
Abstract
Background
Ensuring good health and well-being for children requires a high quality of life (QOL). Sustainable development has led to the elimination of many chronic and epidemic diseases. QOL is a multifaceted system encompassing several dimensions, including social, physical, and psychological functioning, which has emerged as a necessary outcome for children with chronic disorders.
Objectives
This study aimed to understand QOL in Egyptian school-age children with type 1 diabetes mellitus (T1DM). It examined sociocultural, economic, and healthcare issues faced by these children, revealing unique determinants such as family dynamics and community perceptions in Egypt, which differ from global data.
Methods
A cross-sectional study was used at the Hospital of Health Insurance outpatient clinics in Banha, Egypt. A group of healthy peers was compared with another group from the outpatient clinic. 412 school children, ages 6 to 12 years, had T1DM, and 412 healthy peer groups with the same child age and gender, the researchers interviewed. Three tools were used: a demographic data sheet, a socioeconomic scale, and the Pediatric Quality of Life Inventory 4.0 Generic Core Scale.
Results
The mean age of children was 12.9 ± 3.2. More than 60% of diabetic children had uncontrolled blood glucose levels, and 60% had poor socioeconomic levels. Children with diabetes had a significantly lower QOL than healthy peers in all dimensions. For the duration of the disease, where emotional function from the QOL was only affected, males revealed significantly higher scores related to school functioning. Children with middle and high socioeconomic status showed a highly significant relationship to school, social, and total QOL.
Conclusion
T1DM had a negative effect on all QOL domains of the school children. The researchers recommended establishing protocols integrated between children's homes, schools, and health insurance hospitals and clinics for providing comprehensive health education.
Introduction
Significant progress has been made in recent years in promoting children's quality of life (QOL) (Buss et al., 2020). Around 146 countries or territories have achieved or are on track to achieve the Sustainable Development Goals for children over 6 years of age (Ma & Zhang, 2020). Moreover, we can increase awareness in our societies regarding the need for proper health and healthy lifestyles and people's right to QOL, especially for the most vulnerable groups, such as children (Moretti et al., 2025).
Diabetes is an epidemic disease that affects 282 million people globally and is expected to reach 482 million by 2036 (Fihla, 2022). It comes in two forms; Type 1 diabetes mellitus (T1DM), the most prevalent chronic condition in children, affects 1 in 500 to 650 children of all ages (Abushanab et al., 2023).
Four nations in the Middle East and North Africa have the highest prevalence of diabetes mellitus worldwide, namely Saudi Arabia, Bahrain, Egypt, and the United Arab Emirates (Al-Rifai et al., 2019). According to the International Diabetes Federation, it was reported that in Egypt, the incidence is 2/200,000 annually, while in Pakistan, it is 8/100,000 per year, and among children younger than adolescents, the frequency was 12.5% (Ogle et al., 2022).
By filling in a crucial research gap in the region, specifically in the Egyptian context, this study makes a substantial contribution to the body of knowledge on QOL among school-age children with T1DM. Current research frequently ignores the particular sociocultural, economic, and healthcare issues that children in low- to middle-income nations like Egypt face, even though it primarily focuses on Western populations or widely generalized pediatric cohorts (Bekele et al., 2022; Ferizi et al., 2018). This study looks at how QOL is affected by several factors, like the structure of the Egyptian educational system, cultural stigmas associated with chronic illnesses, and restricted access to insulin and monitoring devices. The study reveals unique QOL determinants, such as the impact of family dynamics and community perceptions in Egypt, that diverge from those found in other countries by comparing these findings to global data.
By offering empirical data on the QOL of school-age children with T1DM in a Middle Eastern setting, this study significantly adds to the body of existing literature. The study emphasizes the complex effects of type 1 diabetes on children's physical, emotional, social, and academic functioning by concentrating on a vulnerable pediatric population. The results highlight how important early and continuous psychosocial support is for managing and caring for diabetes. Furthermore, by pinpointing particular areas where interventions are required to enhance health-related QOL outcomes, the study provides insightful information for educators, legislators, and healthcare professionals. The findings form the basis for creating family-centered, culturally aware, and school-based initiatives that improve the lived experiences of kids with type 1 diabetes. Besides, this study supports the integration of holistic care approaches within pediatric diabetes services, contributing to both practice improvement and health policy development.
Review of the Literature
Type 1 diabetes is a chronic condition referred to as juvenile diabetes mellitus or insulin-dependent diabetes (Rom et al., 2019). In this condition, the pancreas is unable to create enough insulin or any at all. Many causes can lead to this condition, including autoimmune response, genetics, environmental triggers such as viruses, and dietary factors (Paschou et al., 2018).
The primary focus of comprehensive health care is on children's quality of survival from chronic illnesses (Murillo et al., 2017). To put it another way, QOL, which took into account children's everyday activities and general well-being, was a key indicator for treatment outcomes (Rosner & Roman-Urrestarazu, 2019). It could be used to assess how well the children's health is working concerning the influence of management policies.
Diabetes mellitus is the leading cause of hospitalization for children (Merino et al., 2019). Additionally, diabetes might lead to a rise in the frequency of parental work absences and children's absences from school. As a result, evaluating the QOL of children with diabetes and the variables that may impact it is crucial. To the best of our knowledge, no research study has been published that addresses the QOL for diabetic children's health in South Africa or Egypt. The country has the highest incidence of type 1 diabetes among schoolchildren, higher than both the Gulf region and the world. Hence, this study aimed to understand the understanding of QOL in Egyptian school-age children with T1DM. It examined sociocultural, economic, and healthcare issues faced by these children, revealing unique determinants such as family dynamics and community perceptions in Egypt, which differ from global data.
This study will answer the following research questions:
Do T1DM children experience a different quality of life compared to their healthy counterparts during school life? What are the factors affecting the quality of life for school-age children with T1DM?
Materials and Methods
Design
A quantitative, cross-sectional study was used. According to Polit and Beck (2020), a cross-sectional design is a cost-effective and practical method for assessing QOL in children with T1DM and a comparison group, avoiding prolonged follow-up and resource-intensive follow-up among children. It efficiently identifies associations between T1DM-related factors and QOL outcomes, providing a representative overview of the population's status.
Settings and Population
The Banha Hospital Health Insurance outpatient clinics in Banha City, Egypt, served as the study's site. In many areas, these clinics offer a range of health treatments to school-age children. Despite the acute issue, schoolchildren with type 1 diabetes were among those who presented to the diabetes outpatient clinic. In contrast, the matched healthy peers who were present at the health insurance hospital outpatient Banha at the ophthalmology clinic and who did not have any chronic disorders were asked about their health-related QOL. Thus, the comments from school-age children focused on leading healthy lives. Next, age and gender comparisons were made between the children with T1DM and their healthy classmates.
Participants in the purposeful sample included 412 school-age children (6–12 years old) of both sexes who had been diagnosed with type 1 diabetes for more than 2 years, as well as 412 healthy school-age friends. The researchers used the EPI-Info statistical program, version 7.2, to determine the appropriate sample size for this descriptive observational study. The sample size calculation was based on an anticipated prevalence of 50%, with a 95% confidence level, a 5% margin of error, and a study power of 80%. This estimation assumed a medium effect size, consistent with similar studies in the literature. The total population of interest was children diagnosed with T1DM for more than 2 years. Children with neurological disorders or those diagnosed with T1DM for less than 2 years were excluded from participation.
Instruments
A self-administered questionnaire composed of three parts was used. The first part was a sociodemographic data sheet that involved: the child's age, sex, birth order, duration of disease, and diabetes family history (if any). The second part is the scale used to assess socioeconomic status, which was originated by El-Tawab (2004). The socioeconomic scale includes four dimensions: educational level for the parent (8 items), parent's occupation (2 items), family lifestyle (3 items), and monthly income for the family (6 items). However, the researchers modified the income regarding the inflation rate and increased it to conform with present income by comparing the golden pound difference value from 2010 to 2024 and the inflation rate by the income scale. The income score was divided into three categories: 85% to 100% (high), 60% to 84% (moderate), and less than 60% was accounted as low income. Modifications were assessed by five pediatric nursing professors and the validity of the content at 0.89. Besides, the Cronbach α was 0.90 which indicates a good internal consistency.
The third part was the Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Scales that were used for school-age children from 6 to 12 years to assess QOL, it is composed of 23 items originated by Petersen et al. (2009). The scale is composed of four dimensions, namely physical functioning (8 items), emotional functioning (5 items), social functioning (5 items), and school functioning (5 items). Each item is rated on a 5-point Likert scale (0 = never, 4 = almost always). Scores are transformed into a 0 to 100 scale. The higher scores indicated a better QOL. To create Scale Scores, the mean is computerized to sum the items over the number of items. To create a psychosocial health summary score, the mean is computerized to sum the items over the number of items in the emotional, social, and school functioning scales, that is give the total scale score, then the mean is computerized to sum all the items over the number of items on all the scales.
Several studies reported a good Cronbach α = 0.88 (Amedro et al., 2021; Hadianfard et al., 2021).
Additionally, Alfaleh et al. (2023) found that the Arabic version of the scale is practical, valid, and trustworthy for application in a variety of healthy settings for school-age children aged 6 to 12 and their parents. PedsQL was finished in fifteen minutes.
Data Collection Procedure
This study was conducted over 11 months, from October 2023 to August 2024. Data collection involved two main stages: clinical data retrieval and questionnaire administration. During routine follow-up clinic visits, each participant was interviewed individually by the researchers in a private setting while they waited for their appointments. After obtaining verbal and written informed consent, the researchers administered the structured questionnaire directly through face-to-face interviews, ensuring consistency in data collection. To assess glycemic control over the preceding three months, the most recent HbA1c values were retrieved from participants’ medical records at the time of data collection. HbA1c levels were categorized as “managed” if the value was less than 7.5% and “uncontrolled” if it was equal to or greater than 7.5%.
Ethical Considerations
The researchers obtained ethical approval from the Institutional Review Board (IRB) of the Faculty of Nursing at South Valley University, Egypt. Official permission was also secured from the manager of the hospital health insurance in Banha, Egypt. Participation in the study was voluntary, and all participants were assured of confidentiality. Written informed consent was obtained from the parents of each child participant, along with the child's assent for those older than seven years. To ensure privacy and data confidentiality, all data were anonymized using unique codes, and identifying information was removed before analysis. Data were securely stored in password-protected files accessible only to the research team and will be retained for a limited period as per ethical guidelines before being permanently deleted.
Statistical Analysis
The Statistical Package for Social Science version 19 was utilized to analyze the data. Data were checked for missing values and outliers. Missing data were assessed for randomness, and cases with substantial missing information were excluded from the analysis. For items with minimal missing responses, pairwise deletion was applied to preserve as much data as possible without compromising the integrity of the results. Outliers were identified through standardized z-scores and reviewed for accuracy prior to inclusion in the analysis. Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to describe demographics. Chi-square has been used for the comparison between the qualitative variables. Inferential statistics of analysis of variance (ANOVA) was used to compare the means of different groups. The P value of <.05 was considered statistically significant.
Results
Sociodemographic Characteristics of Participants
A total of 412 school-age children were recruited in the current study. More than half of the participants were male, 52.9%. The average age of participants was M = 12.9 ± 3.2 years. Nearly fifty percent, 48.3%, of the studied group were second- or third-child birth order. About 60.2% were classified as low socioeconomic level. More than half of the children (52%) were diagnosed with DM for more than 5 years. Moreover, 62% of the studied group had uncontrolled glycemic levels (Table 1).
Distribution of the Studied Group with T1DM According to Their Sociodemographic Data.

Notes: N = number, % = Frequency, yrs. = Years.
Differences Between Groups Based on Sociodemographic Data and Quality-of-Life Items
The distribution of males and females is nearly identical in both the studied group and the healthy group (47.1% females vs. 52.9% males in both groups). The Chi-squared test (χ2 = 0, P = 1.00) indicates that sex distribution is the same in both groups, meaning there is no statistical difference.
The studied group has an average age of 13.5 ± 3.4 years, while the healthy group has an average of 12.9 ± 3.2 years. Independent sample t-test (t = 0.79, P = .4) suggests that the difference in age between the two groups is not statistically significant. Besides, QOL dimensions were assessed, which revealed that the average physical well-being among the studied group was (M = 64.6 ± 18.8) versus (M = 90.8 ± 7.1) among healthy groups. The difference is statistically significant (P < .0001), suggesting that the studied group has much lower physical well-being compared to the healthy group. Additionally, it was revealed that the average score of the emotional well-being dimension was (M = 78.3 ± 18.8) among the studied group, whereas it reached (M = 95.6 ± 5.1) among the healthy group. The significant difference (P < .0001) indicates worse emotional well-being in the studied group. To sum up, significant differences were found in sex and age distribution between the two groups. The studied group shows a significantly lower QOL across all measured domains (physical, emotional, social, school, and total QOL compared to the healthy group. For more details, see Table 2.
Comparison Between the Studied Group and the Healthy Group Related to Sociodemographic Data and Quality of Life Items.

QOL Items Based on the Sociodemographic Data of the Studied Children With T1DM
The results revealed that emotional well-being is significantly lower in females (M = 62.6 ± 19.2) compared to males (M = 66.3 ± 18.3) with a P-value of P = .04. No significant differences between males and females in other QOL domains (physical, social, school, and psychosocial aspects. No significant differences were found in any QOL domains between the two age groups (6–9 years vs. 9–12 years), with all P-values of >.05, indicating no statistically meaningful age-related differences in QOL. Additionally, emotional well-being is significantly lower in children with a disease duration of
QOL Items Regarding Their Sociodemographic Data of the Studied Children With T1DM.
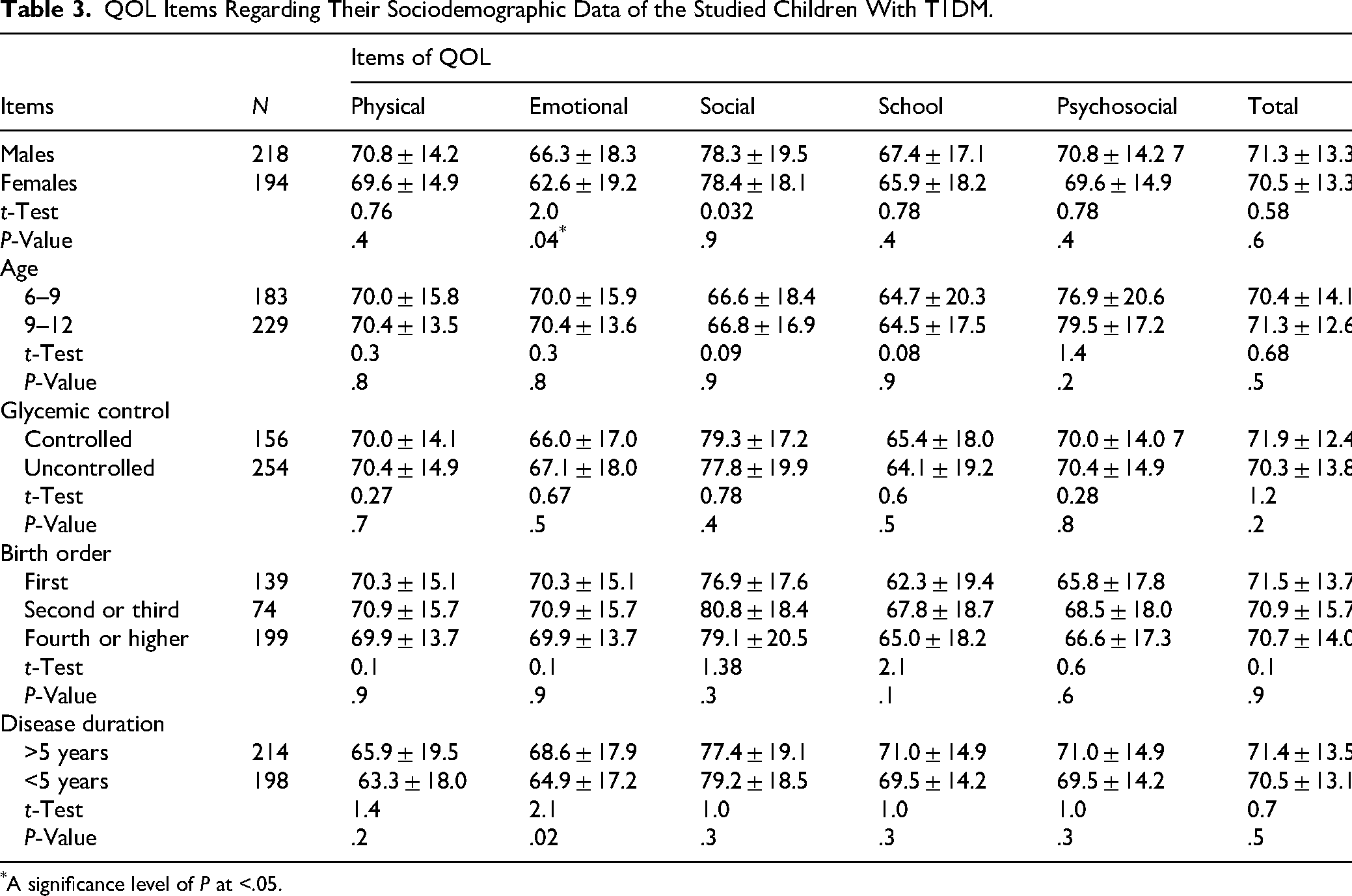
A significance level of P at <.05.
QOL Items Based on the Sociodemographic Data of Children's Families With T1DM
Independent sample t-test and ANOVA were utilized to assess the mean differences in the items of QOL based on the sociodemographic data of the child's family. The results indicated that social well-being is significantly lower in the low socioeconomic group (M = 62.1 ± 17.6) compared to the moderate (M = 67.5 ± 20.0) and high (M = 69.5 ± 19.8) socioeconomic groups, with a significant P-value of P = .004. Besides, school-related well-being is also significantly lower in the low socioeconomic group (M = 76.3 ± 18.7) compared to the moderate (M = 81.2 ± 17.4) and high (M = 81.6 ± 20.6) groups, with a P-value of .03. Total QOL is significantly lower in the low socioeconomic group (M = 69.4 ± 12.9) compared to the moderate (M = 72.7 ± 13.3) and high (M = 74.3 ± 14.0) groups with a P value of .01. Other QOL domains (physical, emotional, and psychosocial well-being) show no statistically significant differences and better scores in higher socioeconomic groups (Table 4).
QOL Items Regarding Sociodemographic Data of Children's Family T1DM.

A significance level of P < .05.
Discussion
In this study, school-age children with T1DM had their QOL evaluated, and the effects of several clinical and demographic factors were investigated. According to the results, children with type 1 diabetes have a substantially lower QOL than their healthy peers, especially when it comes to their physical and mental health. It was shown that several variables, such as sex, socioeconomic level, and length of illness, affected QOL scores. These findings offer crucial information for legislators, educators, and healthcare professionals.
In the current study, T1DM children have poor QOL items in all dimensions, including emotional, physical, social, and academic achievement. While highly statistically significant differences between T1DM children compared by healthy group peers at (P < .0001) for all items. These findings were similarly found in a study performed by Bekele et al. (2022) and Alhaddad et al. (2023), who reported that the children with chronic disorders, had poor progress toward QOL items, compared with the healthy group. Moreover, the children with T1DM had a negative QOL compared with healthy peer children (Al Alwan et al., 2022).
Compared to the health group, children with T1DM showed noticeably worse physical health. This result is consistent with a study performed by Khemakhem et al. (2020) who found everyday obstacles from frequent glucose testing, insulin administration, and dietary limitations which could lower levels of physical activity and negatively impact perceptions of general health. Additionally, changes in blood glucose levels can cause physical symptoms like fatigue that worsen their QOL.
Furthermore, children with T1DM also showed significant effects on psychosocial well-being, which includes emotional, social, and school-related experiences. These children expressed more emotional discomfort, which could be related to their fear of hypoglycemia episodes and the anxiety that comes with managing their illness. Furthermore, social well-being scores were lower, which could be related to limitations on peer participation or feelings of loneliness. These findings were consistent with studies performed by Al Shaikh et al. (2020), who reported that diabetic children had QOL than control children. The QOL items are negative for school and emotional items. However, there was no statistical difference between the physical and social QOL scale within the studied and control groups.
The study found that emotional well-being was significantly lower in females compared to males, suggesting that females with T1DM may be more vulnerable to emotional distress. This result is consistent with a study performed by Alshahrani et al. (2024) indicating that females often experience higher levels of anxiety and depression related to chronic illnesses. This may be due to greater self-awareness and societal expectations regarding body image and health. Therefore, targeted mental health interventions, particularly for female patients, should be considered as part of diabetes care programs.
Furthermore, concerning physical function, the majority of diabetic children had no statistically significant difference from the healthy group, due to changes in growth that occur in school children, differences in caloric intake with rapid growth, and participation in sports, all of which contribute to the poor physical QOL scores between children with T1DM. This finding was in line with a study performed by Lim and Stewart (2017) who stated that children with diabetes, in particular girls, were found to be less active than those without the condition.
In the current study, it was reported that socioeconomic factors played a significant role in QOL outcomes, with children from lower-income families reporting lower social and school-related well-being. The financial burden of diabetes management, including the cost of insulin, glucose monitoring devices, and specialized diets, can create stress for families and limit access to optimal care. Additionally, children from lower-income households may face educational challenges due to increased school absences related to diabetes management. These findings were consistent with studies performed by Noueiri and Nassif (2018) and Siddiqui et al. (2017) who revealed that socioeconomic status predicts poor HR QOL scores. These findings reinforce the need for policy interventions aimed at ensuring equitable access to diabetes care and school-based support programs for children with T1DM.
In this study, most children with diabetes suffer from several problems, such as emotional problems, more than control groups, and this may be due to the severe stress they are exposed to due to the chronic disease and the high financial costs of medical treatments, which is reported by Aljawarneh et al. (2023). The involvement of children with diabetes in the disease and its complications or other chronic diseases, and their lack of independence may be responsible for the decreased emotional QOL.
The current study reported that children with a shorter duration of diabetes (<5 years) had significantly lower emotional well-being compared to those with a longer disease duration (>5 years). This may suggest that the initial years following diagnosis are the most challenging, as children and their families adjust to the new lifestyle demands of diabetes management. Over time, coping mechanisms and adaptation strategies may develop, leading to improved emotional resilience. These findings were consistent with studies performed by de Wit et al. (2022) and Puri et al. (2013) who concluded that numerous psychological and cognitive issues were shown to be more common in children who were recently diagnosed, older at onset, had lower maternal educational attainment, had elevated HbA1c, or came from lower socioeconomic backgrounds. These results emphasize the importance of early psychological counseling and structured diabetes education programs to support newly diagnosed children.
The social aspects of the QOL scale in the current study are positively impacted by a family history of diabetes, but the school aspects are negatively impacted. Poor educational domains may be characterized by negative school absenteeism, but the social elements may be the best because of less psychological stress and the greatest coping mechanisms with the condition among children with a family history of diabetes for one or more parents. This finding was consistent with a study conducted by Alfaleh et al. (2023) who revealed that school children with lower HbA1c levels and regular blood glucose monitoring have better QOL with diabetes symptoms, despite guardians’ dissatisfaction with current diabetes management in schools.
Strengths and Limitations
The study focused on school-age children with T1DM, a vulnerable population. It assesses QOL, providing valuable patient-reported outcomes and psychosocial impact. Validated instruments enhance reliability and comparability. Besides, this study offers baseline data for future research and supports well-being strategies. However, the study has many limitations despite its significant contributions. The ability to prove a causal relationship between T1DM and QOL outcomes is limited by the cross-sectional methodology. Future longitudinal research could pinpoint important intervention points and offer deeper insights into how QOL changes over time. Self-reported measurements were also used in the study, which raises the possibility of response bias. A more thorough knowledge of the lived experiences of children with T1DM may be possible with more studies that integrate objective health indicators and qualitative data.
Clinical Implications
Significant ramifications for nursing practice and healthcare policy result from this study's findings. In the continuous care of children with T1DM, nurses are essential, and knowing what affects their QOL allows for more individualized, comprehensive treatment. Regular QOL assessments, for instance, can be incorporated into follow-ups to help nurses detect children who could be experiencing emotional or social difficulties in addition to medical ones. According to the study, school-based diabetic support programs are also necessary, and nurses can work with educators to develop and implement these programs. Furthermore, the findings highlight the significance of including psychosocial support services into pediatric diabetes care protocols at the policy level, guaranteeing that interventions go beyond glucose control to target children's overall well-being. More child-centered care and better long-term results may result from these useful applications.
Regular diabetes care should include mental health assistance, especially for children who have just received a diagnosis. Peer support groups and diabetes education programs are two examples of school-based interventions that may lessen the detrimental effects of T1DM on social and academic experiences. To guarantee equitable care and improved QOL outcomes for all children with T1DM, governments should also concentrate on expanding lower-income families’ access to diabetes resources.
Conclusion
In conclusion, this study emphasizes how T1DM significantly affects school-age children's QOL, especially in the areas of physical and mental health. Children from lower socioeconomic backgrounds may need additional social and academic support. Besides, children with diabetes experience poorer physical and psychosocial well-being, highlighting the need for comprehensive care that includes psychological support. The length of the illness, sex, and socioeconomic status were identified as the main determining factors. To improve the general well-being of children with T1DM, our results highlight the necessity of a multidisciplinary approach to diabetes care that includes social, psychological, and medical support networks.
Supplemental Material
sj-pdf-1-son-10.1177_23779608251369588 - Supplemental material for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study
Supplemental material, sj-pdf-1-son-10.1177_23779608251369588 for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study by Amira Adel Mohammed, Roqia Saleem Awad Maabreh, Mahmoud H. Alrabab’a, Anwar M. Eyadat and Salam Bani Hani in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608251369588 - Supplemental material for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study
Supplemental material, sj-pdf-2-son-10.1177_23779608251369588 for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study by Amira Adel Mohammed, Roqia Saleem Awad Maabreh, Mahmoud H. Alrabab’a, Anwar M. Eyadat and Salam Bani Hani in SAGE Open Nursing
Supplemental Material
sj-doc-3-son-10.1177_23779608251369588 - Supplemental material for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study
Supplemental material, sj-doc-3-son-10.1177_23779608251369588 for Quality of Life Among School-Age Children With Type 1 Diabetes Mellitus: A Cross-Sectional Study by Amira Adel Mohammed, Roqia Saleem Awad Maabreh, Mahmoud H. Alrabab’a, Anwar M. Eyadat and Salam Bani Hani in SAGE Open Nursing
Footnotes
Acknowledgments
The authors extend their appreciation to Health Insurance Hospital, Banha, Egypt.
Ethical Statement
The ethical approvals were obtained from the institutional review board (IRB) committee of the Faculty of Nursing of South Valley University, Egypt. This was followed by obtaining ethical approval from a selected hospital, after obtaining approval from the MOH for this hospital to participate in the study (2024/144). All methods in this study were carried out under the institutional research committee's ethical standards, as well as the Helsinki Statement and its subsequent revisions or similar ethical standards. Written informed consent was obtained from all participants.
Authors’ Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data that were analyzed during this study are directed to the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.