
Abstract
Introduction
Vital signs monitoring is a common task for nursing and midwifery students during their clinical rotation. Therefore, it is important to evaluate the students’ attitudes toward this skill.
Objective
To evaluate the attitudes of nursing and midwifery students toward vital sign monitoring and identify the key factors that influence them.
Methods
A descriptive, correlational, cross-sectional research design was employed, utilizing an online self-administered questionnaire. The study participants were selected through a simple random sampling method. The translated V-scale instrument was used to assess the nursing students’ attitudes toward vital sign monitoring. Descriptive statistics were computed, and multivariate linear regression was employed for data analysis.
Results
The total number of participants in this study was 215 students. The study found that the mean score for students’ attitudes regarding vital sign monitoring was 3.17 (SD = 0.37). Notably, the communication subscale received the highest mean score of 4.16 (SD = 0.56). The workload subscale, on the other hand, had the lowest mean score, 2.37 (SD = 0.76). The backward stepwise regression revealed that academic programs such as midwifery (β = .146, t = 2.17, P < .05) and grade point average (GPA) (β = .172, t = 2.55, P < .05) are statistically significant predictors for student's attitudes toward vital signs monitoring. The adjusted R2 of .038 suggested that approximately 3.8% of the variance in attitude level toward vital signs monitoring was explained by the academic program of midwifery and GPA (R2 = .047, adj. R2 = .038, F(2, 212) = 5.271, P < .01).
Conclusion
The participating students in this research exhibited moderate attitudes toward vital sign monitoring. The most positive attitude was in the communication subscale, while the most negative attitude was in the workload subscale. We identified academic program variables like midwifery and GPA as significant predictors of students’ attitudes toward vital signs monitoring.
Introduction
Vital signs assessment constitutes a foundational nursing priority and an integral component of delivering safe and high-quality care (Elliott, 2021). It's considered crucial data to evaluate one's current state of health and underlying medical conditions (Jugović-Pavlović & Simin, 2023). Also, they are considered a necessary part of monitoring patients in hospitals (Brekke et al., 2019). The term “vital” is attributed to these parameters due to their critical role in initiating clinical evaluations (Sapra et al., 2025). The four primary vital signs encompass body temperature, pulse rate, respiration rate, and blood pressure (Kebe et al., 2020). They are the easiest, least expensive, and most crucial data acquired on hospitalized patients (Kellett & Sebat, 2017). Additionally, the process of measuring vital signs for patients often requires a duration of 5 min (Dall’Ora et al., 2021).
One of the fundamental tasks for nurses in hospitals is monitoring vital signs (Redfern et al., 2019). All patients need to have their vital signs regularly checked to gather the necessary information for identifying abrupt, serious, and life-threatening problems (Özsaban et al., 2022). Regularly checking vital signs helps prevent serious problems because unusual readings often happen before bad outcomes, and these can be caught with careful monitoring. However, several studies reported a deficiency in monitoring vital signs (Mok et al., 2015; Redfern et al., 2019; Saber & Khudhair, 2021). Previous studies have revealed a frequent neglect of vital signs monitoring (Kamio et al., 2018; Weenk et al., 2019). Neglect of monitoring vital signs resulted in patient death (Elliott & Endacott, 2022). Also, the primary cause of unnecessary fatalities in acute hospitals is insufficient clinical monitoring (Kamio et al., 2018). In addition, inadequate sets of vital signs observations may cause further delays in the detection of deterioration (Cardona-Morrell et al., 2016).
The number of nursing programs in Arab nations has expanded, helping to satisfy the growing demand for nurses (Sweileh et al., 2019). Moreover, a total of 5,318 nursing students are now registered at Jordan's 14 nursing faculties and 33 governmental hospitals (Jebreel, 2017). Vital signs monitoring is a frequently assigned nursing task during clinical rotations that engages nursing students (Alshehry et al., 2021). Nursing schools begin instructing nursing students about vital signs as early as the first year. The noninvasive nature of vital sign procedures often grants nursing students autonomy in performing vital sign monitoring on patients, with minimal guidance from clinical instructors or nurses (Alshehry et al., 2021). However, the competence of nursing students in identifying early signs of patient deterioration and their timeliness in reporting abnormal vital signs to experienced healthcare professionals are being criticized (Leonard & Kyriacos, 2015). Additionally, the attitudes of nursing and midwifery students toward vital signs monitoring remain unknown. Given how important it is to monitor vital signs quickly and accurately to spot when a patient is getting worse, nursing and midwifery students need to have enough knowledge, the right attitudes, and the skills to monitor vital signs and recognize deterioration (Alshehry et al., 2021).
Literature Review
Several studies identified specific factors that could influence the attitudes of nursing and midwifery students toward monitoring vital signs. Jugović-Pavlović and Simin (2023) found that gender and degree of qualification were the main factors affecting nursing student's attitudes toward vital signs monitoring. In addition, Alshehry et al. (2021) identified that university, age, gender, academic year level, and perceived knowledge significantly influenced nursing students’ attitudes toward vital signs monitoring. However, these studies advocate for additional research to identify factors that impact nursing and midwifery students’ attitudes toward vital sign monitoring.
The proposed research aims to advance our comprehension of nursing and midwifery students’ attitudes toward vital sign monitoring. In addition, the outcomes would improve university faculty members’ understanding of the necessary measures to enhance their proficiency in knowledge and skills related to vital signs. Furthermore, this research will identify specific areas within vital signs that warrant greater emphasis in the design of educational programs for nursing and midwifery students. Based on the available information, this study aims to evaluate the attitudes of nursing and midwifery students toward vital sign monitoring and identify the key factors that influence them.
Methods
Design
A descriptive, correlational, cross-sectional research design was employed, utilizing an online self-administered questionnaire, to evaluate the attitudes of nursing and midwifery students toward vital sign monitoring and identify the key factors that influence them at Al-Balqa Applied University in Jordan. This research was carried out among Jordanian nursing and midwifery students who were aged 18 years or older. The data collection spanned the period from November 1, 2023 to December 3, 2023.
Sample
The study employed a probability random sampling method to select participants. The researcher entered a list of potential participants (the sample frame) into a computer. The researcher then electronically selected the students at random from a complete list using a random number generator, and only these selected individuals received the survey link. Based on a medium effect size, a significance level of .05, and a power level of 0.8, the estimated sample size needed was at least 103 participants for multiple regression analysis with seven predictors (Faul et al., 2009). However, to prepare for possible dropouts or incomplete answers, more participants were included, leading to an expected total of 124 students. However, we implemented oversampling to account for attrition or incomplete responses, resulting in an anticipated total of 124 students.
Eligibility criteria included willingness and ability to participate, enrollment as nursing and midwifery students, being 18 years or older, having internet access, and ability to read and understand the Arabic language. Freshman students were excluded due to their limited exposure to clinical courses.
Measures
The initial section of the instrument encompassed demographic data (age, gender, marital status, academic program, academic level, grade point average [GPA[, and residency). The second session is the V-scale instrument, which was developed by Mok et al. (2015). However, the present study utilized the Arabic version of the V-scale instrument (Alnjadat et al., 2025).
The instrument comprises 16 items that are distributed across five domains: workload (four items), communication (three items), technology (four items), knowledge (three items), and key indicators (two items) (Alnjadat et al., 2025). Three items in the tool were revised to fit nursing students (Alshehry et al., 2021). The modified tool revealed acceptable validity after testing by five experts (Content Validity Index [CVI] = 1) and acceptable reliability after data collection by 30 nursing students (Cronbach's alpha = .88; Alshehry et al., 2021).
The response scale employs a 5-point Likert scale (ranging from 1 to 5), where the values correspond to the following: 1 = strongly disagree, 2 = disagree, 3 = neither, 4 = agree, and 5 = strongly agree. By summing the responses for each item, the total score is computed. The potential score range spans from 16 (lowest) to 80 (highest). A lower score indicates a negative attitude toward vital sign monitoring, while a higher score signifies a positive attitude (Ertuğ, 2018; Mok et al., 2015). However, to simplify the interpretation of the results, the total attitude level will be categorized into three categories. If the mean attitude score falls below 1.7, it will be considered a negative attitude level; if the mean attitude score lies between 1.8 and 3.4, it will be considered a moderate attitude level; and if the mean attitude score exceeds 3.5, it will be considered a positive attitude level.
The psychometric testing results for the original instrument demonstrated acceptable validity and reliability (Cronbach's alpha = .71, Intraclass Correlation Coefficient [ICC] = 0.85) (Mok et al., 2015). Additionally, researchers conducted a pilot study to evaluate the readability of the Arabic version of the V-scale instrument. In addition, the psychometric properties of the Arabic version of the V-scale instrument showed that the obtained factor structure explained 54.81% of the variance, and all the fitting indices met the judgment criteria (Alnjadat et al., 2025). The reliability test for the Arabic version of the V-scale instrument showed that the Cronbach's alpha values for the five subscales were between .72 and .86, and the overall Cronbach's alpha for the entire scale was above .9 (Alnjadat et al., 2025).
Ethical Considerations and Consent to Participate
Ethical approval was secured from the Institutional Review Board (IRB) at Al-Balqa Applied University under the reference number (100/8/2023/2024) for data collection. Informed consent was sought online from each participant. The research team comprehensively explained the study's objectives and anticipated outcomes. Participants were assured of voluntary participation, with the right to decline or withdraw at any point without the need for justification and without facing any penalties. Furthermore, the confidentiality and anonymity of the participants were preserved throughout the whole study, encompassing both data collection and analysis. Moreover, the researchers included their email addresses on the informed consent form to facilitate responses to participant inquiries and to deliver study data upon request.
Data Collection
The participants were selected through a simple random sampling procedure. The study tool comprised of a self-administered questionnaire. Demographic data and the main questionnaire were collected. The data was collected using Google Forms and subsequently exported as an Excel file. The researchers provided a Google Form link containing the study survey to the study participants who met the inclusion requirements through the Microsoft Teams class. The data collection spanned from November 1, 2023 until December 3, 2023. The online Google Forms ensured complete anonymity of all submitted responses, with no gathering of any identifiable data. To preserve participant confidentiality, the data obtained from the questionnaires was coded, and only the researchers were granted permission to view it. Finally, the data was securely stored in a computer that required a password for access.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS), version 27, was employed for data analysis. Descriptive statistics, including minimum and maximum scores, frequency, percentages, mean, and standard deviation, were utilized to describe and analyze demographic data based on the level of measurement. Additionally, inferential statistics, specifically multivariate backward stepwise regression, were employed to identify factors influencing nursing and midwifery students’ attitudes toward vital sign monitoring. We examined the assumptions of the regression analysis by looking at scatter diagrams of residuals versus projected residuals and normal probability plots of residuals.
Results
Participant's Demographic Characteristics
The total number of participants in the present study was 215 students. The mean age of participating students was (M = 20.25, SD = 1), and the mean GPA was (M = 70.61, SD = 8.01) (Table 1). The majority of participants were female (n = 182, 84.7%), single (n = 192, 89.3%), studying nursing (n = 144, 67%), and in the second year of studying (n = 181, 84.2%). Furthermore, more than half of the research participants residing in villages accounted for over half of the total sample (n = 119, 55.3%).
Participants Demographic Characteristics (N = 215).

Note. M = mean; SD = standard deviation; GPA = grade point average.
Descriptive Statistics for the Attitudes Subscales
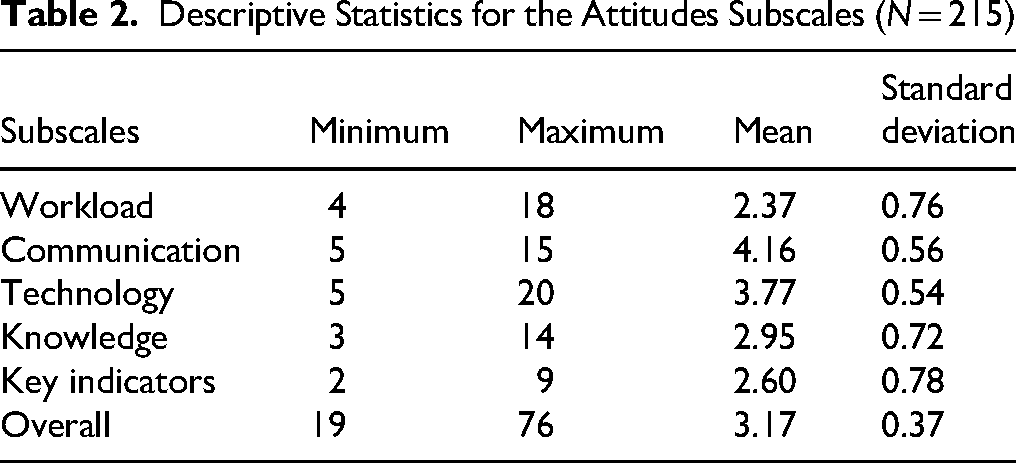
The minimum score among students was 19, while the maximum score was 76. The overall score for students’ attitudes toward vital signs monitoring was 3.17, with a standard deviation of 0.37. The communication subscale had the highest mean score, with a value of 4.16 and a standard deviation of 0.56. Conversely, the workload subscale had the lowest average score (M = 2.37, SD = 0.76), as shown in Table 2.
Descriptive Statistics for the Attitudes Subscales (N = 215).
Students Attitudes Toward Vital Signs Monitoring
Among the participants of this study, the majority (41.9%, n = 90) on the workload subscale expressed disagreement with feeling overwhelmed by measurements of the vital signs frequently for their patients. In contrast, the lowest percentage of participants reported that the vital signs monitoring is a boring task (n = 3, 1.4%) (Table 3).
Students Attitude Toward Vital Signs Monitoring (N = 215).

Strongly disagree.
Disagree.
Neutral.
Agree.
Strongly agree.
More than two-thirds of students in the communication subscale agreed that blood pressure is often the first parameter that reflects abnormality when a patient deteriorates (n = 136, 63.3%). In contrast, no students expressed strong disagreement regarding their confidence in reporting deteriorating vital signs in a manner that would prompt the team registered nurse (RN) in charge or clinical instructor to review the patient (n = 0, 0%).
More than half of participating students in the technology subscale agree that they can relate vital signs readings to the physiology and pathophysiology of presenting diseases (n = 127, 59.1%). On the other hand, only three students (1.4%) strongly disagree that SpO2 is a more reliable indicator in reflecting early signs of respiratory dysfunction than respiratory rate.
More than one-third of participants in the knowledge subscale disagree that electronic vitals monitoring results in casual monitoring (n = 85, 39.5%). Conversely, only five participants (2.3%) strongly agree that electronic vitals monitoring results in casual monitoring.
Less than half of the participating students in the key indicators subscale disagree that the respiratory rate value is the least important sign of deterioration (n = 103, 47.9%). On the other hand, only four students (1.9%) strongly agree that the respiratory rate value is the least important sign of deterioration.
Factors Affecting Students Attitude Toward Vital Signs Monitoring
Backward stepwise regression was conducted to refine the predictive model for age, gender, marital status, academic program, academic level, GPA, and residency as potential predictors. The analysis utilized a backward elimination method, with a criterion set at a probability of F-to-remove greater than or equal to 0.100. The final model, entered with academic program and GPA exhibited a high degree of predictability for attitudes level toward vital signs monitoring.
The results revealed that the final model was statistically significant in predicting attitude levels toward vital signs monitoring (F(2, 212) = 5.271, P < .01). The standardized coefficients indicated significant contributions from academic programs such as midwifery (β = .146, t = 2.17, P < .05) and GPA (β = .172, t = 2.55, P < .05). The adjusted R2 of .038 showed that about 3.8% of the variance in the attitude levels toward vital signs monitoring was explained by factors like academic programs, including midwifery, and GPA (Table 4).
Factors Affecting Students Attitude Toward Vital Signs Monitoring (N = 215).

Note. Model summary: R2 = .047, adj. R2 = .038, F(2, 212) = 5.271, P < .01.
B = unstandardized beta; SE B = standard error for the unstandardized beta; β = standardized beta; GPA = grade point average.
Discussion
Vital signs monitoring constitutes a frequently assigned task for nursing and midwifery students during their clinical rotations. However, there is a scarcity of evidence addressing the views of nursing students toward the monitoring of patient's vital signs (Jugović-Pavlović & Simin, 2023). Therefore, this study aims to evaluate the attitudes of nursing and midwifery students toward vital sign monitoring and identify the key factors that influence them.
The overall mean score of students’ attitudes toward vital sign monitoring was 3.17 out of 5, which can be interpreted as a moderate attitude level. This result could be related to inadequate knowledge regarding vital signs monitoring, as 41.9% of participants reported that they agree and strongly agree that their knowledge in interpreting vital signs to identify clinical deterioration is limited. Furthermore, we can attribute these findings to insufficient experience in clinical practice. Nevertheless, a previous study indicated the potential for students to lack enough guidance and oversight in monitoring vital signs throughout their clinical rotation (Alshehry et al., 2021; Jugović-Pavlović & Simin, 2023). In addition, the results could be explained by a lack of awareness of the importance of vital signs monitoring on quality of care and patient safety. These findings are consistent with a previous study that found poor-to-moderate attitudes among nursing students toward vital signs monitoring (Alshehry et al., 2021). In contrast, a previous study reported that the attitude of nursing students toward vital signs monitoring was ambivalent (Jugović-Pavlović & Simin, 2023).
The current study results revealed that the highest mean score was for the communication subscale. About 192 (91.2%) of nursing students agree and strongly agree to report deteriorating vitals to the team RN in charge or clinical instructor to review the patient. However, this result is expected since nursing students are instructed to report any aberrant vital signs or changes in the client's vital signs to the clinical instructor or the nurse on duty for reassessment and appropriate intervention. This result is similar to previous studies that found high scores in the communication subscale (Alshehry et al., 2021; Jugović-Pavlović & Simin, 2023; Mok et al., 2015).
In contrast, the lowest mean score was for the workload subscale, which is a favorable result. However, the highest percentage of participants in the workload subscale disagree that they are feeling overwhelmed to complete the different frequencies of vital signs collection of their patients. Additionally, only 25 students (11.6%) agree or strongly agree that performing vital signs monitoring is time-consuming. Furthermore, 46 students (21.4%) reported that they find vital signs monitoring to be a boring task. This result may be due to students seeing vital signs monitoring as an extra task in addition to their other clinical duties. However, students in the clinical setting perform other duties, such as blood extraction, medication preparation, and administration, and also perform electrocardiograms. Furthermore, this finding could be related to the fact that some students might consider noninvasive techniques to be beyond the scope of necessary abilities to be obtained during their nursing and midwifery degree.
In the current study, the highest percentage of students agreed that blood pressure is often the first parameter that reflects abnormality when a patient deteriorates. These results could be related to a lack of knowledge regarding pathophysiology and body compensatory mechanisms. However, an earlier systematic review demonstrated that respiratory rate, rather than blood pressure or oxygen saturation, was the most reliable indicator of patient deterioration (Brekke et al., 2019). This finding is consistent with a previous study, which found that most nurses report blood pressure is often the first parameter that reflects abnormality when a patient deteriorates (Alshehry et al., 2021; Jugović-Pavlović & Simin, 2023; Mok et al., 2015).
More than half of participating students in the technology subscale agree that they can relate vital signs readings to the physiology and pathophysiology of presenting diseases. Also, less than half of the participating students in the key indicators subscale disagree that the respiratory rate value is the least important sign of deterioration. This result could be related to the fact that the majority of study participants are in their second year of studying, and in this year, the nursing and midwifery students completed the physiology and pathophysiology courses. Additionally, other educational materials provided by universities to nursing and midwifery students, including medical-surgical courses, could assist these students in connecting vital sign readings to specific diseases.
More than one-third of participants in the knowledge subscale disagree that electronic vitals monitoring results in casual monitoring. Conversely, only five participants strongly agree that electronic vitals monitoring results in casual monitoring. These findings suggest a deficiency in nursing and midwifery students’ knowledge and attitudes regarding the significance and appropriate utilization of technology, specifically pulse oximeters for assessing vital signs. Therefore, this finding implies the need for training sessions for nursing and midwifery students regarding the utilization of electronic vital signs devices in patient monitoring. This result goes against an earlier study that showed most students mistakenly agreed that electronic vital signs monitoring was just casual monitoring (Alshehry et al., 2021).
The present study revealed that approximately 3.8% of the variance in attitude level toward vital signs monitoring was explained by academic program, such as midwifery, and GPA. This low explanatory power could be related to the presence of some variables that were not examined in this research, such as motivation, self-efficacy, prior experience with patient care, and availability of simulation labs. Also, this finding could be related to the homogeneity of the sample, meaning that the sample was taken from only one university. This result highlights the importance of addressing these variables in future studies in different settings.
The current study results revealed a significant positive relationship between academic programs such as midwifery, GPA, and attitudes toward vital signs monitoring. This result could be explained by the fact that midwives have greater expertise in monitoring vital signs, particularly for pregnant mothers and babies, who may differ from other patients in terms of physiological characteristics and risk factors (Royal College of Nursing, 2017). Also, midwives may have a more positive perception of the value and importance of vital signs monitoring (Quayle, 2020). In addition, they may have more effective communication and teamwork skills in vital signs monitoring.
The current study predicts a positive relationship between GPA and attitudes toward vital signs monitoring. However, the GPA of nursing students indicates their level of competence and skills in measuring and interpreting vital signs, which may impact their confidence and willingness to perform these skills. In addition, GPA is a reflection of a nursing student's academic success and performance, which may impact how important they believe vital sign monitoring is for patient care and safety.
These results contradict a previous study, which found age, gender, university, academic year, and perceived knowledge as significant predictors of the student's attitudes toward vital signs monitoring (Alshehry et al., 2021; Jugović-Pavlović & Simin, 2023). In addition, a previous study found that degree qualification, level of experience, and working in a general ward with a specialty were predictors of a positive attitude toward vital signs monitoring among respondents (Mok et al., 2015).
Strengths and Limitations
This is the first study that assesses nursing and midwifery students’ attitudes toward vital sign monitoring in Jordan. However, this study has some limitations. First, it only involved nursing and midwifery students from a single university in Jordan, which may limit the applicability of the results to other contexts. Second, it used self-administered online questionnaires, which may introduce bias due to the participants’ tendency to choose the correct answer rather than their honest opinion. Third, using simple random sampling may not represent the whole population of nursing and midwifery students. Future research should expand the sample to include nursing and midwifery students from different universities and geographic regions to increase the generalizability of the findings. Also, conducting future studies using stratified random sampling might represent the whole population of nursing and midwifery students. Additionally, future research should include exploration of personal and clinical-related variables and their relationship with nursing and midwifery students’ attitudes toward vital signs monitoring. Moreover, future studies should adopt a mixed-method exploratory design to further investigate the nursing and midwifery students’ attitudes toward vital signs monitoring.
Implications for Practice
The findings of this study highlighted the need for curriculum enhancement and training interventions to nursing and midwifery students regarding vital signs assessment and physiological indicators of clinical deterioration. Also, a comprehensive grasp of physiological compensatory mechanisms and the underlying pathophysiology driving changes in vital signs is essential for nursing students to improve their clinical reasoning skills in interpreting early signs of clinical decline. However, educational efforts should emphasize the identification of initial indicators of clinical deterioration and highlight the critical role of vital signs examination in early detection. In addition, educational resources pertaining to vital signs should be strengthened in both theoretical and practical nursing courses. Moreover, during clinical rotations, nursing students would benefit from additional guidance provided by clinical instructors, nurses, and hospital staff. This supplementary support helps foster positive attitudes toward vital signs monitoring.
Conclusion
The present study evaluated the nursing and midwifery students’ attitudes toward vital signs monitoring. The participating students demonstrated moderate attitudes in this regard. Notably, the communication subscale exhibited the most positive attitude, while the workload subscale revealed the most negative attitude. Furthermore, the variables of academic programs, such as midwifery and GPA, emerged as significant predictors of students’ attitudes toward vital sign monitoring.
Footnotes
Acknowledgments
We would like to express special thanks for all nursing and midwifery students who participated in this study.
Ethical Considerations
Ethical approval was secured from the Institutional Review Board (IRB) at Al-Balqa Applied University under the reference number (100/8/2023/2024) for data collection.
Consent to Participate
Informed consent was sought online from each participant. The research team comprehensively explained the study's objectives and anticipated outcomes. Participants were assured of voluntary participation, with the right to decline or withdraw at any point without the need for justification and without facing any penalties. Furthermore, the confidentiality and anonymity of the participants were preserved throughout the whole study, encompassing both data collection and analysis. Moreover, the researchers included their email addresses on the informed consent form to facilitate responses to participant inquiries and to deliver study data upon request.
Authors’ Contributions
All authors contributed significantly to the work reported, encompassing conception, study design, execution, data acquisition, analysis and interpretation, and other relevant areas. They actively participated in drafting, revising, and critically reviewing the article. Furthermore, they provided final approval for the version to be published and reached a consensus on the journal selection for submission. Each author accepts accountability for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.