
Abstract
Objectives
This study aims to assess the linguistic and cultural validity of the translated Multidimensional Scale of Perceived Social Support (MSPSS) in Persian, ensuring that the nuances of social support are adequately captured and comprehended by Iranian cancer patients.
Methods
In this cross-sectional study, 400 cancer patients from Iran were assessed using the MSPSS. By using exploratory factor analysis (with Maximum Likelihood factor analysis and Promax rotation) and confirmatory factor analysis, the construct validity of this scale was assessed. To check for internal consistency, the average inter-item correlation, Cronbach's alpha, and McDonald's omega coefficients were used.
Results
Most of the participants ranged in age from 49 to 59 years (n = 102, 34%). Two factors were extracted from EFA and the total cumulative variance explained by these factors was 61% of the total variance. Item factor loadings varied between 0.613 and 0.949. Internal consistency coefficients were considered acceptable (>0.7).
Conclusions
The Farsi version of the MSPSS as a self-report measure showed acceptable reliability and validity. Consequently, the scale can be used by nurses to evaluate perceived social support among Farsi-speaking cancer patients that can help them to take necessary actions to decrease the level of concern in these patients.
Background
Cancer remains one of the leading causes of morbidity and mortality worldwide, with the World Health Organization estimating approximately 19.3 million new cancer cases and 10 million cancer-related deaths globally in 2025 (WHO, 2022). These staggering figures highlight the urgent need to address not only the physical but also the psychosocial dimensions of cancer, which significantly impact patients’ overall well-being (Yoo et al., 2017). While the physical symptoms of cancer, such as fatigue, pain, and changes in appearance, are well-documented, the emotional and social challenges faced by cancer patients are equally profound and warrant closer attention (Yoo et al., 2017).
A cancer diagnosis often triggers a cascade of emotional responses, including anxiety, depression, and fear, which can persist throughout the treatment journey and beyond (Paley et al., 2023). The psychological burden of cancer is further exacerbated by social withdrawal and isolation, as patients may feel stigmatized or misunderstood by their communities (Costa et al., 2016). These emotional and social challenges can significantly impair patients’ quality of life, making it essential to identify resources that can help mitigate these effects.
One of the most critical resources for cancer patients is social support, which has been shown to play a pivotal role in enhancing emotional resilience, improving coping mechanisms, and fostering a sense of belonging and security (McDonough et al., 2019). Social support encompasses various forms of assistance, including emotional, informational, and instrumental support, all of which contribute to the patient's ability to navigate the complexities of their illness (Zamanian et al., 2021). Emotional support, such as empathy and understanding from family and friends, can provide comfort and reassurance, while informational support, such as advice and guidance, can help patients make informed decisions about their treatment (Chen et al., 2021). Instrumental support, including practical assistance with daily tasks, can alleviate some of the physical burdens associated with cancer, allowing patients to focus on their recovery.
The benefits of social support for cancer patients are well-documented. Studies have shown that patients with strong social networks experience lower levels of anxiety and depression, better treatment adherence, and improved overall quality of life (Ciria-Suarez et al., 2021; García-Torres et al., 2020). For instance, encouragement from family and friends can empower patients to remain resilient and actively engage in their treatment, while support groups provide a platform for patients to share their experiences and gain insights from others facing similar challenges (Clifton et al., 2022). Moreover, social support can act as a buffer against the emotional toll of cancer, helping patients maintain a positive outlook and a sense of control over their lives (Chen et al., 2021).
Despite the clear benefits of social support, the nature and effectiveness of such support can vary significantly across different cultural contexts. In Iran, where familial and societal structures hold profound significance, the dynamics of social support may manifest uniquely. Traditional values, familial interdependence, and cultural norms shape the way individuals perceive and seek support during their cancer journey (Sharif Nia et al., 2017). Family members often play a central role in providing care and emotional support, while friends may offer additional layers of companionship and practical assistance (Mokhtari et al., 2022). Understanding these cultural nuances is essential for developing effective interventions that can enhance social support for Iranian cancer patients. Given the importance of social support in the cancer journey, it is crucial to have reliable and valid tools to measure perceived social support in this population.
Review of Literature
Various scales exist for measuring social support in cancer patients, each with its unique focus and strengths. Scales such as the Medical Outcomes Study Social Support Survey (Moser et al., 2012), Social Support Questionnaire (Sarason et al., 1983), and Cancer Perceived Agents of Social Support (Goldzweig et al., 2010) have been widely used to assess different dimensions of social support, including emotional, informational, and instrumental support. However, for this study, we chose the Multidimensional Scale of Perceived Social Support (MSPSS), developed by Zimet et al. (1988), due to its specific advantages in capturing perceived social support from three distinct sources: family, friends, and significant others. The MSPSS is particularly well-suited for this study because it provides a concise yet comprehensive assessment of social support, making it easier to administer in clinical settings while still offering robust psychometric properties (Zimet et al., 1988). Unlike other scales that may focus on broader or more general aspects of support, the MSPSS allows for a nuanced understanding of how different social networks contribute to the well-being of cancer patients.
This is especially relevant in the Iranian cultural context, where family and close social ties play a central role in providing support during illness. Additionally, the MSPSS has been validated in multiple languages and cultural settings, demonstrating its adaptability and reliability across diverse populations (Dambi et al., 2018). Its adaptation and validation within the Iranian cultural framework remain limited, with only a few studies attempting to translate and validate the scale in Iran (Bagherian-Sararoudi et al., 2013; Ghorbani et al., 2014; Roohafza et al., 2016). These studies often lacked rigorous methodology, highlighting the need for a more systematic approach to ensure the scale's relevance and validity for Iranian cancer patients.
The MSPSS is particularly valuable because it captures the multidimensional nature of social support, allowing researchers and healthcare providers to assess the specific sources of support that are most beneficial to patients. Family support may be more stable and enduring, while support from friends may fluctuate based on the severity of the disease or individual circumstances (Procidano & Heller, 1983). By understanding these dynamics, healthcare providers can tailor interventions to address the unique needs of each patient, ultimately improving their emotional and physical well-being.
Social support is a critical resource for cancer patients, offering a buffer against the emotional and social challenges associated with the disease. The MSPSS provides a valuable tool for assessing perceived social support, but its adaptation to the Iranian cultural context requires careful consideration. This study aims to address this gap by rigorously evaluating the linguistic and cultural validity of the Persian version of the MSPSS, ensuring that it accurately captures the nuances of social support for Iranian cancer patients. By doing so, we hope to provide healthcare providers with a reliable tool to assess and enhance social support, ultimately improving the quality of life for cancer patients in Iran.
Methods
This methodological cross-sectional study was carried out between February to October 2024. Patients from two Tehran oncology clinics were recruited for this study.
Inclusion and Exclusion Criteria
Study inclusion criteria were: (1) a confirmed cancer diagnosis; (2) undergoing active treatment for cancer (surgical, chemotherapy, or radiotherapy treatments); (3) patients aged >18 years; (4) ability to speak Persian; and (5) willing and able to complete the study. Exclusion criteria were: (1) not in active cancer treatment and (2) patients with psychiatric disorders. No restrictions were considered for cancer types.
MacCallum et al. (1999) recommended a minimum sample size of 200 cases for psychometric studies. To ensure the construct validity, it was necessary to invite 400 individuals to participate (two different samples for construct validity). The participants were approached in the hospital wards following their surgeries. After receiving a thorough explanation of the study's objectives, they were invited to voluntarily participate and complete the perceived social support scale. The response rate for this study was 92%.
The Original Version of the Scale
The perceived social support scale was developed by Zimmet and deals with measuring an individual's perception of support from three sources: family, friends, and a significant other (Zimet et al., 1988). Response options are scored on a 5-point Likert scale (0–4) with the following scores: 4: never, 3: rarely, 2: sometimes, 1: often, and 0: always. It should be noted that items 4, 5, 7, and 8 were inverse items.
Translation
The scale was translated from English to Persian by the established translation protocols (Gudmundsson, 2009). Two skilled translators proficient in both English and Persian independently translated the perceived social support scale into Persian version. An expert panel, consisting of the authors of this article, and two professional translators, carefully reviewed and combined the two translations. Following this, an expert English translator was hired to translate the combined Persian version back into English. The panel of experts then reviewed and approved this final version. Then the panel of experts compiled and compared the results of the back-translation with the original scale to detect any differences and similarities between the original scale and the back-translated version. All items are translated into Persian and back-translated into English without any required modifications.
Normal Distribution, Outliers, and Missing Data
Skewness (±3) and kurtosis (±7) were used to individually investigate the univariate distribution of data. Also, the multivariate normality distribution was assessed by the Mardia coefficient of multivariate kurtosis (<8). Mahalanobis d-squared (p < 0.001) was used to determine whether there were any multivariate outliers (Sharif Nia, Kaur et al., 2021). The missing data were assessed using multiple imputations, and exploratory factor analysis used the pairwise deletion method to handle missing data.
Construct Validity
To assess the construct validity, the original dataset consisting of 300 cases was randomly split into two datasets, each containing 150 cases. The first dataset was subjected to Promax rotation, Maximum Likelihood Exploratory Factor Analysis (MLEFA), and Kaiser normalization. The eigenvalues (λ) were computed as the sum of squared factor loadings across all items (k) for each factor, representing the proportion of variance in each item that can be attributed to the factor. The eigenvalue was then divided by the total number of items to determine the percentage of total variance explained by each factor (Sharif-Nia et al., 2024). The Kaiser–Meyer–Olkin (KMO) measure exceeding 0.8 and the significance of Bartlett's test of sphericity (p < 0.001) were considered to confirm the suitability and relevance of the data for conducting factor analysis. The Eigenvalues of more than 1, communalities of more than 0.2, and factor loadings of more than 0.3 were also used for the factor extraction (Sharif Nia, She et al., 2021). The optimal number of factors has been determined using parallel analysis, a reliable statistical method that helps identify the ideal number of factors to keep in factor analysis (Hosseini et al., 2022). The MLEFA and parallel analysis were performed using JASP 19.
In the next step, the factor structures obtained from MLEFA were analyzed and confirmed by conducting confirmatory factor analysis (CFA) based on the second random dataset (n = 158) using AMOS version 27. The following model fit indices were used to assess the model fit: Comparative Fit Index (CFI), Normed Fit Index, Goodness-of-Fit Index, Relative Fit Index, and Incremental Fit Index (IFI) was >0.9; Parsimony CFI was >0.50; and for Minimum Discrepancy Function divided by degrees of freedom (CMIN/DF) < 5 was considered good (Hosseini et al., 2022).
Convergent and Discriminant Validity
Also, convergent validity was evaluated. For convergent validity, composite reliability (CR) should be greater than 0.7, and average variance extracted (AVE) should be greater than 0.5 for each construct. Fornell and Larcker (1981) stated that for psychological constructs, if AVE is less than 0.5, but CR is more than 0.7, the convergent validity can be considered acceptable. For the assessment of discriminant validity, we employed the heterotrait-monotrait (HTMT) ratio of correlations, as suggested by Henseler, Ringle and Sarstedt (2015). The HTMT ratio compares the average of the heterotrait-heteromethod correlations to the average of the monotrait-heteromethod correlations. A value below 0.90 signifies that divergent validity has been established between two reflective constructs (Henseler et al., 2015).
Reliability
The Cronbach's alpha, McDonald's omega, average inter-item correlation coefficient (AIC), CR, and Maximal Reliability (MaxR) were calculated to estimate the internal consistency and construct reliability. If the α, Ω, CR, and MaxR were greater than 0.7, and AIC values of 0.2–0.4 were interpreted as acceptable internal consistency (Hosseini et al., 2022).
Ethical Approval
The Ethics Committee of Mazandaran University of Medical Sciences (Sari, Iran) gave its approval to this study (Ethics code: IR.MAZUMS.IMAMHOSPITAL.REC.1403.016). The participants were given a thorough explanation of the study's goals and methods, as well as assurances that their participation was entirely voluntary. An informed consent was signed by each participant for participation in the research. Then, the researcher would give the scale to the patient to complete by themselves.
Results
Demographic Characters
Most of the participants ranged in age from 49 to 59 years (n = 102, 34%) and were primarily male (n = 162, 60.7%). See Table 1 for further demographic information.
Demographic Characteristics of Cancer Patients.

The Results of MLEFA
The results of MLEFA using the first random dataset (n = 150) extracted two factors accounting for 61% of the variance comprising nine items. The two items were removed from the original version. Moreover, the results of the KMO (0.821) and Bartlett's test of sphericity (p < 0.001, Chi-square = 1837.25, df = 36) showed the sampling was adequate and appropriate for conducting the factor analysis. The detailed results of the MLEFA are shown in Table 2.
The Result of MLEFA on the One Factor Persian Version of Perceived Social Support Scale (n = 150).

h2: Communalities; λ: eigenvalue.
The Results of CFA
The CFA was conducted to confirm and validate the factor structure obtained from MLEFA using the second random dataset (n = 150). The results showed that the data fit the model well as evidenced by (χ2 (26) = 89.36, p < 0.001, χ2/df = 3.437, CFI = 0.972, IFI = 0.972, TLI = 0.951). Figure 1 shows the results of the CFA final model.

The Results of the Confirmatory Factor Analysis (CFA) Model.
Convergent Validity and Reliability
The results showed that AVE for extracted factors was greater than 0.5, indicating good convergent validity. Cronbach's alpha, McDonald's omega, CR, and MaxR were greater than 0.7, and AIC was more than 0.2, demonstrating good internal consistency and construct reliability (Tables 1–3). As for divergent validity, the results of the HTMT ratio showed that the correlation between Work-Related Pain and Activity Limitations and Work Ability Prognosis 0.380, was lower than 0.90, demonstrating good discriminant validity for all constructs.
Indices of Construct Reliability, Convergent, and Divergent Validity (n = 158).
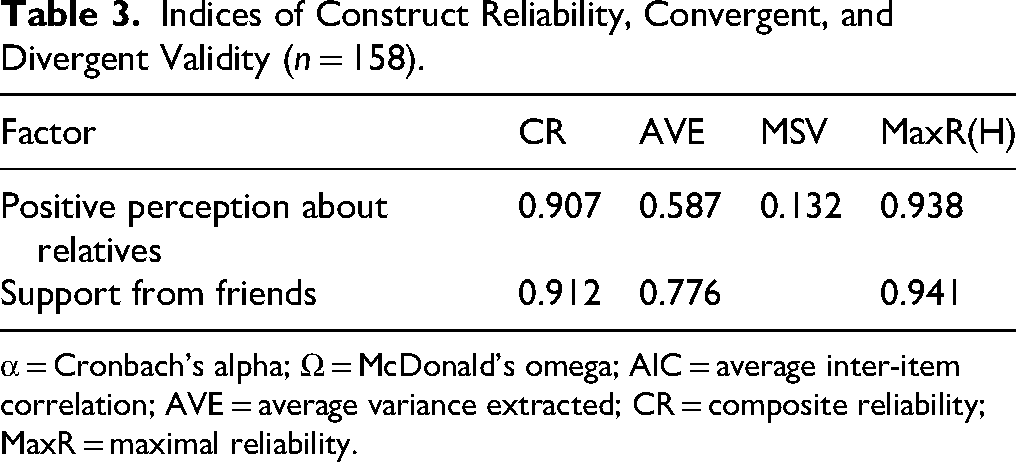
α = Cronbach's alpha; Ω = McDonald's omega; AIC = average inter-item correlation; AVE = average variance extracted; CR = composite reliability; MaxR = maximal reliability.
Discussion
Perceived social support is recognized as a crucial social determinant of health, serving as an effective moderating factor in individuals’ ability to cope with and adapt to life circumstances. It significantly impacts both physical and mental well-being, life satisfaction, and various dimensions of overall quality of life (Procidano & Smith, 1997). The study findings indicated that the MSPSS demonstrated acceptable validity and reliability.
Social support, being a subjective and multidimensional construct, is influenced by sociocultural contextual factors (Dambi et al., 2018). Given that the primary MSPSS comprises three factors (perception of support from family, friends, and other significant individuals), it becomes essential to explore the factor structure of this scale among Iranian cancer patients. The results of our exploratory factor analysis revealed that the Persian version of the MSPSS exhibits a two-factor structure that collectively accounts for 61% of the variance. In contrast, previous studies have predominantly supported the three-factor structure of the MSPSS, which includes perception of support from family, friends, and other important people. These three factors explained variances of 79.3% (Canty-Mitchell & Zimet, 2000), 41.20% (Canty-Mitchell & Zimet, 2000), and 80.05% (Sharif et al., 2021), respectively. In China context, the two-factor structure of the variance scale explained 74.03% (Wang et al., 2021).
The first factor within the two-factor structure of the MSPSS in our present study pertains to the positive perception of relatives. This factor involves an individual's subjective assessment or belief regarding the availability of help and resources from their family (Clark, 2022).
Given that cancer patients often face significant physical, psychological, and social challenges—such as anxiety, distress, and depression—family support becomes a critical coping resource (Alaloul et al., 2021; Zeilani et al., 2022). In the present study, this factor explained 42% of the total variance of the MSPSS. In other studies, consistent with the original version, this factor has been identified as one of the main dimensions of the MSPSS (Sharif et al., 2021; Wang et al., 2021). For example, in the study by Wang, who investigated the psychometric properties of this scale in family caregivers of patients with schizophrenia in China, 9.75% of the instrument variance was explained by the family factor. A reason that could explain these results in line with the present study may be cultural. In Asian societies, including Iran, the family holds a valuable position, and cultural norms emphasize the family's role as a vital source of care and support for its members, especially during illness or injury (Ghazzawi et al., 2016; Naseri & Taleghani, 2012; Tabatabaeichehr et al., 2019). For cancer patients, family members and spouses emerge as the most significant providers of social support (Salim et al., 2019). Given that the items within this factor underscore cancer patients’ perceptions of family support, it is essential for nurses to focus on emotional support, assess the quantity and quality of available family support resources, and address patients’ perceptions. By actively involving the family, healthcare professionals can enhance support provision and alleviate patients’ stress.
The second factor in the Persian version of the MSPSS pertains to the perception of support from friends. Elbert Hubbard eloquently describes a friend as someone who “knows everything about you and still loves you,” while Helen Keller emphasizes that “walking with a friend in the dark is better than walking alone in the light.” In the present study, 19% of the variance was explained by this factor. The results of a study, which examined the psychometric properties of the scale in urban adolescents, showed that adolescents receive more social support from friends, which is consistent with the present study (Canty-Mitchell & Zimet, 2000). Contrary to the above findings, another study that examined the psychometric properties of this scale in family caregivers of patients with schizophrenia showed that family caregivers of patients with schizophrenia receive less support from friends and other support networks outside the family (Wang et al., 2021). In justification of these findings, it can be stated that perceived support from friends can vary across different populations and groups (Procidano & Heller, 1983). For example, caring for patients with schizophrenia requires a lot of time and energy, so family caregivers have limited time to receive support from friends and other support networks outside the family (Canty-Mitchell, J., 2000), while social support from friends’ holds particular importance for cancer patients. Research indicates that a decline in friendships can impact patients’ overall quality of life and their physical and emotional well-being (Evans et al., 2015; Fehr & Harasymchuk, 2017). People who experience the support of close friends have a more positive outlook when facing problems and show more effective adaptation to illness (Procidano & Heller, 1983; Taylor et al., 1986).
In the original version of the MSPSS, social support from family, friends, and other significant individuals is categorized into emotional, informational, and instrumental domains. However, some studies emphasize distinguishing between perceived social supports from different networks. Findings from these studies indicate that perceived family support tends to be more stable and enduring, while friendships may fluctuate based on factors such as the severity of the disease, prior experiences with cancer patients, and individual circumstances and life desires (Procidano & Heller, 1983; van Eijk et al., 2022). Additionally, the definition of “other significant people”—those who impact an individual's self-concept and emotions and can provide support during crises like cancer—varies across cultures. These individuals may include spouses, parents, friends, or professional caregivers (Hatteberg, 2021; Zimet et al., 1988). Different studies have reported different factor structures using different methods. In the present study, items assessing perceived support from other important people were grouped under the family support factor. However, in a study by Chou (2000) and Wang et al. (2021), these items were merged with the factor related to supporting friends. In Wang's study, unlike the present study, the family subscale was retained as a factor, while the friends and significant others subscales were merged into a single “nonfamily” scale. In other studies (Teh et al., 2019; Tonsing et al., 2012), the significant others and friends scale were considered as a factor. Different characteristics of participants and sociocultural factors may explain these differences. Cultural norms are another reason for explaining these findings. In Asian cultures, people avoid sharing their personal issues with anyone other than their family members (Taylor et al., 2004). These discrepancies highlight the need for further research to clarify this concept, particularly within the cancer patient population.
Confirmatory factor analysis revealed a two-factor model for the MSPSS, which differs from the original three-factor theory (family, friends, and significant others) (Zimet et al., 1988) and also most of the previous studies that have been done with other samples and in different populations are different (Sharif et al., 2021; Wang et al., 2021). This discrepancy suggests disagreement regarding the underlying structure of the MSPSS. Factors such as sample size, diverse populations, and cultural variations may contribute to these differences. In the study, the scale exhibited acceptable reliability, as evidenced by a high Cronbach's alpha coefficient. Previous research has consistently supported the reliability of this scale, with Cronbach's alpha coefficients exceeding 0.7 (De Maria et al., 2018; Wang et al., 2017). Although measuring reliability through test–retest provides further evidence of measurement stability over time, it was not examined in the present study.
Strengths and Limitations
The study also demonstrates a comprehensive approach to assessing reliability, incorporating Cronbach's alpha, McDonald's omega, AIC, CR, and MaxR. This multifaceted evaluation ensures that the internal consistency of the scale is thoroughly examined. The use of contemporary statistical techniques, such as parallel analysis and the HTMT ratio, reflects the study's commitment to employing best practices in scale validation.
Clinically, the study adds practical value by validating a tool that can help healthcare providers assess perceived social support among Persian-speaking cancer patients, enabling targeted psychosocial interventions. Furthermore, the high response rate suggests strong participant engagement and reduces the risk of nonresponse bias, thereby enhancing the reliability of the study outcomes.
While the findings of the present study contribute to existing research, it is essential to acknowledge its limitations. First, our sample consisted exclusively of cancer patients from medical centers affiliated with a single university in Tehran. Consequently, the generalizability of our results to other patient populations may be limited. Second, we employed a self-report tool in our study, which inherently carries the risk of participants exhibiting social desirability bias.
Third, social support is a latent variable, and unfortunately, a gold standard criterion against which to evaluate the MSPSS was not available in Iran. Consequently, the validity of this criterion could not be thoroughly investigated in our study, emphasizing the need for further research in this area.
Nursing Implications
The study on the validity and reliability of the Persian version of the MSPSS in Iranian cancer patients has important implications for nursing practice. These include utilizing the MSPSS tool for patient assessments to tailor interventions, developing individualized care plans based on social support levels, promoting patient education on the importance of social support, collaborating with multidisciplinary teams to address patient needs, and engaging in ongoing evaluation to contribute to evidence-based practice.
Conclusion
The Persian version of the MSPSS demonstrates acceptable psychometric properties. Our investigation covered various aspects of validity and reliability, affirming the suitability of this scale. The Persian version MSPSS can serve as a valuable resource in clinical and research contexts, enabling assessment of individuals’ perceived support levels and informing targeted interventions to enhance support networks.
Footnotes
Acknowledgment
The authors would like to express their sincere gratitude to all the cancer patients who participated in this study and generously shared their experiences. The authors also extend our appreciation to the nursing staff and healthcare professionals at Tehran oncology clinics for their support and assistance in facilitating the data collection process. This research would not have been possible without the collaboration and dedication of the entire team.
Ethical Approval
The Ethics Committee of Mazandaran University of Medical Sciences (Sari, Iran) gave its approval to this study (Ethics code: IR.MAZUMS.IMAMHOSPITAL.REC.1403.016). The participants were given a thorough explanation of the study's goals and methods, as well as assurances that their participation was entirely voluntary. An informed consent was signed by each participant for the participation in the research. Then, the researcher would give the scale to the patient to complete by themselves.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.