
Abstract
Introduction
Despite the World Health Organization declaring COVID-19 no longer a public health emergency, reports of long COVID persist globally, raising concerns about its impact on individuals.
Objective
This retrospective study aimed to explore the symptom experiences of individuals with long COVID-19 and examine the relationship between those experiences and perceived negative health status in Thailand.
Methods
The study focused on individuals with moderate to severe COVID-19 infections. Between July 3, 2022 and December 1, 2022, we conducted telephone interviews with 86 individuals who tested positive for SARS-CoV-2 and received outpatient care in Bangkok. The COVID-19 Yorkshire Rehabilitation Screening was utilized to measure symptom occurrence, duration, severity, and health status on an 11-point numerical rating scale from 0 (none or excellent) to 10 (the worst). A Spearman rank correlation was used to analyze the relationships between long COVID symptoms and negative perception of health status.
Results
Among the participants, 75.6% had long COVID, with a median of three symptoms lasting for a median duration of 5.6 months. Difficulties in performing daily activities were most common, reported by 50.8% of participants. The majority (80.0%) experienced itching, headache, cognition, muscle pain, continence, and sleeping problem for 6 months. Loss of taste was the most severe symptom, with a mean severity rating of 8.8. There were significant positive relations between a negative perception of health status and multiple symptoms, symptom severity, functional disability, and additional symptoms.
Conclusion
Individuals with moderate to severe COVID-19 infection who experienced long COVID had poorer perceived health status. To effectively manage and improve the health status of individuals with long COVID, nurses should provide follow-up care, assess not only the occurrence of symptoms but also their duration and severity, and evaluate performance outcomes.
Introduction
Although the World Health Organization (WHO) has declared that the coronavirus 2019 disease (COVID-19) is no longer a public health emergency (WHO, 2023a), there have been reports from individuals across the world about experiencing long COVID. According to WHO (2021), long COVID is defined as an illness that occurs within 3 months after infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and lasts for at least 2 months. Studies have estimated that approximately 50%–70% of hospitalized cases, 10%–30% of nonhospitalized cases, and 10%–12% of vaccinated cases may experience long COVID (Davis et al., 2023). Common symptoms of long COVID include fatigue and shortness of breath (Aiyegbusi et al., 2021; Arjun et al., 2022; Cha & Baek, 2021; Fernández-de-Las-Peñas et al., 2021; Zeng et al., 2023), which can last from 1 month to several months (Tran et al., 2022). Several factors have been associated with long COVID, including older age, female gender, comorbidities, obesity, predominant variant at the time of infection, and unvaccinated status (Aiyegbusi et al., 2021; Jabbari et al., 2022; Perlis et al., 2022; Robertson et al., 2023).
In Thailand, as of December 1, 2022, there were 4,704,642 reported cases of COVID-19 and 33,285 deaths, with a 77.0% vaccination rate for two doses (Department of Disease Control, 2023). Individuals with a confirmed SARS-CoV-2 infection received essential drugs for supportive care at home, provided at no cost. Nurses conducted daily calls to track vital signs, follow up on symptoms, manage medications, and deliver health education, counseling, and emotional support. They also communicated with the doctors to identify patients at high risk of severe disease progression and facilitate referrals when necessary. However, once patients were discharged upon completing isolation, a follow-up was not conducted as it was not included in the reimbursement package. Instead, patients were advised to seek care according to their healthcare scheme. Therefore, conducting this study in Thailand is important to understand the burden of long COVID and its impact on individual health status. The findings can inform future healthcare strategies regarding the need for extended reimbursement to support ongoing care for patients with long COVID when necessary.
The perceived health status is an individual's subjective evaluation of their physical, psychological, and social well-being, and it is affected by long COVID. Among individuals who initially had mild to moderate COVID-19 and experienced long COVID, the impact on their general well-being ranged from moderate (43%) to severe (33%) (O’Mahony et al., 2022), and the median score for perceived health status was 78 out of 100, indicating a good overall health status (Han et al., 2022). However, there is limited understanding of the perceived health status as an impact of individuals with moderate to severe COVID-19 who experienced long COVID in the literature.
Review of Literature
The Theory of Unpleasant Symptoms provides a useful framework for assessing the duration, quality, intensity, and distress of symptoms (Lenz et al., 1997). Nurses can use this framework to understand how symptoms across these dimensions affect an individuals’ ability to function independently and provide appropriate support to manage symptoms. However, despite long COVID symptoms in the literature (Davis et al., 2023; Lopez-Leon et al., 2021), only a few studies report on their duration and severity. For instance, Blomberg et al. (2021) found that 52% (32 out of 61) of home-isolated patients diagnosed with COVID-19 in Norway experienced long COVID at 6 months, while Silverberg et al. (2022) reported a median duration of 11 months for long COVID among individual who tested positive for SARS-CoV-2 antibodies in the United States. With regard to symptom severity, Herrero-Montes et al. (2022) found that hospitalized COVID-19 survivors in Spain reported a mean score of 7.7 (SD: 6.5) out of 24 points for the severity of post-COVID pain. Similarly, Ziauddeen et al. (2022) found that adults in the United Kingdom who thought they had COVID-19 in the Spring of 2020 had a mean score of 5.5 (SD: 1.4) out of 10 points for fatigue severity.
In addition, the Theory of Unpleasant Symptoms suggests that symptoms can have a significant impact on functional, cognitive, and physical performance (Lenz et al., 1997). While quality of life is the most common reported outcome for long COVID, functional health status and perceived health status have also been studied. Several studies found that individuals with long COVID reported impaired quality of life when compared to those without the condition (Aiyegbusi et al., 2021; Han et al., 2022; Líška et al., 2022; de Oliveira et al., 2022; Sarda et al., 2022; Tabacof et al., 2022; Verveen et al., 2022). In one particular study, functional health status was used as an outcome, and it showed that 32.0% (808 out of 2,550) of individual with long COVID reported severe functional limitations, indicating a need for assistance with daily activities (Ziauddeen et al., 2022). Likewise, another study conducted in the UK found a strong correlation between symptom severity and the health status of long COVID patients (O'Connor et al., 2022). However, two additional studies reported little impact of long COVID on the general well-being and overall health status (Han et al., 2022; O’Mahony et al., 2022).
The literature review highlights the limited understanding of the duration and severity of long COVID symptoms and their impacts on individuals’ lives. Additionally, there are inconsistencies in the reports on the effects of long COVID on the general well-being and health status, indicating a need for more research in this area. Despite the existing knowledge gaps, particularly in relation to the general well-being and health status, this study aims to contribute by exploring the symptom experiences of individuals with long COVID who have had severe to moderate COVID-19 infections and examining the relationship between those experiences and perceived negative health status. The research hypothesis is that there is a positive correlation between symptom severity, functional disability, additional symptoms, and perceived negative health status.
Methods
Design
This was a retrospective, single-facility study to investigate participants’ experience of long COVID, characterized by the presence of symptoms lasting for at least 2 months after acute infection with SARS-CoV-2. The study adhered to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Research Questions
The research questions for this study were as follows: (1) What were the experiences of individuals with long COVID in terms of their symptoms? and (2) How were these experiences related to their perceived negative health status?
Sample
The study recruited individuals aged 18 years or older who had tested positive for COVID-19 through reverse transcription polymerase chain reaction (RT-PCR) testing and had moderate to severe infection.
Inclusion/Exclusion Criteria
To be included in the study, individuals needed to be registered to receive a home care service at an outpatient facility in Bangkok between July 29, 2021 and October 31, 2021. As part of the service, they received tele-case management, herbal medicines or antivirals (favipiravir), and meals for 14 days. Those who died during the home isolation period or within 6 months after discharge, as well as individuals who were too ill to respond to the questionnaire, were excluded from the study.
The sample size for this study was calculated based on a 0.3 (one-tailed) effect size taken from the literature (O'Connor et al., 2022), using the G*Power 3.1 program with the correlation: bivariate normal model. This study required a minimum of 67 participants to maintain a significance level of 5% (α) and statistical power of 80% (1−β). To account for potential losses due to changes in phone numbers, an additional 20% of participants were included, resulting in a total of 81 participants in the study. We used Excel and the RANDBETWEEN function to randomly select participants from a list of 908 patients who had been classified as having a moderate to severe infection.
Data Collection
Between June 9, 2022 and September 25, 2022, we made multiple attempts to contact eligible individuals via the phone numbers that they provided on the day of their admission. During these phone calls, we invited them to participate in the study and provided them with information about its purpose. Those who expressed interest in participating were sent participant information sheets and consent forms by mail. In total, 86 participants provided full written informed consent, with 69 consenting by mail and the remaining 17 consenting via SMS with digital informed consent provided in pictures.
Between July 3, 2022 and December 1, 2022, all participants underwent phone interviews to ensure their full understanding and accurate responses to the self-report version of the COVID-19 Yorkshire Rehabilitation Screening (C19-YRS) questionnaire. These interviews aimed to capture the participants’ symptom experiences 6 months after being discharged from the home care service. The chosen duration of 6 months was based on reports from the WHO (2021) and the existing literature (Arjun et al., 2022; Blomberg et al., 2021; Huang et al., 2022) indicating that some individuals with long COVID experience symptoms for 6 months.
To ensure data collection consistency and minimize information bias, a 1-day training session was conducted for the nine interviewers. The training covered important aspects such as the informed consent process, accurate reading of questionnaire questions, and proper guidance for the participants to rate the severity of their symptoms on a scale of 0–10. The questionnaire itself included an introduction script outlining its purpose and instructions. Additionally, a guide for the rating scale was provided alongside each question to serve as a reminder for interviewers, with specific focus on assessing perceived negative health status (where 0 represents excellent and 10 represents the worst).
Data Collection Tool
The C19-YRS questionnaire, self-report version, was selected for this study because it included relevant variables that align with the research objectives, particularly focusing on long COVID symptoms and perceived health status. The questionnaire in English is designed to measure the occurrence and severity of symptoms of long COVID as well as overall health. The questionnaire consisted of 22 items and is divided into four subscales.
The first subscale, symptom severity, includes 10 items such as breathlessness, cough, swallowing, fatigue, continence, pain, cognition, anxiety, depression, and posttraumatic stress disorder (PTSD). Item 1–10 are rated on an 11-point numerical rating scale ranging from 0 (none of this symptom) to 10 (extremely severe level). Higher summed scores (ranging from 0 to 100) on this continuous variable indicate more severe symptoms.
The second subscale, functional disability, consists of five items such as communication, mobility, personal care, activities of daily living, and social role. Item 11–15 are scored with an 11-point numerical rating scale from 0 (no problem) to 10 (inability to do). Higher summed scores (ranging from 0 to 50) on this continuous variable indicate more severe functional problems.
The third subscale, overall health (item 16), includes only one item (item 16) and is assessed using an 11-point numerical rating scale from 0 (the best health) to 10 (the worst health). It is a continuous variable.
The fourth subscale, additional symptoms, contains six items, including palpitations, dizziness, weakness, sleep problems, fever, and skin rash. Item 17–22 are rated on an 11-point numerical rating scale from 0 (none of this symptom) to 10 (extremely severe level). Higher summed scores (ranging from 0 to 60) on this continuous variable indicate more severe additional symptoms. The participants were also given the opportunity to report any other symptoms not listed in the questionnaire.
The questionnaire had been previously validated in research with a Cronbach's α coefficient of 0.89 (Halpin et al., 2021; O’Connor et al., 2022), and it was used with permission from the developer.
The researchers translated the questionnaire from English to Thai, targeting individuals with a literacy rate of at least 6 years of schooling. The Thai version was tested on three individuals with primary school education to ensure its comprehensibility. The content validity of the translation was assessed through two rounds of evaluation by three technical experts conducted on March 24, 2022 and April 16, 2022, as part of the Ethics Committee's approval process for the study. In this study, the Cronbach's alpha coefficient for the Thai version was found to be .88, indicating excellent internal consistency (Devellis, 2012). The study made slight modification to the original version of the C19-YRS questionnaire, which included adding the duration of symptoms and removing an item related to social role (Item 15) due to the context of the Thai culture. However, a separate study that translated the C19-YRS questionnaire from English to Thai conducted during the same period as the present study reported a Cronbach's alpha coefficient of .72 (Partiprajak et al., 2023).
Institution Review Board Approval
The study received approval from the ethics committee, and all participants provided written informed consent prior to their participation.
Statistical Analysis
Descriptive statistics were utilized to analyze the data. For categorical variables, frequency and percentage were used, while for continuous variables, mean and standard deviation or median (interquartile range: IQR) were used. Before conducting correlation analyses, the normality of the variables related to symptom severity, functional disability, and additional symptoms, and perceived negative health status was assessed using the Kolmogorov–Smirnov test. However, none of the variables met the normality assumption (p-value < .001). Therefore, nonparametric statistics, the Spearman rank correlation test, was used to examine the relationships between long COVID symptoms and perceived health status.
Results
Sample Characteristics
A total of 86 participants took part in the study, with 75.6% of them experiencing long COVID. The participant characteristics of those with and without long COVID are summarized in Table 1. Of all the participants, 55.8% were male, and the median age was 53.1 years. Universal health coverage was held by 53.5% of the participants (46 out of 86). Additionally, 66.3% had underlying medical conditions, and 88.4% had been vaccinated.
Sample Characteristics at Baseline.

Note. SD = standard deviation; COVID-19 = coronavirus disease 2019; CXR = chest x-ray.
Research Question Results
Prevalence and Multi-Dimension of Long COVID Symptoms
The study found that 75.6% of participants experienced long COVID, with a 95% confidence interval between 65.3% and 83.6%. Out of the 65 participants who had long COVID, the median number of symptoms was 3, with an IQR of 2–7. The median duration of long COVID symptoms was 5.6 months, with an IQR of 3.7–6 months since the time of the acute phase of the infection. The occurrence and duration are presented in Figure 1, which shows that difficulties in performing daily activities were the most commonly reported symptom, experienced by 50.8% of participants. A majority (80.0%) of participants reported experiencing itching, headache, cognition, muscle pain, continence, and sleeping problems for a duration of 6 months.

Occurrence and duration of long COVID symptoms.
The severity of symptoms is presented in Figure 2, and the study found that loss of taste was the most severe symptom, with a mean severity rating of 8.8.
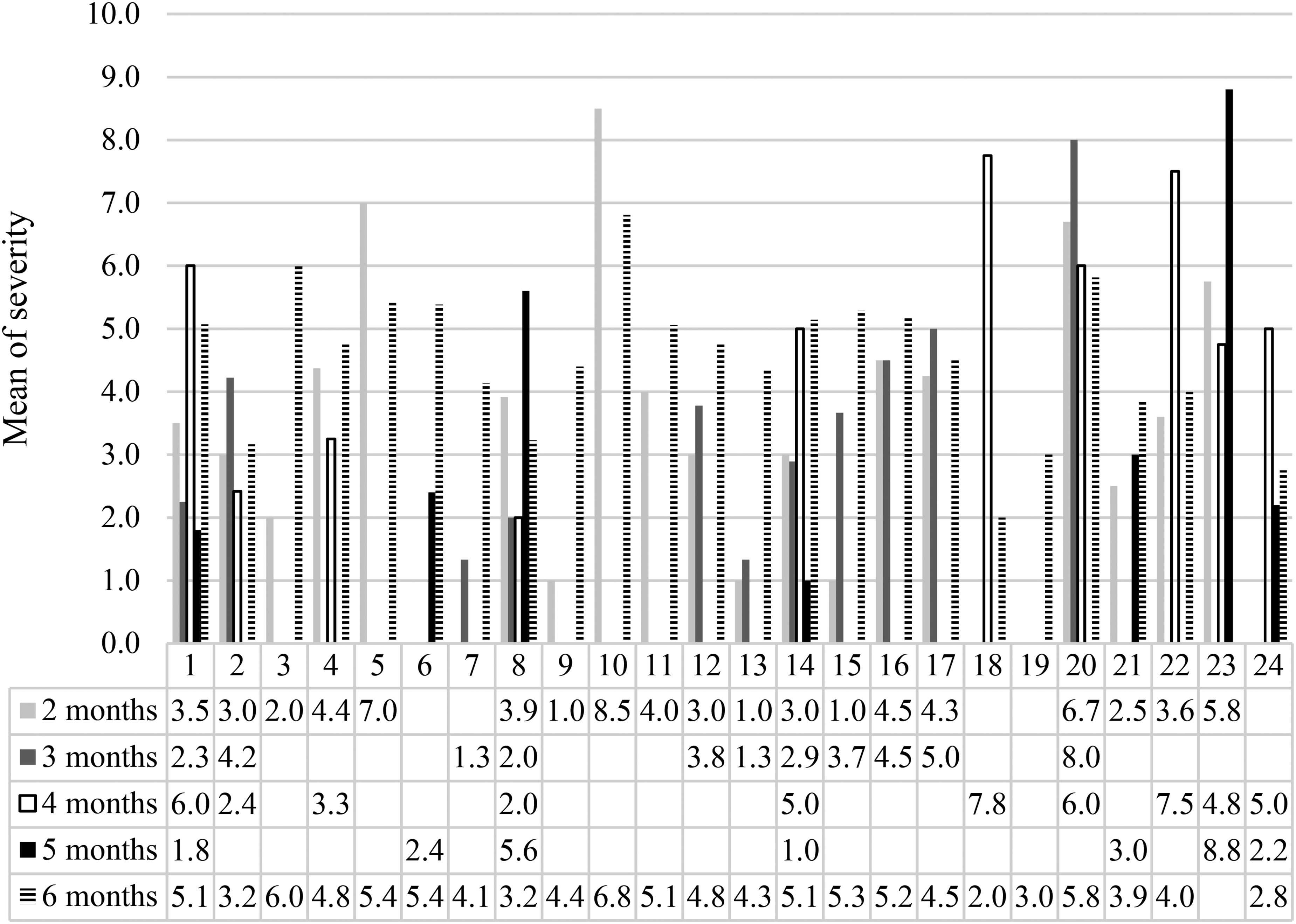
Severity of long COVID symptoms.
Relationship Between Symptom Experience and Perceived Negative Health Status
In Table 2, the scores of each subscale were as follows: symptom severity (breathless, cough, swallowing, fatigue, continence, pain, cognition, anxiety, depression, PTSD screen), a mean score of 8.3 (SD = 9.6), out of 100; functional disability (communication, mobility, personal care, daily living), a mean score of 5.1 (SD = 6.4), out of 40; additional symptoms (palpitations, sleeping problems, fever, skin rash, hair loss), a mean score of 3.9 (SD = 6.4), out of 40; and perceived negative health status, a mean score of 1.5 (SD = 2.4), out of 10.
The C19-YRS Subscales.

Note. CR19-YRS = COVID-19 Yorkshire Rehabilitation Scale; SD = standard deviation; IQR = interquartile range; Perceived negative health status of 10 reflecting the worst; item severity of 10 reflecting the worst symptom.
Multiple symptoms demonstrated a significant correlation with perceived negative health status (ρ = .453, p-value < .001). Additionally, perceived negative health status showed a significant correlation with symptom severity, functional disability, and additional symptoms. Notably, symptom severity, functional disability, and additional symptoms were also found to be significantly correlated with each other (Table 3). These findings indicate that as symptom severity, functional disability, and additional symptoms increase, perceived negative health status tend to worsen.
Correlations Between Long COVID Symptoms and Perceived Negative Health Status.

Note. Perceived negative health status of 10 reflected the worst, and item severity of 10 reflected the worst symptom.
Discussion
The aim of this study was to evaluate the symptom experiences of individuals with long COVID and examine the relationship between those experiences and perceived negative health status. The results indicated that 75.6% of participants experienced long COVID, with multiple symptoms ranging from two to seven symptoms, and an average duration of 5.6 months. Difficulties in performing daily activities emerged as the most commonly reported symptom, while muscle pain was the symptom with the longest duration. Loss of taste was identified as the most severe symptom.
The findings revealed a higher occurrence of long COVID among specific groups, including females, individuals with primary education, low-income individuals, those with comorbidities, and the unvaccinated. These findings are consistent with other research studies (Blomberg et al., 2021; Global Burden of Disease Long COVID Collaborators et al., 2022; Huang et al., 2022; Robertson et al., 2023), which have also observed a high prevalence of long COVID among women, individuals with low socio-economic factors such as low education level and low-income level, those with comorbidities, and individuals without vaccination These results emphasize the importance of considering these factors when nurses assess at-risk population in which symptoms of long COVID are frequently observed.
In this study, the most frequently reported symptoms were difficulties in performing daily activities, breathlessness, and fatigue. While breathlessness and fatigue have been commonly reported in other studies (Aiyegbusi et al., 2021; Cha & Baek, 2021; Lopez-Leon et al., 2021), difficulties in performing daily activities have been reported as often. It is important to note that in our study, difficulties in performing daily activities referred to feel tired when doing housework or work. While this symptom is similar in meaning to breathlessness, it may be more easily understood in the Thai context. These common symptoms are related to respiratory system, which is also affected by SARS-CoV-2 infection through apoptosis, epithelial damage in the airway, and systematic inflammation (Davis et al., 2023).
In terms of symptom duration, the participants in this study reported that three specific symptoms (continence, pain, and cognition) under the severity subscale and two symptoms (sleeping problems and itching) under the additional symptom subscale lasted for a duration of 6 months. Other studies have also reported similar findings for the participants who initially had COVID-19 infection before the availability of COVID-19 vaccines, such as fatigue lasting for 2 months (Saad et al., 2021), 6 months (Blomberg et al., 2021), and even up to 11 months (Silverberg et al., 2022), while dyspnea lasted for 2 months (Saad et al., 2021). The duration of long COVID symptoms may be due to the impact of the SARS-CoV-2 virus on different pathogenesis mechanisms, such as immunology, virology, vascular tissue, neurological and cognitive systems, respiratory system, and gastrointestinal system (Davis et al., 2023).
While previous studies have not focused on symptom severity in long COVID, this study found that PTSD, hair loss, and loss of taste were reported as the most severe symptoms. This contrasts with previous studies that reported pain (Herrero-Montes et al., 2022) and fatigue (van der Maaden et al., 2023; Ziauddeen et al., 2022) as the most severe symptoms. Symptom severity indicates seriousness of the condition, and it is important to note that patients may be most bothered by these severe symptoms.
The Theory of Unpleasant Symptoms (Lenz et al., 1997) suggests that individuals who encounter a higher number, longer duration, and greater severity of symptoms are likely to experience greater challenges in maintaining their performance, including functional and cognitive activities. This study provides support for the theory by demonstrating a significant association between a higher number of long COVID symptoms and poorer health status among participants. Also, we identified strong correlations between symptom severity, functional disability, additional symptoms, and perceived negative health status. This suggests that individuals with more symptoms and severity experience a greater impact on their overall health status.
In Thailand, studies on long COVID have been published in local peer-reviewed journals. However, these studies did not adhere to the WHO (2021) definitions of long COVID, which define it as an illness occurring within 3 months after infection with SARS-CoV-2 infection and lasting for at least 2 months. As a result, the implications of these studies are limited. The Thai healthcare system's response to COVID-19 has been recognized and awarded by the United Nations Public Service Awards (UNPSA) in 2021 (UNPSA, 2023). However, its primary focus has been on stopping transmission, and once the isolation period is over, the work is considered complete. Currently, there is no active system in place to provide specialized care for individuals with long COVID. Instead, individuals are encouraged to seek care from the routine healthcare system where healthcare team, including nurses, may not have specialized expertise in managing long COVID.
Strengths and Limitations
Phone interviews offer an interactive approach to data collection, which distinguishes them from online survey. This interactive nature allows interviewers to gather accurate responses directly from the participants. However, it is important to acknowledge several limitations that are presented in this study. Firstly, data collection at a single setting may limit generalizability of the results. Secondly, the self-report nature of the data collection may have introduced inaccuracies or recall bias, particularly for those whose initial infection occurred 10–12 months ago. Thirdly, the questions used in this study were slightly modified from their original form, making it challenging to compare results with other studies using the same instruments. Finally, the distress dimension in the Theory of Unpleasant Symptom was not assessed in this study, which may limit the understanding of the emotional impact of long COVID.
Implications for Practice
The study has shown that long COVID symptoms can be both severe and long-lasting, highlighting the need to evaluate not only the occurrence of symptoms, but also their duration and severity. Nurses play a crucial role in assessing multiple dimensions of long COVID symptoms and suggesting appropriate care strategies for managing them. In addition, as many COVID-19 cases can be effectively managed at home, nurses can develop user-friendly tools such as symptom checklists and warning signs to assist individuals in making informed decisions about seeking additional care. These efforts align with WHO's (2023b) recommendation that safe and scalable care is a critical component of managing COVID-19 over the long term. Also, it is crucial for policymakers to consider the establishment of specialized clinics dedicated to managing long COVID.
Conclusions
Our study found a high prevalence of long COVID, with symptoms varying in occurrence, duration, and severity. While some symptoms, such as difficulty of performing daily activities, breathlessness, and fatigue, were common, other symptoms, including continence problems, pain, cognitive impairment, sleeping problems, and itching, persisted for 6 months. The most severe symptoms reported were PTSD, hair loss, and loss of taste. We found a significant association between a higher number of long COVID symptoms and worse health status. Additionally, perceived negative health status demonstrated significant correlation with symptom severity, functional disability, and additional symptoms.
Footnotes
Acknowledgments
The authors extend their gratitude to all study participants for their time to complete the questionnaire. Additionally, the authors would like to express appreciation to Lecturer Dr. Kanjanee Phanphairoj, Faculty of Nursing, Chulalongkorn University, for her valuable statistical guidance.
Author Contributions
BP: The conception and design of the study, acquisition of data and final approval of the version to be submitted. SJ: The conception and design of the study, analysis, interpretation of data, drafting the article, revising it critically for important intellectual content and final approval of the version to be submitted. ST: Acquisition of data and final approval of the version to be submitted. KM: Acquisition of data and final approval of the version to be submitted. JP: Acquisition of data and final approval of the version to be submitted. MS: Acquisition of data and final approval of the version to be submitted. TS: Acquisition of data and final approval of the version to be submitted. OK: Acquisition of data and final approval of the version to be submitted. SF: Acquisition of data and final approval of the version to be submitted. TT: Acquisition of data and final approval of the version to be submitted. PI: Acquisition of data and final approval of the version to be submitted. KS: Acquisition of data and final approval of the version to be submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Fund, Thailand Science Research and Innovation (grant number FFB650090/0017, 2022).
IRB Approval
The study received approval from the Ethics Committee for Research related to COVID-19 Disease and Public Health Emergency, Department of Disease Control in Thailand (Reference number: FWA 00013622 dated April 25, 2022)”, and all participants provided written informed consent prior to their participation.