
Abstract
Introduction
Hypertension is the most common older adults’ health problem in Indonesia. Older adults experience various changes in their life that often contribute to their ability to manage health problems, especially in chronic diseases.
Objectives
This study aimed to understand the problems and needs of self-management of older adults with hypertension.
Methods
This was a qualitative exploratory descriptive design. Data collection was conducted among 62 participants. Participants were 15 older adults with hypertension and 11 older adults’ families, 12 primary care nurses, seven medical doctors, 11 health volunteers, three heads of primary care, and three district health officials selected by purposeful sampling. Data were collected using semistructured, face-to-face interviews (older adults and their families) and focus group discussion (healthcare workers). Data analysis was carried out qualitatively descriptively using an inductive thinking process; Colaizzi's measures were used for analysis.
Results
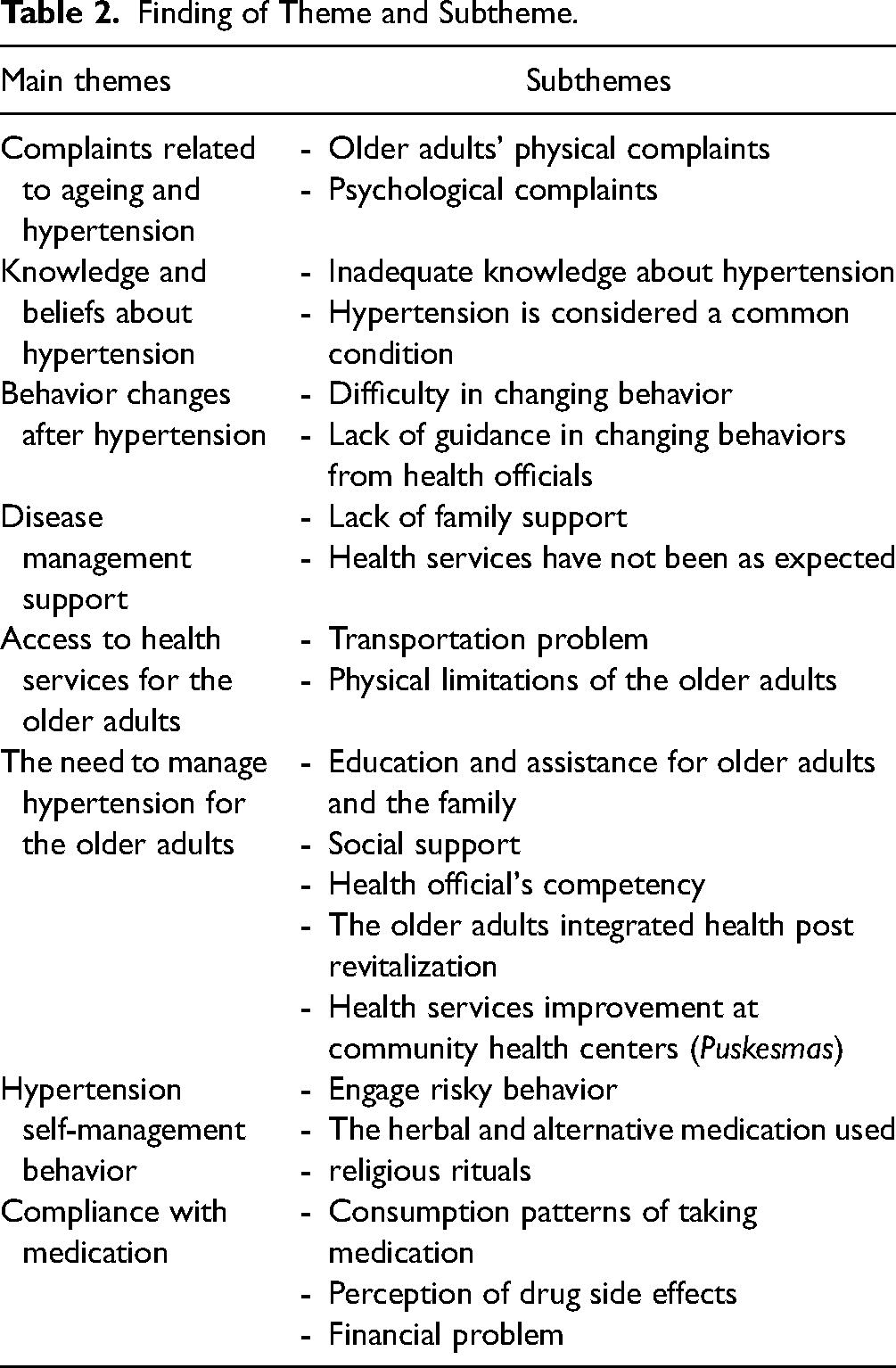
This study identified eight main themes: (1) complaints related to aging and hypertension, (2) knowledge and beliefs about hypertension, (3) behavior changes after hypertension, (4) disease management support; access to health services for older adults, (5) the need to manage hypertension for older adults, (6) disease management support, (7) hypertension self-management behavior, and (8) compliance with medication.
Conclusion
This study provided evidence regarding older adults’ problems and needs in managing hypertension. These findings should be considered while providing nursing care at the community level to initiate the self-management of hypertension in older adults.
Introduction
The older adult population increased almost twice during 50 years (Central Bureau of Statistics, 2022). Hypertension is persistent among the older adults in Indonesia (Sari et al., 2021). Data show the prevalence of hypertension in the age group 55 to 64 years 55.23%, 65 to 74 years 63.22%, and >75 years 69.54 (Indonesian Ministry of Health, 2018). Hypertension is a significant risk factor for cardiovascular diseases, artery disease, stroke, kidney disease, peripheral artery disease, and hypertensive retinopathy (Muhadi, 2016). Therefore, hypertension prevention is a method for controlling noncommunicable disease, which is the highest cause of death in the world.
The increasing prevalence of chronic diseases such as hypertension is associated with aging and the resulting behavioral changes in individuals, families, communities, and healthcare providers. Current knowledge recommends health promotion to be delivered in the context of individuals and families. Therefore, patients and their families are expected to engage in behaviors that promote health and modify their lifestyles (Khemthong & Saravitaya, 2010; Malarvizhi et al., 2015). Self-management is believed to facilitate better health outcomes for patients, caregivers, and involved stakeholders, making it one of the strategies to minimize the burden of chronic diseases (Khemthong & Saravitaya, 2010). Self-management is considered one of the strategies for providing care for chronic health problems such as hypertension.
Review of the Literature
Being older adults means that many changes occur from various physical, mental, and social aspects, and those changes may affect the ability of older adults in the management of hypertension (Oliveros et al., 2020). Furthermore, hypertension needs lifetime management (Guasti et al., 2022; Wenger & Bilen, 2020; Zhou et al., 2019). Based on studies report the problems of older adults in managing hypertension (McGurgan et al., 2022). Individuals and families with hypertension have different experiences of long-term management of hypertension. These include feeling too healthy, forgetting to comply with medication (Indonesian Ministry of Health, 2018), lack of knowledge (Sinuraya et al., 2017), transportation problems to access healthcare (Setiawan et al., 2017), lack of family support, and problems among family (Costa & Nogueira, 2008; Gholamnejad et al., 2018).
For self-management, the reference for this can be made to the Individual and Family Self-Management Theory (IFSMT) (Polly & Sawin, 2009). This theory defines self-management as a process in which individuals and families utilize knowledge and beliefs, self-regulation skills and abilities, and social facilitation to achieve health outcomes. Self-management operates within the context of specific health conditions, the physical and social environment, and the individual and family's risk and protective factors. Self-management can be applied to chronic conditions as well as health promotion efforts (Polly & Sawin, 2009). Self-management is measured based on consistent behaviors related to adherence to plans and active information, as well as adherence to treatment. Previous studies reported the challenges faced by older adults in managing hypertension, such as medication noncompliance (Burnier et al., 2020), lack of knowledge (Oliveros et al., 2020; Uchmanowicz et al., 2018), and familial influences (Presilia et al., 2020). Therefore, conducting explorations using qualitative approaches would be beneficial. In Indonesia, based on studies about older adults with hypertension use qualitative approaches; thus, this study aims to explore the needs and problems of older adults to manage hypertension.
Methods
Design
This study used a qualitative exploratory descriptive design. This study was employed to understand the problems and needs of the older adults to manage hypertension. This method is suitable for reporting commonalities mentioned in data, particularly for exploratory work where frequency contributes to the analysis (Vaismoradi et al., 2013). Data were collected using in-depth interviews and focus group discussion (FGD) in April 2020. Deep interviews were conducted for 1 to 1.5 h per participant.
Research Questions
This study aims to explore the problems and needs of the older adults to manage hypertension. Previous research reported in similar or earlier articles can strengthen our hypothesis in designing or analyzing the research conducted in our current study. There were four topics for an in-depth interview and focus group discussion:
What are the problems of older adults in managing hypertension in the community? What are the needs of older adults in managing hypertension in the community? How are the health services for older adults with hypertension? What is the role of social support for older adults with hypertension?
Sample and Settings
For interview, this study was conducted in a community and healthcare facility Indonesia. The participants were selected when the older adults visited the older adults integrated health post (Posyandu Lansia). All respondents were Muslim. Based on the criteria and data saturation, this study involved 15 older adults and 11 families from three selected community health centers in Indonesia as the research sites. For FGD, the healthcare professionals involved in this study included nurses, doctors, the head of the community health center, and sections from the South Tangerang Health Office in Banten. The sections from the health office included the Family Health section, Non-Communicable Disease Control and Prevention section, and Primary Care section. Meanwhile, the participants from the health volunteers were the cadre members of the older adults integrated health post. Before this study, the participants and researchers did not have any relationship. The total number of participants was as follows: 12 nurses, seven doctors, three heads of community health centers, three heads of sections from the health office, and 11 cadre members of the older adults integrated health post. The participants invited to this study have agreed to participate. The total informants in this study were 62 informants, with three district health officials selected by purposeful sampling. In-depth interviews and focus group discussions were carried out to collect the data. The community-dwelling data were collected in three areas of community health centers in South Tangerang City, namely: Pisangan, Pamulang, and East Ciputat. These locations were chosen based on the high prevalence of hypertension in these three community health centers. The prevalence of hypertension on the area was 22.2%, 32.4%, and 41.9%, respectively (Febrianti & Mustakim, 2019; Hasanah & Fadlilah, 2021).
The study included older adults who were registered as hypertensive patients at the community health center, were aged 60 years or older, had a family member acting as an informal caregiver, and were able to speak Indonesian. Older adults were excluded if their systolic blood pressure was greater than 220 mmHg or their diastolic blood pressure was 120 mmHg or higher, or if they had documented cognitive impairment. Family caregivers were included if they were related to the older adult with hypertension (such as a spouse, child, son-in-law, or sibling), were willing to provide informal care and support at home, and lived in the same household as the older adult. Family caregivers were excluded if they had documented cognitive impairment. The inclusion criteria for primary care nurses and medical doctors were as follows: they had to be nurses or medical doctors working in community health centers with a minimum of 1 year of work experience, and they had to be willing and capable of providing detailed information related to health services associated with hypertensive older adults. For the head of primary care, the inclusion criterion was serving as the head of the reference. Meanwhile, the inclusion criteria for district health officials were as follows: they had to be serving as an official in the Family Health Section, Primary Services, or the Prevention and Non-Communicable Disease Control Department in the South Tangerang Health Office, and they had to be willing and capable of providing in-depth information about health services related to hypertension in older adults.
The data analysis process involved repeatedly reading the complete transcript to extract relevant meanings pertaining to the experiences of older adults in managing hypertension. Irrelevant phrases and sentences were excluded, focusing on significant data. Keywords were identified by filtering information from participants that aligned with the research objectives. These keywords were then carefully formulated into themes, ensuring consistent meaning and validating them based on participants’ statements. Subsequently, subthemes were derived from related themes, which were further organized into themes that represented the overarching concepts. The alignment of these themes with the research objectives was ensured. The research findings were presented concisely, using a narrative format and tables that followed the structure of specific research objectives, themes, and subthemes, providing a comprehensive depiction of each theme's formation in relation to each research objective: Community health centers, willing and able to provide in-depth health service information related to older adults with hypertension.
Variables/Instruments
The principal project investigator of this study conducted the interviews. An example of an interview guide is shown in Table 1. The interview guide was developed with careful consideration of the research objectives and the scope of the study. It was pilot-tested on participants who had similar characteristics to those of the research participants. The questions focused on the needs and issues in the management of hypertension. Initially, demographic data about the older adults and their families were collected, including age, gender, marital status, education, profession, and their relationship with the older adults.
Sample Questions for Semistructured Interviews.

The interview with older adults and their families was focused on the following aspects: (1) participants’ understanding of hypertension and older adulthoods, (2) common symptoms experienced by older adults, along with the management of hypertension symptoms in older adults, (3) experiences in caring for older adults with hypertension, (4) family support in caring for older adults with hypertension, (5) health services for older adults with hypertension at health centers and in the community, including the challenges faced. The interviews and focus group discussions with healthcare professionals were focused on the following aspects: (1) activities and services for managing older adults with hypertension, (2) roles and activities of healthcare professionals in caring for older adults with hypertension, (3) issues and needs of healthcare professionals in caring for older adults with hypertension.
Data Collection
The interviews were conducted by the principal investigator (UK) who had a nursing background with prior training in qualitative research. UK and BAK developed semistructured questions that guided the interviews (Table 1). The interviews were conducted according to the agreed-upon terms and in an environment that was comfortable and calm at the informant's home. The researcher obtained prior consent from the informant if the interview process was recorded, and the researcher carried paper as a field note-taking tool during the research implementation process. The field note-taking tool was used to record nonverbal responses from participants, as well as environmental aspects and situations observed by the researcher. The interviewers explained the study purpose and content of the study and gained written consent. Informants who were illiterate gave verbal permission to one of their family members to sign the written consent on their behalf. Older adults were asked to freely describe their perceptions.
The interviews lasted a maximum of 40 min. The questions were pilot tested to the first participant met by the interviewer. No amendment was made after the investigators held an evaluation meeting about the pilot interviews. Meanwhile, the time required for the FGD was approximately 60 min. The FGD was conducted after obtaining consent and scheduling for the FGD session. The FGD took place in one of the rooms at the community health center. All information from the participants has been included in this article.
All interviews were digitally recorded with field notes kept, so, there is no need to conduct repeat interviews. The field note-taking tool was used to record nonverbal responses from participants, as well as environmental aspects and situations observed by the researcher. DWS validated the interpreter-facilitated interviews (Williamson et al., 2011) and transcribed all verbatim in Bahasa Indonesia, by which the data were analyzed. The verbatim test was conducted to ensure that everything is qualified.
Data Analysis
The interviews and focus group discussion took place over 2 months and were recorded using a digital recorder. The transcription took place as soon as possible after the interview was completed. Data were analyzed using thematic content analysis steps. The data analysis process involved repeatedly reading the complete transcript to extract relevant meanings pertaining to the experiences of older adults in managing hypertension. Irrelevant phrases and sentences were excluded, focusing on significant data. Keywords were identified by filtering information from participants that aligned with the research objectives. These keywords were then carefully formulated into themes, ensuring consistent meaning and validating them based on participants’ statements. Subsequently, subthemes were derived from related themes, which were further organized into themes that represented the overarching concepts. The alignment of these themes with the research objectives was ensured. The research findings were presented concisely, using a narrative format and tables that followed the structure of specific research objectives, themes, and subthemes, providing a comprehensive depiction of each theme's formation in relation to each research objective. After summarizing the data from the participants, the researchers clarified the participants’ responses that had been previously provided to the researchers.
Ethical Consideration
The present study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the ethical committee of the Faculty of Nursing University of Indonesia with number 41/UN2.F12.D/HKP.02.04/2018. All participants were informed about the research procedure. Written informed consent was obtained from all participants. All the participants whose data were collected received information about the protection of personal data.
Results
Demographic Information
Informants in this research were 62 participants for interview and FGD. Participants were 15 older adults with hypertension and 11 older adults’ families, 12 primary care nurses, seven medical doctors, three health volunteers, three heads of primary care, and three district health officials who were selected by purposeful sampling. The age of informants was collected only among older adults. Among older adults’ informants, 60% were in the group aged 61 to 70 years old. The majority of informants were women (80.7%); the level of education of older adults were elementary school (53.3%), the older adults’ family junior school (45.5%), the nurse's diploma in nursing (75%), medical doctor and chief of health center graduated from university (100%), the district health official graduated master level (100%).
The main findings of the study revealed eight themes (Table 2): complaints related to aging and hypertension, access to health services for older adults, knowledge and beliefs about hypertension, behavior changes following hypertension diagnosis, disease management support, the necessity of managing hypertension for older adults, hypertension self-management behaviors, and medication compliance.
Finding of Theme and Subtheme.
Complaints Related to Aging and Hypertension
This theme includes two subthemes based on Table 1.
Older Adults’ Physical Complaints
Physical problems experienced by older adults encompass symptoms related to hypertension as well as those associated with the aging process. These perceived complaints include symptoms directly linked to hypertension, such as dizziness and headaches, as well as those associated with aging, such as vision and hearing impairments. Participants expressed: “That is just headache, I want to sleep all day … it is in the back of the head.” (P9) “The older adults have hearing loss and are short-sighted.” (P29)
Psychological Complaints
Psychological problems refer to mental health issues perceived by older adults that they experience, such as: “After hypertension, I got the emotion problems, I became angry.” (P8). “I could not control my emotion.” (P12) “Father's emotions are never controlled; I am sometimes confused to deal with it.” (P17)
Knowledge and Beliefs About Hypertension
Knowledge and beliefs about hypertension encompassed the understanding and perceptions of older adults regarding hypertension, as well as any pre-existing beliefs they held about the condition. In this research, the study team aimed to deepen understanding by confirming participants’ comprehension of hypertension's definition, symptoms, and treatment. From participants’ responses, the researchers were able to infer the average level of knowledge among participants regarding hypertension. The subthemes identified within knowledge and beliefs about hypertension in this study included inadequate understanding of hypertension and the perception of hypertension as a common condition.
Inadequate Knowledge About Hypertension
Older adults showed an inadequate understanding of hypertension and its management, as quoted below: “No, I do not know what hypertension is, I just keep in mind the blood pressure is high, then the health official gives me those drugs, if it is a little better then I stop.” (P5) “Yes, if high blood pressure can be cured if we continue to take high blood pressure medication.” (P7) “I do not know about high blood pressure, is.” (P6) “We often provide health education in the community, one of which is about hypertension, but there are still older adults who lack understanding about hypertension and its treatment.” (P41)
Hypertension is Considered a Common Condition
The results of qualitative interviews indicated that hypertension was often regarded as a common condition by older adults. They did not consider hypertension to be something serious that required changes in behavior or effective disease management, as stated in the following interview statements: “It is just a common thing; I just don't think about it.” (P14) “High blood pressure, let it go, just break it.” (P14)
The health official stated: “So sometimes patients with hypertension are so proud of their hypertension. ‘Yes, my blood pressure is high, or my cholesterol is high.’ They are proud; sometimes we meet the client like that.” (P39)
Behavior Changes After Hypertension
Older adults generally found it challenging to make behavioral changes as a result of hypertension.
Difficulty in Changing Behavior
“Yes, it is hard to make changes to my behavior.” (P4) “I could not far from deep fried food” (P8)
The health official stated: “Awareness is still lacking.” (P27)
Lack of Guidance in Changing Behavior From Health Officials
The older adults feel there needs to be more guidance from health officials to make behavior changes. “In community health centers, I do not educate on how to make behavior changes, but the health official gives us information about we should reduce salt and exercise.” (P3)
Disease Management Support
Disease management support refers to the assistance perceived by older adults in managing their health problems.
Lack of Family Support
“There is no one to remind me when I do not take medicine.” (P4)
Health Services Have Not Been as Expected
“I do not want to go to community health centers; the queue is long, and the service only check the blood pressure.” (P1)
Access to Health Services for the Older Adults
Barriers to accessing health services for older adults were divided into two sub-themes, obstacles caused by transportation and older adults’ physical limitations.
Transportation Problem
Older adults often experience barriers to healthcare because of the distance; no one accompanies them to the health center. Those affect other problems, such as not being compliant to take medication because of the no antihypertensive drugs for older adults. “There is no transportation to go to the health centers, the cost of taxi bike much more expensive than the cost for health services.” (P4) “I go to community health centers to check my health, when someone accompanies me.” (P12)
Physical Limitations of the Older Adults
In addition to obstacles caused by transportation, obstacles to health services were also caused by physical limitations from the older adults. “I want to go to community health centers, but I am afraid, during on the street, I am getting old, very easy to be tired.” (P2)
The Need to Manage Hypertension for the Older Adults
This exploratory study identified five needs of the older adults (15 older adults and 11 families) in managing hypertension in the community, they were as below.
Education and Assistance for Older Adults and the Family
“Yes, I want to know a good management for the high blood pressure.” (P1)
“Yes, I was told to reduce cigarettes or something, but it is my habit, I need help how to reduce the cigarettes, not just to say reduce it.” (P23)
Social Support
Older adults needed support in managing their illnesses, such as taking medication regularly, adopting healthy behaviors, and receiving social support from the older adults’ integrated health post. “If someone always tells me, maybe it could be more routine to take medicine.” (P10) “Who can take medication for a lifetime? Surely there will be missed to taking medication the older adults need support from around him.” (P28)
Health Officials’ Competency
The competence of health officials, especially nurses, still needed improvement. “We have lack of training.” (P27) “We need training for nurses, especially about the nursing care. So there will be focus on nursing care, not medical treatment only.” (P41)
The Older Adults Integrated Health Post Revitalization
The older adults needed of activities in the older adults integrated health post could be improved, such as gymnastics access to antihypertensive drugs for the older adults in the older adults integrated health post, improvement of facilities and infrastructure in the older adults integrated health post, and health volunteer regeneration and training for health volunteers. “I want other activities in the older adults integrated health post, such as gymnastics, counselling, or other activities.” (P2) “We need training for health volunteers, such as on gymnastics, food, or nutrition for the older adults.” (P29)
Health Services Improvement at Community Health Centers
Health officials identified the preventive and promotional activities that needed to be carried out. However, there were numerous activities at the community health centers. “Yes. indeed, we see that community health centers should more activities on prevention.” (P34) “But because the function of community health centers now has shifted, not only besides promotion, preventive also rehabilitative but also … curative and rehabilitative.” (P35)
Hypertension Self-Management Behavior
Self-management behavior was the behavior shown by older adults to manage hypertension. Some older adults still engaged in risky behavior, frequently used herbs and alternative treatments, and relied on religious rituals.
Engage in Risky Behavior
Older adults still engaged risky behavior (already explained before education). such as less consumption of vegetables and fruit, eating salty foods, and fatty foods such as fried foods, smoking habits, drinking coffee, and lack of exercise. “I eat less fruit and vegetables; I do that, ha..ha..” (P8) “I do not exercise. (P11) “Yes, the community eat less vegetables and fruits, they afraid of getting uric acid.” (P35)
The Herbal and Alternative Medication Used
Most older adults used herbal medicines, because they fear the side effects of antihypertensive. “I use the herbs, such as habatusauda, ginger, chayote, celery, and so on.” (P6)
Religious Rituals
“Alhamdulillah, I like dhikr, I like to do the dhikr, begging my illness to be removed, the tensions are to go down, to be healthy.” (P7)
“I had better Umrah this 40 million, I sujud in front of the house of God, asking for apologizes, God willing.” (P10)
Compliance With Medication
Older adults did not comply with the medication because of fear of side effects, forgetfulness, or financial problems.
Consumption Patterns of Taking Medication
“Sometimes, I take the medicine today, and tomorrow I skip the medication; that is my pattern.” (P3).
“I take medication half of doses recommended by health officials.” (P6)
“If there is medicine, I take medicine routinely, but if there is no medicine, I do not take.” (P12)
Perception of Drug Side Effects
Perception of side effects of drugs was one part of the problem of taking medication adherence. “If you take too much medicine, there will be many chemicals in your body, so if I do not feel headache, I do not take medicine, I train my body to be free from medicine.” (P6)
Financial Problems
Financial problems became one of the obstacles for older adults in complying with their medication regimen. “If there is medicine, I take the medicine; if not, I do not take medicine, because you have to buy it, sometimes there is money, sometimes not hehehe.” (P7).
Discussion
To our understanding, this marks the inaugural examination into the challenges and requirements associated with self-management among older adults diagnosed with hypertension in Indonesia. Furthermore, it represents a limited inquiry that scrutinises this phenomenon through diverse lenses. The researchers gathered insights from various sources, including older adults, their families, primary care nurses, medical doctors, health volunteers, primary care administrators, and district health officials.
This study identified eight main themes, they were: complaints related to aging and hypertension, knowledge and beliefs about hypertension, behavior changes after hypertension, disease management support, access to health services for older adults, the need to manage hypertension for older adults, hypertension self-management behavior, and compliance with medication. This study was qualitative research that combines two data collection methods, namely interviews and FGDs. The participants (15 older adults) involved in the study encompass older adults with hypertension and their families, as well as healthcare providers and policymakers in the community.
The types of complaints often felt by the older adults in this study were related to the signs and symptoms of hypertension, such as dizziness or headaches, as well as complaints related to the aging process, such as visual function, musculoskeletal and hearing loss, or joint pain. Information related to physical problems is beneficial for the care of older adults. The older adults were often associated with various health complaints. It is mentioned that 78% of older adult respondents in their study experienced health problems mainly related to chronic diseases, such as eye problems, problems with the digestive tract, problems related to blood circulation, or metabolic disorders and 40% had symptomatic problems every day (Setiawan et al., 2017).
Older adults with hypertension often experienced emotions such as depression and anxiety (Ostir et al., 2006). Research in Indonesia showed that 24.9% of the older adults show depression symptoms (Madyaningrum et al., 2018). Previous study found an association between positive emotions and lower blood pressure in older Mexican American races (Ostir et al., 2006). Negative emotions such as depression or anxiety contribute to the etiologies of hypertension (Jonas et al., 1997). The emotional health aspects of the older adults must always be considered in the nonpharmacological treatment program of hypertension as part of additional therapy for patients with hypertension (Ostir et al., 2006). Hypertension is less common in individuals who do not experience anxiety, whether mild or severe, and nonpharmacological treatments such as foot massage effectively lower blood pressure in older adults with hypertension. Additionally, foot massage helps reduce anxiety levels (Anwar et al., 2022).
This study supports the findings of previous research, indicating that nearly half of the people with hypertension had limited knowledge about the condition (Sinuraya et al., 2017). This study may lead to low awareness about hypertension and its management (Hussain et al., 2016). Previous studies suggested that knowledge influences hypertension management (Yuliyana et al., 2018). Other studies have found that knowledge is correlated with hypertension complications and compliance in treating hypertension and blood pressure control (Kilic et al., 2016).
The older adults expressed difficulty making behavior changes. Behavior change was problematic because it involves many factors (Kilic et al., 2016). This condition was due to the need for more guidance from health workers. Similar to findings in previous studies, health workers need to adequately guide patients and their families in managing their health properly. Older adults noted that health officials often needed to provide more individualized healthcare tailored to their specific needs (Beverly et al., 2014).
This study found noncompliance with medication and frequent complaints often due to lack of family involvement in older adults’ daily care and problems among families (Costa & Nogueira, 2008; Gholamnejad et al., 2018; Parsa et al., 2018). Family support positively influences the behavior of older adults in controlling hypertension (Herlinah et al., 2013). Older adults also needed more support from health officials. Health workers were perceived as not listening to the complaints of older adults, not giving enough time for discussions, and having unfriendly facial expressions. These factors made older adults reluctant to visit the health center. This result supports previous studies (Setiawan et al., 2017).
Older adults reported that transportation as a barrier to accessing health services, such as no family members accompanying the older adults’ visitors to the health center, unfriendly public transportation for older adults, and the cost of transportation (Setyoadi et al., 2013). Besides the transportation problem, a physical limitation also contributed to the older adults to access health services (Madyaningrum et al., 2018).
This indicated that older adults need health services that are closer to their homes. This study identified five key needs for managing hypertension in older adults: education, social support, proficient health officials, improvement of the older adults’ integrated health post, and enhanced community health centers. Health education could improve an individual's skills in managing their health problems, while support was essential as it directly influences the success of hypertension management (Costa & Nogueira, 2008). The collaboration between doctors and trained nurses has been proven to reduce hospitalization, and improve blood pressure and lipid management in patients with coronary heart disease (Health Quality Ontario, 2013).
The older adults still engaged in risky behavior. Research in the older adults’ group in Pekanbaru found the older adults with uncontrolled hypertension was 52.6%. The factors contributing to uncontrolled hypertension were smoking, not routinely taking antihypertensive drugs, and high sodium consumption (Mitra & Wulandari, 2019). Another study found that older adults with hypertension tend to less exercise and low adherence to the hypertension diet and one of the studies show that there was increase in compliance level on the knowledge and psychomotor and family support (Sari et al., 2022; Usman et al., 2023). So, intervention in behavior modification was needed to help control blood pressure.
The older adults did not show compliance with hypertension medication (Mitra & Wulandari, 2019). Previous study stated that only 50% of chronic disease clients adhere to their treatment, and in cases of hypertension, noncompliance with medication is closely related to uncontrolled blood pressure and the emergence of complications from diseases such as stroke, myocardial infarction, heart failure, and death (Peacock & Krousel-Wood, 2017). An Indonesian study found that 74% of older adults in Indonesia use medicine without a prescription from a doctor.
Strengths and Limitations
This study can provide an understanding of the lives of older adults with noncommunicable diseases from their point of view and perspective of the problems and needs of older adults with hypertension in managing their health problems. Nevertheless, this study also has some limitations—first, older adults’ informants in Indonesia with low literacy made member checking unfeasible. Even though there is some debate about the effectiveness of member checking as a method of pursuing rigor in qualitative research (Morse, 2015), comparing the participant's answers with Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) logbooks from the intervention phase was expected to confirm the consistency of their answers. Nurses as educators for noncommunicable diseases must be aware of the needs of hypertensive patients to care for themselves. The skills of these nurses must be continuously improved.
Implications for Practice
This research can provide direct information for primary health facilities about managing hypertension in the older adults. In addition, this research is basic research to develop a model of advanced age nursing care with community-based hypertension. This research has implications for nursing services at community health centers, including the development of a collaborative role between healthcare professionals and the community. By utilizing supportive applications, this collaboration can strengthen information sharing, communication, motivation, and program evaluation.
Conclusions
In conclusion, the findings of this study highlight a range of significant problems and needs concerning the management of hypertension in older adults. It is crucial to consider these identified problems and needs when planning the management for older adults, aiming for controlled hypertension. Controlled hypertension, in turn, will delay the progression of the disease, ensuring that older adults do not suffer from complications associated with hypertension.
To build upon these insights, future research endeavors will focus on developing a Model of Community-Based Nursing Care. This model comprehensively addresses the identified issues and needs by integrating community resources and nursing care practices. Subsequently, a quasi-experimental research study involving older adults with hypertension will be conducted to assess the effectiveness of the proposed model in enhancing hypertension management outcomes among this demographic. These future endeavors represent crucial steps toward advancing our understanding and improving the overall care and support for older adults with hypertension.
Footnotes
Acknowledgment
The authors thank all informants in our study during the difficult period and local research assistants who supported us to collect the data.
Author Contributions
UK was involved in conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resource, validation, visualization, writing—original draft, and writing—review & editing; BAK in conceptualization, data curation, investigation, and project administration; YA in conceptualization, data curation, investigation, project administration, and validation; BB in data curation, validation, and visualization; and DWS in conceptualization, validation, resource visualization, writing—review & editing.
Consent for Publication
We have obtained participants’ consent for the publication of this study's results, ensuring that the personal data will not be included.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Study Approval Number
This study received ethical approval from the ethical Committee of the Faculty of Nursing University of Indonesia with number 41/UN2.F12.D/HKP.02.04/2018