
Abstract
Introduction
Emergency nurses in Egypt face a high risk of workplace violence, but their subjective experiences are not well understood.
Objective
This study aimed to explore the causes, sources, types, and coping strategies related to workplace violence among emergency nurses in Egypt.
Methods
A descriptive qualitative design was used. Data were collected from 312 emergency nurses in an Egyptian hospital setting via an open-ended qualitative questionnaire and analyzed using directed content analysis.
Results
The primary cause of violence was work pressure (reported by 61% of nurses), driven by a lack of protection and staff shortages. The main sources of violence were external, from patients’ relatives (62%), and internal, from hierarchical disputes (18%). Verbal abuse was the most prevalent type of violence (78%), followed by physical violence (16%). The most common response was notifying supervisors (55%), though many nurses also reported significant emotional distress and avoidance coping.
Conclusion
This study reveals that workplace violence against emergency nurses in Egypt is driven by a dual threat of external-family and internal-organizational pressures. These findings underscore the need for targeted interventions that not only manage patient-family interactions but also address systemic organizational failures and internal hierarchical conflicts to ensure nurse safety.
Introduction
Workplace violence in emergency departments poses a significant challenge to healthcare systems worldwide, with emergency nurses facing heightened risks due to the high-pressure, unpredictable nature of their work (Chazel et al., 2023). This pervasive issue, encompassing physical, verbal, and psychological aggression, compromises nurse well-being, team morale, and patient care quality (Pich & Roche, 2020). Globally, up to 80% of nurses report experiencing some form of workplace violence during their careers, underscoring its widespread impact (Pich & Roche, 2020). In Egypt, where cultural and organizational factors may uniquely shape these experiences, there is a critical gap in qualitative research exploring nurses’ subjective encounters with violence (Alyousef & Alhamidi, 2022).
Emergency nurses are particularly vulnerable to aggression from patients, their families, or individuals with mental health challenges, driven by the emotional intensity and resource constraints of emergency settings (Alobaidan et al., 2024; Hassmiller & Wakefield, 2022). This violence contributes to job stress, burnout, and turnover intentions, threatening the sustainability of the nursing workforce (Stafford et al., 2022). While quantitative studies have documented prevalence rates, qualitative approaches are essential to capture the nuanced, context-specific experiences of nurses, particularly in understudied regions like Egypt (Bradshaw et al., 2017; El-Gazar et al., 2024). By employing a qualitative lens, this study aims to address this gap, offering insights into the causes, sources, types, and coping strategies of workplace violence in Egyptian emergency departments, informing culturally relevant interventions.
Review of Literature
Studies consistently identify emergency departments as high-risk environments for violence due to their unpredictable case mix, high patient volumes, and resource constraints (Ayasreh & Hayajneh, 2021). A systematic review of 18 studies found that verbal abuse is the most prevalent form of violence, reported by up to 90% of emergency nurses, followed by physical assaults, such as pushing or spitting (Ayasreh & Hayajneh, 2021). Contributing factors include understaffing, prolonged waiting times, and inadequate security measures, which exacerbate tensions between staff and patients or their families (Al-Qadi, 2021). These incidents have far-reaching consequences, including increased psychological distress, reduced job satisfaction, and higher turnover intentions, which compromise patient care quality (Li et al., 2021; Pariona-Cabrera et al., 2024). For instance, Li et al. (2021) demonstrated that exposure to violence mediates nurses’ intent to leave through diminished resilience, highlighting the need for organizational interventions.
Nurses’ responses to workplace violence vary, reflecting both individual coping mechanisms and systemic influences. Reporting incidents to supervisors is common but often ineffective due to lack of follow-up, leading to disillusionment (El-Gazar et al., 2023). Other strategies include avoidance, emotional suppression, or perseverance, which may mitigate immediate risks but contribute to long-term burnout (Speroni et al., 2014). A meta-analysis of interventions, found that de-escalation training and policy reforms, such as zero-tolerance frameworks, reduce violence incidents and improve nurse retention when supported by organizational commitment. However, the effectiveness of such interventions varies across contexts, underscoring the need for tailored approaches (Okubo et al., 2022).
While global research provides a robust foundation, studies in the Middle East, particularly Egypt, are limited, with most focusing on quantitative prevalence rather than qualitative depth (Alyousef & Alhamidi, 2022). Egypt's socio-cultural context significantly shapes workplace violence dynamics, influencing its forms, reporting behaviors, and institutional responses. Hierarchical healthcare structures prevalent in Egyptian hospitals often discourage nurses from reporting violence, as they may face blame or lack administrative support (Elsharkawy et al., 2025). Cultural norms emphasizing family involvement in patient care amplify risks, as relatives, driven by emotional distress or distrust in the system, frequently direct aggression toward nurses (El-Gazar & Zoromba, 2024). For example, a qualitative study found that family expectations of immediate care in emergencies lead to verbal and physical confrontations, particularly during peak hours (Elsharkawy et al., 2025). Moreover, societal stigma surrounding sensitive issues, such as sexual harassment or racial discrimination, suppresses reporting, as nurses fear retaliation or social judgment (Kafle et al., 2022; Velásquez, 2024). These factors create a culture of underreporting, with Al-Qadi (2021) noting that only 30% of Egyptian nurses formally document violent incidents, masking the issue's true scope.
The scarcity of qualitative research in Egypt represents a critical gap, as quantitative studies fail to capture the lived experiences of nurses navigating these cultural and organizational challenges. Qualitative approaches are particularly suited to explore how nurses perceive violence, interpret its causes, and develop coping strategies within Egypt's unique context (Bradshaw et al., 2017). For instance, Alyousef and Alhamidi (2022) highlighted that Saudi nurses’ experiences of violence are shaped by cultural expectations of deference, suggesting similar dynamics in Egypt. Additionally, institutional factors, such as limited training budgets and weak enforcement of violence prevention policies, exacerbate vulnerabilities in Egyptian hospitals (Atta et al., 2025; El-Gazar & Zoromba, 2021). Understanding these nuances is essential for developing interventions that address both universal and context-specific drivers of violence.
Therefore, a clear gap persists in the literature. While global research provides a robust quantitative foundation, there is a distinct lack of qualitative inquiry into the lived experiences of emergency nurses within the unique socio-cultural and organizational context of Egypt. Accordingly, the Egyptian context demands a deeper, qualitative lens to unpack the complexities of how violence is perceived, experienced, and managed by frontline nurses.
Objective of the Study
The research design—descriptive qualitative—has been meticulously chosen to align with the study's objectives, allowing for a rich, exploration of the lived experiences of emergency nurses facing workplace violence. The primary aim of this study is to explore and understand the multifaceted nature of workplace violence experienced by emergency nurses in Egypt, including its causes, sources, manifestations, and the coping strategies employed by nurses. This approach enables participants to articulate their experiences and perceptions freely, providing a detailed account of the complexity and dynamics of violence in healthcare settings. Such qualitative insights are instrumental in understanding the multifaceted nature of workplace violence, including the emotional, psychological, and professional repercussions for nurses. By capturing these detailed narratives, the current study not only contributes to a more nuanced understanding of workplace violence but also identifies potential areas for intervention, supporting the development of more effective policies and practices that address the root causes and impacts of such violence in emergency healthcare settings (Bradshaw et al., 2017; Lim et al., 2022).
Methods
Design
This study employed a descriptive qualitative design. Data were collected using an online, open-ended qualitative questionnaire designed to gather narrative responses from emergency nurses about their experiences with workplace violence. This approach was selected to capture a wide range of perspectives across a large sample, aligning with qualitative principles that prioritize richness of data over statistical generalization (Palinkas et al., 2015). While not a face-to-face interview, the use of a written, anonymous questionnaire was chosen to potentially facilitate more candid and detailed responses on a sensitive topic. The design's flexibility allowed participants to express their views freely, which is essential for exploring the multifaceted nature of violence in healthcare settings.
Setting
Data were collected from registered nurses employed in the Emergency Hospitals, XXX University a major healthcare provider in the Delta region, Egypt, which offers a diverse and dynamic setting for understanding the prevalence and nature of workplace violence in emergency care. The hospitals serve a diverse patient population and include both general and specialized emergency departments. Throughout the research, adherence to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines for qualitative research was rigorously maintained (Tong et al., 2007).
Sample and Recruitment
The study included 312 registered nurses working in the mentioned setting. A large sample was intentionally sought to capture a comprehensive breadth of experiences with a complex phenomenon and to approach data saturation, where new data does not generate new themes. Using a qualitative questionnaire with a large sample is methodologically supported for exploring a phenomenon across a heterogeneous population (Thomas et al., 2024). Using a purposive sampling strategy, participants were recruited from various departments and shift patterns (day and night) to ensure a diverse range of experiences and perspectives. Eligibility criteria required nurses to have at least six months of experience in the emergency department and a willingness to share their experiences.
Data Collection Instrument and Validity
An open-ended qualitative questionnaire, developed by the researchers for this study (see Supplemental File 1), was used for data collection. The term “questionnaire” is used to accurately reflect that data were collected via a self-administered Google Form rather than a verbal interview. The questionnaire's development was guided by a comprehensive review of workplace violence literature (Gacki-Smith et al., 2009; Hahn et al., 2008; Kumari et al., 2021). Preliminary discussions with emergency nursing staff to ensure questions were relevant and comprehensive. The questions were structured around key domains such as the causes, sources, types, and responses to violence to ensure all research questions were addressed. To ensure content validity and clarity, the questionnaire was pilot-tested with a small group of emergency nurses. Their feedback was used to refine the questions to be more evocative of rich, insightful narratives. This iterative process ensured the final instrument was grounded in existing research and tailored to the specific context of emergency nursing.
Study Procedure
Data were collected from June 2024 to September 2024. The final questionnaire was distributed via a Google Form link to all eligible emergency nurses within the hospital system. The first page of the form provided an overview of the study's purpose, informed participants of their right to withdraw at any time, and assured them of the anonymity and confidentiality of their data. Consent was implied by the voluntary completion and submission of the questionnaire.
Ethical Considerations
The study received approval from the Research Ethics Committee, Faculty of Nursing, XXXX University (approval number: 60-e) and adhered to the principles of the Declaration of Helsinki. Ensuring participants’ autonomy, confidentiality, and voluntary participation. All participants were informed of the study's purpose, their right to decline or withdraw, and were assured of anonymity. Given the sensitive topic, the introductory text acknowledged the potential for emotional distress and reminded participants of their right to skip any question. Furthermore, contact information for confidential psychological support services was provided to all participants should they experience distress from recalling these events.
Analysis
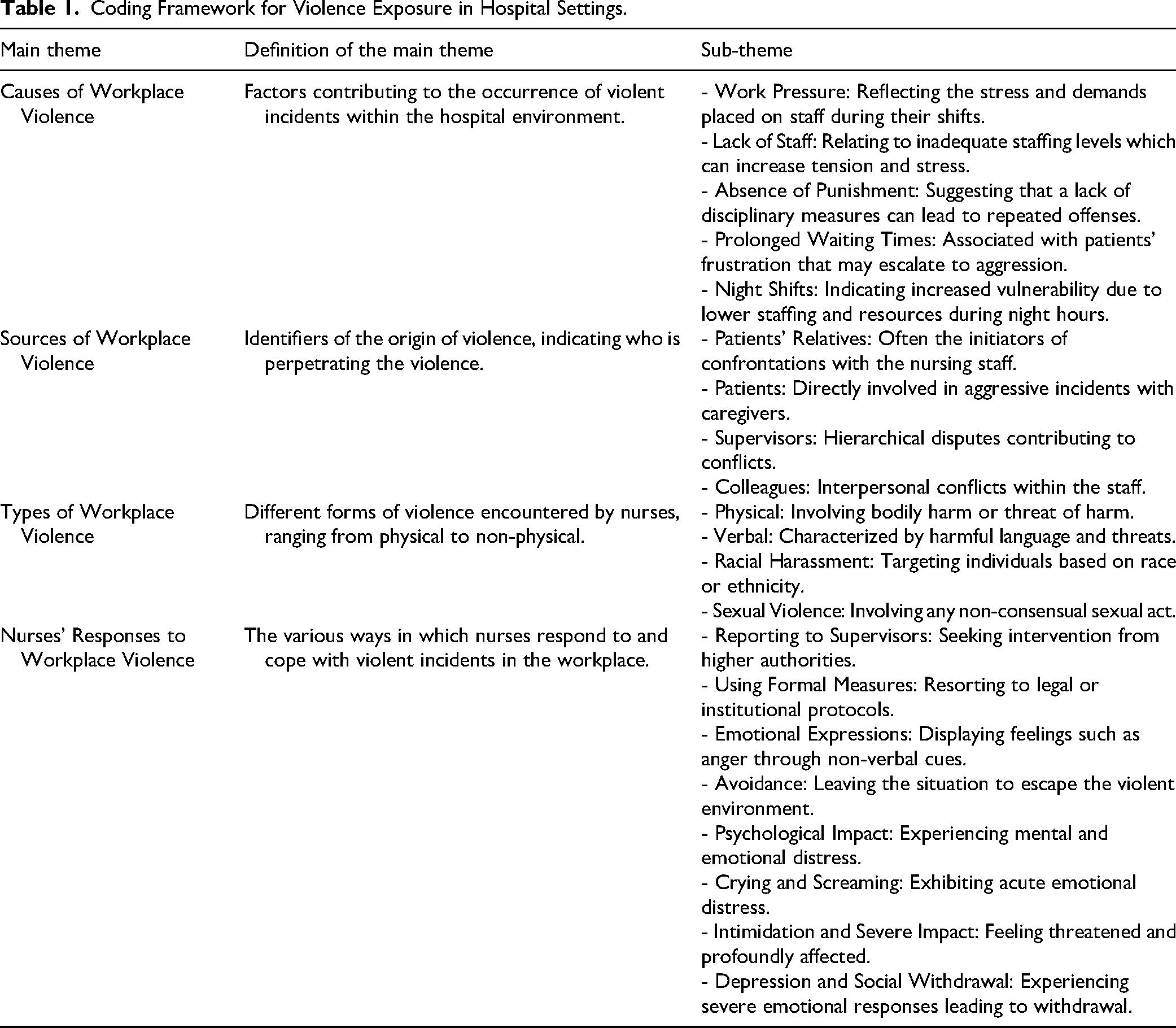
Data were analyzed using directed content analysis. This approach is fundamentally inductive, as all coding categories are derived directly from the text data; however, the process was guided by the study's research questions, which provided an initial framework for analysis (Hsieh & Shannon, 2005). The analysis followed the phases of preparation, organization, and reporting as described by Elo & Kyngäs, (2008). First, in the preparation phase, researchers read the responses multiple times to achieve immersion. In the organization phase, responses were exported from Google Forms to an Excel spreadsheet for cleaning and then imported into NVivo software. A team of researchers independently developed initial inductive codes from a subset of the data. The coding framework was then refined through discussion, and a final codebook was applied to the entire dataset. Related codes were grouped into sub-themes and then abstracted into overarching main themes corresponding to the research questions (Table 1).
Coding Framework for Violence Exposure in Hospital Settings.
To describe the prominence of themes within this large qualitative sample, the frequency of codes was quantified. This technique is used not for statistical generalization but to provide a descriptive summary of the most salient topics reported by participants, a common practice in qualitative descriptive research.
Trustworthiness
The trustworthiness of the study was established using the criteria of Lincoln and Guba.
Credibility
Credibility, or the confidence in the truth of the findings, was enhanced through multiple strategies.
Transferability
Transferability, or the degree to which findings can apply to other contexts, is supported by providing a thick description of the research setting and participants. This study details the context of a large university hospital system in Egypt, the purposive sampling strategy, a large and diverse sample of 312 emergency nurses, and the inclusion criteria. This allows readers to make informed judgments about the relevance of the findings to their own settings.
Dependability and Confirmability
Dependability (the stability of findings over time) and confirmability (the objectivity of the findings) were addressed through a detailed audit trail. Meticulous records were kept of the entire research process, including the raw data, the development of the codebook, coder discussions, and the NVivo analysis reports. This transparent process allows another researcher to follow the analytical steps. Furthermore, the researchers engaged in reflexivity through peer debriefings to acknowledge and challenge their preconceptions as healthcare professionals, thereby ensuring that the findings were grounded in the participants’ data rather than researcher biases.
Results
The qualitative data analysis identified four central themes concerning workplace violence experienced by emergency nurses: (1) causes of workplace violence, (2) sources of workplace violence, (3) types of workplace violence, and (4) nurses’ responses to workplace violence. These themes, detailed below with illustrative participant quotes, reflect the intricate interplay of organizational, systemic, and interpersonal factors that perpetuate violence in emergency departments.
Theme 1: Causes of Workplace Violence
Nurses overwhelmingly attributed workplace violence not to isolated incidents, but to a foundation of systemic and organizational stressors that create a volatile environment. The most frequently cited cause was immense work pressure, reported by 189 nurses. This pressure was compounded by a perceived lack of protection (153 nurses), an absence of punitive measures for aggressors (106 nurses), prolonged waiting times for patients (102 nurses), chronic staff shortages (95 nurses), and the heightened vulnerability of nocturnal working hours (52 nurses).
The intense, fast-paced nature of the emergency department was described as a battle. One nurse articulated this challenge: “Every shift feels like a battle against time and resources. The stress is overwhelming.” (Nurse 83) “When there are no consequences for aggression, it sends a message that such behavior is tolerated.” (Nurse 221)
Another nurse highlighted the direct link between understaffing and risk, stating, “We are so short-staffed, especially at night. It's not just stressful, it's dangerous. There is no one to call for help” (Nurse 145)
Theme 2: Sources of Workplace Violence
The analysis showed that violence originates from multiple sources, forcing nurses to navigate aggression from both external and internal fronts. The most common source by far was patients’ relatives (identified by 247 nurses), who are often acting out of fear and frustration. This was followed by hierarchical disputes with management (75 nurses), direct aggression from patients (74 nurses), and internal staff conflicts (45 nurses). One nurse described the dynamic with families: “The aggression from patients’ families can be intense. They often blame us for the system's failures.” (Nurse 276) “Disputes with management often escalate quickly. Their pressure only adds to the stress.” (Nurse 111)
This was echoed by another participant who felt that internal conflicts were just as damaging as external ones: “Sometimes the fight is not with the patients, but with your own colleagues or supervisors. It makes you feel completely alone” (Nurse 203)
This finding is critical, as it reveals that organizational tensions and internal power dynamics are themselves a source of workplace conflict, suggesting that mitigation strategies must address both patient-facing interactions and internal institutional culture.
Theme 3: Types of Workplace Violence
Nurses reported experiencing a wide spectrum of violence, from pervasive psychological abuse to direct physical assault. Verbal abuse was the most widespread form, reported by 287 nurses, highlighting its normalization within the emergency department. This was followed by physical violence (118 nurses). Less frequent but deeply impactful were instances of racial harassment (6 nurses) and sexual violence (2 nurses), which reveal intersectional dimensions of aggression. A nurse reflected on the lasting psychological toll of verbal abuse: “The verbal assaults can be just as damaging as physical ones. The words can haunt you.” (Nurse 17) “Being targeted for my race adds another layer of fear to my job. It's demeaning and exhausting.” (Nurse 117)
The pervasiveness of physical threats was also clear, as one nurse shared, “I was pushed against a wall by a patient's son just last week. I didn't even report it because I thought, ‘what's the point?’ It happens all the time. “ (Nurse 54)
These findings underscore the need for comprehensive prevention strategies that recognize and address the entire spectrum of violence, acknowledging the severe psychological burden that all forms of abuse place on healthcare workers.
Theme: Nurses’ Responses to Workplace Violence
In response to violence, nurses engaged in a range of behaviors that revealed a tension between relying on formal systems and resorting to personal coping mechanisms. The most common response was notifying supervisors (171 nurses), followed by pursuing other formal measures (145 nurses). However, these official actions were paralleled by responses indicating significant emotional impact and self-preservation, such as expressing frustration through facial expressions (102 nurses), avoiding the violent scene (78 nurses), and simply trying to continue duties despite emotional turmoil (74 nurses).
The reliance on reporting indicates a desire for institutional support, yet this was often met with disillusionment. As one nurse stated: “I always report incidents to my supervisor, but it often feels like it falls on deaf ears.” (Nurse 67) “There are times I've had to walk away from a situation. My safety comes first.” (Nurse 9)
The lasting psychological impact was a strong sub-theme, with one nurse stating, “I have anxiety now. Every time the door to the department opens loudly, I jump. You carry that fear home with you” (Nurse 198)
This dual-track response highlights a significant gap in organizational support, where nurses feel compelled to seek formal help but are ultimately forced to depend on their own internal coping resources to navigate a hostile work environment.
Demographic Considerations
Demographic variables such as age, gender, and years of experience were not explicitly collected in this study. However, the sample's diversity—drawn from multiple emergency departments and shift patterns—likely encompasses a broad range of demographic profiles. The lack of demographic-specific analysis limits the ability to assess their influence on violence experiences, though the consistency of themes across the large sample (n = 312) suggests that workplace violence is a pervasive issue transcending individual differences. Future studies could investigate demographic factors to elucidate their role in shaping nurses’ encounters with violence.
Discussion
This qualitative study provides a critical exploration of workplace violence experienced by 312 emergency nurses in a major Egyptian healthcare setting, directly addressing the aim to understand its multifaceted nature—encompassing causes, sources, types, and nurses’ coping strategies. Through content analysis, the findings reveal how systemic, organizational, and cultural factors converge to perpetuate violence, offering unique insights into Egypt's healthcare context while contributing to global efforts to protect nurses. The study's emphasis on work pressure as the primary cause, patients’ relatives as the dominant source, verbal abuse as the most prevalent type, and reliance on institutional reporting or personal coping strategies highlights both universal and context-specific challenges. By situating these findings within theoretical frameworks and international literature, this discussion critically evaluates their significance, limitations, and implications for practice and policy.
Causes of Workplace Violence
The study identified work pressure as the leading cause of workplace violence (189 nurses), followed by lack of protection, absence of punitive measures, prolonged waiting times, staff shortages, and nocturnal working hours. This finding corroborates prior research linking high-stress environments to increased violence, attributing it to systemic issues such as understaffing and resource scarcity (Lim et al., 2022). The unique emphasis on nocturnal working hours, however, suggests that temporal vulnerabilities exacerbate violence in Egypt's resource-constrained settings, a factor less prominent in high-resource contexts like Australia (Pich & Roche, 2020). This finding supports the Job Demands-Resources (JD-R) model, where excessive demands—such as understaffed night shifts—amplify conflict (Bakker et al., 2023). The absence of punitive measures reflects organizational policy gaps, consistent with Middle Eastern studies advocating for stronger safeguards (El-Gazar et al., 2024). Critically, these systemic drivers suggest that violence in Egypt is not merely interpersonal but rooted in structural deficiencies, necessitating reforms that address both universal stressors and local resource challenges.
Sources of Workplace Violence
Patients’ relatives were the primary source of violence (247 nurses), followed by hierarchical disputes with management, direct patient interactions, and internal staff conflicts. This predominance of family-driven aggression aligns with global evidence that emotional distress among relatives often manifests as violence toward healthcare staff (Abou-Abbas et al., 2023; Alyousef & Alhamidi, 2022). In Egypt, cultural norms emphasizing family involvement in care amplify this risk, contrasting with Western settings where patient-driven aggression is more common (Stafford et al., 2022). Hierarchical disputes with management, however, reveal a distinct organizational dynamic, supported by research on abusive supervision (Okubo et al., 2022). This suggests that Egypt's pronounced hierarchical healthcare culture fosters internal hostility, a finding less evident in flatter systems like those in Europe (Zoromba, Abousoliman et al., 2024). These dual sources—external and internal—highlight the study's contribution to understanding how cultural and organizational factors intersect to drive violence, urging interventions that address both community expectations and workplace dynamics in congruence with studies recommended adapting the workplace happiness model to include specific cultural and social considerations can enhance the effectiveness of psychosocial and cultural interventions (Aprilia et al., 2024; Porras Velasquez, 2024).
Types of Workplace Violence
Verbal abuse was the most reported type (287 nurses), followed by physical violence, racial harassment, and sexual violence. This echoes literature documenting the prevalence of verbal aggression in healthcare, often normalized and underreported (Pich & Roche, 2020), while the incidence of physical violence aligns with heightened risks faced by emergency nurses globally (Stafford et al., 2022). The low reporting of racial and sexual harassment, however, points to intersectional vulnerabilities suppressed by cultural stigma, a pattern more pronounced in Egypt than in Western contexts where reporting mechanisms are stronger (Alyousef & Alhamidi, 2022; Chazel et al., 2023). This challenges assumptions that violence is primarily physical, revealing a significant psychological burden that may be underaddressed in Egypt due to societal taboos. The study's documentation of these diverse forms underscores its role in exposing hidden dimensions of violence, necessitating culturally sensitive interventions to address psychological and discriminatory impacts.
Nurses’ Responses to Workplace Violence
Most nurses notified supervisors (171 nurses) or pursued formal measures (145 nurses), though many also reported emotional distress or relied on avoidance and perseverance. This reliance on institutional reporting reflects a need for organizational support, yet the emotional toll suggests deficiencies in current systems, consistent with studies noting inadequate post-incident care consistent with findings in Jordan (Al-Oweidat et al., 2023). In Egypt, hierarchical constraints may limit assertive responses, aligning with the Conservation of Resources (COR) theory, where nurses conserve emotional resources under stress (Hobfoll, 1989). Unlike high-resource settings offering debriefing (Zoromba, Abualruz et al., 2024), Egypt's limited psychological support forces reliance on personal coping, risking long-term burnout. This study's focus on coping strategies highlights their inadequacy in Egypt's context, contributing critical insights into the need for systemic support to enhance nurse resilience.
The study's findings resonate globally while offering distinct contributions shaped by Egypt's context. Work pressure and lack of protection mirror challenges in under-resourced systems worldwide (Lim et al., 2022), but the prominence of family-driven violence and hierarchical disputes reflects cultural and organizational nuances seen in Middle Eastern and Asian settings (Abou-Abbas et al., 2023; Li et al., 2021). Unlike European studies emphasizing patient aggression (Chazel et al., 2023), Egypt's findings highlight external (family) and internal (management) sources, enriching global perspectives on violence drivers. The underreporting of harassment, driven by stigma, parallels Middle Eastern research but contrasts with higher reporting in Western systems, underscoring the need for culturally tailored reporting mechanisms. By bridging local and global insights, this study enhances the international discourse on workplace violence prevention.
Strengths and Limitations
This study's strength lies in its large sample and qualitative depth, capturing nuanced experiences of workplace violence in Egypt. However, limitations include reliance on self-reported data, which may introduce bias due to underreporting, particularly of sexual violence or racial harassment, influenced by stigma or fear of retaliation. The single-site focus in Egypt restricts generalizability, as cultural and institutional dynamics—such as hierarchical structures—may not apply elsewhere. The descriptive qualitative design, while rich in narrative, cannot quantify prevalence or establish causality, limiting policy applications. The absence of demographic data (e.g., gender, age, years of experience) further constrains analysis of how these factors influence violence exposure or coping, as prior research suggests gender and experience shape vulnerability (Che Huei et al., 2020). Future studies should adopt mixed-methods approaches and include demographics to enhance generalizability and depth.
Implications
The findings offer actionable implications for clinical practice, policy, and education, tailored to Egypt's context yet applicable globally. To address work pressure and nocturnal vulnerabilities, hospitals should increase staffing, particularly for night shifts, and deploy trained security personnel, as supported by effective violence prevention programs. For family-driven violence, mandatory de-escalation and family communication training, proven effective in reducing aggression, should be implemented. To counter verbal abuse, zero-tolerance policies paired with awareness campaigns can shift cultural norms, while robust reporting mechanisms and legal protections are needed for physical and discriminatory violence. Psychological support, including accessible counseling and post-incident debriefing, is critical to enhance coping and reduce burnout, addressing gaps in Egypt's current systems. Educationally, nursing curricula should integrate violence prevention and resilience training. Hospitals must foster safety-oriented cultures, with leadership accountable for policy enforcement, ensuring sustainable reforms. These interventions, evaluated through ongoing research, can safeguard nurses’ well-being, improving patient care and organizational resilience in Egypt and similar settings.
Conclusions
This study provides an exploration of workplace violence against emergency nurses in an Egyptian healthcare setting, identifying key triggers, forms, sources, and coping strategies through a descriptive qualitative lens. The analysis reveals the pervasive nature of verbal and physical violence, driven by factors such as work pressure, staff shortages, and inadequate protections, with sources ranging from patients’ relatives to internal staff conflicts. Nurses’ responses reflect a diverse array of adaptive and reactive measures. More broadly, this research underscores the urgent need for systemic interventions to mitigate workplace violence, advocating for robust policies, enhanced training, and further studies to protect emergency nurses and strengthen healthcare systems. To advance prevention efforts, future research should prioritize the evaluation of specific strategies, such as de-escalation training, zero-tolerance policies, and enhanced security measures, within the Egyptian context. Additionally, studies exploring cultural and organizational barriers to implementing these strategies could provide critical insights for policymakers and hospital administrators. Longitudinal research assessing the long-term effectiveness of prevention measures in reducing workplace violence is also essential. These findings compel healthcare institutions and policymakers to act decisively, prioritizing nurse safety as a foundational element of quality patient care and a resilient healthcare workforce worldwide.
Supplemental Material
sj-docx-1-son-10.1177_23779608251363858 - Supplemental material for Experiences of Workplace Violence and Coping Strategies Among Emergency Nurses in Egypt: A Descriptive Qualitative Study
Supplemental material, sj-docx-1-son-10.1177_23779608251363858 for Experiences of Workplace Violence and Coping Strategies Among Emergency Nurses in Egypt: A Descriptive Qualitative Study by Mohamed Ali Zoromba, Mohamed Hussein Ramadan Atta, Sameer A. Alkubati, Shimmaa Elsayed and Naglaa Gamal Eldien Abdelhafez Hariedy, Asmaa Ali Ahmed Mohamed, Heba Emad El-Gazar in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251363858 - Supplemental material for Experiences of Workplace Violence and Coping Strategies Among Emergency Nurses in Egypt: A Descriptive Qualitative Study
Supplemental material, sj-docx-2-son-10.1177_23779608251363858 for Experiences of Workplace Violence and Coping Strategies Among Emergency Nurses in Egypt: A Descriptive Qualitative Study by Mohamed Ali Zoromba, Mohamed Hussein Ramadan Atta, Sameer A. Alkubati, Shimmaa Elsayed and Naglaa Gamal Eldien Abdelhafez Hariedy, Asmaa Ali Ahmed Mohamed, Heba Emad El-Gazar in SAGE Open Nursing
Footnotes
Acknowledgements
The authors would like to thank all nurses for their voluntary participation in the study. This study was supported via funding from Prince Sattam Bin Abdulaziz University (project number PSAU/2025/R/1446).
ORCID iDs
Author Contribution
MZ, MA, SE, and HE planned the study and made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. MZ, SA, NA, and AM were major contributors in writing and drafting the manuscript. MZ and MA were major contributors in writing the Discussion section. All authors given final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have agreed on the final version and meet at least one of the following criteria (recommended by the ICMJE):
1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; 2) drafting the article or revising it critically for important intellectual content.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.