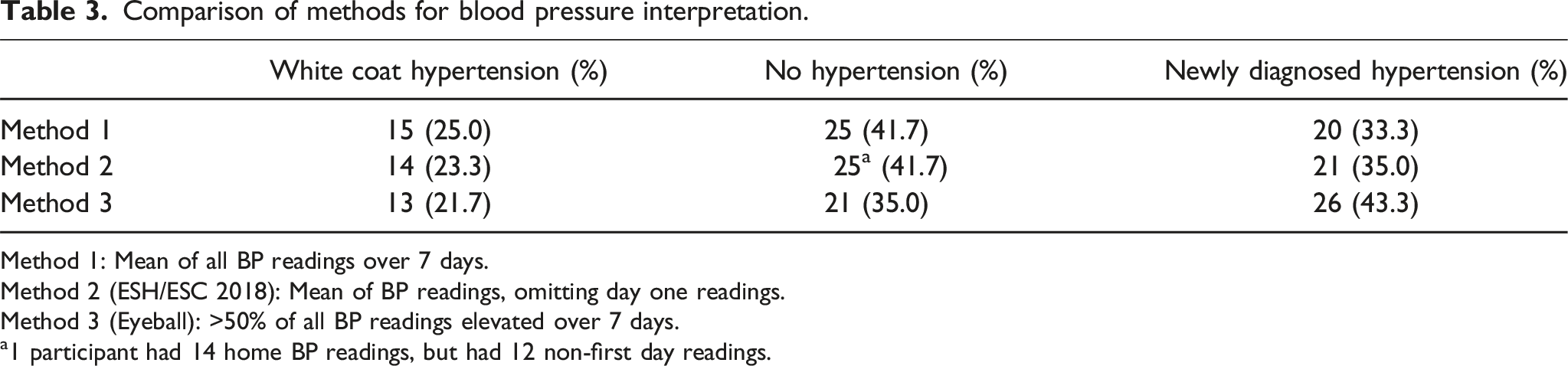
Method 1: Mean of all BP readings over 7 days.
Method 2 (ESH/ESC 2018): Mean of BP readings, omitting day one readings.
Method 3 (Eyeball): >50% of all BP readings elevated over 7 days.
a1 participant had 14 home BP readings, but had 12 non-first day readings.
Diagnosis and GAD-7 scores.
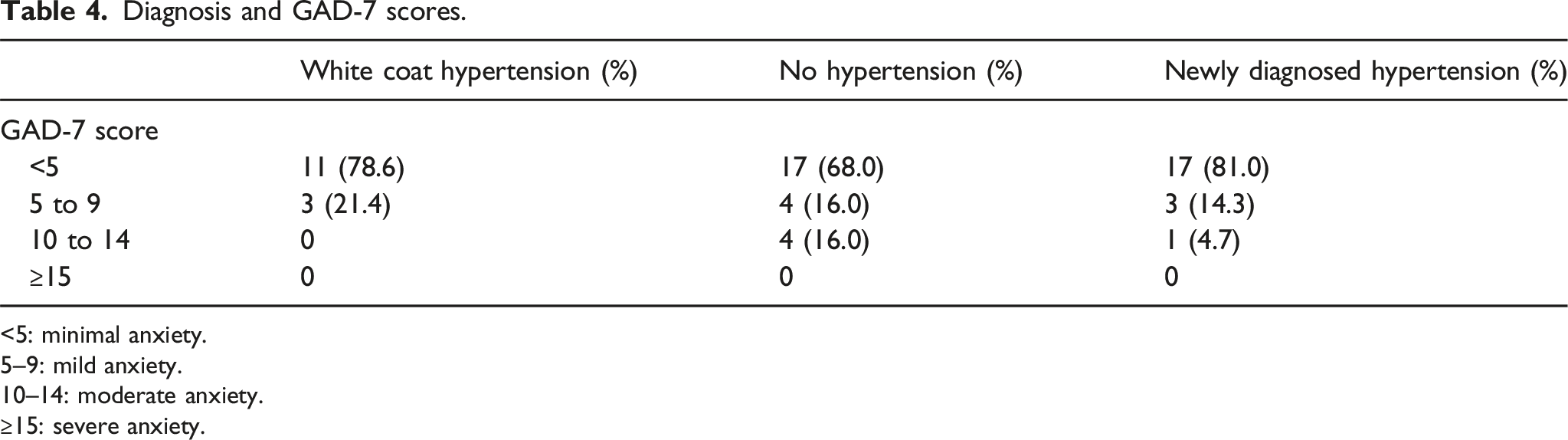
<5: minimal anxiety.
5–9: mild anxiety.
10–14: moderate anxiety.
≥15: severe anxiety.
Discussion
Hypertension phenotypes
This study found that 23.3% of untreated individuals with elevated blood pressure (BP) attending a primary care clinic in Singapore had white coat hypertension (WCH), consistent with reported prevalence rates of 15% to 30% in prior studies.8,9 Additionally, 35% of participants had newly diagnosed hypertension, within the 5% to 37.3% range seen in international studies.17,18 These findings highlight the significant prevalence of both WCH and hypertension among individuals with elevated clinic BP. To ensure timely and accurate diagnosis, physicians should advocate for home self-monitoring, which distinguishes between hypertension phenotypes, and reduces misdiagnosis and inappropriate treatment.
WCH and anxiety
Psychological characteristics, particularly anxiety, have been previously linked to WCH. 19 Our study, conducted among individuals without any known psychiatric conditions, found no difference in anxiety levels between individuals with WCH and those without. This finding aligns with prior research finding no association between general anxiety traits and WCH. 20 Interestingly, studies focused on context-specific anxiety, such as anxiety directly related to clinic visit suggest that a patient’s expectation of high BP or stress during the visit can lead to a transiently elevated BP. 21 These findings suggest that WCH may be more closely linked to context-specific anxiety surrounding the clinic visit rather than general anxiety traits. Recognition of this finding could guide interventions targeted at reducing patient stress during visits to optimize diagnostic precision.
Home blood pressure interpretation
Despite the small sample size, this feasibility study highlights the potentially profound impact of home BP interpretation methods on the ability to diagnose hypertension phenotypes accurately. Calculating the mean BP readings across seven days showed comparable accuracy to the 2018 ESH/ESC guideline-based approach in excluding hypertension. The guideline-based approach excludes the day-one readings as these readings are usually higher and unstable, possibly stemming from anxiety associated with BP self-monitoring. 22 Interestingly, this approach resulted in one more individual being diagnosed with hypertension instead of WCH.
In contrast, the “eyeball method” led to five (12%) additional individuals being newly diagnosed with hypertension. This commonly practiced method involves a clinician visually scanning BP readings to determine the presence of elevated readings.13,23 However, this method is imprecise, contributing to potential misdiagnosis and overtreatment. Many physicians continue to adopt this practice due to time constraints in consultations and the frequent use of handwritten BP records, which render the calculation of mean readings a challenge.13,24
Addressing these challenges necessitates a multi-pronged approach. Patients and caregivers should be actively encouraged to perform home BP measurements and those with Bluetooth®-enabled devices should connect them to the associated app to facilitate BP tracking. Physicians should be reminded to adopt guideline-based practices and advocate for digital home BP recording to ensure the fidelity of readings and simplify interpretation. Additionally, digital solutions that automate the conversion and interpretation of handwritten BP records would enable appropriate care for patients who cannot use digital tools. Collectively these measures could improve the accuracy of home BP interpretation, facilitating improved diagnostic accuracy and treatment.
Limitations
This study has several limitations as a single-center feasibility study. Firstly, the findings are not generalizable to the wider Singapore population because participants were recruited from a single primary care clinic. Secondly, subject recruitment was challenging due to the restrictions imposed by the COVID-19 pandemic. Concerns over disease transmission and patient safety resulted in a protracted enrollment period. Future multicenter studies with larger, more representative populations could overcome these limitations and validate the study findings.
Conclusion
This study provides potentially valuable insights into the prevalence and diagnosis of white coat hypertension, with over half of individuals with elevated clinic BP found to have WCH or undiagnosed hypertension. These findings highlight the need for primary care physicians to promote home BP self-monitoring and adopt standardized, guideline-based methods for home BP interpretation. The clinician “eyeball method” could result in an overdiagnosis of hypertension and unnecessary pharmacological treatment; it should be replaced by guideline-backed practices. Future studies should focus on simplifying the integration of these evidence-based practices into daily primary care practice, thereby enhancing diagnostic accuracy and ensuring appropriate treatment for patients.
Supplemental Material
Supplemental Material - Prevalence of white coat hypertension (WCH) among individuals with elevated clinic blood pressure: A feasibility study
Supplemental Material for Prevalence of white coat hypertension (WCH) among individuals with elevated clinic blood pressure: A feasibility study by Jing Yi Lim, Prawira Oka, Lynette Ong, Jannathnisha Binte Mohideen Pitchay and Wei Ling Ng in Proceedings of Singapore Healthcare
Footnotes
Acknowledgments
The authors would like to thank Dr Tan Ngiap Chuan for his mentorship.
Author Contributions
PO and WLN conceptualized the study. JYL, PO, LO, JBMP and WLN performed subject recruitment and data collection. PO performed data analysis. JYL, PO, LO, JBMP and WLN interpreted the results. JYL and PO drafted the manuscript. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in kind (research expertise) by the SingHealth Polyclinics Research Department and received no grant from any funding agencies.
Ethical Statement
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to subject confidentiality but are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.