
Abstract
Mothers frequently fulfill the role of primary caregiver for children diagnosed with type 1 diabetes mellitus (T1DM). A T1DM diagnosis has a significant impact on the child and the wider family unit. The objective is to develop understanding of mothers’ experiences caring for children diagnosed with T1DM in the cultural context of the Middle East to facilitate enhanced health service provision and support. This study used a qualitative design. Data were collected in individual semistructured interviews. Participants were mothers of Arabic descent and Muslim belief who had a child diagnosed with T1DM within the last 12 months. All mothers were registered at the health service where this research was conducted and resident in the United Arab Emirates at the time of this study. COREQ guidelines informed reporting of the research and findings. Participating mothers described initial reactions of shock and disbelief, followed by transition to near ordinary and near normal (85% normal) family functioning. Family, culture, and faith emerged as critical supports in the whirlwind daily challenge of balancing the multiple demands and competing needs of the newly diagnosed child and the broader family. This study is the first of its kind from countries comprising the Gulf Cooperation Council. The findings provide insight into the challenges and support needs of mothers caring for children newly diagnosed with T1DM in an Arab Muslim context. The findings also provide a basis for enhancing health service support and suggest themes to inform further research.
Introduction/Background
Type 1 diabetes mellitus (T1DM) is a chronic disease requiring complex daily management. The impact of a T1DM diagnosis on a child and their family is substantial. The International Diabetes Federation (IDF) Atlas (8th edition) estimates that there are 1,106,500 children globally with T1DM (International Diabetes Federation, 2017). In the six Middle Eastern countries comprising the Gulf Cooperation Council (GCC), the absence of accurate data sets makes it difficult to quantify the current prevalence of T1DM among the region’s indigenous and expatriate populations (Sarant, 2014). However, the IDF Atlas estimates 175,800 children (aged 0–19 years) in the Middle East and North Africa Region have T1DM, with 0.43 per 1,000 people being in the United Arab Emirates (UAE; International Diabetes Federation, 2017).
T1DM is an autoimmune disease where the body’s own immune system attacks and destroys the insulin-producing beta cells in the pancreas. A child may be diagnosed with T1DM within the first few months of life. However, the majority (>85%) are diagnosed before the age of 20 with a marked peak in diagnosis between the ages of 10 and 14 (Frese & Sandholzer, 2013). Twenty-five percent of those with T1DM are diagnosed as young adults or adults (Maahs, West, Lawrence, & Mayer-Davis, 2010). Management of T1DM requires lifelong insulin replacement therapy via an insulin pump or subcutaneous injection multiple times a day (Brinkman, 2017). If not managed correctly, long-term complications include retinopathy, neuropathy, cardiovascular disease, foot damage, and kidney difficulties (Brinkman, 2017). Problems with thyroid function are also associated with T1DM (Brinkman, 2017).
Review of Literature
T1DM diagnosis has widespread implications for both child and family. Many studies have described the experiences of parents and families caring for a child with T1DM. Parents in the Netherlands reported feeling overwhelmed as they sought to accept a diagnosis of T1DM and learn the complicated skills and routines required (Boogerd, Maas-van Schaaijk, Noordam, Marks, & Verhaak, 2015). Management of T1DM confronts parents with dynamic and ongoing processes that are both complex and difficulty to master. A group of American parents whose children had been diagnosed between 4 and 11 years prior to being interviewed reported still struggling to master the fluctuations of T1DM (Smaldone & Ritholz, 2011). In contrast, Welsh parents, whose children had lived with T1DM for 7 to 10 years felt that they had mastered the daily management required; however, grief, guilt, and anger continues to emerge at times (Bowes, Lowes, Warner, & Gregory, 2009). For parents in Winnipeg, life with T1DM was described as seeking to achieve balance between protecting their child and enabling the child to “be like everyone else” (Nurmi & Stieber-Roger, 2012, p. 530). This pursuit for normality was also described by English parents and children living with T1DM. Although T1DM results in disruption, change, and adapting to “a potentially life-threatening illness,” each person endeavored to achieve a “normal life” (Marshall, Carter, Rose, & Brotherton, 2009, p. 1709). Swedish families interviewed 1 year after their child was diagnosed with T1DM spoke of life as “ordinary yet different,” particularly disrupted at times when blood sugar levels fluctuated with a negative impact on the whole family (Wennick & Hallström, 2007, p. 299).
The qualitative findings in the papers reviewed above present a picture of caregiving that is relentless and physically, psychologically, and emotionally burdensome. Polish researchers administered the Caregiver’s Burden Scale (Macera, Eaker, Jannarone, Davis, & Stoskopf, 1993) to identify specific factors that affected the level of burden of caregivers experienced by parents of children with T1DM (Kobos & Imiela, 2015). Overburdening was associated with factors such as being the sole caregiver, isolation, lower educational level, and economic status. Caregiver burden has been identified as multidimensional phenomena, subject to change and influenced by factors such as characteristics of the caregiver, the demands required, and the level of involvement required (Chou, 2000). Chou’s Model of the Caregiver Burden defines burden as “an individual’s subjective perception of overload in one or more perspectives: physical, psychological, social and financial” (p. 405). Caregiver burden has become a widely researched outcome largely measured by quantitative measures. However, Bastawrous (2013) urges against a reliance on such measures and recommends the inclusion of qualitative data to “capture important contextual elements of the caregiving experience” (p. 432).
Most studies describing family or parental experiences of caring for a child with T1DM were conducted in Western settings, including the United Kingdom (Marshall et al., 2009; Rankin et al., 2014), United States (Rearick, Sullivan-Bolyai, Bova, & Knafl, 2011; Rechenberg, Grey, & Sadler, 2017; Smaldone & Ritholz, 2011; Whittemore, Jaser, Chao, Jang, & Grey, 2012), and Australia (Thorsteinsson, Loi, & Rayner, 2017). In some countries, a young child’s mother becomes the primary person responsible for disease management until the child develops the maturity and capacity to self-manage (da Cruz, Collet, de Anrade, da Nobrega, & da Nobreg, 2017; Kobos & Imelia, 2015). However, studies focused specifically on mothers’ perceptions, experiences, and the impact of having a child diagnosed with T1DM are limited (Abolhassani, Babaee, & Eghbali, 2018; Khandan, Abazari, Tirgari, & Cheraghi, 2018; Rechenberg et al., 2017; Thorsteinsson et al., 2017).
No studies focused on mothers’ experiences of T1DM have been conducted in the GCC region. Although two studies from Iran (Abolhassani et al., 2018; Khandan et al., 2018) examined the experiences of mothers caring for children with T1DM, there are significant cultural, language, and contextual differences between Iran (where the primary language is Persian) and Arabic-speaking UAE. The study reported here reflects the desire of specialist T1DM health service providers in the UAE’s largest Emirate (Abu Dhabi) to better understand the needs of mothers in caring for a child during the first 12 months of T1DM diagnosis. Improved understanding in this area will support enhanced service provision. The purpose of this study of qualitative case insights was to elicit in-depth understanding of UAE mothers’ perspectives and experiences of having a child diagnosed with T1DM. It also aimed to identify the role of family, community, and culture during the first months after diagnosis and clarify the role the health-care team play during this period.
Methods
This study used a case-based qualitative descriptive design to explore the perspectives and experiences of mothers whose child had been diagnosed with T1DM. Mothers’ perspectives and experiences were captured in semistructured interviews.
Recruitment
Participants were purposively sampled through the T1DM mothers’ support group at Sheikh Khalifa Medical City (SKMC), Abu Dhabi. One of the present researchers was responsible for participant recruitment based on specific inclusion criteria. Potential participants were telephoned and invited to participate in the study. Participation rates were low. This was attributed to the heavy time demands on mothers arising from looking after a child with T1DM plus broader family responsibilities, and the inclusion criterion focused on new diagnosis. Five mothers consented to participate. However, one interview was excluded from the analysis because the audio file had not recorded correctly and was incoherent.
Inclusion Criteria
Mothers of Arabic descent and Muslim belief resident in the UAE at the time of the study, who were registered at SKMC with a child newly diagnosed with T1DM (within the last 12 months).
Ethical Considerations
This study was approved by the SKMC Institutional Research and Ethics Committee (REC-10.06.2014: RS-302). SKMC is a major health service provider in the Abu Dhabi Government Health Services Network. All participants provided informed consent to participate in this study.
Sample
Study Participants.

T1DM = type 1 diabetes mellitus; T2DM = type 2 diabetes mellitus.
Data Collection
This study was conducted at SKMC in Abu Dhabi, UAE, in 2015. Participants completed 45- to 60-minute individual interviews at the SKMC diabetes clinic. Conversational questions were used to guide the semistructured interviews (Online Appendix 1). Before commencing each interview, the purpose of the interview was explained to participants (in Arabic). An interview sheet was provided for each participant in their own language (Arabic). Participants were informed that they could withdraw from the study at any time, and confidentiality was emphasized. Researchers obtained permission to record the interview, and participants completed signed consent forms. Interviews were conducted in Arabic by the Arabic speaking research team member, supported by another (non-Arabic speaking) researcher.
Data Analysis
Yin’s (2010) five phases of analysis provided the conceptual framework for the data analysis. Information for analysis comprised audio files from the four Arabic transcripts of interviews included in the analysis, the English translation of each interview and handwritten notes taken by the interviewer. Audiotapes were listened to multiple times, with verbatim transcriptions from pigeon Arabic to formal Arabic to English. The Arabic speaking members of the research team reviewed the accuracy of translation and data interpretation. Data were cross-checked by all members of the research team.
Phase 2 of the analysis (disassembling of the data) required extraction of individual responses to each research question from the database. Audiotapes and transcripts were reviewed several times to ensure the content, tone, and accurate capture of participants’ feelings. Phase 3 involved extracting significant statements from the disassembled data, and reassembling these statements under the five key areas explored in the interviews. Reassembled data were interpreted in collaboration with members of the research team (Phase 4). The final stage of data analysis (Phase 5) drew together the reassembled data. Data were interpreted to identify an overarching theme, with three subthemes that illustrated the complexity of participants’ experiences.
Undertaking the research and data analysis required careful attention to the transcultural nature of the study. Each member of the research team resided in the UAE or had significant experience working in the Middle East. The research team included an Arabic speaking researcher with cultural competence specific to the UAE context.
Results
The analysis revealed an overarching theme journeying from disbelief and shock to acceptance and patience. This portrayed a common experience described by participating mothers. Three separate subthemes emerged that illustrated participants’ experiences, specifically: initial impact of diagnoses; what helped; and how it is now. Verbatim quotations from participants (using pseudonyms) are included to illustrate the findings.
Initial Impact of Diagnosis
Although it was close to 1 year since diagnosis, each mother could clearly recall the experience of initial disbelief and shock following diagnosis. It was a time of distressing emotions, and the mothers described wide-ranging worry and concern for their child. … we could not believe this happened … all of us are very shocked, I was very much worried about my son (KHULUD) [I am] … so upset and confused, I could not believe it, as she is still very young. (FATIMA) This was not expected to happen to our daughter … [I] cry with bitterness and pain. (A’ISHA) Who can I communicate with if he has any issues or is unconscious? (KHULUD) … [and] what about his future? Will he be able to get married? (KHULUD) I’m so worried about the future … taking insulin all her life. (A’ISHA) I was so worried about the consequences of spreading the news among them, which may have a negative or bad effect on my daughter’s future. (FATIMA) The school was not cooperative in taking care of her health, but after an argument with the school management, the treatment has changed and become much better. (A’ISHA) I requested my husband to keep this incident confidential and not to disclose it to neighbors or some other relatives, particularly those who are not educated. (FATIMA)
What Helped?
Mothers spoke of ways in which faith, family, and culture impacted on their experience, while also mentioning some of the challenges in these interactions.
Faith and Culture
The pivotal role that participating mothers’ spiritual connections and faith played in coping with this diagnosis was apparent. I pray much and do lots of supplications for her. (FATIMA) My parents keep praying and keep reciting versus of the Holy Quran, and repeating certain supplications to Allah. (BASMAH) I have a strong faith in Allah, and we as Muslims should surrender to Allah’s destiny. (A’ISHA) It is said that olive leaf helps in reducing the blood sugar to reach normal percentage. (KHULUD) During Ramadan, I encourage them to fast. When we visit peoples’ houses I let them take [a] small amount, so they will not feel different than other children. (BASMAH)
Extended Family
One mother spoke of how much relatives and friends had assisted her. We have been supported fully by all relatives and friends, and this support made our life run smoothly and easily. (A’ISHA) My family live here in the country and because I didn’t tell them early about the incident, they blamed me much. I was very much confused, shocked, and upset of the new situation. In general, yes, I have received full support from my family. (FATIMA)
Health-Care Professionals
Participating mothers identified how health-care professionals had assisted them. The positive impact of contact with physicians, nurse educators, and nurses in clinical settings and schools was evident in mothers’ reports of their interactions with clinicians. I got full support from the ER, the pediatric physician comforted me a lot and made me feel that I’m strong and brave enough to face the new situation. (FATIMA) One of the health professional supports that helped the most was the treating physician … [who had an] excellent technique and instilled hope in ourselves. (KHULUD) The nurses and educator were so good and so gentle. (FATIMA) All the medical staff was so cooperative. (A’ISHA) The health education … (A’ISHA) … in relation to the food given and timing of blood sugar testing. (FATIMA) The school nurses played a major role and helped us a lot. (FATIMA) The quantity of injections needed [were] unavailable in the pharmacy. (KHULUD) Phoning the clinic and nobody answers. (KHULUD) For me, I think everything was so perfect, probably the supplies and the medicine if [they] were brought to me, it would be much better than getting it myself as I was alone here in the hospital with my daughter and I didn’t like to leave her. (FATIMA) booklets with coloring explaining diabetes in a simple way for kids themselves. (A’ISHA)
And Now
In contrast to the shock, disbelief and confusion experienced on diagnosis, and the multitude of worries that threatened to overwhelm participating mothers, they indicated a significant shift toward acceptance and an almost normal life. But over the time, the situation has been changed and become almost ordinary and acceptable to us. (KHULUD) I can say the impact of the incident on us, over time became almost normal. (A’ISHA) Gradually over time, we adapted to the new situation. (BASMAH) The situation became normal, up to 85%. (KHULUD) They (family) encouraged me to be optimistic and … they supported me morally and materially … over time the impact of the incident on us became almost normal. (A’ISHA) There was an impact on my life personally and on the relation[ship] I have with my husband, who noticed this clearly and told me that I had become nervous and my relation[ship] with him and with others became a little different. (KHULUD) My relation[ship] with my husband became a little different than before. (A’ISHA) I sympathize with [my daughter with T1DM] … sometimes I get upset and nervous of her behavior and endless requests. (FATIMA) Our relations[hips] with our friends in general were so good, and some of them became closer and friendlier to us. (FATIMA) It has been changed much. (FATIMA) … we have changed the eating pattern for the entire house. (BASMAH) We wake up in the morning and first thing I check blood sugar before having breakfast. After breakfast, I give the dose needed and their father usually, takes them to their school. The school nurse takes care during my absence and she keeps in touch with me 2–3 times daily. I get them home from school for their lunch. Before going to bed, I check blood sugar and give the dose needed. I myself, go to bed almost after midnight, when I’m certain that all the tasks have been made. (FATIMA) Usually, I check my daughter’s blood sugar before and after the meals and at frequent times of the day. I prefer to cook at home and in the afternoon, I go to bed with her to get some rest. After I wake up, I check her blood sugar again. If it is low, I usually give her fresh juice. (A’ISHA) Type 1 diabetes mellitus management tasks in a typical day. BSL = blood sugar level.
The vigilance and monitoring required was such that siblings were involved in observation and administration of insulin. Before T1DM diagnosis, each child went to school and the mother was able to rest assured that her child was safe. Frequent contact with the school had now become the norm, and a readiness to drop any other activity became a necessity. Despite the changes required since the participating mothers had learned that their child had T1DM, each mother described the transition made and the factors that had supported and enabled them to see their situation as almost ordinary. Figure 2 presents the key points of this journey from the point of diagnosis (where shock, disbelief, and worry threatened to overwhelm) to a point of acceptance and patient management of the demands and challenges of caring for a child with T1DM.
Mothers’ responses to their child’s diagnosis with type 1 diabetes mellitus. SKMC = Sheikh Khalifa Medical City.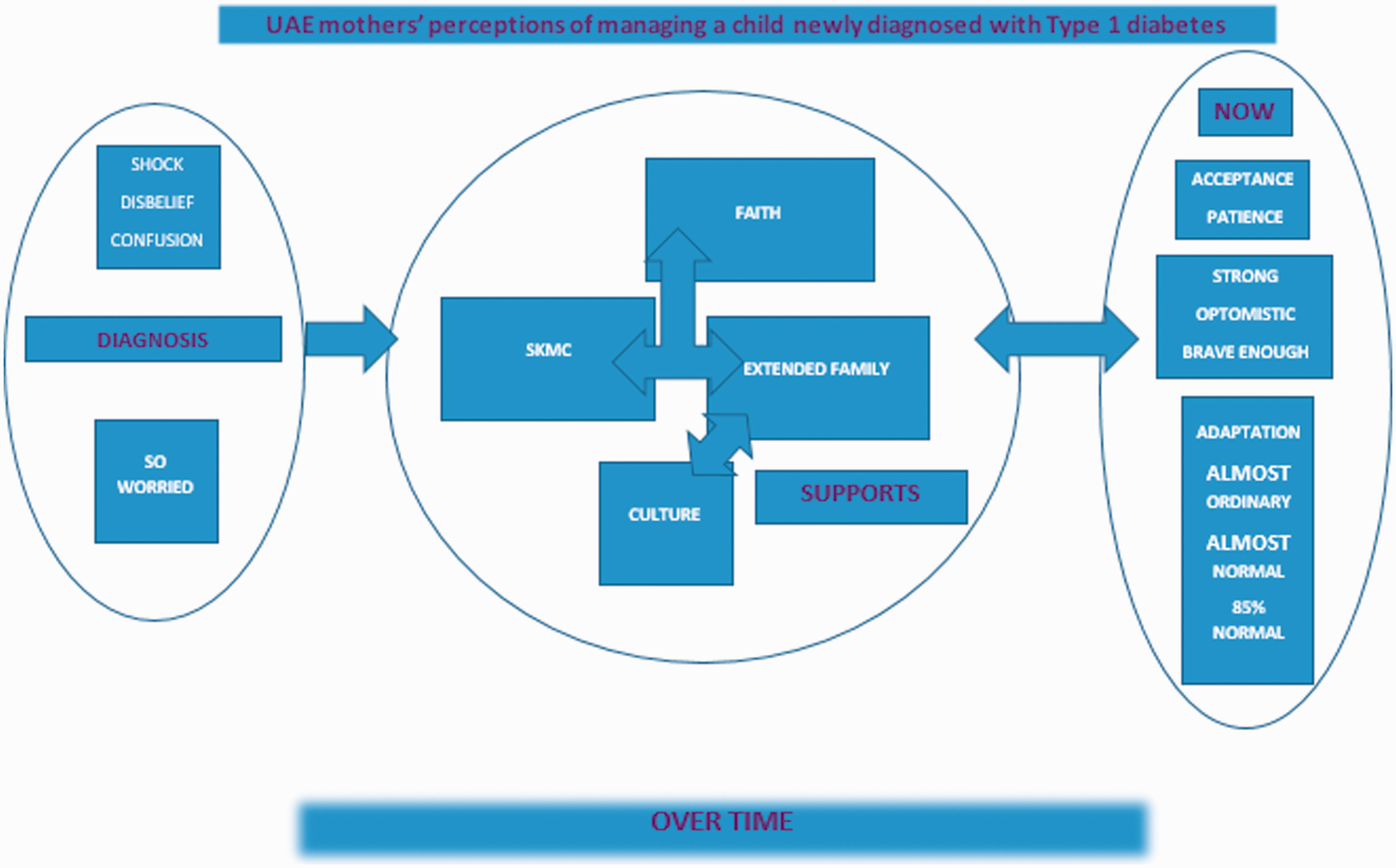
Discussion
Participating mothers described initial reactions of shock and disbelief, followed by transition to near ordinary or near normal (85% normal) family functioning. Family, culture, and faith emerged as critical supports in the whirlwind challenge of balancing multiple demands of a typical day, which included the often competing needs of the newly diagnosed child versus the broader family. The emotional distress described by mothers at their child’s initial T1DM diagnosis (including feeling overwhelmed, shocked, upset, confused, and overcome with disbelief, worry, and fear) was consistent with that described by parents in Western countries (Bowes et al., 2009; Jönsson, Lundqvist, Tiberg, & Hallström, 2015). In 2005, Welsh researchers described the unexpectedness and rapidity of a T1DM diagnosis as placing parents in a situation they felt ill-equipped to manage (Lowes, Gregory, & Lyne, 2005). Swedish researchers described this time as one of complexity and challenge for the entire family (Jönsson et al., 2015). A study conducted in 2013 reporting on Iranian mothers’ experience of diagnosis also spoke of shock, concern, and worry for their child’s future, and for one mother, anger at the unfairness of this diagnosis for her young child (Abolhassani et al., 2018).
In this study, mothers feared the impact of T1DM on their child’s physical well-being, but also feared the stigmatizing behaviors and attitudes they believed would be directed toward their child as a result of this diagnosis. These mothers had tertiary qualifications in either nursing or pharmacy and could perhaps be expected to be aware of advances in treatment for T1DM and thus more hopeful for their child’s future. Nevertheless, worry about adverse judgments, including exclusion from being able to marry, was expressed. Limited understanding of the condition in the broader family and among friends or acquaintances further contributed to the worries these mothers described. These fears were congruent with the recently described experience of stigmatization of children with T1DM and their parents living on the West Bank in Palestine (Elissa, Bratt, Axelsson, Khatib, & Sparud-Lundin, 2017). Palestinian parents reported attempts to conceal the disease and keep it secret, and the children’s feelings of being different from others. Similarly, participants in this study feared the impact on their child when others found out about the T1DM diagnosis. Just as the mothers in this study feared for their children’s future employment and marriage prospects, mothers in Iran feared that their daughters with T1DM would not be accepted in the community and worried as to whether a man would be interested in marrying a woman with T1DM (Khandan et al., 2018). Experiencing diabetes stigma is not unique to Middle Eastern countries or to mothers parenting a child with T1DM. Recognition of the potential adverse impact of diabetes stigma on self-care and social identify in adults living with T1DM in Australia has recently led to the development of the self-report Type 1 Diabetes Stigma Assessment Scale (Browne, Ventura, Mosely, & Speight, 2017). This scale incorporates three broad areas: treated differently, blame and judgment, and identity concerns. A review of research on stigma directed toward adults with diabetes (both T1DM and Type 2 DM) found a range of specific fears, including being sick, contagiousness, and rejected as a marriage candidate (Abdoli, Doosti Irani, Hardy, & Funnell, 2018). Concerns as to marriageability were noted among young Asian women, with delayed marriage reported in Iran and India (Abdoli et al., 2018), while one “unmarried Arab male in Australia described … males and females with diabetes as less desirable candidates for marriage due to a perceived connection between diabetes, erectile dysfunction and the passing of diabetes to their children” (Abouzeid, Philpot, Janus, Coates, & Dunbar, as cited in Abdoli et al., 2018, p. 116). To date, it appears that no studies have focused on assessing the parameters of diabetes stigma in the T1DM pediatric population or identifying culturally specific beliefs that influence stigma toward children with T1DM and their families.
As mothers in this study sought to adapt and manage their distress, there were supports that provided significant benefit. Each participating mother described support received from extended family including a listening ear, moral and material support, encouragement, sympathy, and prayers to Allah on their behalf. The strongly positive role of faith and family permeated the experience of these mothers. Abdel-Khalek (2011) suggested that consistent with other monotheistic religions, Islam includes a range of practices that adherents can use as coping mechanisms when confronted with situations such as that encountered by mothers in this study. Participants specifically mentioned prayers and supplications to Allah made by the mother herself or family members, and faith and acceptance or surrender to the will of Allah. Saudi Arabian researchers recently drew attention to the limited research exploring the role of spiritual coping and religiosity among practicing Muslims experiencing psychological and physical health-related challenges (Cruz et al., 2016). The value that mothers in this study placed on their faith as a coping strategy was consistent with the Saudi study (Cruz et al., 2016) and supports the recommendation that a focus on spiritual coping be actively incorporated in health-care delivery.
The availability of adequate social support has been linked to improved disease control and decreased stress (Zysberg & Lang, 2015), while the adverse impact of limited psychosocial support on the quality of life reported by maternal caregivers looking after children with T1DM has been reported by Australian researchers (Thorsteinsson et al., 2017). However, mothers in this study identified interactions with extended family and friends as largely positive and an integral component of what helped them to manage and adapt to caring for a child with T1DM. In describing Emirati society, D’raven and Pasha-Zaidi (2016) highlighted a focus on group-based achievements and a concern for “the care, protection and welfare of others.” It may be that as members of a collectivist society (Cooper & Brownie, 2018, p. 911), these mothers perhaps had access to a greater level of family support than is generally available to mothers in individualistic societies.
Specific aspects of Islamic culture assisted with coping with the diagnosis of T1DM and managing the disease and also influenced the ways in which families attempted to balance the needs of the child with T1DM and the desire to remain connected and actively participating in cultural events. The importance of fasting during the holy month of Ramadan (as one of the five pillars of Islam) presented specific challenges. The importance of this practice is such that while children and those with chronic diseases are exempt from fasting, many continue to fast. The challenges of managing the Ramadan period of fasting and associated social events where large amounts of sweet foods are served (such as those associated with breaking the fast after dusk each day) have been widely described (Elissa et al., 2017; Peterson, Nayda, & Hill, 2012; Sahay & Nagesh, 2016; Zabeen et al., 2014). In this study, mothers highlighted the importance of inclusion in fasting and breaking their fast with family and friends for the child, so the child did not feel different from the rest of the family.
Each mother spoke strongly of the role that faith, culture, and extended family served in their transition from shock, disbelief, and confusion to now, being able to view themselves as strong, optimistic, and brave enough. The experiences of mothers in this study appear to contradict those reported in other studies, with reference to faith and religion strikingly absent in studies reported in countries such as the United States (Rechenberg et al., 2017), Wales (Bowes et al., 2009), and Australia (Thorsteinsson et al., 2017). Although faith, culture, and extended family were highly valued, these supports were not without challenges that required negotiation and compromise.
A particular challenge for health professionals providing treatment for children with T1DM is associated with the complexity of the information and skills that are required for effective T1DM management. Rankin et al. (2014) reported parents distressed by information overload and terrified as to how they would manage when they took their child home after the initial diagnosis. Researchers in Scotland emphasized the importance of providing reassurance and attending to the emotional needs of parents of children newly diagnosed with T1DM before providing the complex information associated with T1DM management (Rankin et al., 2014). Of particular note, mothers in the study emphasized the reassurance and sense of hope offered to them; they valued the kindness and gentleness with which they were supported by their health professionals. Contacts with medical and nursing services available to these participants were identified as integral to adjusting to this major change in the child and family’s life.
Understanding the experience of parenting a child with T1DM provides insights into the challenges faced by mothers as primary caregivers. All mothers in this study reported feeling satisfied, comfortable, supported, and assisted by the staff with whom they interacted. It is important to note that given their professional training in health care, these mothers may have already been familiar with testing blood sugar levels, administering injections and monitoring a person’s health status. Nevertheless, these mothers specifically mentioned practical education (including dietary information), blood glucose monitoring, mothers’ support groups, and the positivity and hope expressed by health professionals. The powerful role that the patient–provider relationship plays in increasing patient satisfaction has been well described (Ayala, Howe, Dumser, Buzby, & Murphy, 2014). In addition, attending to parents’ personal and emotional needs has been reported to promote parental satisfaction and self-efficacy in caring for a child with T1DM (Kratz, Uding, Trahms, Villareale, & Kieckhefer, 2009). Peer support accessed through attendance at support groups has been identified as a means of reducing mothers’ isolation (Smaldone & Ritholz, 2011)
After almost 1 year since the T1DM diagnosis had been made, mothers in this study reported that life was now near normal, while also describing the multiple daily demands in caring for a child with T1DM. Swedish researchers explored the experiences of families in which a child had been diagnosed with T1DM 3 years earlier (Wennick, Lundqvist, & Hallström, 2009). Family members spoke of T1DM as being deeply rooted in their everyday life, while impacting each person in different ways; parents also felt that the family were more united as a result of the illness (Wennick et al., 2009). The experience of adapting and transitioning to what was now perceived as normal was also described by English researchers who suggested that despite differences in culture, length of time since diagnosis, and ages, families living with a child with T1DM shared similar experiences (Marshall et al., 2009).
Near normal or almost normal was qualified with reference to the impact on relationships and increased anxiety around caring for a child with T1DM. Recent studies have identified significant levels of stress and posttraumatic stress in mothers caring for children with T1DM (Rechenberg et al., 2017). For some mothers, the sense of an impossible task leading to burnout has been described (Lindström, Åman, Norberg, Forssberg, & Anderzén-Carlsson, 2017); for others, worry has been conceptualized as a core aspect of trying to make sure the child is safe (Watt, 2017). The constant management tasks associated with T1DM that mothers in this study described reflected those in other studies, with a typical day including blood glucose monitoring, insulin administration, dietary management, frequent contact with the child’s school, vigilance, and needing to be always available (Boogerd et al., 2015; Lindström et al., 2017).
Strengths and Limitations
Each participant had completed qualifications in nursing or pharmacy, and this is a potential limitation of this study. However, educational attainment in GCC countries is high (reported to be higher than countries such as the United States), and these mothers are likely representative of this generation of women in the UAE (Marmenout & Lirio, 2014). Despite high literacy rates, participation in the workforce remains low, thus these participants may have had little experience working as health professionals (Social Vision, 2016). Each of the participants had attended the support group conducted within the hospital, perhaps indicating a proactive approach to seeking support and coping style, and this presents a possible source of bias in the sample. The small number of cases recruited for this study with all participants accessing a single health service limits the generalizability of these findings. However, the in-depth analysis of the data enabled a comprehensive picture of the experience of these Arabic mothers that has not previously been reported and is worthy of consideration for those providing services to mothers of children newly diagnosed with T1DM.
Implications for Practice
The findings from this study underscore the importance of recognizing contextual, cultural, and spiritual factors when caring for families where a child is newly diagnosed with T1DM. Clinicians are encouraged to appreciate the value of including a focus on spiritual coping in health-care delivery. Likewise, the value of emotional support for mothers as caregivers needs to be an integral component of service provision for families with a child with T1DM. Education programs delivered to schools and community educations that focus to build understanding of T1DM are required to reduce stigmatizing behaviors and attitudes. In settings where child-friendly educational materials are not readily available, the development of such resources needs attention. Given that access to Internet services is readily available across the GCC countries, online support services for children with T1DM and their families require consideration.
Implications for Nursing Research
This study provides an insight into the challenges to be negotiated by a mother caring for a child newly diagnosed with T1DM in the Middle East. The findings suggest multiple areas for further nursing research. These mothers were educated as health professionals and had all participated in a support group conducted at the hospital. To obtain a broader perspective on the experiences of Arabic speaking mothers in the GCC region, replicating this study with a larger group of nonhealth professional mothers who have had no significant contact with T1DM prior to their child being diagnosed with this condition is recommended. Likewise, the authors suggest accessing participants for a further study who have not attended a support group after their child was diagnosed will T1DM.
Mothers in this study were concerned about the potential impact of stigma on their child. Research identifying contextual and cultural beliefs underpinning stigmatizing attitudes and behaviors experienced by children with T1DM and their families in this region is essential to ensure that programs to raise community awareness about T1DM are culturally specific.
The adverse impact on the mental health and well-being of mothers caring for a child with T1DM has been described in studies undertaken in other parts of the world. Although the psychological distress experienced by these mothers is evident in the findings, this study focused primarily on supporting and enabling factors. Information specific to adverse impacts on mental well-being such as a formal diagnosis of depression was not obtained. Further research examining the impact on mental health and psychological well-being of mothers, availability of specialist mental health services, and support and willingness to access such supports would enable further enhancement of health service support.
Conclusion
This study provides insight into the challenges and support needs of mothers who are providing care to a child newly diagnosed with T1DM in an Arab Muslim context. The impact of a T1DM diagnosis is substantive, with profound psychological and physical demands on mothers and impacts for the broader family. When asked what helped, mothers reported faith, culture, extended family, and the presence of competent and empathic health professionals as important support factors. The present findings provide a basis for enhancements in health service support along with themes to inform further research.
Supplemental Material
Supplemental material for Case-Based Insights: Arab Muslim Mothers’ Experiences of Managing a Child Newly Diagnosed With Type 1 Diabetes Mellitus
Supplemental Material for Case-Based Insights: Arab Muslim Mothers’ Experiences of Managing a Child Newly Diagnosed With Type 1 Diabetes Mellitus by Rachel Cathrine Rossiter HlthScD Jennifer Louise Cooper DPubHlth Suhad Issa Marjei BSN Sharon Brownie DBA in SAGE Open Nursing
Footnotes
Data Accessibility
The deidentified qualitative data used in this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.