
Abstract
Introduction
Sepsis is an emergency condition that necessitates immediate and appropriate nursing interventions for improving patient outcomes. Nurses have an essential role to play in recognizing the early warning signs of sepsis, implementing timely healthcare treatments, and providing comprehensive care to enhance patient outcomes. This study examines the barriers and facilitators affecting the implementation of the Sepsis Six protocol among nurses in acute care settings in Jordan.
Objectives
This study aimed to identify nurses’ perceived barriers and facilitators affecting their implementation of the Sepsis Six guidelines in acute care settings in Jordan.
Methods
This cross-sectional descriptive study was conducted among a convenience sample of 180 nurses working in acute care settings (i.e., the ICU, CCU, ED, burns unit, and dialysis unit) at a university hospital. An online survey from a previous study was used to evaluate the nurses’ perceived barriers and facilitators affecting their implementation of the Sepsis Six guidelines in acute care settings.
Results
This study revealed that the main barriers facing the critical care nurses were environmental, which included lack of time, lack of sufficient staffing, and lack of available beds. Meanwhile, the main facilitators were emotional and intentional. For example, the nurses believed all of the Sepsis Six steps and guidelines to be very important for improving patient outcomes and decreasing sepsis-related complications.
Conclusion
This study revealed that barriers related to knowledge, environment, and resources can affect nurses’ compliance with sepsis guidelines. On the other hand, the findings revealed many strategies and facilitators which can improve nurses’ compliance with these guidelines and hence improve patient outcomes. These facilitators include ongoing education and training, the availability of resources, and effective teamwork and sepsis-related communication. However, further research is required to further investigate the barriers and facilitators that can affect nurses’ adherence to sepsis guidelines.
Introduction
Sepsis remains a major global health challenge, contributing to significant morbidity and mortality (WHO, 2024). According to the World Health Organization (WHO), sepsis affects approximately 48.9 million people annually, leading to 11 million deaths worldwide (Rudd et al., 2020). While high-income countries have established structured sepsis protocols, limited data exist on the burden and management of sepsis in low-income countries, including Jordan.
In Jordan, the prevalence of sepsis corresponds with global estimates; with 48.7% of patients admitted to intensive care units (ICUs) developing sepsis and 51.3% experiencing septic shock (Al Omar et al., 2021). Sepsis-related mortality in Jordan is significantly high, reaching 57.8% compared to 6.0% in non-septic ICU patients (Abu-Humaidan et al., 2021). Additionally, sepsis survivors may experience long-term complications, including functional and cognitive deficits, recurrent hospitalization, coagulopathy, sepsis-induced immunosuppression, acute renal injury, acute respiratory distress, cardiac dysfunction, and increased healthcare expenses (Hajj et al., 2018). The economic burden of sepsis is substantial, with readmission costs exceeding $1.1 billion globally (Goodwin et al., 2015). Data on sepsis and the epidemiology of sepsis among adult patients in Jordan are lacking (Al Omar et al., 2021). This underscores the need for more research, enhanced awareness and context-specific interventions to address the global burden of sepsis (La Via et al., 2024).
Despite international recommendations for early sepsis recognition and management, adherence to standardized protocols remains inconsistent. Several sepsis management protocols have been recognized as effective guidelines for timely management; however, their implementation is influenced by multiple barriers and facilitators.
Literature Review
Sepsis requires rapid identification and therapy to prevent its high morbidity and mortality rates (La Via et al., 2024). Research indicates that sepsis significantly increases nurses’ workloads, accounting for 22.8% of total workload variance (Alıcı & Öztürk Birge, 2024) and requiring an average care duration of 1.8 h due to the use of antibiotics, vasopressors, and invasive mechanical ventilation (Alıcı & Öztürk Birge, 2024). Nurses play an important role in identifying sepsis and providing rapid therapy, particularly in acute care settings (Rababa et al., 2022). Implementing evidence-based sepsis recommendations improves early diagnosis and management, lowering treatment costs and morbidity and fatality rates (Streitova et al., 2024). The Surviving Sepsis Campaign (SSC) produced six sepsis guidelines (the Sepsis Six), which include checking blood culture and lactate levels and providing broad-spectrum antibiotics, intravenous fluid, oxygen, and vasopressors (Hu et al., 2020).
Previous studies have shown that adherence to evidence-based sepsis recommendations can reduce mortality rates and improve patient outcomes (Frank et al., 2023). The timely application of these guidelines has been linked to decreased death rates among ICU patients with sepsis (Hu et al., 2020), while an evidence-based approach also lowers readmission rates (Jacobs, 2020). By improving the early detection and prompt management of sepsis, lowering patient morbidity and mortality, and raising overall quality of care, Spoon et al. (2020) reported that the adoption of standardized sepsis guidelines greatly improved nurse-patient outcomes. According to their study, nurses are more likely to act quickly and efficiently when they are following evidence-based protocols, which directly improve clinical outcomes. Additionally, following these recommendations was linked to improved consistency and confidence in nursing practice. Gustad et al. (2024), for instance, found that nurses who used structured monitoring tools, like observation sheets and systematic vital sign measurement protocols, were able to identify deterioration indicators sooner. Better coordination and quicker physician intervention in sepsis care were made possible by this proactive monitoring.
However, a survey conducted among nurses at a Swiss medical institution found a lack of awareness and knowledge about sepsis, indicating a need for rapid and continued educational interventions (Regina et al., 2023). Regular training can improve care quality and raise awareness of sepsis prevention among ICU nursing staff (Streitova et al., 2024). A significant barrier to implementing evidence-based sepsis recommendations is the lack of knowledge among nurses (Muratkoc, 2018). Other challenges include work environment issues such as insufficient reinforcement and motivation, severe workload, inadequate staffing, and resource shortages (Mosavianpour et al., 2016; Muratkoc, 2018; Roberts et al., 2017).
Promoting early diagnosis and rapid management of sepsis in acute care settings is essential, along with ensuring the appropriateness and reliability of nursing care. Recognizing barriers and facilitators to applying sepsis recommendations is crucial for improving adherence and enhancing patient outcomes (Mosavianpour et al., 2016; Roberts et al., 2017). Studies have identified several challenges and facilitators to applying sepsis guidelines in acute care settings in the West (Mosavianpour et al., 2016; Muratkoc, 2018; Roberts et al., 2017). However, in developing countries, inadequate adherence to sepsis standards remains an unresolved problem requiring further research (Streitova et al., 2024). To date, no studies have analyzed the barriers to and facilitators of sepsis assessment and management among ICU nurses in Jordan. Therefore, this study aimed to identify nurses’ perceived barriers and facilitators affecting their application of the Sepsis Six guidelines in the acute care units at a selected hospital in Jordan. Understanding these dynamics is essential for optimizing patient outcomes and informing policy reforms in Jordanian healthcare settings.
Methods
Design
This cross-sectional descriptive study was conducted on nurses working in adult critical care units [ICU, coronary care unit (CCU), emergency department (ED), burns unit, and dialysis unit] at a selected university hospital in Jordan. This study was carried out in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to promote transparency and rigor in the reporting of its methodology and findings.
Research Questions
What are the perceived barriers and facilitators among nurses to implementing the Sepsis Six Performance Bundle in acute care settings in Jordan?
Sample
A convenience sample of 180 nurses was recruited in the current study. A total of 220 critical care nurses work at the hospital, and the target sample size for this study was over 80% of the total population. Convenience sampling was employed to obtain a large sample within the limited time allowed for data collection in the study setting. Additional factors that influenced the choice of convenience sampling included the limitations of variation, geographic proximity, and the accessibility of participants for data collection. The sample size was calculated using G* power analysis, with a significance level of 0.05, a statistical power level of 0.8, and a medium effect size.
Inclusion Criteria
The inclusion criteria were all nurses who had been working in adult critical care units (ICU, coronary care unit (CCU), emergency department (ED), burns unit, and dialysis unit) at a selected university hospital in Jordan for at least one year.
Exclusion Criteria
Nurses were included if they had been working in the adult critical care units (i.e., ICUs, CCUs, the ED, burn units, and dialysis unit) at the selected hospital for at least one year. Nurses were excluded if they worked in medical-surgical floors or pediatric units, or if they had less than one year of experience in the adult critical care units.
Instrumentation
The current study utilized an online survey adopted from a previous study (Muratkoc, 2018; Roberts et al., 2017). The survey consists of three parts, with the first part including five questions about demographic information such as age, gender, and marital status. This type of demographic data collection facilitates a thorough examination of the sample's attributes and improves the interpretability of results by spotting possible differences in attitudes, perceptions, and clinical procedures among various nursing workforce subgroups (Polit & Beck, 2021). In particular, incorporating marital status enables researchers to investigate whether social and personal factors, like work-life balance, family obligations, or emotional support networks, may impact nurses’ motivation, stress levels, or time availability, all of which can impact their use of guideline-based care (Yildirim & Aycan, 2008). Previous studies have demonstrated that individual variations in demographic and psychosocial characteristics can influence how receptive medical professionals are to novel clinical protocols, such as those pertaining to time-sensitive interventions like the Sepsis Six bundle (Roberts et al., 2017). As a result, gathering marital status is more than just a descriptive tool; it may also identify key moderators or mediators in the adoption of evidence-based practices, facilitating the creation of more specialized support or training programs. The second part includes 54 questions related to perceived barriers to and facilitators of applying sepsis guidelines, and each of the 54 questions comprises two opposing statements rated on a 5-point Likert scale ranging from (1) very unimportant to (5) very important (Roberts et al., 2017). Finally, the third part includes 7 close-ended questions, two related to the identification and management of sepsis guidelines and five related to resources, education, and skills. Four nurses with expertise in sepsis reviewed the questionnaire to check for face and content validity, and the questionnaire was then piloted on 10 nurses, who were excluded from the primary study, to ensure the clarity of the questionnaire items.
Data Collection Procedure
The researcher met with the selected hospital's nursing manager to discuss the eligibility criteria for participation and prepare a list of eligible participants and their emails. All eligible nurses were invited to participate through an invitation email, which included the aims of the study, a brief explanation of the study, and the rights and responsibilities of the participants. This was followed by a reminder email two weeks later to increase the response rate. All nurses who accepted the invitation then received another email containing the consent form and the study survey. Data collection was carried out in January 2024.
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Review Board (IRB) at the university and the study setting. Written informed consent was obtained from the participating nurses, who were informed that they could withdraw from the study at any time. The privacy and confidentiality of the collected data were maintained throughout the study.
Statistical Analysis
Means and standard deviations were used to describe the continuous measured variables, while frequencies and percentages were used to describe the categorically measured variables. The Kolmogrove-Smirnove (KS) statistical test of normality and histograms were used to assess the statistical normality of the metric variables’ assumption. Pearson's bivariate test of correlation was used to assess the correlations between the metric-measured variables. Also, Pearson's bivariate correlation test was used to explore potential confounding relationships among the metric variables. Missing data were handled using pairwise deletion to maximize the use of available data while minimizing bias. The latest version of the SPSS IBM statistical computing test was used for the statistical analysis, with an alpha significance level of 0.050.
Results
Sample Characteristics
One hundred and eighty critical care nurses enrolled in the study and completed and returned the study survey. Table 1 displays the nurses’ sociodemographic and professional characteristics. Of the total sample, 52.8% were male and 23.9% had never been married. Around 34% of the nurses had between 1–4 years of experience and 24.4% held a master's degree in nursing. As for their working units, 21.1% of the nurses worked in the CCU, 22.2% in the ED, 35.6% in the medical-surgical ICU, and 21.1% in other units (i.e., dialysis and burn units).
Descriptive Analysis of the Nurses’ Sociodemographic and Professional Characteristics.

CCU: Cardiac Care Unit; ED: Emergency Department; ICU: Intensive Care Unit
Research Question Results
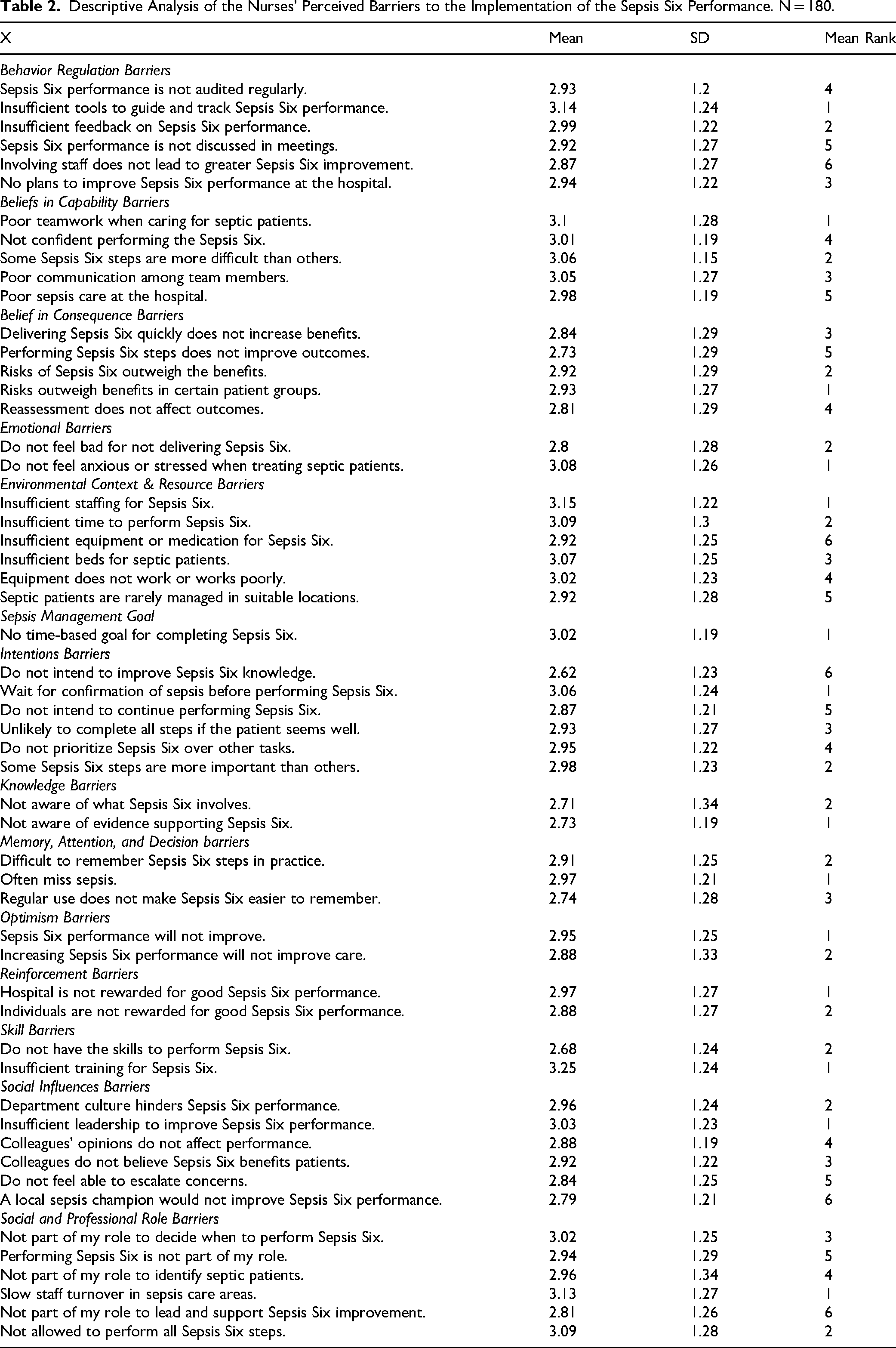
The absence of tools to direct and monitor the sepsis management process was the most frequently cited behavioral regulation obstacle to SSPB implementation. Nurses who believed in capability barriers cited three primary issues: poor communication among sepsis care team members, difficulty carrying out specific SSPB steps, and a lack of teamwork. The idea that the risks of some SSPB interventions outweigh their benefits for particular patient populations was the main obstacle in the area of belief in consequences and effectiveness. When it comes to emotional barriers, nurses frequently expressed a lack of urgency or anxiety when caring for septic patients. Lack of comprehension of the scientific data underlying the SSPB interventions was the main knowledge-related obstacle.
The primary challenges in terms of environmental context and resources were a shortage of time, beds, necessary equipment, and insufficient staffing. The inability to recall every SSPB step during standard clinical practice was the main memory, attention, and decision-making obstacle. Nurses cited a lack of noticeable gains in SSPB performance at work as one of the optimism-related obstacles. The primary obstacle to reinforcement was the lack of a system of rewards for nurses who successfully applied the bundle. According to nurses, the biggest obstacle to successfully completing SSPB steps is a lack of training, which is followed by a lack of specialized skills. The propensity to put off taking action while awaiting confirmation when uncertain about particular SSPB steps was a major obstacle in terms of intentions. The two most commonly mentioned social influence barriers were a workplace culture that does not support SSPB implementation and a lack of leadership to advocate for SSPB improvement. Finally, low staff turnover in sepsis management units was the biggest social/professional role-related barrier, limiting new ideas and innovative approaches. There perceived obstacles are detailed in Table 2.
Descriptive Analysis of the Nurses’ Perceived Barriers to the Implementation of the Sepsis Six Performance. N = 180.
Routine auditing of SSPB procedures was the behavioral regulation facilitator that was most frequently mentioned. Nurses’ confidence in carrying out SSPB interventions was the main driver of belief in capabilities. Facilitators included the conviction that the SSPB's advantages outweigh any potential drawbacks and that proper implementation can enhance patient outcomes in the belief in consequences and effectiveness domain. Guilt over not delivering the SSPB was the main emotional facilitator. In terms of knowledge-related facilitators, nurses emphasized their familiarity with the components of SSPB and the scientific data that backs its application. The availability of beds and the supplies and drugs required to treat septic patients were environmental facilitators.
The desire to increase one's own understanding of sepsis and the equal value placed on each SSPB step were the top facilitators in the intentions domain. There are six interventions. The simplicity of learning SSPB steps and their regular application in clinical procedures served as facilitators for memory, focus, and decision-making. The conviction that SSPB performance will gradually improve was a prevalent facilitator of optimism and reinforcement. In the skills domain, nurses mentioned having the necessary competencies and proper training to carry out SSPB tasks efficiently. The ability to escalate clinical concerns was the primary social influence facilitator, and the freedom to carry out each SSPB step on one's own was the primary social/professional role facilitator. Table 3 provides specifics about these facilitators.
Descriptive Analysis of the Nurses’ Perceived Importance of Various Sepsis Six Performance Indicators at Work.

The barrier domain with the highest overall domain ratings (Table 4) was environmental context and resources (mean agreement = 3.03/5). This was followed by beliefs about the goals of sepsis management (mean agreement = 3.01), sepsis management self-efficacy (3.00), and social/professional role identity (2.99). Behavioral regulation, skills, emotional reactions, knowledge, beliefs about consequences, memory, and decision-making were among the barrier domains that received lower ratings. Emotional motivation, on the other hand, was the facilitator domain that was most highly rated (mean importance = 3.76/5). This was followed by intentions to act (3.74), optimism regarding the implementation of SSPB, environmental context/resources, and self-belief in capability. Skills, social influence, behavioral regulation, and reinforcement were the facilitator domains with the lowest ratings.
Descriptive Analysis of the Nurses’ Perceptions of the Sepsis Six Performance Main Domains.

Discussion
Sepsis is a complicated condition that can pose serious consequences on patients’ health and countries’ health systems. Given that the Sepsis Six performance guidelines have been shown to decrease these consequences, this study aimed to identify nurses’ perceived barriers to and facilitators of implementing the Sepsis Six guidelines in acute care settings. The findings revealed that the nurses’ top perceived Sepsis Six performance barriers were the environmental contexts and resources barriers, followed by the belief in sepsis management goals barriers. These were followed by the belief in capabilities to manage sepsis barriers and the social and professional role barriers. On the other hand, emotional facilitators were the top facilitator group, followed by the intentions facilitators, and then the optimism about sepsis management facilitators.
Many challenges face nurses when applying sepsis guidelines, including knowledge, environmental, and organizational barriers. In terms of the environmental barriers to the nurses’ performance of the Sepsis Six, the study revealed insufficient staffing, equipment, medication, time, and beds to be primary barriers. This finding aligns with previous research by Burney et al. (2012) and Mosavianpour et al. (2016), which also identified a lack of beds, insufficient equipment, and heavy workloads as major barriers to the application of sepsis guidelines. Furthermore, a recent study conducted in Khartoum revealed that supply limitations (e.g., lack of sterile equipment), poor communication among staff, and administrative or policy barriers can hinder the dissemination and implementation of the Sepsis Six guidelines (Jarelnape, 2023). The current study also revealed that the nurses were not allowed to perform some of the Sepsis Six steps, leading to delayed sepsis management. Similarly, Roberts et al. (2017) reported that the restricted role of nurses is a main barrier to their application of sepsis guidelines. Therefore, allowing nurses to independently perform all sepsis management steps and enabling them to initiate treatment, especially first-line antibiotics, without waiting for doctors’ orders is essential for decreasing patient complications and mortality rates (Roberts et al., 2017). The current findings also align with a previous qualitative study, which reported laboratory results waiting time, lack of necessary equipment, and nurses not having the authority to take blood cultures or initiate the first dose of antibiotics as being the main reasons for delays in sepsis management (Matthaeus-Kraemer et al., 2016).
Our finding that the lack of tools to guide nurses in applying sepsis guidelines constitutes a main barrier is supported by the studies of Bani Hamad et al. (2024) and Frank et al. (2023), who reported the importance of written tools for improving nurses’ sepsis-related practices. Also similar to the current study, Roberts et al. (2017) and Bentley et al. (2016) reported that lack of audit and feedback on sepsis performance is considered a main barrier to nurses’ implementation of sepsis guidelines. Another main barrier revealed in the present study was nurses’ lack of knowledge related to sepsis assessment and management, which is consistent with the finding of Rababa et al. (2022) that lack of knowledge and unfamiliarity with the Sepsis Six guidelines can lead to the delayed identification of sepsis. For example, nurses may be unfamiliar with the signs of sepsis and may mistakenly believe that patients with a low temperature do not require sepsis care (Muratkoc, 2018). In addition to the need for increased knowledge, the regular application of sepsis guidelines can make it easier for nurses to remember the steps involved and improve their performance (Frank et al., 2023).
This study found that a lack of reinforcement and motivation is a major barrier to nurses’ application of the Sepsis Six guidelines, which is consistent with the finding of a Canadian study that nurses and physicians who are motivated are more likely to follow the Sepsis Six guidelines (Mosavianpour et al., 2016). A limited number of research studies have discussed intention barriers to the application of sepsis guidelines, reporting that the uncertain diagnosis of sepsis can lead to delayed management and initiation of broad-spectrum antibiotics. In turn, this can increase hospital length of stay and increase sepsis-related morbidity and mortality rates (Arabi et al., 2021; Burney et al., 2012). The findings of this study align with a recent study in Egypt, which identified a lack of resources and equipment as being a significant barrier to the implementation of sepsis guidelines (Mohamed et al., 2023). Unfortunately, in Jordan, there is a lack of data on sepsis and the main barriers and facilitators that impact the application of sepsis guidelines. Therefore, there is a need for further qualitative and quantitative studies in Jordan which identify and explore the primary barriers and facilitators associated with implementing these guidelines.
As for the perceived facilitators, the current findings revealed that the most important facilitators were good teamwork and communication, which is consistent with the findings of previous studies (Jarelnape, 2023; Reich et al., 2018; Roberts et al., 2017). The current findings regarding the importance of leadership and improving team performance in facilitating Sepsis Six performance are consistent with the findings of Reich et al. (2018) that a lack of leadership or support can hinder nurses from applying sepsis guidelines. Further, intention facilitators and emotional facilitators, such as feeling guilty about not performing sepsis management, were also found to be main facilitators in this study. In other words, these emotional factors encourage nurses to properly perform all of the Sepsis Six guidelines. In addition, the availability of equipment and sufficiency of resources were found to enhance nurses’ compliance with the Sepsis Six guidelines. The current finding that the consequences of applying sepsis guidelines outweigh the benefits is consistent with previous studies, which have reported that the timely performance of the Sepsis Six guidelines can improve patient outcomes and decrease mortality and hospital length of stay (Venkatesh et al., 2022). The finding of Lindberg et al. (2020) that full compliance with sepsis guidelines can decrease mortality rates supports the current finding that regular assessment and reassessment of patients with sepsis is considered an important facilitator of nurses’ application of the Six Sepsis guidelines. A recent systematic review of 24 studies revealed that implementing sepsis guidelines in the emergency department (ED) can enhance the timely management of septic patients and improve their outcomes (Sungkar et al., 2018). The current findings are also consistent with the findings of Kabil et al. that independent nursing initiatives, such as the prompt administration of intravenous fluids, can reduce morbidity and mortality rates (Kabil et al., 2023).
Strengths and Limitations
Given that the data was collected from only one geographical area, the generalizability of the findings may be limited. Additionally, the use of non-probability convenience sampling may have led to selection bias, which may threaten the internal validity of the study. Furthermore, this type of sampling may not adequately represent the larger population, raising concerns about external validity. However, while random sampling is more rigorous, it can be time-consuming and costly. Another limitation of this study is that data were collected from a single region, which may limit the generalizability of the findings to other healthcare settings with different organizational structures, resources, or cultural contexts.
Implications for Practice
The results of this study offer a number of practical insights that can guide enhancements in the application of the Sepsis Six Performance Bundle (SSPB) in clinical settings.
One of the main obstacles, according to nurses, is the lack of organized instruments to direct and monitor SSPB implementation. Consistency and adherence to the SSPB may be improved by creating and incorporating digital prompts, care pathways, or user-friendly checklists into electronic health records. The main challenges identified in the current study were poor communication, a lack of teamwork, and hierarchical barriers. Establishing official communication procedures and outlining each team member's duties and responsibilities can help to reduce these problems and enhance cooperation, especially in high-stress situations like sepsis management.
Numerous nurses expressed a lack of specialized training and a lack of knowledge about the SSPB. Enhancing knowledge, confidence, and clinical performance requires regular, scenario-based training programs that are specific to the SSPB steps and refreshers on the clinical evidence that supports them. Implementation was severely hampered by environmental constraints like a shortage of beds, insufficient staffing, and limited equipment. In order to support prompt sepsis care, hospital leadership should place a high priority on resource planning, particularly during peak hours and in high-risk units.
One common obstacle was having trouble remembering the SSPB steps for everyday practice. Memory and decision-making may be improved by incorporating SSPB prompts into digital systems and providing visual cues like posters or quick-reference cards. One demotivating factor mentioned was the lack of a formalized system for rewards or feedback. Adherence and accountability can be strengthened by putting in place a feedback system, such as unit-level reporting or monthly performance dashboards.
Low levels of stress or emotional urgency during sepsis care were reported by nurses to impair performance. Reframing sepsis care as life-saving and time-critical through leadership reinforcement and education could increase responsiveness and emotional engagement. One frequently mentioned obstacle was waiting for confirmation during uncertain SSPB steps. When appropriate, institutions could review and update their policies to permit licensed nurses to independently start certain time-sensitive interventions.
Nurses believed that the workplace culture was hostile to SSPB implementation and that there was a lack of leadership. Adoption may be encouraged and a supportive environment may be created by identifying and assisting clinical champions or change agents at the unit level. The study found that self-efficacy, belief in sepsis management goals, and environmental context were the most important perceived barrier domains. The biggest gains in SSPB implementation might result from giving priority to interventions that target these particular areas.
Healthcare organizations can more successfully handle the various obstacles to SSPB adoption and take advantage of current facilitators by coordinating practice enhancements with these empirically derived insights. In the end, this may result in better patient outcomes and better sepsis care delivery.
Conclusions
The effective implementation of sepsis guidelines by nurses is essential for improving patient outcomes, including reducing sepsis-related morbidity and mortality. Overcoming key barriers such as insufficient training, lack of tools, inadequate staffing and resources, and poor teamworks is critical to enhancing the quality and timeliness of sepsis care. This study highlights the need for targeted strategies to support early sepsis detection and prompt symptom management. Ongoing interprofessional educational programs about sepsis management for both physicians and nurses, and the provision of specific written and quick tools/checklists, can facilitate the early assessment and management of sepsis and may improve nurses’ adherence to sepsis guidelines. Further interventional studies are needed to assess the barriers to and facilitators of the implementation of sepsis guidelines in critical care settings. Future studies that include larger samples of multidisciplinary participants and that cover more than one geographical area are recommended to improve the generalizability of the findings and the reliability and validity of the data.
Footnotes
Acknowledgments
We thank Al-Balqa Applied University for facilitating the study procedure
Ethical Statement
The Institutional Review Board (IRB) at Al-Balqa Applied University approved our study (approval: 2024/2023/3/17) on March 17, 2024. Respondents gave written consent for review and signature before starting the study.
Author Contribution Statements
All authors contributed equally to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.