
Abstract
Introduction
Compassionate care is considered as the main part of the nurses’ identity and a core component of nursing care. One clinical environment where patients experience a lot of pain and nurses play a vital role in delivering care is the intensive care unit (ICU).
Objective
Considering the importance of compassionate care in intensive care units, this study aimed to assess the relationship between the work environment and nurses’ compassion in intensive care units.
Methods
In this cross-sectional survey, a total of 235 nurses were randomly selected from the intensive care units of four educational hospitals of Tabriz University of Medical Sciences from January to March 2021. Data were collected by demographic questionnaire, the Sussex-Oxford Compassion for Others Scale (SOCS-O) and the Practice Environment Scale of the Nursing Work Index (PES-NWI).
Results
The results showed that there was a significant and inverse relationship between the patient per nurse ratio and the mean score of nurses’ compassion (P < .05). Moreover, Pearson correlation coefficient showed that the mean total score of the nursing work index had a significant positive relationship with the mean score of the compassion for others (r = 0.16, P = .016).
Conclusion
Health care managers and leaders should pay more attention to the promotion of nurses’ working environments and they should remove the organizational barriers of compassionate care delivery.
Introduction / Background
One of the approaches that has recently been emphasized in health care professions, especially in nursing, is compassionate care (Straughair et al., 2019). Compassionate care is considered as the main part of nurses’ identity and a most valuable asset (McCaffrey & McConnell, 2015). Compassion is seen as moral virtue and moral orientation, resulting in caring behaviors and good quality healthcare in practice (Fotaki, 2015).
Compassion has been defined as “an openness to the suffering of others with a commitment to relieve it” (Zamanzadeh et al., 2017). Compassionate care is a complicated process that requires a set of skills such as caring for the patient, emotional engagement in caring, feeling intimate with the patient, and expressing humility and humanity which is accompanied by taking action and trying to reduce the patient's pain and suffering (Ghafourifard et al., 2022).
Communicating with warmth, using positive body language, using jokes and short conversations are some helpful strategies for expressing compassion (Ferraz et al., 2020). Moreover, allocating enough time to identify the patients’ needs alongside supporting, respecting, and valuing them are mentioned as characteristics of compassionate nurses. By delivering compassionate care, nurses reassure patients that the person is more valuable than a disease or diagnosis (Dillane et al., 2018).
When the interactions between health care providers and patients and their families occur based on compassion, it helps to build a trustworthy relationship that involves the participation of the patient and his/her family in health care delivery (Ghafourifard et al., 2022). Therefore, nurses should try to develop compassion in their work environment and gain sufficient information and knowledge in providing compassionate care delivery, which is called "compassion literacy" (Burridge et al., 2017).
Review of Literature
According to the literature review, compassionate care has been associated with improved recovery, improved sense of responsibility, better control of health care, and increased patientsatisfaction (Younas & Maddigan, 2019). Furthermore, compassionate care could improve patients’ independence and lead to the provision of safe and high quality care. Saving time and cost, nurses’ satisfaction with their profession, improved professional development, and moral empowerment are other consequences of compassionate care for nurses (Babaei et al., 2016; Tehranineshat et al., 2019). In addition, compassion as a common human feeling is considered an ethical virtue that is used in all cultures, even when there are differences between the culture of nurses and patients (Singh et al., 2018).
Although compassion has many benefits, various barriers may hinder the providing of this type of care in health care settings (Blewitt et al., 2015). The barriers such as lack of human resources, lack of time, work pressure, low salaries of nurses compared to other health care professionals, a large amounts of paperwork, lack of organizational support, and lack of appreciation and support from managers have been reported in previous studies (Valizadeh et al., 2018).
Based on the available evidence, the lack of a compassionate attitude among nurses leads them to do routine and physical care rather than providing high-quality compassionate care (Babaei & Taleghani, 2019). In addition, lack of manager support for compassionate care and excluding it in the assessment of nurses’ performance, alongside high pressure to perform tasks in a limited amount of time, could impact the development of compassionate care in health care settings (Henderson & Jones, 2017).
Creating a compassionate care environment in health care organizations, regardless of any deficiencies in the workplace, can help to improve the quality of nursing care (Babaei et al., 2016). To flourish compassion, it requires a work environment that facilitates the promotion of compassionate care (Tierney et al., 2019). The characteristics of a work environment can facilitate or hinder the provision of compassionate nursing care (Joolaee et al., 2018). In this regard, the International Council of Nursing (ICN) defines a positive workplace environment as an environment that supports decent and appropriate work, ensures the health, safety, and personal well-being of staff, and supports high quality patient care that finally improves the motivation, productivity and performance of individuals and organizations." (Zangaro & Jones, 2019).
The results of previous studies show a significant relationship between job satisfaction and a healthy work environment (Salehi et al., 2020; Wu et al., 2020). In contrast, an unhealthy work environment could lead to low quality of nursing care (Guirardello, 2017), nurse burnout (Sodeify & Habibpour, 2020), increased nurse turnover (Wan et al., 2018), medication errors (Joolaee et al., 2016), and delayed and missed nursing care (Kim et al., 2018).
Although compassionate care is the cornerstone of the nursing profession and high quality health care, working in environments that are constantly dealing with the suffering and even death of patients may affect nurses’ compassionate behavior (McVicar et al., 2021). In some contexts, nurses may separate themselves from patients and try to deliver routine care rather than compassionate care that is active, committed, and empathetic (Blewitt et al., 2015).
The evidence suggests that compassionate care, as a complex concept, needs further investigation in different clinical settings (Tehranineshat et al., 2019). One of the clinical environments where patients experience a lot of pain and nurses play a vital role in delivering care is the intensive care unit (ICU). The intensive care unit is a very complex and dynamic workplace where patients are in critical condition and experience many sufferings; therefore, nurses could play an essential role in alleviating their sufferings and providing compassionate care (Azevedo Filho et al., 2018). The ability to manage emotionally challenging situations not only allows nurses to tolerate pain and suffering but also enables them to express compassion toward others (Durkin et al., 2019). So, it is essential to identify ways that enable healthcare providers to deliver compassionate care in the challenging environment of an intensive care unit (Barratt, 2017). In a recent study in Canada, Roze des Ordons et al. (2020) found that contextual factors of the clinical environment of intensive care units, such as physical design and esthetics, could impact nurses’ compassion. Moreover, they found that use of technology in these units results in health care providers taking their attention away from the more difficult emotional suffering and paying more attention to the physical aspects of care.
Patients in intensive care units experience a lot of pain and suffering and they need to receive compassionate care (Saechao et al., 2017). It seems that working context could impact nurses’ compassionate behavior. Therefore, this study aimed to assess the relationship between the working environment and nurses’ compassion in the intensive care units.
Methods and Materials
Design
This multicenter cross-sectional study was conducted in four educational hospitals affiliated with Tabriz University of Medical Sciences, Tabriz, Iran.
Research Question(s)
There was two main research question was: Is there a relationship between the nursing work environment and nurses’ compassion for others? And, is there a correlation between nurses’ compassion with their demographic and clinical characteristics?
Sample
There are two general and two specialized educational hospitals (heart disease and orthopedic hospitals) in the university. We selected all of them for more generalization of findings. Data collection lasted from January to March 2021. Krejcie and Morgan's (1970) table was used to calculate the sample size of the study. A total of 235 nurses working in the intensive care units were selected by random sampling method.
Inclusion/Exclusion Criteria
Inclusion criteria included nurses who had at least a bachelor's degree in nursing with at least 6 months working experience in the intensive care unit. Nurses who did not answer more than 3 questions of the questionnaire were excluded from the study.
Assessment Tools
Data were collected by a demographic questionnaire including the participant's demographic and clinical data such as age, sex, marital status, working unit, years of experience, shift type, and ICU type. Moreover, the main variables (compassion and working environment) were assessed by the following scales:
The Sussex-Oxford Compassion for Others Scale (SOCS-O) was used to assess nurses’ compassion levels. The questionnaire was developed in 2020 and includes 20 questions. It consists of 5 subscales and each subscale has 4 items: Recognizing suffering (questions 1-6-11-16), understanding the universality of suffering (questions 2-7-12-17), feeling for the person suffering (questions 3-8-13-18), tolerating uncomfortable feelings (questions 4-9-14-19), and acting or being motivated to act to alleviate suffering (questions 5-10-15-20). The answer to each question is scored based on 5-point Likert scale including: (1 = not at all true, 2 = rarely true, 3 = sometimes true, 4 = often true, and 5 = always true). The total score on this scale ranged from 20 to 100. In a previous study, the Cronbach's alpha for this scale was reported between 0.75 and 0.93 for the whole scale and between 0.75 and 0.93 for the subscales (Gu et al., 2020). In this study, the validity and reliability of the Persian version of the SOCS-O Scale were assessed by the content validity method. For this purpose, after forward-backward translation of the questionnaire by an expert in the field of English, the questionnaire was given to ten professors working in the Faculty of Nursing and Midwifery to comment on the scale. The item content validity index (I-CVI) of the final version of the scale ranged from 0.82 to 1 and the scale content validity index (S-CVI) ranged from 0.86 to 0.97, which indicated a high content validity. The Cronbach's alpha coefficient of this scale was 0.93.
The Practice Environment Scale of the Nursing Work Index (PES-NWI) was used to measure the nursing practice environment. This questionnaire was developed by Lake (2002). It consists of 5 subscales: Nurse's participation in hospital affairs (9 questions), Nursing foundations for quality of care (10 questions), Nurse manager ability, leadership and support of nurses (5 questions), Staffing and resource adequacy (4 questions), and Collegial nurse-physician relations (3 questions). The answers to each question were scored based on 4 points Likert scale including 1 (strongly disagree), 2 (disagree), 3 (agree), and 4 (strongly agree). The average scores were calculated for each subscale. The validity and reliability of this scale have been assessed by Smith and Parker (2015) by reporting a Cronbach's alpha of 0.71. In another study by Gu and Zhang (2014), Cronbach's alpha for each domain was reported to be between 0.85 and 0.95 which indicates the higher consistency of the scale. We used the Persian version of PES-NWI developed by Elmi et al. (2017). They assessed the psychometrics of the Persian version of this scale and reported a Cronbach's alpha coefficient of 0.98. The Cronbach's alpha of 0.95 was obtained in our study.
We used a method published in Lancet by McHugh et al. (2021) for calculating a patient to nurse ratio. We asked each nurse how many nurses and patients were on the ward during the last shift the nurse worked, and by averaging them to ward level, the average nurse-to-patient ratio was calculated across all wards in the hospitals.
Institutional Review Board Approval
The ethical approval of the study was obtained from the Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran. The purpose of this study was explained to all participants and they were assured of the confidentiality of the collected data. The informed consent form was obtained from all participants.
Statistical Analysis
The collected data were analyzed by SPSS software (version 21). Assessment of the normality of data was done by the Kolmogorov–Smirnov test. Data were analyzed using descriptive statistics including mean and standard deviation, t-test, ANOVA, and Pearson correlation coefficient. A p-value less than 0.05 was considered statistically significant.
Results
Background Characteristics of the Nurses
Based on the findings of this study, the mean age of nurses was 31.84 ± 5.81 years. Most of the nurses participating in the study were female (73%). Moreover, the majority of the participants were married (61.1%). In terms of educational degree, the majority of participants (92%) had a bachelor's degree in nursing. Other demographics are shown in Table 1. The mean years of experience in nursing were 8.09 ± 5.53 years. The participants’ experience in the intensive care units was 5.71 years. Most of the nurses (91.2%) work rotation shifts. The mean of the patient to nurse ratio was 2.89 ± 1.09.
Comparison of Nurses’ Compassion Based on the Demographics of Participants.

Research Question Results
The mean total score of nurses’ compassion
Based on the results, the mean total score of nurses’ compassion using the SOCS-O tool was 72.42 ± 9.57. The results of the study showed that the highest score was related to the understanding the universality of suffering subscale (15.16 ± 2.62) and the lowest score belonged to the tolerating uncomfortable feelings subscale (14.14 ± 2.18) (Table 2).
Mean Score of the Sussex-Oxford Compassion for Others Scale (SOCS-O) Subscales Based on the Nurses’ View.

Correlation of nurse’s compassion with demographic and clinical characteristics
The analysis of the mean score of nurses’ compassion in terms of nurses’ gender, age, education level, marital status, work experience, and working shift showed no statistically significant differences (P > .05). However, the results showed a significant and inverse relationship between the patient per nurse ratio and the mean score of nurses’ compassion (P < .05). Based on the results of the study, the mean score of nurses’ compassion according to the type of hospital was statistically significant, so that the highest score belonged to the nurses working in a special hospital (82.57 ± 3.05) and the lowest score belongs to the nurses working in a general hospital (71.27 ± 9.64) (P < .05).
Nurses’ view on practice environment
Table 3 shows the mean score of the Practice Environment Scale of the Nursing Work Index (PES-NWI) by each domain. Based on the results, the mean total score of the PES-NWI scale was 1.99 ± 0.51 (in a possible range of 1 to 4). The highest and lowest score belonged to the collegial nurse-physician relations subscale (2.39 ± 0.73) and the nurse manager's ability, leadership, and support of nurses subscale (1.85 ± 0.69), respectively.
the Practice Environment Scale of the Nursing Work Index (PES-NWI) Subscales Based on the Views of Nurses.

Correlation of the Nursing Practice Environment with Nurses’ Compassion for Others
Data analysis using the Pearson correlation coefficient showed that the mean total score of the nursing work index had a significant positive relationship with the mean score of the compassion for others (r = 0.16, P = .016). Moreover, the mean score of each domain of the nursing work index questionnaire, except for the collegial nurse-physician relations domain, showed a positive relationship with the mean score of compassion for others (P < .05). (Table 4).
Correlation Between the Mean Score of (SOCS-O) Domains and the Mean Score of Each Domain of PES-NWI Questionnaire (Pearson Correlation Test).
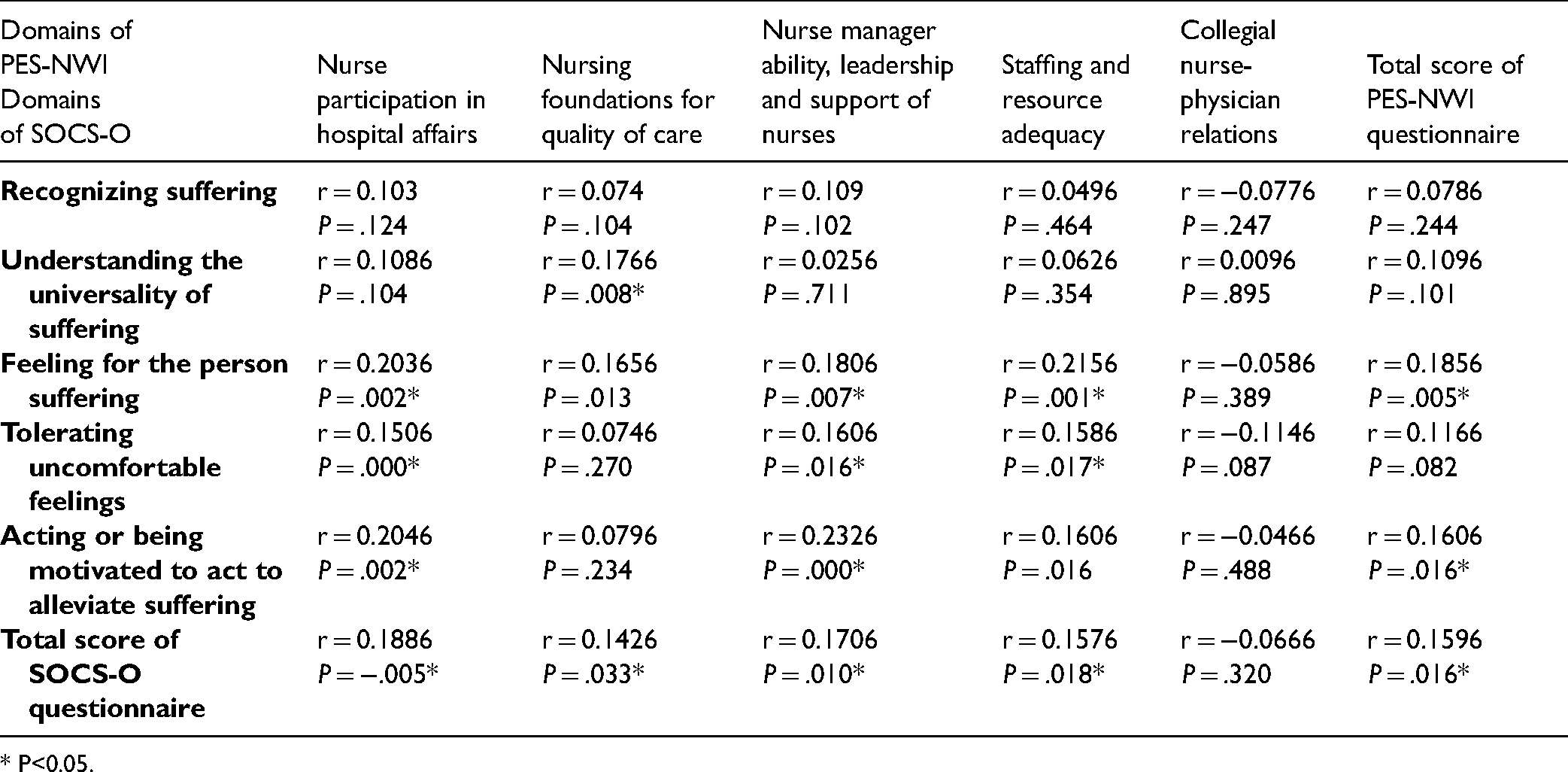
* P<0.05.
Discussion
This study aimed to assess the relationship between the nursing work environment in the intensive care units and nurses’ compassion for others. Based on the results of the study, the mean total score of nurses’ compassion was 72.42 ± 9.57 out of 100. In a recent study conducted on Turkish nurses by Kaplan Serin et al. (2021), the total score of compassion using the 24-item Compassion Scale (CS) tool was 94.49 ± 12.62 out of 120 which indicates a high level of compassion among nurses. In a recent study in Egypt, Abozied et al. (2020) studied the viewpoint of 140 patients on compassionate care. The results showed a high level of compassionate care in the studied settings.
According to the result, among the several domains of Compassion for Others Scale (SOCS-O), the highest score belonged to the "understanding the universality of suffering" domain and the lowest belonged to the "tolerating uncomfortable feelings" domain. It seems that the understanding of the universality of suffering is more tangible and acceptable to nurses. According to the nurses’ perspective, tolerating uncomfortable feelings caused by patients’ problems was the most difficult domain of compassion. It could be noted that patients admitted to the intensive care unit have a variety of needs and are critically ill; therefore managing the emotions of these patients seems challenging.
According to the findings, there was no significant relationship between the mean score of nurses’ compassion and their gender. The result of a study by Arkan et al. (2020) is in line with the results of our study. In contrast, Salazar (2015) found that women were more compassionate than men. It seems that these differences are due to the differences between women and men in terms of affections and feelings.
There was no statistically significant relationship between nurses’ educational level and the mean score of compassion. Unlike our results, a study by Arkan et al. (2020) showed a positive relationship between nurses’ education and compassion. In contrast, in a study conducted in the Netherlands by López et al. (2018), a significant negative correlation was found between the level of education and the level of compassion for others; it means that by increasing educational level, the score of compassion is decreased. In this study, no significant relationship was found between nurses’ marital status and the mean score of compassion, which is consistent with the results of a study by Martins et al. (2013).
In an ethnographic study conducted in Iran by Babaei and Taleghani (2019), one of the most important barriers to compassion from the nurses’ point of view was the lack of nurses’ sufficient motivation to provide compassionate care and ignoring the consequences of this type of care in the patient's recovery process.
The findings showed a significant negative correlation between the mean of patient to nurse ratio and the mean score of nurses’ compassion. It means that with increasing the number of patient per nurse, the mean score of nurses’ compassion is decreased. I a recent study, Aiken et al. (2018) assessed the working environment among nurses working in 46 different hospitals in the UK. The results showed that when the patient per nurse is increased, the nurses would have less time to interact with the patient and his/her family to manage their possible concerns. According to the literature review, spending more time with patients to relieve their anxiety and providing effective communication are effective strategies for expressing compassion in clinical settings. Therefore, decreasing the patient-to-nurse ratio in health care settings could help nurses to spend more time for active listening to the patients (Ghafourifard et al., 2022).
In the present study, the mean total score of nurses’ work environment index was 1.99 ± 0.51 out of 4 which is lower than a score (2.15 ± 0.36) of a study conducted in the intensive care unit in Brazil (Azevedo Filho et al., 2018). Moreover, in a recent study done in Oman by Al Sabei et al. (2020), the score of working environment index was higher than the cut-off point of this tool and it indicates the favorable working environment index in their study. In another study conducted by Albashayreh et al. (2019), the score of the working environment index using the PES-NWI tool was moderate. The working condition in different countries varies based on the factors such as organizational resources, staffing, and leadership.
Among the various domains of the working environment index measured by the PES-NWI tool, the highest score belonged to the “collegial nurse-physician relations” domain. It means that nurses and physicians have a collegial interaction in the studied intensive care units. The evidence highlights the importance of nurse-physician collaboration in clinical settings (Pakpour et al., 2019). Although they perform different tasks in the clinical environment, they are expected to communicate professionally with each other and share the common goal of improving the quality of health care (Pakpour et al., 2019; Wang et al., 2017). Collegial nurse-physician relations are defined as a collaborative decision-making process in which nurses and physicians share the goals and outcomes for providing high – quality care (Tan et al., 2017).
In a study in Brazil, Azevedo Filho et al. (2018) found a positive correlation between the domains of the working environment and the domain of collegial nurse-physician relations. In line with other studies (Al Sabei et al., 2020; Koon, 2020), the domain of collegial nurse-physician relations obtained the highest score of the Nursing Work Index.
The lowest score on the Nursing Work Index belonged to the "Nurse manager ability, leadership, and support of nurses" domain which indicates the weakness of nursing managers in providing a supportive environment for nurses. Nurse managers could play a main role in establishing healthy work environments for nurses (Wei et al., 2018). In a study in the United States, Kelly and Todd (2017) showed the positive impact of nursing leadership on the working environment.
The results of our study showed a positive correlation between the nursing work environment and nurses’ compassion. It means that when the nurses’ work environment is good, nurses deliver more compassionate care to their patients. This finding highlights the importance of the nursing work index in providing compassionate care by nurses. Based on the literature review compassion towards others is influenced by individual and organizational factors. In a qualitative study on nurses, Zamanzadeh et al. (2018) found that providing organizational support could improve the nurses’ capacity for compassion. Therefore, the managers of health care systems should try to create a conducive environment for compassionate care (Valizadeh et al., 2018). In this regard, the health care managers could provide educational courses for improving the skills of healthcare providers on compassionate care (Lown, 2015).
Spandler and Stickley (2011) argued that it is impossible for nurses to develop compassionate communication with patients while they are dealing with several problems such as work-related stress due to lack of resources, the lower nurse-patient ratio, and personal problems. Therefore, modification of organizational factors by managers and leaders will have a great effect on nurses’ ability for providing compassionate care.
Strengths and Limitations
This is the first study which assessed the impact of work environment on nurses’ compassion. However, considering that this study is a cross-sectional study, conclusions regarding causality of compassion for others cannot be drawn. Another limitation is the context of the intensive care units which differ from other non-intensive care units. Therefore, the results of the study could be generalized to the intensive care units. It is suggested to compare the nurses’ compassion between nurses working in the intensive care units with nurses working in other clinical contexts in the future studies. Moreover, conducting a mixed method study in this field may provide more information on this phenomenon.
Implications for Practice
Overall, findings from this study have several implications for improving the compassionate care in clinical settings. This study shows that good working environment of nurses is associated with higher nurses’ compassion toward others and highlights the importance of work environment for cultivation of compassionate care in clinical practice. Moreover, nurse managers could play a main role in establishing healthy work environments and supporting nurses for developing compassionate care. For this, they should try to remove the organizational barriers such as heavy work load and paper works. In addition, nurses should improve their personal ability for showing compassion toward others.
Conclusion
The results of the present study showed that working environment of nurses in intensive care units could affect nurses’ compassion toward others. According to the results, the nursing work index had a positive correlation with the mean score of nurses’ compassion. Therefore, health care managers and leaders should pay more attention to the promotion of nurses’ working environments and they should remove the barriers of compassionate care delivery. There are some organizational barriers such as excessive workload and unsupported organizational culture in the health care environment which needs more attention by health care leaders. Development and successful implementation of strategies for identifying, removing, and managing the barriers of compassionate care at the personal and organizational level could have important role for fostering compassionate practice. Moreover, nurses working in the intensive care units should develop the attributes of compassionate care and try to meet the patient’s need by demonstrating altruism and caring behaviors.
Footnotes
Acknowledgments
This study is part of MSc thesis in the field of nursing at Tabriz University of Medical Sciences. The authors thank all nurses who helped to do this study.
Author Contributions
SN, MG, and AG participated in study conception and design. SN collected the data. Data analysis and Drafting of the article were done by MG, SN, and AG. All authors reviewed the manuscript and participated in approval of the final paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tabriz University of Medical Sciences, (grant number 65954).