
Abstract
Background
Placenta accreta spectrum (PAS) disorders have become more noticeable as a serious and potentially life-threatening obstetric concern due to a rise in prevalence from 0.12% to 0.31% in recent years. New preventive measures, such as the bladder filling technique, seek to identify the bladder's borders, protect it, and displace it away from the lower uterine segment during placental removal.
Aim
To determine whether the saline bladder filling technique prevents the incidence rate of intraoperative bladder injuries among pregnant women undergoing PAS surgery.
Method
Systematic searches were conducted in PubMed, Embase, and the Cumulative Index to Nursing, Allied Health Literature and, Google Scholar from 2013 to 2023. The Cochrane Risk of Bias (ROB 2.0) and ROB in Nonrandomized Studies of Interventions tools were used to assess the quality of the selected studies
Findings
A total of 2,094 articles were initially retrieved, and after screening, four articles met the eligibility criteria and were included in the final. The primary outcome of this systematic literature review (SLR) indicates that the utilization of the bladder filling technique was associated with a reduced occurrence of bladder injury, with an incidence range of 4.5% to 21.9% when the bladder filling technique utilized, in contrast to an incidence range of 13.1% to 32.4% when the bladder-filling technique was not utilized. Furthermore, the utilization of the bladder filling technique was found to be correlated with a reduced surgical procedure time and decreased blood loss.
Conclusion
This SLR reveals that utilizing the bladder filling technique during PAS surgeries decreases the occurrence of intraoperative bladder injury, which, in turn, reduces the occurrence of other intraoperative complications, including intraoperative blood loss. Therefore, healthcare providers and policymakers should start developing surgical protocols for the use of this technique, as it has the potential to significantly impact the outcomes of pregnant women undergoing PAS surgeries.
Introduction
Placenta accreta spectrum (PAS) refers to a group of obstetric conditions characterized by abnormal placental attachment to the uterine wall (Horgan & Abuhamad, 2022; Wortman & Alexander, 2013). It poses significant challenges during pregnancy and childbirth and requires specialized management to ensure the best possible outcomes for both the mother and the fetus (Fonseca & Ayres de Campos, 2021; Jauniaux et al., 2019). PAS disorders have emerged as a substantial and potentially life-threatening obstetric concern, with a rising prevalence from 0.12% to 0.31% over the past 3 decades (Zhang et al., 2017). Additionally, these disorders are associated with a reported mortality rate of around 7.0% (Liu et al., 2021).
Several risk factors may contribute to the development of PAS (Morlando & Collins, 2020). Previous uterine surgeries, such as cesarean sections or myomectomies, can disrupt the normal architecture of the uterine wall and trigger issues. Other risk factors include advanced maternal age, multiple pregnancies, and placenta previa, which occur when the placenta covers the opening of the cervix (Fonseca & Ayres de Campos, 2021).
The management of PAS involves careful planning to mitigate potential risks (Tillu et al., 2019), and delivery is typically scheduled in a specialized center with expertise in managing PAS cases and the necessary resources to handle potential complications. The timing of delivery must also be carefully considered, taking into account the gestational age of the fetus, maternal well-being, and the availability of the necessary skilled surgical team (Eller et al., 2009). During surgery for PAS, the primary objective is the safe management of the abnormally adherent placenta to minimize maternal morbidity and prevent complications associated with placental invasion (Herzberg et al., 2022; Manidip & Soma, 2020). Various surgical techniques, such as in-bloc hysterectomy or other specialized approaches, may be employed depending on the extent of placental invasion and the overall clinical scenario (Alves et al., 2021). Manual removal and controlled traction are not appropriate management options for PAS, as these techniques are more suited to cases of normal placental attachment (Bartels et al., 2024).
The bladder-filling technique has emerged as a potential preventive measure against operative injury in recent years. It allows the creation of a physical barrier to potential damage by filling the bladder with a saline solution, displacing it away from the lower uterine segment and thus reducing the risk of inadvertent injury during placental removal. To evaluate the feasibility and safety of the technique, a structured review of the existing literature is necessary.
Objective
This systematic review aims to determine the effectiveness of the bladder filling technique in terms of reducing the incidence of intraoperative bladder injury among pregnant women undergoing PAS surgery.
Search Keywords and Combinations Used Across Databases.
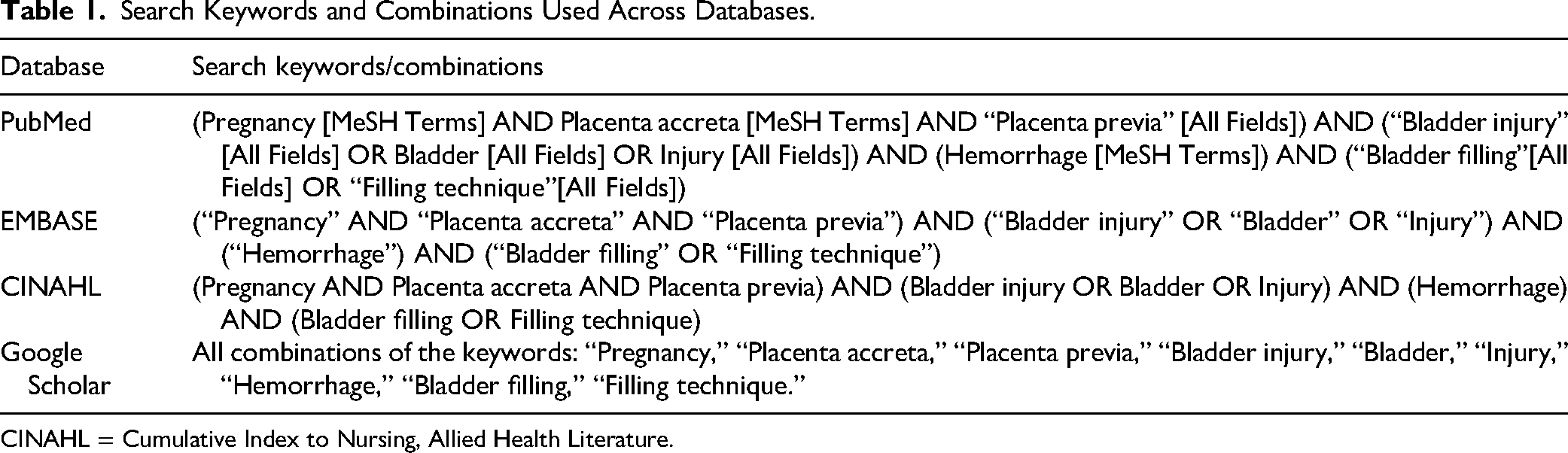
CINAHL = Cumulative Index to Nursing, Allied Health Literature.
Material and Methods
Protocol
This systematic review was reported as closely as possible following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021).
Eligibility Criteria
The following inclusion criteria were applied:
Participants: Patients undergoing placenta accreta surgery.
Interventions: Bladder filling techniques.
Comparison: No or other methods
Outcome: The primary outcome is the incidence of bladder injury after using of the bladder filling technique. Secondary outcomes are the duration of the operation and the incidence of other intraoperative complications.
Study design: Prospective or retrospective comparative studies.
Studies published between 2013 and 2023 were included. Patients with systemic diseases, syndromes, bleeding disorders, long-term medications such as anticoagulants and anti-inflammatory medications, and those who have undergone other adjunctive surgical procedures, as well as case reports, case series, noncomparative studies, review articles, meta-analyses, letters to the editor, and non-English studies, were excluded.
Information Sources, Search Strategy, and Selection Process
A comprehensive and systematic search was conducted across various electronic databases, including PubMed, EMBASE, Cumulative Index to Nursing and Allied Health Literature, and Google Scholar. Additionally, a manual search was performed for the reference lists of the selected studies to identify any potentially eligible studies. The results were documented and presented as illustrated in the PRISMA diagram (see Figure 1). The search strategy comprised a combination of MeSH terms, Embase subject headings (Emtree) terms, and relevant free-text keywords. Using a combination of keywords and controlled vocabulary (such as MeSH terms) is important for capturing relevant articles (see Table 1). Once duplicate records were removed using a reference manager (EndNote 8.0, Clarivate Analytics, Philadelphia, PA), the titles and abstracts of the remaining retrieved studies were evaluated based on predetermined eligibility criteria. The full texts of potentially eligible studies underwent a thorough examination for the final inclusion or exclusion decision. Two authors (NF and WS) independently and in duplicate performed this process using the Rayyan website tool (http://rayyan.qcri.org).

PRISMA Diagram for Study Selection.
Data Collection of Processes and Data Items
The data were extracted from eligible studies, and the extraction process was independently conducted by two authors (NF and WM) using a prepiloted extraction form to ensure reliability. The extracted data included general information (journal name, authors’ names, country, reference citation, and study author contact details), characteristics of the included studies (study design, aim of the study, setting, inclusion and exclusion criteria, ethical approval status, sample size calculation, and significance level), participant characteristics (participant description, age, location, obstetric history, and gestational age at delivery), and outcomes of interest (incidence of bladder injury). Additionally, intraoperative and postoperative outcomes, such as the length of hospital stay, incidence of complications, duration of the operation, type of procedure, and amount/type of filling material, were recorded.
Risk of Bias in Individual Studies
The risk of bias (ROB) in the included studies was independently assessed by two authors (NF and WS) using the Cochrane ROB (ROB 2.0) tool for randomized studies (Sterne et al., 2019) and the ROB in Nonrandomized Studies of Interventions (ROBINS-I) tool for nonrandomized clinical trials (Sterne et al., 2016). The tools were employed for the quality assessment of included randomized controlled trials (RCTs) and CCTs, respectively.
The ROB 2.0 tool is a revised version of the Cochrane ROB tool, structured into five bias domains: (D1) bias due to the randomization process, (D2) bias due to deviations from intended interventions, (D3) bias due to missing outcome data, (D4) bias due to the measurement of the outcome, and (D5) bias due to the selection of the reported result. For each domain and study, the ROB was categorized as low risk, some concerns, or high risk. The ROBINS-I tool covers seven bias domains: (D1) bias due to confounding, (D2) bias in the selection of participants into the study, (D3) bias in the classification of interventions, (D4) bias due to deviations from intended interventions, (D5) bias due to missing data, (D6) bias in the measurement of outcomes, and (D7) bias in the selection of the reported result.
The included studies were evaluated for the risk of low, moderate, serious, critical, or no information ROB based on the aforementioned domains of the ROB 2.0/ROBINS-I tools. ROB figures were generated using the ROB visualization (robvis) tool. Two authors (NF and WM) independently assessed the ROB of all included studies.
Results
Study Selection
A total of 2094 articles were retrieved from these combined electronic databases. Among them, 762 duplicates were eliminated using the EndNote bibliographic citation manager, resulting in 1,332 distinct articles. After a review of the titles and abstracts of these 1,332 records, 1,316 unrelated records were excluded, which left 16 records providing relevant information about the feasibility of the bladder filling technique for preventing intraoperative bladder injury in pregnant women undergoing placenta accreta surgery.
These 16 records, presented as text articles in either full-text or PDF format, underwent meticulous scrutiny. Among them, 12 articles were excluded from the study, and further details are provided in Appendix 1. The remaining four studies fulfilled the criteria for in-depth analysis and were thus incorporated into this systematic literature review (SLR). Figure 1 illustrates the PRISMA diagram with details of the search strategy outcomes and the sequential steps leading to the identification of the four eligible articles. No relevant studies were found from a manual search in the reference lists of the selected articles.
Study Characteristics
The characteristics and results of included studies were summarized in Table 2. Four studies were included in the final analysis.
Summary of Study Characteristics of the Included Studies.

RCT = randomized controlled trial; PAS = placenta accreta spectrum.
Study Population
The pregnant women recruited for the studies were aged between 20 and 46 years old. All studies included a control group in which the bladder was not filled (Ali et al., 2019; Celik et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018). All patients were recruited between 2015 and 2018 for the RCTs (Ali et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018). However, Celik et al. (2019) recruited all patients retrospectively between January 2009 and January 2019 for both intervention and control groups. Özcan et al. (2018) included women with placenta percreta; however, the study did not specify whether these cases exclusively involved bladder invasion or other visceral structures. In contrast, Celik et al. (2019) included women with placenta percreta who underwent cesarean hysterectomy but explicitly excluded cases where percreta involved bladder invasion and required intentional bladder opening, indicating that the included cases pertained to other visceral structures. Cases with hysterectomy due to deep uterine lacerations, cases due to uterine atonia, and cases with percreta and bladder invasion where the surgeon intentionally opened the bladder were all excluded from Celik et al.’s (2019) study. Kuznetsova et al. (2020) included women with PAS who underwent a planned cesarean section followed by metroplasty surgery. Ali et al.'s (2019) study included women who underwent elective CS with the presence of any risk factor for urinary bladder injury, such as current placenta previa and/or any type of placenta accreta.
Setting of Studies
The included studies were conducted in Russia (Kuznetsova et al., 2020), Egypt (Ali et al., 2019), and two studies were conducted in Turkey (Celik et al., 2019; Özcan et al., 2018). All included RCTs were conducted in university hospitals (Ali et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018); these RCTs were all single-center trials. Meanwhile, the data for Celik et al.'s (2019) retrospective study were collected from one university hospital and one education and research hospital in Turkey. All patients were recruited by the Department of Obstetrics and Gynecology at the respective hospitals in which the included studies were conducted.
Nature of Study Methods
Three included studies were randomized controlled clinical trials (Ali et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018) in which patients were randomized either into the filled-bladder or the nonfilled-bladder group; one study only was a retrospective cohort study (Celik et al., 2019). All studies were approved by the Committee of Ethics in the respective selected hospitals. All studies declared that there were no conflicts of interest.
Details on Intervention
In all studies (Ali et al., 2019; Celik et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018), various interventions related to bladder filling and cesarean section procedures were explored. Across the studies, there were several commonalities and differences in the types of surgical approaches used for cesarean deliveries. All studies reported that all surgeries were performed under general anesthesia. Both Celik et al. (2019) and Ali et al. (2019) employed a Pfannenstiel incision for their cesarean sections. In contrast, Özcan et al. (2018) mentioned that a midline periumbilical incision was utilized. Kuznetsova et al. (2020) employed various surgical approaches during their cesarean deliveries, including medium or lower midline laparotomy, double incision cesarean section for fetal extraction safety, metroplasty, and bladder defect suturing.
All four studies utilized different amounts of saline solution for bladder filling, ranging from 200 mL to 300 mL (Ali et al., 2019; Celik et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018). Three studies used 200 mL of saline for bladder filling (Ali et al., 2019; Celik et al., 2019; Kuznetsova et al., 2020), while Özcan et al. (2018) used 300 mL of saline. The studies applied bladder filling at various stages, such as before surgery and after inducing anesthesia, during bladder mobilization, or before a cesarean hysterectomy. In Celik et al.'s (2019) and Ali et al.'s (2019) studies, bladder filling was performed before surgery after inducing general anesthesia. In the study of Özcan et al. (2018), the bladder was filled during surgery. Additionally, after completing the surgical procedure, the balder was filled with diluted methylene blue in all patients to ensure the detection of any overlooked bladder injuries (Özcan et al., 2018). Furthermore, Kuznetsova et al. (2020) mentioned that bladder filling was performed at the bladder mobilization stage before metroplasty was performed.
ROB Within Individual Studies
The ROB of the included RCTs was assessed using the Cochrane ROB (ROB 2.0) tool for randomized studies (Ali et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018; Table 3 and Figure 2). Concerning the bias domain related to the randomization process, the studies by Kuznetsova et al. (2020) and Özcan et al. (2018) were judged to have some concerns since both studies did not provide any information about the method of randomization or allocation concealment. In contrast, the study by Ali et al. (2019) was judged to have a low ROB in this domain, as the method of randomization and allocation concealment was reported using closed envelopes.

Risk of Bias Figure for RCTs (Judged with ROB-2 Tool).
Risk of Bias Table for RCTs (Judged with ROB-2 Tool).
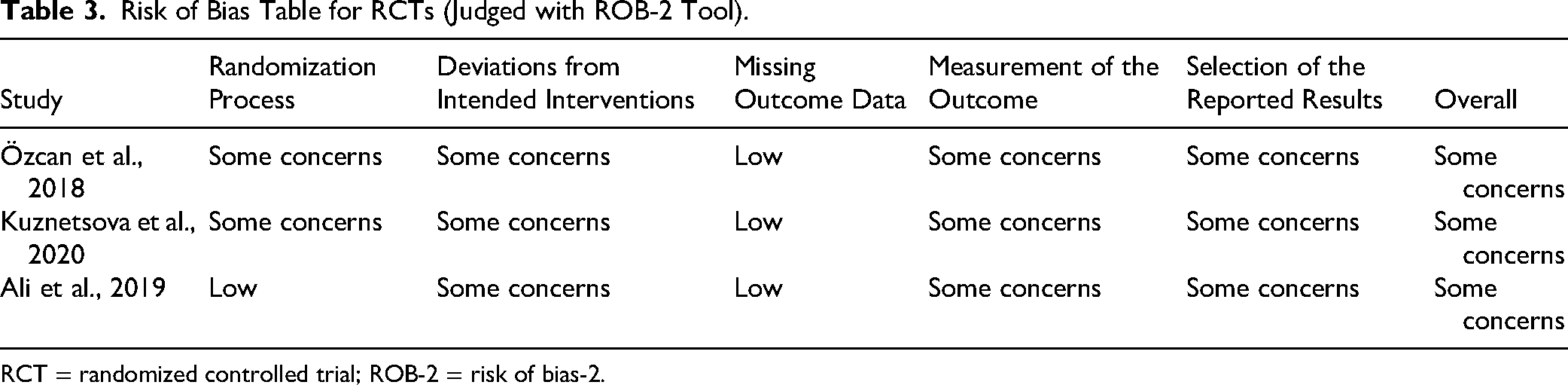
RCT = randomized controlled trial; ROB-2 = risk of bias-2.
Regarding the bias domain due to deviations from intended interventions, due to the nature of the intervention, all patients were unaware of the intervention received, while clinicians were aware of the intervention in all studies. Therefore, all studies were judged to have some concerns in this domain. Concerning the bias domain due to missing outcome data, all studies were judged to have a low ROB in this domain, as the outcome data were likely available for all patients. Concerning the bias domain due to the measurement of the outcome, no information about the blinding of outcome assessors was reported in all studies. However, due to the nature of the intervention, outcome assessors were aware of the intervention received, resulting in all studies being judged to have some concerns in this domain. Regarding the bias domain due to the selection of the reported result, none of the studies reported the availability of a trial protocol or statistical analysis plan. Consequently, all studies were judged to have some concerns in this domain. Overall, all studies were judged to have some concerns about the ROB, as each study was found to have at least one domain with some concerns about bias (Ali et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018). However, the ROB of the included retrospective cohort study was assessed using ROBINS-I for non-RCTs (Celik et al., 2019). The study by Celik et al. (2019), was judged to have a moderate ROB because the selection of participants into the study was probably not based on participant characteristics observed after the start of the intervention, intervention groups were clearly defined, outcome data were available for all participants, probably the outcome measure hadn't been influenced by knowledge of the intervention received, and probably there were no multiple outcome measurements within the outcome domain in the study (Table 4 and Figure 3).

Risk of Bias Figure for Celik et al. (2019) Study (Judged with ROBINS-I Tool).
Risk of Bias Table for Celik et al. (2019) Study (Judged With ROBINS-I Tool).

ROBINS-I = Risk of Bias in Nonrandomized Studies of Interventions.
Results of Individual Studies
The results of outcomes of interest are summarized in Table 5.
Results of Outcomes of Interests in the Included Studies.

Primary Outcome (The Incidence of Bladder Injury)
The incidence of bladder injury was significantly lower in the group using the bladder-filling technique compared to the group without the technique across all included studies. The incidences of bladder injury using the bladder-filling technique ranged between 4.5% and 21.9%, while without the technique, the incidence ranged between 13.1% and 32.4%. Statistical analysis revealed significant differences in bladder injury incidence between the two groups. In Özcan et al. (2018), the incidence was 21.9% in the filling group and 32.4% in the nonfilling group (p = .07). Although the p-value for Özcan et al. (2018) did not reach statistical significance, the trend suggests a potential benefit. In Kuznetsova et al. (2020), bladder injury occurred in 4.5% of patients with the bladder-filling technique and 31.5% without it (p < .01), showing a 27% difference between the two groups. Ali et al. (2019) reported bladder injury in 5.2% of patients with the technique and 13.1% without it (p = .04). Lastly, Celik et al. (2019) found the incidence to be 10.2% with the filling technique and 30.8% without it (p < .05). As shown in Table 5, the overall incidence of bladder injury was 10.6% (15 out of 141 cases) when the bladder-filling technique was used, and 26.1% (34 out of 130 cases) when it was not. These findings highlight the potential benefit of the bladder-filling technique in reducing bladder injury during cesarean deliveries in PAS cases. Statistical analysis supports the notion that the bladder-filling technique significantly reduces the risk of bladder injury compared to traditional methods.
Secondary Outcomes
Duration of Operation
The duration of operation was reported in all included studies. All studies indicated a shorter operation duration when the bladder filling technique was used, with durations ranging between 44 and 105 min using the bladder filling technique, while the duration ranged between 63 and 211 min without the bladder filling technique (Ali et al., 2019; Celik et al., 2019; Kuznetsova et al., 2020; Özcan et al., 2018). This difference in the duration of the operation was statistically significant in all studies except Özcan et al. (2018). Kuznetsova et al. (2020) reported the longest duration of operation in both groups, with a mean duration of 165 ± 7.1 min and 211 ± 4.1 min with and without the bladder filling technique, respectively. This longer duration of operation was attributed to the nature of the operation, as organ-preserving surgery (metroplasty) was performed by Kuznetsova et al. (2020), while planned cesarean hysterectomy was conducted by Özcan et al. (2018) and Celik et al. (2019). Ali et al. (2019) reported the shortest duration of operation in both groups, with a mean duration of 44.7 ± 11.4 min and 63.5 ± 13.2 min with and without the bladder filling technique. Specifically, in Ali et al. (2019), a normal cesarean section was performed.
Postoperative Hospital Stays
Three studies investigated the postoperative hospital stays associated with the bladder filling technique (Ali et al., 2019; Celik et al., 2019; Özcan et al., 2018). All of the three studies found a longer hospital stay in cases the bladder filling technique was used. However, the difference was not statistically significant between both groups, except in the study of Ali et al. (p < .001; Ali et al., 2019).
Discussion
This SLR has evaluated clinical studies conducted on examining the use of bladder filling technique for prevention the bladder injury. This SLR is the first SLR that reviewed the feasibility of utilizing the bladder filling technique as a preventive measure for intraoperative bladder injury in pregnant women undergoing PAS surgery. The findings presented in this SLR illuminate a critical aspect of obstetric surgery, particularly in cases of PAS, where the risk of intraoperative bladder injury looms large, with an incidence of 9.3% in patients undergoing uterine-preserving surgery or hysterectomy (Friedrich et al., 2023). PAS, characterized by abnormal placental attachment to the uterine wall, poses substantial challenges during both pregnancy and childbirth (Horgan & Abuhamad, 2022). The potential for bladder injury during surgical interventions in these cases underscores the need for preventive measures to ensure the well-being of both the mother and the fetus (Han et al., 2022).
The included studies encompass a variety of surgical approaches employed with the bladder filling technique, raising the possibility of variations in the results of outcome measures and other critical aspects. Cesarean hysterectomy, which featured in two included studies (Celik et al., 2019; Özcan et al., 2018) involves the surgical removal of both the uterus and the placenta. This approach, although effective in addressing PAS, is typically linked to extended operation durations and heightened blood loss. These factors can significantly impact the outcomes associated with the bladder filling technique, including its effectiveness in preventing bladder injury compared to another type of surgeries. In both studies (Celik et al., 2019; Özcan et al., 2018) a planned cesarean hysterectomy, which was found to offer a considerable financial benefit compared to having separate surgeries due to substantially shorter hospital stays and reduced overall surgical time (Seago et al., 1999). Kuznetsova et al. (2020) introduced metroplasty surgery, alongside cesarean delivery, entails the surgical repair of the uterus, often necessary for cases with uterine abnormalities. The addition of metroplasty introduces an additional surgical element that can influence the overall duration of the operation. This was noticed in the study of Kuznetsova et al. (2020), who reported a longer duration of operation in both groups compared to other studies. This, in turn, may have implications for the bladder filling technique's effectiveness in preventing bladder injury, as a more prolonged surgery could increase the potential for complications. Differences in incision types were also observed, with some studies employing Pfannenstiel incisions (Ali et al., 2019; Celik et al., 2019), while others utilized midline periumbilical incisions (Özcan et al., 2018).
In this SLR, the included studies were done in various countries and hospitals in Turkey, Egypt, and Russia. A critical assessment of the methodological quality of the included studies reveals several shortcomings. All studies, except for one, were RCTs. The ROB assessment using the Cochrane ROB tool indicated some concerns in various domains, particularly regarding randomization processes, blinding, and selection of reported results. Many studies lacked details about randomization methods and allocation concealment, potentially affecting the validity of their findings (Spieth et al., 2016), as the method of randomization was not reported in two studies (Kuznetsova et al., 2020; Özcan et al., 2018), while Ali et al. (2019) used closed envelopes for patient randomization. Furthermore, blinding of outcome assessors was not reported in any study, which could introduce measurement bias (Barcot et al., 2020). None of the studies reported the availability of a trial protocol or statistical analysis plan, and this can hinder transparency and reproducibility in research, potentially leading to biased or unverifiable results (Campbell et al., 2022).
Sample size calculation is crucial in clinical trials to ensure statistical power, which determines the trial's ability to detect meaningful treatment effects, ensuring reliable and scientifically valid results while optimizing resource utilization (Nayak, 2010). None of the included studies calculated the required sample size, such shortcoming in the included studies can lead to inconclusive or misleading results, undermining the study's scientific validity and clinical relevance (Thomas & Juanes, 1996). Some studies may not calculate sample sizes due to their exploratory or pilot nature, or due to resource constraints (Lakens, 2022).
Limitations and Implications for Practice
This review presents certain limitations, notably the potential for language bias stemming from the focus on English-language studies, which may have excluded relevant non-English research. Additionally, some studies lacked sufficient detail, limiting comprehensive analysis particularly regarding intervention specifics and ROB assessment. Although the bladder-filling technique appears promising in reducing bladder injury, operative time, and blood loss during PAS surgeries, however, the existing evidence lacks the strength needed to endorse its regular use in clinical practice (Atallah et al., 2020; Fonseca & Ayres de Campos, 2021). Consequently, its use must be approached with care until confirmed by rigorously designed, high quality research, ideally through randomized controlled trials. In the meantime, healthcare institutions should promote continuous professional development to ensure that clinicians are adequately trained in the technique's application, enhancing both safety and surgical outcomes.
Conclusion
The findings of this SLR suggest that the bladder-filling technique shows promise as a strategy for reducing the risk of intraoperative bladder injury during PAS surgery. However, the evidence currently available is not robust enough to support its routine adoption in clinical practice. Successful implementation of this technique will depend not only on its demonstrated efficacy but also on its feasibility and acceptance within the medical community. It is essential that further well-designed studies, particularly RCTs, be conducted to better evaluate its benefits and limitations before widespread integration into clinical protocols.
Footnotes
Author Contributions
Nawras Fashafsheh contributed to conceptualization, methodology, study selection, quality assessment, data extraction, data analysis, writing—original draft, and writing—review and editing; and Ismail A. Elhaty contributed to conceptualization, writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Competing Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.