
Abstract
Background
Assessment of children's health status creates means that may promote their health. This study aimed to investigate the self-perceived health status of school-age children in Jordan.
Methods
The study employed a descriptive and cross-sectional design. Children were recruited from two settings: schools and hospitals. Convenient sampling was used to include eligible children. Children reported their health status using the Child Health and Illness Profile-Child Edition. Data from the study were analyzed using descriptive statistics, t-tests, and one-way analysis of variance.
Results
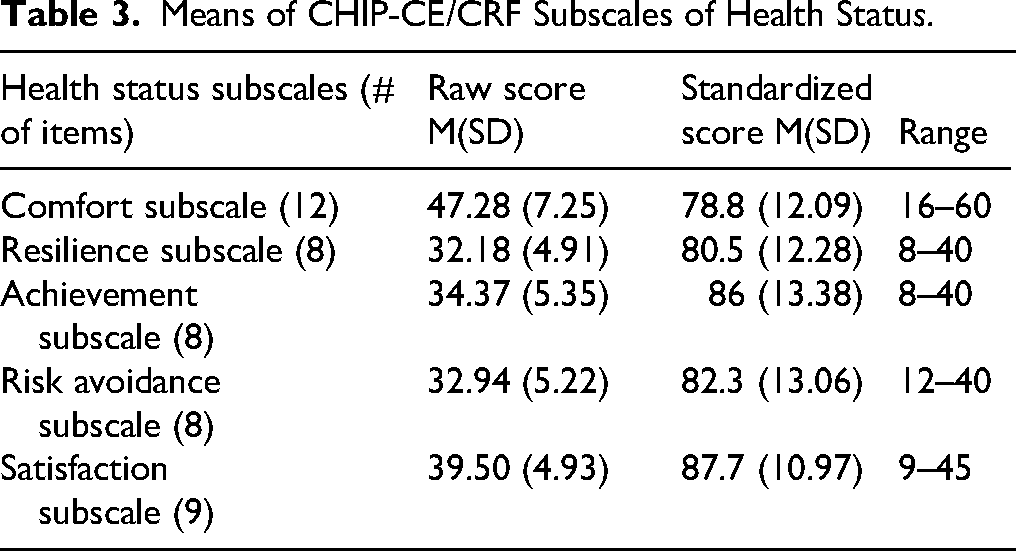
The satisfaction subscale (i.e., satisfaction with oneself and health) has the highest mean (M = 87.7), followed by the achievement (M = 86) subscale that reflects appropriate role functioning in school and with peers, while the comfort subscale (i.e., the experience of physical and emotional symptoms) has the lowest mean (M = 78.8). Girls reported significantly higher scores in the achievement and risk avoidance domains than boys. Achievement and resilience were significantly higher among 10- and 11-year-old children than among 9-year-old children. Additionally, the risk avoidance domain was higher among children aged 11 and 12 than among those aged 8 and 9. The father's educational level and smoking status were other factors that significantly affected the children's health status.
Conclusion
The reports of health status by school-age children varied across different domains. The study concluded that there is a need for significant interventions by family, school, and health care providers, particularly nurses, to improve children's health status in the comfort domain.
Keywords
Introduction
There is a growing focus on children's health in research, with proposals for interventions aimed at improving their health, wellbeing, and academic achievement (Riley, 2004). When the health status of children improves, the likelihood of growth, development, and learning will be maximized (Pérez-Cuevas & Muñoz-Hernández, 2014). However, the focus should shift from child survival to wellbeing (Langridge et al., 2022; Riley, 2004). Children's health is often regarded as a key indicator of the country's security and economic wellbeing (Andrieieva & Hakman, 2018). Estimating children's health can be used to identify both the positive and negative factors that can impact a child during childhood and later in adulthood. However, assessing children's health is more complicated than evaluating adults’ health (Andrieieva & Hakman, 2018; Riley, 2004). It involves estimating children's physical, psychosocial, mental, and functional development through different age groups (Andrieieva & Hakman, 2018). Current health studies targeted children themselves to create means to support their health and general wellbeing, developmental abilities, academic performance, and future health outcomes (Langford et al., 2014).
Review of Literature
Based on their development, school-age children have a unique awareness and concerns about their health experience (Hockenberry, Wilson & Rodgers, 2021; Riely et al., 2004). Thus, obtaining direct data from children themselves about their health status may reduce the likelihood of incorrect or underreporting of data from parents, teachers, and healthcare providers, who may only notice the child in certain situations (Alves Rodrigues & Alves Apóstolo, 2010; Riley, 2004). Children can provide valuable information about their health through age-appropriate health questionnaires. After the age of six, children may provide sufficient data without referring to their parents (Riley, 2004).
Theoretically, health status is described as a multidimensional state of physical and mental health, social and role activities, everyday functioning, and self-perceptions of wellbeing (Wilson & Cleary, 1995). A child's health status is a dynamic state of vital functions that is linked to biological age and the physical and intellectual abilities influenced by genetic, environmental, and adaptive responses during the growth process (Langford et al., 2014). Children's health status is influenced by their experiences with health, current health problems, functional impairment, and social and cultural norms (Rezende et al., 2017). Assessing children's health status should encompass biological, physical, and subjective variables, including physical, mental, and everyday functioning and activities, as well as self-perceptions of wellbeing (Andrieieva & Hakman, 2018; Riley, 2004; Seligman, 2008). These variables are provided among domains of satisfaction, comfort, resilience, risk avoidance, and achievement (Riley, 2004). The domains of satisfaction, comfort, and risk avoidance assess how children perceive health, wellbeing, threats, risks, and symptoms. The relationship with peers, school performance, and socially defined roles is assessed through the achievement domain. The resilience domain encompasses the subconcepts of family involvement and physical activity (Riley et al., 2004).
Assessing children's health status is difficult and requires multidimensional measures (Andrieieva & Hakman, 2018; Langridge et al., 2022). A mixed approach that combines day-by-day assessment of social and psychological functioning with standard medical methods may provide a holistic estimate of a child's health status (Matza et al., 2004). Numerous standard health measures have been developed for children. Recently, the Child Health and Illness Profile-Child Edition (CHIP-CE) was developed for children 6 to 11 years old. The CHIP-CE is a self-report health status instrument that comprehensively evaluates children's symptoms, age-related functioning, wellbeing, and resilience factors that influence future health and risky behaviors (Forrest et al., 2004; Riley et al., 2004). Another subjective measure is health-related quality of life, which encompasses personal concepts of competencies, satisfaction, and wellbeing, as well as situations that may influence individuals’ perceptions of their daily functioning (Rezende et al., 2017).
Western literature included health status studies on ill children, such as the effects of various treatment modalities. Rather than illnesses and diseases, recent studies emphasize that school-age children are susceptible to functional disorders that may occur due to rapid growth and development during specific periods of childhood, the impact of overload from school demands, and poor living conditions (Andrieieva & Hakman, 2018).
The WHO–UNICEF–Lancet Commission report (2020) claimed that children over five should be the core of sustainable development goals, yet children's voices are influential forces for change. Child rights could be violated through many domains, such as poverty, gender bias, and discrimination, inadequate nutrition, violence and war, and poor access to education, health services, clean water, and shelter.
Studies emphasize the health status of both ill and healthy school-age children. However, children's reports about their health status may be affected by factors such as age, gender, socioeconomic status, and cognitive abilities (Riley, 2004). Boys and girls viewed illness in different ways; girls were more likely to accept the idea of being sick and live with the limitations of their diseases than boys. This could be due to differences in their social role and expectations from their families and societies (Iley, 2007). Similarly, girls reported higher scores on the risk avoidance domain than boys (Langridge et al., 2022). Riley (2004) stated that children can reliably report on their health by the end of their first year of primary school. They can also experience difficulties in reporting their emotional states (Harris et al., 1989). Along the same line, differences were reported between older and younger children in terms of resilience, achievement, and satisfaction domains (Langridge et al., 2022). Another factor that mediates the health status of children is family characteristics. Using the US National Health Interview Survey, Case et al. (2002) studied the relationship between child health and family income. The study revealed that children from poorer families have significantly poorer health outcomes than those from wealthier families. The same study reported that children from poorer families complained of poorer health, that have the same effect on those children when they entered adulthood, as they had more serious chronic conditions. Similarly, children from low-income families reported lower scores in the risk avoidance and resilience domains (Starfield et al., 2002).
Jordan Context
Jordan's population accounts for 10.3 million. It is referred to as a young society, as children comprise 37% of the population (UNICEF, 2022). The issues of improving children's health status and promoting healthy lifestyles have become particularly important in the context of Jordan's socioeconomic transformations.
According to the education system, children are enrolled in primary education for a specified number of years, either in the public or private sector (Ministry of Education, 2024). However, public schools face several challenges, including overcrowded classrooms, deteriorating facilities, the need for more effective teacher training (USAID, 2020), and bullying (Shahrour et al., 2020). Moreover, the Jordan National Micronutrient and Nutrition Survey (JNMNS) 2019 showed that the prevalence of undernutrition is low in school children. However, overweight and obesity prevalence is concerning among around a quarter of school-age children, with slightly less than half of children being vitamin D deficient. Almost one-third of children are anemic (Ministry of Health, UNICEF, WFP, Jordan Health Aid Society International, Department of Statistics, Biolab, Ground Work, 2021). Therefore, anemia is reported as the most common health problem among children (2017–18 Jordan Population and Family Health Survey). These counteracting indicators may threaten the health and functional abilities of school-age children. To the best of the researchers’ knowledge, the current study is among the few that have been conducted on the health status of school-age children as reported by themselves. This study aimed to investigate the self-perceived health status of school-age children (6–12 years) in Jordan. Therefore, the data from this study may contribute to the knowledge about children's health status, quality of life, overall morbidity, and unrecognized health needs in Jordan. Accordingly, healthcare professionals, nurses, health planners, and policymakers can plan and implement strategies to meet the increased needs of school-age children based on a more holistic approach, aiming to improve their health status and address specific needs related to a particular functional domain.
The study has the following research questions:
What is the means of children's self-perceived health status in terms of five domains (satisfaction, comfort, risk avoidance, resilience, and achievement). Are there differences in children's self-perceived health status according to demographic variables (and child's gender, age, monthly family income and parents’ educational level), health insurance, and father smoking.
Methods
Study Design
The design used in this study was a descriptive cross-sectional.
Sample and Sampling
The target population consisted of school-age children aged 6 to 12 years old. Children were selected from two settings: healthy children were selected from primary schools, and ill children were selected from hospitals. In Jordan, primary education is mandatory for children aged 6 to 16. It is provided by three sectors: public education (57%), private education (36.7%), and the United Nations Relief and Work Agency (2.96%) (Ministry of Education, 2024). Children were recruited from two settings: schools and hospitals. Four schools were randomly selected from a large directorate in the central region of Jordan. Convenient sampling was used to include eligible children in each selected school. Random selection was applied to choose two hospitals from the list of hospitals in the central region of Jordan: one public hospital and one university-affiliated hospital. Children in the selected hospitals were conveniently selected from the pediatric clinic or the pediatric ward. The inclusion criteria were children aged between 6 and 12 years with normal cognitive abilities. Researchers excluded children with critical illnesses (i.e., any severe problem with the airway, breathing, or circulation, or acute deterioration of conscious states such as severe asthma and rheumatic valve disease) or developmental problems (i.e., delays or abnormal patterns of development in the areas of communication/language, motor skills, problem-solving or social and adaptive behavior such as Apraxia and Dyslexia) from the study.
The G power program was used to calculate the sample size in this study. The F test was utilized using an Alpha level of 0.05, an effect size of 0.2, and a power of 0.95 (Faul et al., 2007). The estimated required sample size was 552 children.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) (Approval number: 10/18/2015) at the university where the researchers of the current study are based, as well as from the Ministry of Education and the Ministry of Health, prior to data collection. Parents or legal guardians were provided with written consent forms for their children's voluntary participation, which required their signatures. Additionally, oral assent was obtained from the children whose parents consented to their involvement in the study, ensuring that the children were also interested in participating.
Data Collection
A self-administered questionnaire was used to collect the data for this study. Data were collected between September and December 2017.
For data collection from schools, the researcher contacted the school principal to facilitate study enrollment and explain the study's purpose and data collection procedure. A cover letter providing a full explanation of the study's purpose and protocol was sent to parents or legal guardians of children to be signed at home and returned to the school. Furthermore, oral assent was obtained from children whose parents had given their approval for their participation in the study, ensuring their interest in participating. The study's questionnaire was distributed in the classroom and completed by the children within a class period. Regarding data collection from hospitals, the children were invited during a waiting time in the pediatric clinic or after admission to the pediatric ward. After obtaining the parents’ consent, the children filled out the questionnaire in a quiet room within the hospital to ensure confidentiality.
In both school classrooms and the hospital setting, the researcher adhered to the guidelines outlined in the administration manual provided by the authors. Socio-demographic information related to the children and their parents was collected from the parents. The questionnaire was administered exclusively to children whose parents consented to participate. The questionnaire was administered on paper. One researcher was designated to distribute the questionnaire to the children, which took approximately 30 to 45 min. The researcher informed the children that they would answer questions about their health, using this moment to discuss health and its significance.
Additionally, the researcher encouraged the children to refer to the pictures to aid their understanding of the questions. To clarify the responses, the researcher utilized examples from the administration manual and read practice items aloud, reminding the children to select only one answer for each question, even if they found it difficult to choose the most appropriate one. The questions were not deemed sensitive or overly personal by parents, and the children expressed no discomfort with the content. Many questions required children to reflect on their health over the past 4 weeks. To facilitate this, the researcher prepared a large calendar to illustrate the specific days encompassed by these 4 weeks, ensuring this was marked before the start of the administration. In the school setting, seating arrangements were made to ensure the privacy of children's responses, and children who were ineligible for participation were moved to a separate classroom for a planned activity.
Measurement
Demographic data. Socio-demographic information related to the children and their parents was collected. Child demographic characteristics included gender, age, and medical diagnosis. The parents’ demographic data were family income, number of children, education level, smoking status, medical insurance, and employment status.
Child Health Status. The Child Health and Illness Profile-Child Edition/Child Report Form (CHIP-CE/CRF) was used to assess the health status of children. The (CHIP-CE/CRF) is a validated instrument that comprehensively explains a child's health features. It is a self-administered questionnaire that assesses children's perceived health, including their perceptions of wellbeing, health, illness, and developmental abilities that positively or negatively impact their health. The instrument is fully illustrated with cartoon-type characters that anchor the five response options for each item, with a total of 45 items. Most items evaluate the frequency of specific behaviors or experiences. They generally employ a five-point response scale. When a recall period is implemented, it usually covers the last four weeks. Scale scores are calculated by averaging the responses of individual items applicable to both domains and subdomains. The higher scores indicate high levels of health status.
The CHIP-CE/CRF contains five domains. Satisfaction with oneself and health consists of nine items (e.g., how often you are proud of yourself). The comfort domain examines the experience of physical and emotional symptoms and restrictions in activity due to illness symptoms. It consists of 12 items (e.g., in the past four weeks, how often did you have trouble breathing). The resilience domain examines behaviors and family involvement that enhance health. It consists of eight items (e.g., in the past four weeks, how often did your parents listen to your ideas).
Risk avoidance examines the avoidance of behaviors that pose health risks. It consists of eight items (e.g., how often did you hang around with kids who get in trouble?). The achievement domain examines developmentally appropriate role functioning in school and with peers. It consists of eight items (e.g., how good are you at making friends?) (Riley, 2004).
The (CHIP-CE/CRF) instrument was validated originally by expert reviewers based on content appropriate for the domains. The Expert reviews provided support for content validity. Feasibility testing, along with assessments of internal consistency reliability, test–retest reliability, and validity, was conducted across four diverse regions in the US, involving six distinct samples that included around 2,000 children. These evaluations have confirmed the practicality of implementing the CHIP in medical environments, homes, and school classrooms, creating a reliable and valid version of the CHIP for children. In the same study, researchers tested the instrument's reliability, and the internal consistency reliability estimate (Cronbach's alpha) ranged from 0.7 to 0.82 (Riley et al., 2004). Moreover, previous studies have revealed the appropriate content validity of CHIP-CE/CRF (Matza et al., 2004; Rebok et al., 2001). The instrument's reliability in the current study ranged from 0.71 to 0.86 across the subscales, as shown in Table 1.
The Reliability of CHIP-CE/CRF Health Status Subscales.

After obtaining approval from the authors, the CHIP-CE/CRF was translated into Arabic, following the WHO guidelines for translation (World Health Organization, 2023). Then, the researchers in this study, experts in child health, and a translator conducted a back-translation of the Arabic version into English. Finally, this English version and the original instrument were compared, and the necessary changes were made accordingly. A pilot study was conducted on the Arabic version prior to data collection. Children of the pilot study were excluded from the study sample.
Data Analysis
The Statistical Package for Social Science (SPSS) version 21 was used to analyze the study's data (IBM Corporation, 2012). Descriptive statistics, including the mean, percentage, and standard deviation, were used for continuous variables. Categorical variables were analyzed using frequencies and percentages. To facilitate comparison between scales with different numbers of items, the subscales of health status were transformed into a score out of 100. Total scores were calculated for all subscales. The differences in children's responses on health status subscales according to their characteristics and parents’ characteristics were analyzed using one-way analysis of variance (ANOVA) and a t-test. Results were considered statistically significant if α ≤ 0.05.
Results
The study approached 1100 students. The number of students who participated in the study was 1050 (95% response rate). However, 100 incomplete questionnaires were excluded from the study; thus, the total sample included was 950. The sample consisted of 616 girls (64.3%) and 334 boys (35.2%). Most of the children's mothers, 358 (37.7%), and fathers, 293 (30.8%), had completed their high school education. Additionally, a significant number of children, 673 (70.8%), were enrolled in medical insurance. Furthermore, over half of the fathers, 529 (55.7%), were smokers. The demographic characteristics of the participants are presented in Table 2.
Demographic Characteristics of Study Participants (N = 950).

Children-Reported Health status
Table 3 presents the means of the raw and standardized scores for the five health status subscales. The satisfaction subscale has the highest mean, followed by the achievement subscale. The comfort subscale has the lowest mean.
Means of CHIP-CE/CRF Subscales of Health Status.
Differences in Children's Health status According to Demographic Variables
Significant differences in children's health status were found in relation to the child's gender, age, father's level of education, and father's smoking status (see Table 4). No statistically significant differences were found in health subscales in regard to medical diagnosis, the mother's level of education, monthly family income, number of children, medical insurance, and employment status.
Significant Differences in Children's Health Status.

Child Gender
The results of the t-test revealed a statistically significant difference in the risk avoidance subscale among girls and boys (t(949) = -9.95, p < 0.001). Girls reported higher means of the risk avoidance subscale compared to boys. The results of the t-test also revealed a statistically significant difference in the achievement subscale between girls and boys (t(949) = -5.89, p < 0.001). Girls reported higher means of achievement subscale (compared to boys). No statistically significant differences were found in other subscales regarding the child's gender.
Childs’ age
The results of the ANOVA test revealed a statistically significant difference in the resilience subscale according to child age (F(5, 945) = 2.49, p = 0.03). Scheffe's post hoc criterion for multiple groups’ comparison was carried out, and a statistically significant difference was revealed between the groups. Children aged 10 years reported higher means of resilience than 9-year-old children (p = 0.037). The results of the ANOVA test also revealed a statistically significant difference in the achievement subscale according to child age (F(5, 945) = 2.82, p = 0.016). Statistically significant differences were found between groups using the Scheffé post hoc criterion for multiple comparisons. Children aged 11 years reported higher means on the achievement subscale than 9-year-old children (p = 0.033). Additionally, the results of the ANOVA test revealed a statistically significant difference in the risk avoidance subscale according to child age (F(5, 945) = 7.65, p < 0.001). Scheffe's post hoc criterion for multiple groups’ comparison was carried out, and a statistically significant difference was revealed between the groups. Children aged 11 years reported higher means of risk avoidance subscale than 8-year-old children (p = 0.001) and 9-year-old children (p = 0.008). Children aged 12 years reported higher means on the risk avoidance subscale than 8-year-old children (p < 0.001), 9-year-old children (p < 0.001), and 10-year-old children (p = 0.017). The results of the ANOVA test also revealed a statistically significant difference in the satisfaction subscale according to child age (F(5, 945) = 2.24, p = 0.048). Scheffe's post hoc criterion for multiple groups’ comparison was carried out, and a statistically significant difference was revealed between the groups. Ten-year-old children reported higher means on the satisfaction subscale than 9-year-old children (p = 0.027).
Father Educational Level
The results of the ANOVA test revealed a statistically significant difference in satisfaction with the health subscale according to fathers’ level of education (F(6,944) = 2.24, p = 0.038). Scheffe's post hoc criterion for multiple groups’ comparison was carried out, and statistical significance was found between the groups. Children whose fathers have diploma degrees reported higher means of satisfaction with the health subscale than children whose fathers have high school (p = 0.023) and master's degrees (p = 0.007). Children whose fathers hold bachelor's degrees reported higher satisfaction with the health subscale than children whose fathers hold a master's degree (p = 0.023). Children whose fathers hold PhD degrees reported higher satisfaction with the health subscale than children whose fathers have less than a high school education (p = 0.032) and those with a master's degree (p = 0.009).
Discussion
This study aimed to assess the health status of school-age children. The satisfaction subscale, which measures satisfaction with oneself and one's health, recorded the highest mean score (M = 87.7). This was followed by the achievement subscale (M = 86), which reflects effective role functioning in school and with peers. In contrast, the comfort subscale, which assesses the experience of physical and emotional symptoms, had the lowest mean score (M = 78.8). Notably, girls reported significantly higher scores in achievement and risk avoidance domains than boys.
Additionally, children aged 10 and 11 demonstrated significantly greater levels of achievement and resilience compared to those aged 9. Furthermore, the risk avoidance domain scores were higher among 11- and 12-year olds than those aged 8 and 9. Lastly, children's health status differed significantly according to the father's educational level and smoking status.
Children's Reported Health status
Children in the current study reported the highest mean scores in satisfaction and achievement domains, respectively. The highest score on the satisfaction domain may be interpreted as indicating that children have high self-esteem and a good perception of their wellbeing. Their high score on achievement may suggest that they were successful in their school performance and their social relationships with peers and teachers. Conversely, the comfort and resilience domains have the lowest means. This result may indicate that the child in the current study experienced high levels of physical and emotional symptoms. Resilience reflects positive, adaptive behavior and serves as a protective factor among children when confronted with stressful conditions. It can be enhanced by social support from family and school, engaging in physical activity, and consuming a proper diet (Meserole et al., 2014). Studies have highlighted the relationship between family support and good physical and mental health (Scrimin et al., 2022; Tang et al., 2021). Prenatal stress may be associated with children's physical and emotional discomfort (Scrimin et al., 2022). To reflect on the Jordanian context, this may mandate policymakers and healthcare providers, particularly nurses, to prioritize overall family wellbeing. Ultimately, the goal is to design comprehensive family support interventions that promote children's comprehensive health status. Similar findings were reported previously among children from Turkey (Canaz et al., 2017). Unlike children in the current study, two studies from the USA showed that children reported high scores on the comfort and resilience domains (Meserole et al., 2014), while less than one-third of the children reported physical discomfort and low satisfaction with their health condition (Trout et al., 2018). Children from Spain reported the highest scores on wellbeing, satisfaction, and risk avoidance, as well as lower scores on performance and resilience (Martínez-Torres et al., 2024). Opposite to the children in our study, children from the Pacific reported higher scores on the satisfaction domain and lower scores on the comfort domain (Langridge et al., 2022).
However, the scores for all domains in the current study were lower than those of children from Spain (Estrada et al., 2012) and the USA (Riley et al., 2004). These results may present a challenge to paying more attention to this age group at all levels, in partnership with Jordan's health, educational, and social sectors.
Differences in the Health status of Children
In the current study, girls reported higher mean scores on achievement and risk avoidance subscales than boys. Similarly, girls in Portugal and Spain reported higher scores on risk avoidance than boys (Alves Rodrigues & Alves Apóstolo, 2010; Estrada et al., 2012). In another study from Romania, girls reported lower levels of health satisfaction, emotional comfort, and physical fitness. Still, they reported higher scores on risk avoidance (Cheie & Miu, 2016). Additionally, girls exhibited higher levels of risk avoidance than boys; however, boys demonstrated higher academic performance and comfort scores than girls in studies from Spain and the Pacific Islands (Estrada et al., 2012; Langridge et al., 2022). Another study found that girls scored higher on risk avoidance, achievement, resilience, and satisfaction than boys, who scored higher only in the comfort domain (Riley et al., 2004). In the current study, gender differences in the achievement domain may suggest that girls tend to study more seriously in class and complete their homework more diligently than boys. Also, in the current study, girls reported higher scores on risk avoidance than boys. One suggestion may be explained within the context of differences in personality attributes between girls and boys; that is, risk-taking is an attribute of a masculine approach to gaining power and position (Byrnes et al., 1999). Another suggestion from a cultural perspective is that parents may put more restrictions and monitoring interventions on girls’ behaviors than on boys.
In the current study, children aged 10 and 11 reported higher mean scores on the resilience, achievement, risk avoidance, and satisfaction subscales than children aged 8 and 9. Also, children aged 12 years reported higher means on the risk avoidance subscale than children aged 8, 9, and 10 years old. This suggests that children may develop better adaptive strategies with age advancement. Along the same line, younger children from Tonga had lower scores on resilience, achievement, and satisfaction domains than older children (Langridge et al., 2022). Younger children expressed more physical symptoms and discomfort than older children, who consistently focused on emotional wellbeing, in a study conducted in Italy (Patron et al., 2021). Inconsistently, a study conducted in England showed that younger children reported higher scores on risk avoidance, satisfaction, achievement, and resilience than older children (Coghill & Hodgkins, 2016). Another result from the current study indicated that children of fathers who hold university-level degrees have higher satisfaction scores with their health than those of fathers who hold lower degrees. Along the same line, a study from Spain found that children of parents with non-university education had significantly higher health complaints than their counterparts whose parents had a university education (Padilla-Moledo et al., 2016).
Strengths and Limitations
This study may have the strength of providing new data on the health status of school-age children in Jordan. However, a few limitations should be stated. First, “causation” could not be evaluated due to the cross-sectional methodology employed in the current study. Selection bias is another limitation, as the children were selected using convenient sampling from the Amman District only. Therefore, the results may not accurately represent the large school-age child population across other Jordanian districts. More replicated studies should include a more representative sample, and a larger sample may allow for additional validation of findings and further analyses to evaluate the health status of school-age children in Jordan. Response bias due to the use of a self-administered questionnaire is another limitation. Future studies examining children's health status could obtain information about children's health from both the child and their parents.
Study Implications
The study findings could inform nursing practice by providing data about children's health status from their perspective and offer a contextual understanding of children's health from different domains, which may motivate nurses to deliver holistic, quality, child-centered care tailored to these domains. For policy-making, the study findings may be considered a tool for monitoring children's health domains from their perspective, considering them active participants. This may add national data on children's health domains to inform the development of more initiatives and health education programs based on these domains. Another recommendation could be to conduct mixed-methods studies, which may provide a comprehensive picture of the health status of school-age children. Collecting information about a child's health status from the child and their parents is also recommended for future studies.
Conclusion
School-age children's reports of health status varied across different domains. The achievement, risk avoidance, and satisfaction scores were rated high. In contrast, the comfort domain was the lowest. Children's health status differed significantly according to children's age and gender, father's educational level, and smoking status. These results suggest the need for further assessment of children's health status and the implementation of significant interventions by family, school, and healthcare providers, particularly nurses, to improve children's health status in the comfort domain.
Footnotes
Ethics Considerations
The ethical approval was received from the Institutional Review Board (IRB) Committee at The University of Jordan. Consent was obtained from the eligible participants after explaining the purpose of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by The University of Jordan.
Declaration of Interest
The authors declare that they have no known interests or personal relationships that influence the work reported in this paper.