
Abstract
Introduction
Newborn danger signs can lead to a high risk of morbidity and mortality without immediate medical interventions. Postnatal mothers are expected to identify these signs and seek appropriate medical care for their newborns where necessary. Cultural beliefs significantly impact how postnatal mothers seek healthcare for their newborns. These beliefs, rooted in traditions and often associated with evil spirits or reliance on traditional healing practices, have been observed across various cultures worldwide. The study explored cultural beliefs and health-seeking practices among postnatal mothers in the Bono East region of Ghana regarding newborn danger signs.
Methods
The study adopted the qualitative approach using a descriptive exploratory design. The study's theoretical framework was guided by the socioecological model by McLeroy et al.. Fifteen participants were selected using the purposive sampling technique. Data was collected by face-to-face interviews using a semistructured interview guide. With consent from participants, interviews were recorded and transcribed verbatim. The thematic analysis approach was employed to analyze the data.
Findings
The study revealed that, while participants were identified to have generally fair knowledge of newborn danger signs, beliefs in spiritual causes of newborn danger signs and use of readily available local remedies like fresh tomatoes and local gin for treating newborn conditions hindered proper health-seeking practice among postnatal mothers.
Conclusion
Findings of the study suggests recommendations for intensive, culturally sensitive health education campaigns at the community level and in the hospitals during antenatal and postnatal services to reduce the influence of cultural practices on newborn care.
Keywords
Background
Culture represents the shared views and practices within a society, where some customs or rituals variably impact maternal and child health outcomes (McLeroy et al., 1988). These beliefs and practices influence health-seeking behaviors, shaping the state of maternal and child health (Aynalem et al., 2023).
Across Africa, beliefs, and traditions place stakeholders and family heads as the experienced people who make decisions and provide education on newborn conditions often leading to delay in receiving effective care (Aubel, 2021; Birhanu & Mathibe-Neke, 2021). Furthermore, most communities in Ghana rely on various forms of treatment including herbal medicines, over the counter medication as well as using the services of traditional healers. It is believed that, the educational status of participants significantly influence their understanding of a good health seeking practice (Adongo et al., 2024).
A qualitative study by Kanton et al. (2023) in Ghana revealed that for diagnosing and treating neonatal danger signs, caregivers primarily used traditional or at-home herbal medicines, followed by pharmacies and hospitals. However, traditional herbal medicine used at home for treatment was most frequently selected by caretakers, which depended on the severity of these danger signs manifested in the neonate. In 2023, an estimated 2.3 million newborns died within their first month of life worldwide, which translates to about 6,300 neonatal deaths every day (United Nations Inter-agency Group for Child Mortality Estimation (UN IGME, 2023)). According to Getachew et al. (2022), improving maternal understanding of newborn dangers significantly reduces neonatal mortality as this knowledge guides mothers on when to take action, enabling them to apply appropriate life-saving techniques to avoid preventable newborn deaths.
The occurrence of Neonatal complications often poses challenges to the provision of care and the engagement of mothers in seeking care. These challenges are primarily attributed to disparities in cultural norms, logistical factors, and financial constraints (United Nations Inter-agency Group for Child Mortality Estimation (UN IGME, 2023)). According to Gyaase et al. (2024), the risk of developing neonatal danger signs in developing countries like Ghana is six times higher than in the developed countries.
According to the Ghana demographic and health survey report, Ghana recorded a neonatal mortality rate of 17 per 1000 live births in the year 2022 (Ghana Statistical Service (GSS & ICF, 2023)). Furthermore, mortality reports from the ministry of health Ghana, placed the Bono East region, which is the study setting as the fourth highest in terms of neonatal mortality with a neonatal mortality rate of 7.5 per 1000 live births out of 16 regions (Ministry of Health, 2022).
Traditional practices wield significant influence over health and healthcare utilization, particularly in rural areas, contributing to suboptimal and inconsistent utilization of maternal and child healthcare services (Abate et al., 2022). In communities where cultural and traditional beliefs in newborn illness are prevalent, such beliefs can cause a significant impact on health seeking practices. They often lead to poor seeking of appropriate medical care, reliance on traditional healers and the use of nonmedical remedies. These interventions can hinder early detection and treatment of potentially serious newborn conditions leading to increased newborn morbidity and mortality.
The extent to which mothers seek healthcare for their neonates depends significantly on their understanding of neonatal danger signs. When mothers possess accurate knowledge about the factors that can lead to neonatal mortality, including recognizing the warning signs, this knowledge becomes a vital tool in preventing many avoidable neonatal deaths (Yosef et al., 2020). This study thus, explored cultural beliefs and health-seeking practices among postnatal mothers regarding Newborn Danger Signs.
Review of Literature
Cultural beliefs rooted in traditions and often associated with evil spirits or reliance on traditional healing practices significantly impact how postnatal mothers seek healthcare for their newborns across various cultures worldwide (Jahan & Islam, 2022; Rent et al., 2022). Across the globe, cultural norms significantly influence vital areas of life including nutrition, education, and healthcare as well as child upbringing. In healthcare setting, culture plays a vital role in shaping health-related perceptions, decisions and attitudes of mothers toward seeking care (Nyaloko et al., 2023).Cultural influences often manifest through traditional knowledge and belief systems, spiritual practices and rituals which has been handed down across generations (Terentius Rugumisa, 2024).
In many African societies, including Ghana, it is commonly believed that, diseases may stem from both physical and spiritual causes which informs a widespread of consultation of traditional healers or herbalist, particularly when the illness is perceived to be spiritually induced (Adama et al., 2021). Cultural values therefore shape the health-seeking behaviors and influence postnatal mother's interaction with healthcare providers (Nyaloko et al., 2023). For instance, a qualitative study by Rent et al.,(2022) in Ghana revealed that, some families and caregivers initially sought care from spiritual or traditional healers and only resorted to professional healthcare services when complications arise. The use of traditional herbal medicine remains a longstanding and respected practice among African people with the belief that certain ailments are beyond medical intervention and require spiritual or traditional healing methods. Hence, these practices persist despite the increasing availability of healthcare services, reflecting the deep rooted cultural beliefs of the people (Adama et al., 2021).
Delay in seeking healthcare may contribute to severe maternal and child health outcomes. In Ghana, these cultural practices are still prevalent, hence the need for culturally sensitive approaches in healthcare delivery to ensure early detection and treatment of potentially serious newborn conditions. The purpose of the study therefore was to explore the cultural beliefs and health-seeking practices among postnatal mothers in the Bono East region of Ghana regarding newborn danger signs.
Methods
Research Design
The study adopted a qualitative approach using the exploratory descriptive research design (Elhami & Khoshnevisan, 2022). The study design was ideal because it provided a flexible and efficient method for interacting with participants about their experiences. This was done by relying on their own words and experiences with regard to beliefs and practices on newborn danger signs.
Study Setting
The research was carried out at the Holy Family Hospital, in Techiman within the Bono East region of Ghana. The Bono East region is one of the 16 regions of Ghana and the hospital serves as the only referral center for Newborn cases in the Bono East region. It also has the largest Neonatal Intensive Care Unit (NICU) in the region where all manner of specialist services are provided. The Holy Family Hospital is the largest amongst five hospitals in the municipality and the main referral point for other hospitals and health facilities within the municipality and region.
Research Question
The study was guided by the research question below:
In what ways do cultural beliefs and practices influence health-seeking behaviors of postnatal mothers regarding newborn danger signs?
Population and Sampling
The study initially recruited 20 participants who met the inclusion criteria through a purposive sampling technique (Campbell et al., 2020). Participants were recruited from the postnatal wards and NICU of the Holy Family Hospital in the Bono East Region which was known to the researchers. There was however no threat to power balance between the researchers and participants as the researchers had no prior contact with participants before data collection. However, data saturation was obtained by the fifteenth participant as no new information was identified to address our study's aims (Braun & Clarke, 2021a). The remaining postnatal mothers were discharged with an explanation from the principal researcher. The inclusion criteria for the study were postnatal mothers whose newborns had an ailment, which caused them to return to the hospital on admission to either the NICU or postnatal ward. However postnatal mothers who had an ailment and had newborns on admission were excluded from the study. Postnatal mothers with ailments were identified through their documented diagnosis at the postnatal wards where they were admitted. The participants were subsequently counseled with the rational for their exclusion from the study clearly explained, while reassurance was provided regarding continuity of care for both mothers and their babies.
Data Collection
Participants who met the inclusion criteria were interviewed face to face using a semistructured interview guide attached as Supplemental Appendix 1. The semistructured interview guide was developed through review of in-depth literature based on the objectives of the study. The guide covered key areas such as beliefs and practices as well as participants health seeking behavior toward the beliefs. The interviews were conducted by the principal researcher who had no prior contact with participants before the interviews were conducted. The principal researcher conducted the interviews due to her knowledge in midwifery and qualitative research. The entire process of data collection lasted from February to April 2024. The research instrument was piloted on two postnatal mothers who were not included in the study by the principal investigator before the commencement of the interview. This was done to ensure that the interview guide was suitable for the target participants. After the piloting, further review was done by all researchers to ensure accuracy of the interview guide. Research participants were identified with the help of the midwifery managers at the various wards. The aims, methods, advantages, and the potential risk of the study were explained to participants in the native language for easy understanding by the ward managers. Those who met the inclusion criteria were referred to the principal researcher for further engagements for the interview. Participants were assured of Privacy, anonymity and confidentiality during data collection to gain their trust and confidence in the study. Voluntary participation was also ensured, and the participants were informed about their right to participate in or withdraw from the interview, with the assurance that their decision will not impact the care provided to their babies at the facility. A quiet office was obtained at the hospital at convenience after their consent was sought and each interview lasted between 40 and 60 min per participant which was audio recorded. Field dairy was kept during data collection process by the principal researcher to record nonverbal cues from participants to ensure rich data. In order to familiarize with the data obtained, audio recordings were made available to all researchers.
Data Analysis
Data were analyzed concurrently with data collection using Braun and Clarke (2021a) thematic analysis approach. Themes were derived deductively with the aid of the data collection tool (semistructured interview guide, Supplemental Appendix 1). All interviews were transcribed verbatim, and each transcript was independently reviewed by two researchers to ensure thorough understanding of the content. However, some interviews which were conducted in Twi were translated into English by the principal researcher who is well vexed with the twi language as part of her primary spoken languages. Words without English translation were replaced with words closer in meaning. Initial codes were generated capturing significant features and patterns across datasets. These codes were then reviewed by all researchers across the entire dataset before progressing to the formation of themes and subthemes. Any discrepancies in coding or interpretation were further discussed among researchers to arrive at consensus. Upon confirmation by all authors the generated themes and subthemes were refined. Final report of findings was produced based on the themes and subthemes after further confirmation.
Methodological Rigor (Trustworthiness)
The authors adopted the Guba (1981) criteria to ensure trustworthiness of the study. These criteria, credibility, transferability, dependability, and confirmability, are essential for establishing rigor in qualitative research.
Credibility was maintained through sustained engagement with participants throughout the data collection process. Additionally, regular debriefing sessions by authors was ensured to discuss the research methodology and the data collection procedures.
Transferability was achieved through an in-depth description of the study design, participant selection, and data collection methods. Data saturation was also ensured to obtain rich data to aid transferability. Through an audit trail and construction of appropriate interview guide using probing questions dependability was ensured. To ensure confirmability, the authors ensured that findings obtained from the data collection were a true representation of data obtained from participants by making sure to carefully confirm findings.
Triangulation refers to the use of multiple methods, data sources, theories, or investigators to enhance the credibility, validity, and richness of a study's findings by establishing identifiable patterns (Stahl & King, 2020). Triangulation was carried out using participants’ primary data sources (such as in-depth interviews) and field notes which was obtained during data collection. These provided an insight into the subjective experiences, beliefs, and practices of the participants in the study.
Ethical Consideration
The study was approved by Institutional Review Board of the Christian Health Association of Ghana (CHAG) with IRB number CHAG-IRB02082023. The research department of Holy Family Hospital granted the approval to recruit postnatal mothers from the NICU and postnatal ward. The study's objectives, benefits, potential risks, and rewards were explained in detail to participants to obtain their consent. Verbal and written consent was obtained from participants before the commencement of the interview after assuring them of anonymity and confidentiality. Participants were informed about their right to participate in or withdraw from the interview, with the assurance that their decision will not impact the care provided to their babies at the facility. The study ensured anonymity by assigning participants with the pseudonyms “DS.”
Results
Data saturation was reached by the fifteenth participant. This occurred when no new information or data were obtained from participants in the qualitative study (Braun & Clarke, 2021b). All postnatal mothers who met the inclusion criteria were interviewed at the NICU and postnatal clinic of the Hospital and none of the participants withdrew from the study.
The age range of participants was between 22 to 43 years. This age bracket represents the reproductive age group where fertility is mostly achieved. The parity of participants ranged between paras 1 to 3. Among the 15 participants, their level of education ranged between Junior high school to tertiary. The ethnic background of participants varied from Bono, Waale, Mou, Dagaati, Sisaala to Busanga and the age of their babies ranged from 3 days to 1 month. This depicts the diversity of people who access care at the study setting. These sociodemographic information of participants has been indicated as Table 1.
Sociodemographic Characteristics of Participants.
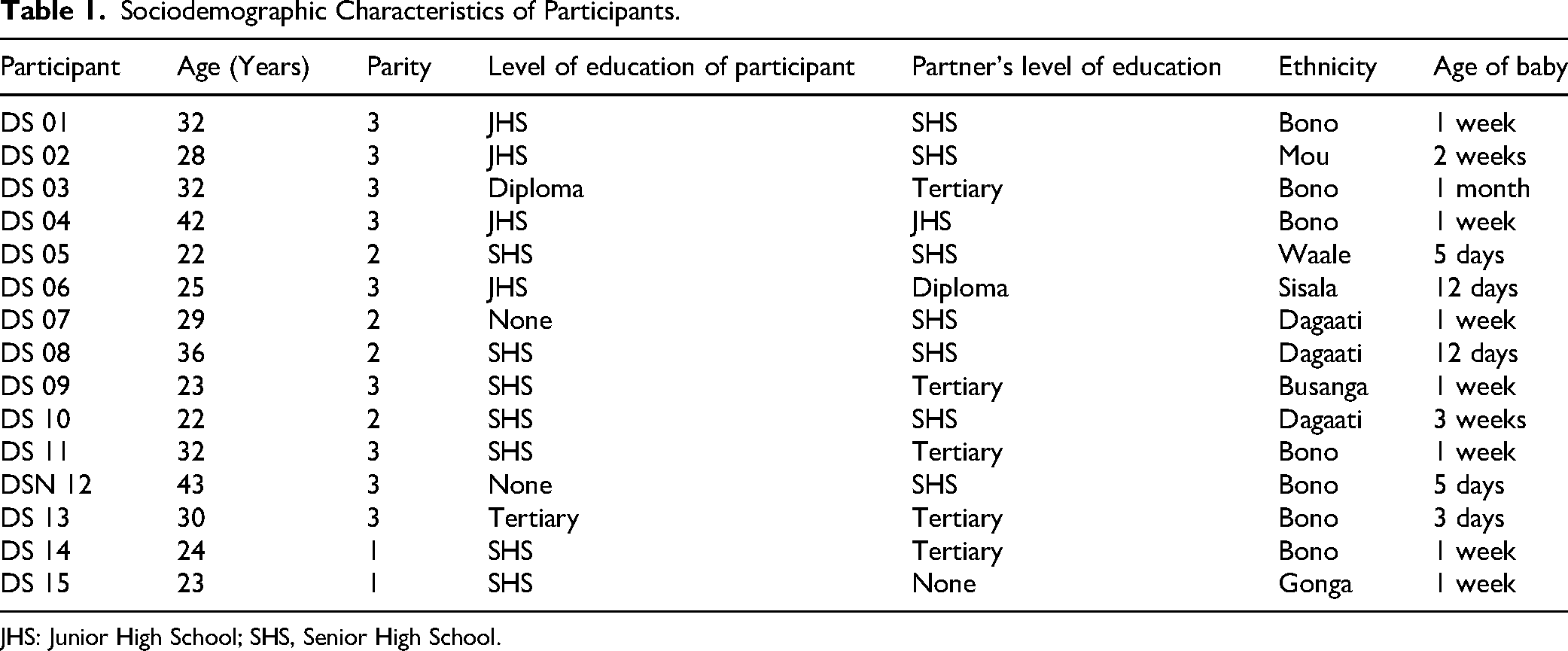
JHS: Junior High School; SHS, Senior High School.
Organization of Themes
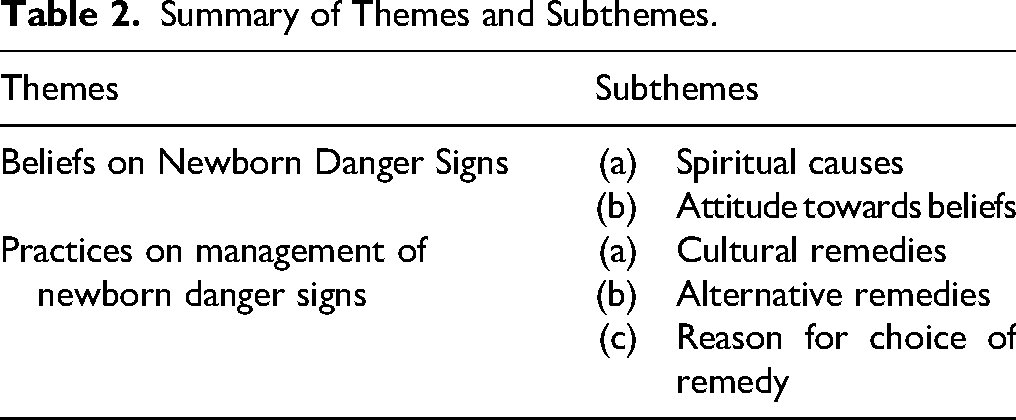
Two major themes and 5 subthemes emerged from the study from the analysis of data using the Braun and Clarke (2021a) approach. This is described in Table 2.
Summary of Themes and Subthemes.
Beliefs on Newborn Danger Signs
Cultural beliefs significantly influence how communities interpret the onset of illness in newborns, shaping the health-seeking practices that postnatal mothers adopt to restore their infants’ health. Each culture has its unique understanding of newborn illness. Despite the diverse ethnic and cultural backgrounds of the study participants, most shared similar belief systems regarding newborn illness.
Spiritual Causes
Many participants believed that newborn illnesses have spiritual causes and, therefore, cannot be effectively treated in a hospital setting. Some participants narrated how people with evil eyes can infect newborns with ill health and believed that, newborn condition like jaundice is caused by spirits.
One participant stated that “Oh yes some childhood illnesses are believed to be transferred by people with evil eyes. For example, some people use herbal preparations to prevent their babies from getting illnesses like ‘Asram,'(sepsis) but if these people come near your child, they can infect them with the condition. Some family members and friends even believe that the jaundice my baby is suffering is a spiritual illness.” (DS 04) “At home, some people are suspected of having evil eyes that can infect a child with disease. To protect your baby, you need to buy a dried chameleon from the market and make a bracelet out of it. When you put the chameleon bracelet on your baby's wrist, no one with evil eyes can infect her. If someone with an evil eye visits, you will see your baby changing color like the chameleon, preventing infection. Some people visit you after birth not out of love, but with the intention of infecting your child with diseases.” (DS 05)
The belief in higher powers and spirits as the cause of newborn illness signifies the deep rooted traditions and its influence on newborn care. From the above descriptions, it can be identified that postnatal mothers and their families consider newborns to be highly susceptible to spiritual threats which require culturally relevant protective actions. Recognizing and respecting these beliefs is essential to create an opportunity for a dialogue between health professionals and communities to develop strategies that integrate cultural practices with evidence-based care.
Attitude Toward Beliefs
Spiritual beliefs are deeply embedded in the traditions surrounding the care of a postnatal mothers and their babies after delivery. These traditional beliefs are often initiated by elders in the community and other significant caregivers. However, when postnatal mothers receive these suggestions, their attitudes towards these beliefs can significantly influence their responses and health-seeking behaviors regarding newborn danger signs.
Participant DS 05 expressed initial hesitation but gave in to the use of herbal preparation eventually. She had this to say “At first, I was completely against the cultural belief and the use of herbal preparations, I was hesitant to use the herbs as I thought it will cause complications to the baby. I didn’t believe that the herbs could heal my baby and wasn’t particularly worried about it, though I did think about it a lot. It wasn’t until I saw the results from using the herbs on my first child that I began to believe they really worked. My mother would boil the herbs and leave for the farm, asking me to bath the baby with them, but I wouldn’t do it. Sometimes she would get angry and throw the herbs away and I felt disturbed by my mother's anger.” (DS 05) “… from the mothers who visited me, everyone had suggestions. Some even said if I didn't follow their advice, I might lose my baby. Since I was a first-time mother, I was afraid and felt compelled to listen to them. Some even claimed that ‘Asram’ had accumulated in the baby's stomach, and if I didn't bath the baby with herbs and have him drink some, he might die.”
The above quotes indicated that, attitudes toward traditional practices are not static but are often influenced by personal experience, family influence, and emotional factors. How these traditional practices are often enforced or encouraged by elder family members demonstrated the strong cultural continuity and pressure younger generations may face to conform to traditional norms.
Practices on Management of Newborn Danger Signs
Community perceptions, interpretations, and responses to newborn illness are often influenced by cultural beliefs and practices passed down through generations. Participants often considered newborn illness to be an out-of-hospital condition, which is best managed through cultural remedies.
Cultural Remedies
In this study, many participants shared cultural remedies they believed to be more effective and quicker than hospital treatments. Some remedies identified in the study included; the use of local herbs, chameleon bracelets, use of fresh tomatoes on newborn skin as well as giving a local gin (akpeteshie) to the newborn baby to drink. These practices were based on the premise that, newborn illness had a spiritual background.
One participant, DS 04 explained how conditions like fever and skin infections can quickly be treated by cultural remedies like herbal preparations. She stated that Some people believed that the jaundice my baby is suffering from is a spiritual illness, and they suggested getting herbal treatment for her. They also say that if a child has a fever, bathing them with herbal preparation can heal them. She continued further by stating that For ‘Asram,’ which makes the baby unable to eat well, you need to use herbal treatment both for bathing and then give them some to drink to heal the condition. Additionally, there is another condition called ‘Ntose,’ a skin infection that cannot be cured by hospital treatment alone. To heal ‘Ntose,’ you must smear the child's body with tomatoes, which is believed to completely cure the condition. (DS 04) “I have also heard of ‘Asram,’ (sepsis) which is not considered a hospital illness. It appears as green veins on the baby's abdomen and skin. When a baby has this condition, you need to bath them with herbs to resolve it. There is also another condition called ‘Ntemkyem,’ (measles), a condition that causes rashes on the skin and inside the stomach. For this, you can smear the baby with local gin (‘akpeteshie’) and give them some to drink, this is believed to resolve the condition since it is not considered a hospital sickness.” (DS 09)
From the above, illnesses are not seen as treatable within the hospital setting, which reflects a fundamental difference in how illness causation and treatment are understood in traditional settings. The phenomenon of seeing some conditions as not treatable in the hospital reflects a lack of trust or perceived inadequacy of healthcare in addressing culturally defined illnesses. This belief can influence health-seeking behaviors, often leading caregivers to prioritize traditional treatments over orthodox medicine.
Alternative Remedies
Most alternative treatment measures indicated by participants were due to their beliefs for newborn danger signs and the common practices identified in the community they find themselves. Most recommended choice of treatment by participants ranged from herbal preparations, over the counter medications at pharmacies to hospital care.
Participant DS 05 believed that, herbal medications are the best remedy and shared that “Herbal preparations can work faster than hospital treatments. You may buy some medications as first aid which would not work, so herbal medications can serve as first aid. However, if the herbal medicine doesn’t heal the baby, you can then visit the hospital for treatment.” (DS 05) “When my father was alive, he would treat my babies with herbs for any ailment, so we didn’t need to go to the hospital. He had different herbs for every condition including ‘soro yare3’ (convulsion).But since he passed away, I prefer going to the hospital rather than using herbs or buying drugs from the drug store.” (DS 02)
The views of the participants above showed how traditional medicine functions as a primary alternative in the treatment of newborn conditions. This is because most herbal treatments are often available at home or from local providers and may be cheaper or more familiar to postnatal mothers. This offers the opportunities for healthcare systems to educate caregivers on warning signs requiring urgent care, and build trust.
Reason for Choice of Remedy
Participants provided a reason for their choice of remedy for newborn danger signs which overall affected their health seeking practice for newborn danger signs. Some reasons stated by participants included financial constraints, confidence in care givers, the type of care received from care providers among other things.
One participant believed that, hospital treatment saves a lot of cost as compared to pharmacy shops or other alternative treatments. She stated that “You know… [Smiles], not all pharmacy shops can be trusted. Some might prescribe the wrong medication, which can lead to complications and end up costing you a lot of money. But if you go straight to the hospital, you won’t have to spend that much in the first place.” (DS 11)
Another participant revealed that, her trust in the kind of care provided by health providers makes the hospital her first point of call before considering any other treatment options. She had this to say “I prefer to seek care at the hospital because they will investigate to determine what is wrong with the baby and provide appropriate help. I might not know exactly what is wrong with the baby and could end up buying drugs that don’t work and may even cause complications. My husband also prefers hospital treatment, he wouldn’t allow alternative treatments.” (DS 06)
The management of newborn danger signs typically involves a combination of cultural and orthodox remedies due to the strong influence of culture and traditions in our diverse society. These cultural practices are important in shaping the health-seeking behaviors of postnatal mothers and their families.
Discussion
Women's behaviors and attitudes during the postnatal period are influenced by personal beliefs and perspectives as well as sociocultural practices in the community (Jahan & Islam, 2022).
Spiritual Causes
The findings from the current study revealed the profound influence of cultural and spiritual beliefs on the health-seeking practices among postnatal mothers. Spiritual interpretation to newborn illness, such as the belief that conditions like jaundice, sepsis, and diarrhea have spiritual origins were prevalent among participants. The findings also revealed that, newborn illnesses can be caused by spiritual forces such as “evil eyes or spirits.” This is consistent with findings from various studies across different cultural environments. For instance, a study by Jahan and Islam (2022) in Bangladesh demonstrated that, new mothers and their babies who are considered vulnerable to evil spirits and evil eyes are made to stay inside to avoid contracting illness from evil spirits. Similarly, Rent et al. (2022) revealed that, in Ghana, healthcare providers described an ancient cultural belief where “evil eye” was seen as the cause of newborn illness and that, traditional healers or herbalists were seen to be better equipped to treat such conditions than the health practitioners. The phenomenon of “evil eyes” as a source of newborn illness in Ghana has been documented by Bell et al. (2020).
In Africa belief system in the supernatural elements are often considered as underlying causes of health issues in infants. Similar beliefs are also identified across regions in Ghana. Such spiritual perspectives can lead to a preference for nonmedical remedies and reliance on traditional healers rather than seeking orthodox medical care. This can delay seeking timely medical interventions thereby exacerbating the severity of newborn conditions. A similar belief system in line with the current study was identified by Joshi et al. (2023) in India where newborn illness was attributed to evil eye and various measures were used to cast off the evil eye from the baby.
Contrasting evidence from studies in other settings demonstrates the inconsistencies in the influence of spiritual beliefs on health seeking practices. Abate et al. (2022) and Sivalogan et al. (2023) revealed that even though traditional beliefs were identified as the cause of illness, it did not hinder health seeking for medical interventions as majority of participants sought medical interventions while few sought alternative treatment for their newborns. Similarly, the current findings contrast with a study by Tette et al. (2020) in Ghana where most caregivers avoided the use of home remedies before seeking professional care. Only a small number administered some form of home treatment including paracetamol before seeking care, even though they were aware of traditional beliefs. Mothers were likely to recognize danger signs as medical conditions requiring immediate hospital management rather than attributing to spiritual causes.
These contrasting findings suggest that, the influence of spiritual beliefs on health seeking practices can vary essentially depending on the effectiveness of health education programs and accessibility of health services. In areas where mothers had great exposure to health education and access to healthcare, spiritual beliefs may have less effect on newborn illness and heath seeking practices. Therefore health providers should collaborate with traditional healers and community leaders to enable an effective strategy to bridge the gap between traditional beliefs and modern healthcare practices.
Attitude Toward Beliefs
In examining the attitude of postnatal mothers toward traditional beliefs regarding newborn danger signs, it is important to recognize the different emotional responses and their impact on health seeking practices. The influence of social networks particularly family and community members played a vital role in shaping mother's attitudes and health-seeking behaviors. The study revealed that, the advice and pressure from elders and peers compelled mothers to adhere to traditional beliefs and practices even when they harbored doubts. The study suggests a response of negative attitude towards these beliefs based on attitudes of hesitation and desperation when confronted with traditional beliefs about newborn danger signs. Similar attitudes were reported in a study by Abdullah et al. (2021) in Bangladesh, where caregivers showed initial doubt toward traditional practices but further relied on advice from traditional healers before considering hospital care. Studies by Ani-Amponsah et al. (2023) and Kanton et al. (2023) revealed that, when it came to cultural beliefs and practices to newborn care, some participants indicated having no choice but to follow the family which they were married, though they were not happy with the treatment of choice for the neonates.
Unlike the findings of this study, findings from Ramamonjinirina et al. (2022) which contradict the finding indicated that majority of mothers sought hospital care as their first option when faced with newborn danger signs even when traditional beliefs existed. This suggests a more positive attitude toward medical care in their study area, promoting better health outcomes. The findings of the study suggest that, social approval and fear of social repercussions can override personal beliefs when seeking care for newborn danger signs.
Cultural Remedies
Cultural diversity is associated with different beliefs and practices which influence utilization of healthcare in the treatment of various conditions and disorders of the newborn in many settings of the world (Adongo et al., 2024).
One interesting key finding of this study is the strong preference for cultural remedies among participants over modern medicine. This was based on the belief that newborn illness had spiritual causes and thus, requires cultural remedies instead of modern treatment. Participants frequently cited local herbs and specific practices, such as chameleon bracelet to ward off evil spirits, use of fresh tomatoes for skin infections and application of local gin for conditions like measles as quicker and more effective remedies than hospital interventions. These findings are consistent with Rent et al. (2022) in Ghana who found cultural remedies such as tying of chameleon amulet to ward off evil spirits causing newborn infections. Similar study in Ghana by Kanton et al. (2023) also revealed the preference of home remedies using traditional herbs by caregivers as a preferred care seeking practice for newborn ailments. The findings from the study suggest a preference for cultural remedies based on spiritual beliefs for newborn illness to be predominant in most regions of Ghana. However, a previous study in India by Joshi et al. (2023) revealed similar findings to that of the current study where spiritual remedies such as spiritual incantations, oil for massaging the body, application of holy flame and giving holy water were considered effective for speedy recovery of newborn illness by warding off evil spirits from the baby. Similarly, a study in Ethiopia by Aynalem et al. (2023) also revealed that, reliance on traditional healers, attributing newborn illnesses to supernatural causes grounded in cultural beliefs, hindered prompt medical care for neonatal danger signs. Cultural remedies often hold deep significance within communities and are integrated into daily practices and beliefs. The perceived effectiveness of these remedies significantly suggest its continued use by mothers instead of seeking care for newborn ailments. These remedies may offer familiar and accessible alternative to modern medicine. Also remedies such as herbs and tomatoes are locally available resources. This further enhances the appeal of these remedies thereby making them not only culturally acceptable but also practical in everyday life in communities.
However, a previous study by Adongo et al. (2024) contradicts these findings as the use of modern medicine and health facilities were considered the preferred choice for most participants compared to traditional healers and herbal medicine. Similarly, studies by Cáceres et al. (2023) and Odwe et al. (2020) also revealed that, in the phase of traditional beliefs as the cause of newborn illness, most participants did not consider it as a barrier to seeking modern medical interventions for their newborn illness which is not in agreement with the findings of the current study. This indicates a shift in some areas toward modern medical care, even while cultural practices remain influential.
While the current findings reveal the efficacy and acceptance of cultural remedies by most communities, it also raises concerns about the potential risk of neglecting modern medical care particularly for serious newborn conditions that may require professional interventions. Balancing the need for traditional and modern healthcare approaches could lead to proper maternal and newborn health outcomes. This can be achieved by stakeholders in healthcare acknowledging cultural beliefs and finding ways to incorporate them into healthcare strategies. This can enhance trust and cooperation with the communities where such practices are predominant.
Alternative Remedies
Alternative remedies were also found to play a significant role in health-seeking practices among postnatal mothers. The study revealed that, health seeking behaviors are often influenced by cultural beliefs, maternal personal experiences with treatment regimen as well as access to health resources. The study also found a poor connection between the use of traditional remedies and modern health care practices. While some participants expressed a preference for herbal remedies, there was a notable reliance on hospital care when these herbal remedies fail. This reliance on traditional medicine aligns with findings from Kanton et al. (2023) who noted the use of herbal treatment and pharmaceutical medicine as the first line of action before turning to hospital interventions when herbal treatments failed. Similarly, a study in India by Joshi et al. (2023), demonstrated a reliance on home remedies as a first line of treatment by mothers before seeking medical care when symptoms worsen. Consistent with the current findings is a previous study by Rent et al. (2022) in Ghana, where health providers identified families to have consulted spiritual healers first and only sought care at the hospital when spiritual remedies failed.
This preference for alternative remedies is often driven by factors such as accessibility, cost, and cultural beliefs as well as knowledge on the severity of conditions. Many mothers may choose herbal treatments due to their familiarity and perceived safety. However, this approach suggests a delay in health seeking for appropriate medical interventions which may lead to increase in newborn mortality.
In contrast, a study conducted by Adongo et al. (2024) revealed an overall high patronage of health facilities as a first line of treatment as compared to traditional healers and home remedies. The outcome of the current findings is also contrary to the findings from Madagascar by Ramamonjinirina et al. (2022) who found majority of participants who experience neonatal danger signs to have sought care from health personnel immediately without considering other remedies.
The positive health-seeking practices of the participants were attributed to increase awareness of danger signs during pregnancy and postpartum periods as well as the educational level of women and their spouse.
Reasons for Choice of Remedy
The reasons behind the choice of remedies were also found to be influential in shaping health-seeking practices among postnatal mothers. Financial constraints were identified as a reason for opting for nonmedical remedies, while a lack of trust in the efficacy of treatments influenced the choice of hospital care. These findings are supported by Adongo et al. (2024), Dizoagl et al. (2025) and Yeboah et al. (2025) who identified efficacy of treatment and attitudes of health personal as barriers to the choice of remedy for newborn care in Ghana. A previous study by Kanton et al. (2023) in Ghana, in alignment with this study discovered that, few participants identified financial constraints as influencing the reason for their choice of health-seeking practice. Abdullah et al. (2021) posits that, inadequate knowledge of danger signs, perceived cultural beliefs, treatment cost and transport expenses as well as lack of decision making power by mothers are reasons for choice of remedy and health seeking among mothers in Bangladesh. Understanding these factors equips healthcare providers to effectively address barriers to healthcare accessibility. These findings emphasize the need for culturally tailored health education initiatives that integrate respect for traditional beliefs while promoting evidenced based neonatal care practices.
Strengths and Limitations of the Study
The interviews conducted in Twi were translated into English while ensuring accurate representation of participants’ views. No issues were encountered with researchers experience with the Twi language, however, for Twi words without direct English meanings, the most appropriate alternative terms were used to convey intended meaning after deliberation among the researchers.
Due to the limited time, the research could not capture healthcare givers perspective about beliefs and practices of newborn danger signs to provide a more in-depth view of the phenomena under study. The study was conducted solely in the Bono East Region, one of the 16 regions in Ghana, which limits the generalizability of the research findings.
Recommendations
Policy makers should prioritize improving media engagements and publications to provide culturally sensitive health education through community engagements to address and correct misconceptions associated with newborn conditions.
Health professionals should ensure that health education programs are tailored to respect the belief systems in the community while gently challenging and clearing misconceptions that may hinder prompt health-seeking practices.
Implication for Practice
The study highlights the need for nurses and midwives to intensify health education programs on newborn health through the use of social media platforms and radio shows. Additionally, providing pictorial checklist and protocols at health facilities can support effective education for women seeking care.
Conclusion
Spiritual beliefs about newborn danger signs significantly influence health-seeking behaviors, with many mothers attributing health issues to supernatural forces. Attitudes toward these beliefs seem to be negative, impacting the willingness to seek timely medical care. Cultural and alternative remedies are commonly used, but there is inconsistency in the preference for medical versus traditional treatments across different settings.
Reasons for choosing specific remedies often involved financial constraints and trust in treatment efficacy. By understanding and addressing these factors, healthcare providers and policymakers can develop strategies to improve outcomes for newborns health and support postnatal mothers in making informed decisions about newborn care.
Supplemental Material
sj-docx-1-son-10.1177_23779608251401820 - Supplemental material for Cultural Beliefs and Health-Seeking Practices Among Postnatal Mothers in Ghana, Bono East Region, Regarding Newborn Danger Signs
Supplemental material, sj-docx-1-son-10.1177_23779608251401820 for Cultural Beliefs and Health-Seeking Practices Among Postnatal Mothers in Ghana, Bono East Region, Regarding Newborn Danger Signs by Emma Annan, Evelyn Yeboah, Mary Ani-Amponsah, Jacqueline Gyapomaa Asibey and Raina Dizoagl in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608251401820 - Supplemental material for Cultural Beliefs and Health-Seeking Practices Among Postnatal Mothers in Ghana, Bono East Region, Regarding Newborn Danger Signs
Supplemental material, sj-doc-2-son-10.1177_23779608251401820 for Cultural Beliefs and Health-Seeking Practices Among Postnatal Mothers in Ghana, Bono East Region, Regarding Newborn Danger Signs by Emma Annan, Evelyn Yeboah, Mary Ani-Amponsah, Jacqueline Gyapomaa Asibey and Raina Dizoagl in SAGE Open Nursing
Footnotes
Acknowledgments
The authors thank all the postnatal mothers who participated in the study and the ward managers for dedicating their time to help with participant recruitment.
Ethics Statement
Ethical clearance was sought from Institutional Review Board of the Christian Health Association of Ghana (CHAG) with IRB number CHAG-IRB02082023.
Consent Statement
Verbal and written consent was obtained from participants before commencement of the data collection. They were assured of anonymity and confidentiality.
Author's Contributions
This study was designed by EY, EA, MAA, JA, and RD. Data was collected by EY and EA. Manuscript was written and reviewed by all authors. All authors read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the results of this study are available from the respective authors upon request. For data protection reasons
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.