
Abstract
Introduction
Caring is an integral part of the nursing profession, often viewed as an abstract and immeasurable behavior. However, caring behaviors can be measured and evaluated, ultimately improving care outcomes and practices. To accomplish this, a valid and reliable tool for measuring caring behaviors is essential. One such tool is the Caring Behaviors Assessment Tool Nursing Version-Short Form (CBAN-SF), which has not yet been translated and psychometrically evaluated in Iran.
Objective
This study aimed to evaluate the psychometric properties of the Persian version of the CBAN-SF.
Methods
A methodological study was conducted at two hospitals affiliated with Shahroud University of Medical Sciences using a cross-sectional approach. The CBAN-SF was translated into Persian following the forward–backward procedure outlined by the World Health Organization (WHO) guidelines. The validity (including face, content, and construct) and reliability (encompassing internal consistency and stability) of the Persian version of the CBAN-SF were assessed. In order to assess construct validity, 400 eligible clinical nurses were included in the study. The first 200 samples were used to conduct exploratory factor analysis (EFA), while the second 200 samples were used to conduct confirmatory factor analysis (CFA). Reliability was gauged through Cronbach's alpha coefficient, MacDonald's omega coefficient for internal consistency, and intraclass correlation coefficient for stability.
Results
The assessment of content validity and EFA resulted in the removal of one item and six others, leaving a final set of 20 items. These were divided into four factors: “dignified care,” “expression of feelings,” “self-sufficiency and self-belief,” and “patient-centered care,” which together explained 56.82% of the total variance. The CFA demonstrated that the model closely matched the observed data. Furthermore, each subscale exhibited strong internal consistency and stability.
Conclusion
It can be concluded that the Persian version of the CBAN-SF shows adequate validity and reliability in evaluating the caring behavior of clinical nurses.
Introduction
Caring behaviors are both verbal and nonverbal interventions made by nurses in the care process, as specifically defined by Watson in the humanistic care theory (Watson, 1999). These behaviors include understanding, smiling, touching, effective listening, empathy, acceptance of feelings, respect for the patient's privacy, and recognition of their individuality (Watson, 1997). The humanistic care theory emphasizes the importance of encouraging patients to be self-reliant, helping them understand their feelings, providing adequate information about their illness/health, and being willing and ready to provide nursing care as additional caring behaviors (Watson, 1997, 1999).
It can be said that caring behaviors increase nurses’ sense of self-sufficiency, self-confidence, emotional well-being, and professional satisfaction, leading to an improvement in the quality of nursing care provided to patients (Young et al., 2019). On the other hand, assessing nurses’ perceptions of caring behaviors provides the opportunity to monitor the quality of care, implement necessary regulations, and improve the care process (Papastavrou et al., 2011). Therefore, assessing this concept from the perspective of nurses and identifying its related factors in clinical settings is of particular importance. Achieving this goal requires the existence of a valid and reliable tool to measure caring behaviors from the perspective of nurses.
Review of Literature
In the scientific literature, caring behaviors are often measured through tools such as the “Caring Behavior Inventory (CBI)” (Wolf et al., 1994), the “24-item Caring Behavior Inventory (CBI-24)” (Wu et al., 2006), the “Caring Behavior Measurement (CBM)” (Lee-Hsieh et al., 2005b), and the “Caring Behavior Assessment (CBA)” (Cronin & Harrison, 1988). The CBI was originally designed with 75 items in 1994 by Wolf et al. (1994). Then, in 2006, Wu et al. developed the CBI-24, which assesses four subfactors: “assurance of human presence,” “knowledge and skill,” “respectful deference to others,” and “positive connectedness” (Wu et al., 2006). Although this inventory is widely used to assess nurses’ and patients’ perceptions of caring behaviors, the subfactors “assurance of human presence” and “knowledge and skills” emphasize more on the technical aspect of care (Akgün et al., 2019). Similarly, the CBM was first developed by Lee-Hsieh in 2005 with 48 items (Lee-Hsieh et al., 2005a). It was then revised, resulting in a reduction to 28 items. These items measure two subfactors: “sincerity, empathy, and respect” and “professional caring behaviors,” with only the second subfactor focusing on caring behaviors (Lee-Hsieh et al., 2005b). In addition, it had a limited application for evaluating the perceptions of nurses and patients regarding caring behaviors (Akgün et al., 2019). The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) recommend that the structure of a tool should be derived from a clear conceptual framework, theory, or model (Terwee et al., 2018). However, the CBI and CBM tools are not based on any nursing theory (Lee-Hsieh et al., 2005b; Wu et al., 2006).
The only CBA is based on Watson's humanistic nursing theory, which was developed by Cronin and Harrison in 1988 with 63 items and 7 subfactors (Cronin & Harrison, 1988). Subsequently, Akgün et al. created the Caring Behaviors Assessment Tool Patient Version-Short Form (CBAP-SF) in 2019, consisting of 27 items and 7 subfactors (Akgün et al., 2019). Following this, Akgün et al. introduced the Caring Behaviors Assessment Tool Nursing Version-Short Form (CBAN-SF) in 2020, which also includes 27 items and 7 subfactors (Akgün et al., 2020). This tool evaluates the concept of caring behaviors from the perspective of nurses as healthcare providers (HCPs), based on a nursing theory. It contains fewer items than the other two tools, and its original version has shown good validity and reliability (Akgün et al., 2020).
In Iran, there are several tools available to assess nurses’ caring behaviors. Two such tools are the Determinants of Nurses’ Caring Behaviors (DNCB) (Salimi & Azimpour, 2013) and the Persian version of the 23-item Caring Dimension Inventory (PCDI-23) (Salimi et al., 2014). The DNCB, with 35 items and six dimensions, was developed and validated by Salimi and Azimpour (2013). Additionally, Salimi et al. (2014) assessed the psychometric properties of the PCDI-23, which measures four factors. Despite the favorable psychometric properties and appropriate number of items, over a decade has passed since the design and psychometric evaluation of these tools. This highlights the need for a newer tool that is both valid and reliable.
The Persian versions of the Caring Behavior Inventory, which include the 24-item (CBI-24) and 16-item (CBI-16), are tools that are occasionally used to evaluate the concept of caring behavior in Iranian nurses (Ghafouri et al., 2021; Khaletabad et al., 2023). The 16-item version of this inventory was translated and validated by Ghafouri et al. (2021), assessing two factors, “Communicating respectfully” and “Professional knowledge and skill,” solely from the perspective of patients (Ghafouri et al., 2021). Azimi Khaletabad et al. (2023) also studied the cultural adaptation and psychometric testing of the 24-item version of this inventory in both Iranian patients and Iranian nurses, measuring four factors: “respectfulness,” “connectedness,” “knowledge and skill,” and “assurance.” Despite being up-to-date and having acceptable psychometric properties, the two aforementioned tools are not based on any nursing theory (Akgün et al., 2019). Therefore, the existence of a valid and reliable tool that addresses the limitations of available tools in Iranian society seems essential. As mentioned earlier, the CBAN-SF not only lacks the shortcomings of the aforementioned tools, but its original version also demonstrates excellent psychometric properties. Consequently, there is a need for a Persian version that accurately measures caring behaviors from the perspective of Iranian clinical nurses. This study was conducted with the aim of culturally adapting and evaluating the psychometrics of the CBAN-SF in Iranian clinical nurses.
Methods
Design and Setting
This methodological study, utilizing a cross-sectional approach, was conducted between May and September 2023 among clinical nurses at two hospitals affiliated with Shahroud University of Medical Sciences, including Imam Hossein (PBUH) and Bahar.
The Caring Behaviors Assessment Tool Nursing Version-Short Form
The CBAN-SF consists of 27 items scored on a five-point Likert scale ranging from “Least important” (1 point) to “Most important” (5 points). The CBAN-SF is a tool used to evaluate nurses’ caring behaviors, with seven subscales measuring different aspects of caring: (a) Humanism/faith hope/sensitivity (items 1–4), (b) Helping/trust (items 5–8), (c) expression of positive/negative feelings (items 9–11), (d) Teaching/learning (items 12–15), (e) Supportive/protective/corrective environment (items 16–21), (f) Human needs assistance (items 22–24), and (g) Existential/phenomenological/spiritual forces (items 25–27). Scores on the CBAN-SF range from 27 to 135, with a higher score indicating a more positive perception of nurses’ caring behaviors (Akgün et al., 2020).
Translation and Cross-Cultural Adaptation
According to our e-mail correspondence and with explicit permission from the original designer, the tool was translated following the established translation process of the World Health Organization (WHO) (Organization, 2009), which involves the forward–backward procedure. Initially, two separate translators translated the tool from English to Persian. A composite translation was then created by selecting the best translation. Subsequently, the revised version was translated back into English by two skilled individuals who cross-checked it with the original English version provided by the study team. The final version was submitted to Professor İlkay Boz for approval, which was granted. Finally, all recommendations were incorporated into the ultimate version of the tool (Khaletabad et al., 2023; Tehranineshat et al., 2023).
Face Validity
In the current stage of the study, two components were evaluated—qualitative and quantitative face validity. The first step involved conducting a qualitative face validity assessment through face-to-face interviews with 10 clinical nurses. These interviews aimed to gather nurses’ perspectives on the appropriateness, difficulty, relevance, and ambiguity of tool items. Moreover, ten clinical nurses were asked to rate the significance of each item on a 5-point Likert scale ranging from “very important” (scored as 5) to “not important” (scored as 1) to determine quantitative face validity. The impact score of the items was computed using the following formula:

The concept of frequency, expressed as a percentage, indicates the proportion of individuals who rate an item as a 4 or 5. The purpose of importance is to determine the average importance score using the Likert scale. The grading procedure involves calculating the average of three factors and considering a frequency of 50%. If the impact score exceeds 1.5, the item will be regarded as appropriate for further analysis and retained. Items with an impact score below 1.5 will be revised and modified (Polit, 2015; Rust & Golombok, 2014).
Content Validity
Similar to the previous section, a content validity assessment was conducted using qualitative and quantitative methods. Twelve experts, including 10 nursing experts and two tool development experts, were interviewed to evaluate the content validity qualitatively. The experts were asked to review a qualitative questionnaire and provide feedback on various aspects, such as grammar, word usage, item placement, and scoring. The questionnaire items were adjusted based on their feedback.
The subsequent phase involved quantitatively assessing content validity by estimating the items’ Content Validity Ratio (CVR) and Content Validity Index (CVI). The experts mentioned above were asked to evaluate the significance of each item based on the criteria (1, “not necessary”; 2, “functional but not necessary”; 3, “necessary”) (Ayre & Scally, 2014). The CVR was calculated using the following formula:

The opinions of an expert panel were utilized to evaluate the tool's Item-Content Validity Index (I-CVI). The I-CVI assesses the relevance of the items on a specific tool to the overall concept under study. The experts individually reviewed each item and provided scores ranging from “not relevant” = 1, “somewhat relevant” = 2, “relevant but in need of review” = 3, and “completely relevant” = 4. The I-CVI of each item was calculated by dividing the number of experts who rated the item with either 3 or 4 points by the total number of experts. Items with an I-CVI score above 0.79 were deemed adequate and acceptable. Items with an I-CVI score between 0.70 and 0.79 were considered questionable and in need of revision. Finally, items with an I-CVI score below 0.70 were deemed unacceptable (Khachian et al., 2023). This approach was followed to ensure the accuracy and reliability of the data obtained. The Scale-Content Validity Index/Average (S-CVI/Ave) was estimated by calculating the average values of I-CVI. An S-CVI/Ave greater than 0.9 is considered acceptable (Polit & Beck, 2010).
The modified Kappa statistic (K*) was calculated for each item to account for the chance agreement among the expert panel using the following formula:

Participants
MacCallum et al. (1999) suggested that the minimum sample size for psychometric studies is 200. Therefore, two separate samples of 200 eligible clinical nurses each, totaling 400 participants, were selected to conduct exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). Four hundred clinical nurses from two hospitals affiliated with Shahroud University of Medical Sciences were chosen through convenience sampling. Participants must hold a Bachelor of Science in Nursing (BSN) or a higher degree, as well as have a minimum of one year of clinical work experience (Tehranineshat et al., 2023).
Construct Validity
The construct validity was assessed using maximum likelihood exploratory factor analysis (MLEFA) with Promax rotation. This analysis was conducted on the first 200 samples. The sampling adequacy for the data was determined using Kaiser–Meyer–Olkin (KMO) and Bartlett's test of sphericity. If Bartlett's test of sphericity is significant (P < .001), KMO values between 0.7 and 0.8 were considered acceptable, while values between 0.8 and 0.9 were deemed excellent (Hejazi et al., 2022; Sharif Nia et al., 2021a).
The item's factor loading was calculated to determine its presence in a latent factor. If the factor loading was approximately 0.33 or higher, the item was included in the factor. The formula used to estimate the critical value (CV) was as follows:

CFA was utilized to validate the goodness-of-fit and ensure that the proposed model closely resembled the actual model within the second 200 samples. In essence, CFA aims to validate the model initially developed through EFA. Therefore, CFA assesses the structure of the construct derived from EFA during this stage.
The model fit was assessed using various fit indices, including the Chi-squared (χ2) test, χ2/degree of freedom (CMIN/df) < 3, root mean square error of approximation (RMSEA) < 0.08, parsimony comparative fit index (PCFI) > 0.5, parsimony normed fit index (PNFI) > 0.5, comparative fit index (CFI) > 0.9, incremental fit index (IFI) > 0.9, Tucker–Lewis index (TLI) > 0.90 (Meyers et al., 2016; Pahlevan Sharif & Sharif Nia, 2020).
Convergent and Discriminant Validity
Convergent and discriminant validity were investigated using the proposed method of Fornell and Larcker (1981) by calculating the average variance extracted (AVE), maximum shared squared variance (MSV), and composite reliability (CR). An AVE value greater than 0.5, a CR value greater than AVE, or a CR value greater than 0.7 indicates appropriate convergent validity. Additionally, if the AVE value exceeds MSV, the tool's discriminant validity is confirmed (Fornell & Larcker, 1981; Pahlevan Sharif & Sharif Nia, 2020).
Reliability
Cronbach's alpha and McDonald's omega coefficients were calculated for each factor to assess internal consistency. A minimum value of .7 for both Cronbach's alpha and McDonald's omega coefficients demonstrates high internal consistency. Furthermore, the construct reliability of each factor was evaluated with a CR and Maximal Reliability (MaxR) value exceeding 0.7, indicating good construct reliability (Khachian et al., 2023; Pahlevan Sharif & Sharif Nia, 2020).
The stability was assessed using an intraclass correlation coefficient (ICC). To achieve this goal, the tool was completed twice by 30 clinical nurses at a 2-week interval. The minimum acceptable value of ICC was considered 0.75 (Pahlevan Sharif & Sharif Nia, 2020).
Normality, Outliers, and Missing Data
Distribution charts and Mahalanobis distance (P < .001) were utilized to evaluate univariate and multivariate outliers. Additionally, an examination of univariate and multivariate normality distribution was conducted, considering skewness (values within ±3), kurtosis (values within ±7), and the Mardia coefficient <8. The data from this study did not show a significant deviation from the normal distribution. A listwise missing procedure was implemented for estimating CFA. Listwise deletion was chosen as the preferred method over imputation because non-response was associated with incomplete and non-response questionnaires (Sharif Nia et al., 2021a). All statistical analysis was performed using Statistical Package for Social Science (SPSS) and Analysis of Moment Structures (AMOS) version 26.
Ethical Considerations
First, necessary permits were obtained from the Vice Chancellor for Research and Technology and the Research Ethics Council of Shahroud University of Medical Sciences (Ethics Code: IR.SHMU.REC.1402.010). Next, essential coordination was established with the officials of Imam Hossein (PBUH) and Bahar hospitals. Finally, all participating nurses were informed about the study's objectives, and their verbal and written informed consent was obtained.
Results
Demographic Characteristics
Four hundred clinical nurses from two hospitals affiliated with Shahroud University of Medical Sciences, Imam Hossein (PBUH) and Bahar participated in this study. Among them, 301 individuals (75.3%) were women, 256 individuals (66.2%) were married. The characteristics of the study participants are shown in Table 1.
The Characteristics of Study Participants (N = 400).

N = Frequency; % = Percent; PBUH = Peace Be Upon Him; BSN = Bachelor of Science in Nursing; MSN = Master of Science in Nursing; SD = Standard Deviation.
Face Validity
The qualitative face validity demonstrates that all tool items are adequate, clear, and essential. Additionally, quantitative face validity indicates that all impact scores were above 1.5.
Content Validity
Based on suggestions from 12 experts, some items were revised for qualitative content validity. Moreover, CVR and I-CVI were calculated for each item regarding quantitative content validity. With a cut-off point of 0.56, only item number 3 (CVR = 0.33) was deleted. Furthermore, the I-CVI values ranged from 0.83 to 1. The S-CVI was determined to be 0.97. Additionally, the K* for all items was satisfactory, exceeding the threshold of 0.7.
Construct Validity
In MLEFA, the KMO value was 0.927, and Bartlett's test of sphericity yielded a value of 3190.483 (P < .001). The model extracted four factors with eigenvalues greater than one from the Persian version of the CBAN-SF. According to Table 2, these four factors collectively accounted for 56.82% of the total variance. Furthermore, items 13, 14, 16, 17, 26, and 27 were removed from the principal tool because their factor loadings were less than 0.3. Consequently, the total number of items in the analysis is now 20.
Maximum Likelihood Exploratory Factor Analysis of the Persian Version of the CBAN-SF (N = 200).
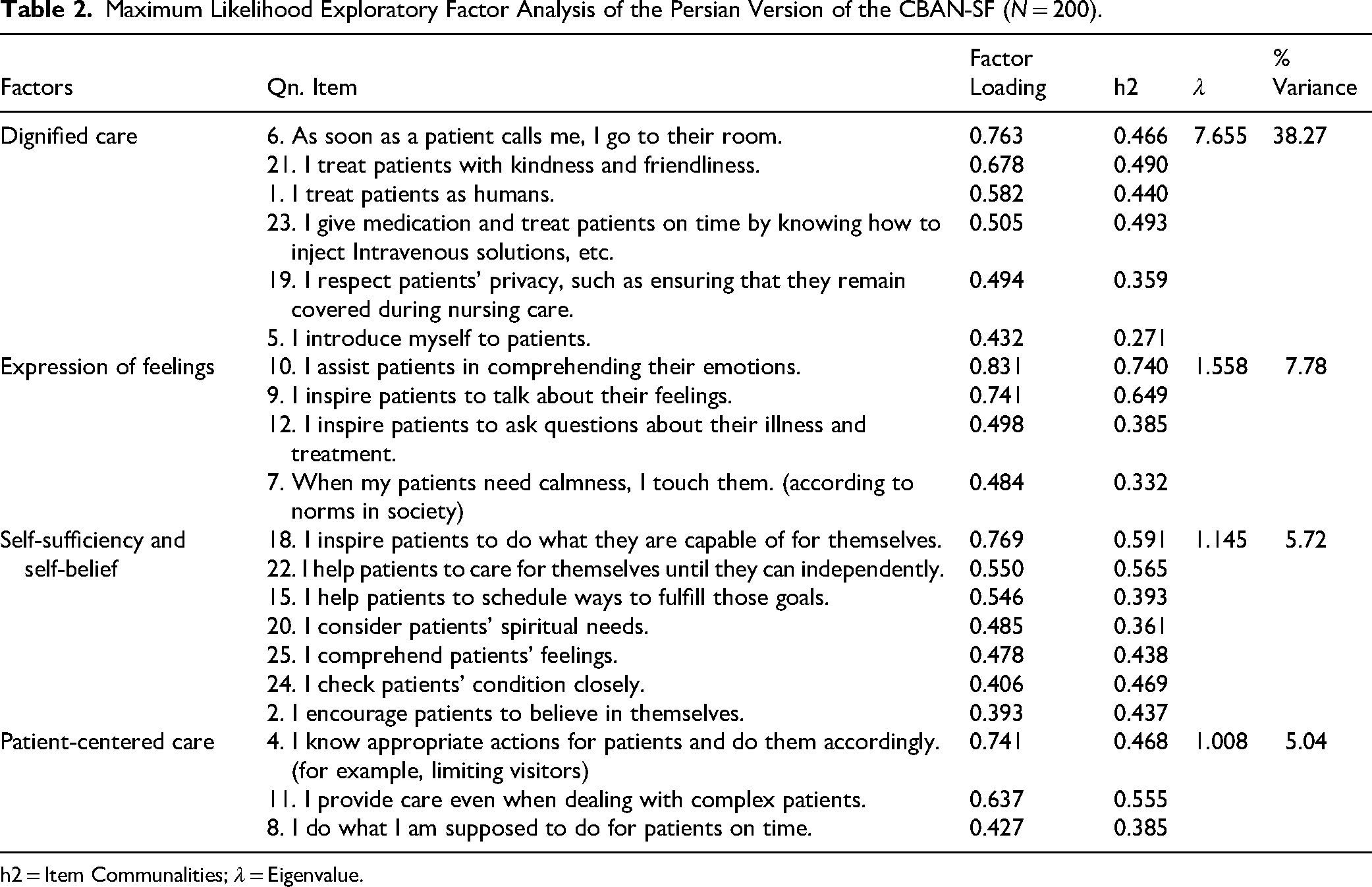
h2 = Item Communalities; λ = Eigenvalue.
The first-order CFA indicated that the four-factor model of the Persian version of the CBAN-SF fit the data well, as shown by an acceptable goodness of fit (Table 3). As shown in Figure 1, the covariances among the factors were above 0.50, suggesting a latent variable underlying them. Consequently, another evaluation of the factors and their correlation was carried out. A second-order CFA was then performed to validate a latent variable called “nursing caring behaviors” (Table 3). Figure 2 displays the second-order structural model and the CFA results.

The Results of the Confirmatory Factor Analysis for the First-order Model of the Persian Version of the CBAN-SF (N = 200).

The Results of the Confirmatory Factor Analysis for the Second-order Model of the Persian Version of the CBAN-SF (N = 200).
Fit Indices of the First- and Second-Order Confirmatory Factor Analysis of the Persian Version of the CBAN-SF (N = 200).

df = degrees of freedom; P = P-value; RMSEA = Root Mean Square Error of Approximation; PCFI = Parsimony Normed Fit Index; PNFI = Parsimony Normed Fit Index; CFI = Comparative Fit Index; IFI = Incremental Fit Index; TLI = Tucker–Lewis Index.
Convergent and Discriminant Validity
As indicated in Table 4, only the AVE for Factor 2 was significantly higher than 0.5. However, Factor 1 (0.404), Factor 3 (0.444), and Factor 4 (0.454) were slightly below 0.5. AVE is a stringent measure for assessing convergent validity, but in psychological studies, a CR of over 0.7 can also be used to evaluate convergent validity (Sharif Nia et al., 2021b; Sharif et al., 2023). Hence, convergent validity was achieved for all four factors following the CR and AVE. In addition, MSV for all factors was more significant than AVE, indicating that the extracted factors are related and that a second-order CFA is necessary.
Convergent and Discriminant Validity and Reliability of the Persian Version of the CBAN-SF.

CR = Composite Reliability; AVE = Average Variance Extracted; MSV = Maximum Shared Squared Variance; MaxR (H) = Maximal Reliability; α = Cronbach's alpha coefficient; Ω = McDonald's omega coefficient; ICC = Intraclass Correlation Coefficient.
Reliability
Based on the results, the four-factor model of the Persian version of the CBAN-SF has acceptable internal consistency and construct reliability. Table 4 demonstrates Cronbach's alpha and McDonald's omega coefficients for all factors exceeding .7, indicating good internal consistency. Similarly, all factors’ CR and MaxR values exceeding 0.7 showed satisfactory construct reliability. The ICC for all factors extracted from the Persian version of the CBAN-SF was also deemed suitable, with an ICC of all items calculated at 0.807.
Discussion
The findings of this study confirm the reliability and validity of the Persian version of the CBAN-SF. Through EFA, the tool contained 20 items and four factors: “dignified care,” “expression of feelings,” “self-sufficiency and self-belief,” and “patient-centered care”. These factors account for 56.82% of the total extracted variance.
The CBAN-SF tool was developed to address the shortcomings of previous nursing care behavior assessment tools. The original version has 27 items and a seven-factor structure (Akgün et al., 2020).
However, Cronin and Harrison (1988) used a 63-item version of the CBA, which differs from the one used in the current study. The 63-item version includes seven factors: (a) humanism/faith, hope/sensitivity, (b) helping/trust, (c) expression of positive/negative feelings, (d) teaching/learning, (e) supportive/protective/corrective environment, (f) human needs assistance, and (g) existential/phenomenological/spiritual forces (Cronin & Harrison, 1988).
In contrast, the Persian version of the CBAN-SF identified four factors through EFA. The first factor extracted was “dignified care,” comprising six items that highlighted a focus on human rights. In this respect, Cairns et al. (2013) conducted a survey to evaluate the importance and meaning of “dignified care” in health and social care. A total of 192 specialists described “dignified care” as encompassing actions such as showing respect, delivering humane treatment, involving patients in decision-making, and safeguarding their privacy (Cairns et al., 2013). “Dignified care” promotes independence, garners respect, preserves individuals’ identities, encourages participation, utilizes effective communication, and is person-centered and holistic (Ariño-Blasco et al., 2005). This factor explained the highest percentage of nursing care behaviors, indicating its significance. In the psychometric analysis of the 47-item version of the CBM, the factor of “sincerity, empathy, and respect” was identified (Lee-Hsieh et al., 2005b). Similarly, in the psychometric analysis of the CBI-42, the factor of “assurance of human presence” was also extracted (Wu et al., 2006). Additionally, in the psychometric analysis of the Persian version of the CBI-16, the factor of “communicating respectfully” was identified (Ghafouri et al., 2021). All of these factors are equivalent to the “dignified care” factor in the current study.
In the Persian version of the CBAN-SF, the second extracted factor is related to the “expression of feelings.” This factor consists of four items emphasizing the mutual perception of emotions and the significance of achieving calmness. It is widely believed that expressing feelings benefits individuals, leading to improved emotions, actions, and overall health. It is essential to mention that in the original version of the CBAN-SF, which contained 27 items, the factor of “expression of positive/negative feelings” was equivalent to the feelings factor in the present study (Akgün et al., 2020).
The third factor extracted in the Persian version of the CBAN-SF was “self-efficacy and self-belief,” consisting of seven items. Self-efficacy is a specific behavioral construct that plays a significant role in behavior modification. It predicts an individual's perception of their ability to overcome obstacles in a particular task and their willingness to make future efforts to tackle various behavioral challenges associated with that task. Self-belief is a crucial factor that can influence individual behavior. Perceived severity, perceived threat, and perceived benefits impact individuals and motivate them to engage in positive behavior change (Ferrer & Klein, 2015; Voigt et al., 2015). In the original version of the CBAN-SF with 27 items, the “supportive/protective/corrective environment factor” and “existential/phenomenological/spiritual forces” were found to equal the “self-efficacy and self-belief” factor in the existing study (Akgün et al., 2020).
The Persian version of the CBAN-SF identified “patient-centered care” as the fourth factor, consisting of three items. “Patient-centered care” is a crucial concept in nursing derived from Florence Nightingale's work. She emphasized the importance of focusing on patients and providing respectful and responsive care to their needs, preferences, and values (Lauver et al., 2002). This component is essential for achieving high-quality care (Esmaeili et al., 2022). In the original version of the CBAN-SF with 27 items, “humanism/faith hope/sensitivity” and “helping/trust” were equivalent to the “patient-centered care” factor in the current study (Akgün et al., 2020).
The CFA was used in this study to assess the compatibility of the Persian version of the CBAN-SF model. The high correlation among the first-order structures suggests that the latent variables do not act as entirely independent variables. Instead, their correlation indicates a more general construct at the second concept level. According to the CFA second-order results, the domains’ correlation with the total scale and their low correlation with each other demonstrate that they are not equivalent. The original version of the CBAN-SF was employed for CFA, and the model was deemed acceptable based on fit indices (Akgün et al., 2020). However, CFA was not conducted for the nursing version of CBA, which consists of 63 items in English and Arabic (O’Connell & Landers, 2008; Youssef et al., 2013).
The Persian version of the CBAN-SF demonstrated strong and excellent internal consistency, as indicated by both Cronbach's alpha and McDonald's omega results. Typically, studies only use Cronbach's alpha to assess the stability of a tool. In a study by Akgun et al. (2020), Cronbach's alpha coefficients for the total scale in CBAN-SF were .974, with subscales ranging from .793 to .904 (Akgün et al., 2020). Similarly, the Arabic version of the CBA, with 63 items, showed a Cronbach's alpha of .91 for the total scale and between .70 and .93 for its subscales (Youssef et al., 2013). Conversely, the English version of the CBA, also with 63 items, displayed a Cronbach's alpha of .75 to .90 (O’Connell & Landers, 2008). Therefore, the internal consistency reliability of these subfactors varied across different cultures.
Akgun et al. (2019) conducted a study to evaluate the reliability and consistency of a Turkish version of a tool known as CBA-Turkish Version (TR). The study demonstrated that the total Cronbach's alpha coefficient of the CBA-TR was .978. Furthermore, the subdimensions of the tool ranged from .84 to 0.97 (Akgün et al., 2019). In addition, Akgun et al. (2021) introduced a new tool called the CBAP-SF. This version consists of 27 items, significantly fewer than the previous version. The research indicated that the total Cronbach's alpha coefficient of the CBAP-SF was .96, with subdimensions ranging from .77 to .94. The earlier version had a large number of items, making it difficult to utilize (Mehtap Akgün et al., 2021).
This study utilized CFA to assess the construct reliability of the Persian version of the CBAN-SF. The stability of the instructions used in the current study is adequate, as all factors were above 0.7. One benefit of measuring CR is that the number of scale items or sample size does not affect the criterion (Vinzi et al., 2010). Moreover, the CBAN-SF demonstrates strong stability with satisfactory ICC, further highlighting the advantages of this tool. Unlike in most similar studies, CR and ICC were not assessed, underscoring the strength of the present study.
The Persian version of the CBAN-SF excluded seven items: 3, 13, 14, 16, 17, 26, and 27, which reduced the total to 20. As a result, its scoring now ranges from 20 to 100. A higher score indicates a more positive perception of nursing care behaviors. Additionally, this tool comprises four factors: “dignified care” (6 items, scores ranging from 6-30), “expression of feelings” (4 items, scores ranging from 4-20), “self-sufficiency and self-belief” (7 items, scores ranging from 7-35), and “patient-centered care” (3 items, scores ranging from 3-15).
Strengths and Limitations
Only clinical nurses working in two hospitals affiliated with Shahroud University of Medical Sciences participated in the data collection. This may limit the generalizability of the results to clinical nurses employed in medical centers affiliated with other universities of medical sciences in the country, as well as non-university centers like private medical centers. Furthermore, the Persian version of this tool has undergone psychometric evaluation within the cultural context of Iran. However, Persian is also spoken in various other countries with unique cultural contexts. Therefore, it is recommended that the mentioned tool be adapted to suit the cultural contexts of Persian speakers in these nations as well.
Given these limitations, the present study has provided a more user-friendly yet valid and reliable tool for assessing the caring behaviors of Iranian clinical nurses. This was accomplished by utilizing a novel and robust methodology that addressed the limitations and shortcomings of previous studies in this field to the fullest extent possible.
Implications for Practice
The Persian version of the CBAN-SF, with its desirable psychometric properties, can serve as a practical instrument for measuring this concept among Iranian clinical nurses. Having a valid and reliable tool to evaluate nursing care behaviors in clinical settings could facilitate the development of effective strategies and approaches to enhance this concept. Ultimately, this would result in the delivery of safe and high-quality nursing care, leading to positive outcomes for patients.
Conclusion
The current study uncovered that the Persian version of the CBAN-SF encompasses 20 items organized into four factors, accounting for approximately 57% of the total variance. This scale demonstrates favorable psychometric properties for evaluating caring behaviors.
Supplemental Material
sj-pdf-1-son-10.1177_23779608251346651 - Supplemental material for Cross-Cultural Adaptation and Psychometric Evaluation of the Persian Version of the Caring Behaviors Assessment Tool Nursing Version-Short Form
Supplemental material, sj-pdf-1-son-10.1177_23779608251346651 for Cross-Cultural Adaptation and Psychometric Evaluation of the Persian Version of the Caring Behaviors Assessment Tool Nursing Version-Short Form by Faezeh Yousefi, BSc, Ali Asghar Parhizkari, BSc, Hamid Sharif-Nia, PhD, Saeed Ghasempour, BScN and Ali Abbasi, PhD in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251346651 - Supplemental material for Cross-Cultural Adaptation and Psychometric Evaluation of the Persian Version of the Caring Behaviors Assessment Tool Nursing Version-Short Form
Supplemental material, sj-docx-2-son-10.1177_23779608251346651 for Cross-Cultural Adaptation and Psychometric Evaluation of the Persian Version of the Caring Behaviors Assessment Tool Nursing Version-Short Form by Faezeh Yousefi, BSc, Ali Asghar Parhizkari, BSc, Hamid Sharif-Nia, PhD, Saeed Ghasempour, BScN and Ali Abbasi, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
This study is a result of a project approved under the number 14010077 at Shahroud University of Medical Sciences. The researchers would like to acknowledge the support of the Vice Chancellor for Research and Technology at Shahroud University of Medical Sciences. Additionally, the authors want to express their heartfelt gratitude to the Vice Chancellors of Imam Hossein (PBUH) and Bahar hospitals, as well as all the participating nurses and other contributors to the execution of this study.
Ethical Considerations
This study was approved under the Code of Ethics IR.SHMU.REC.1402.010 at the Ethics Council for Biomedical Research at Shahroud University of Medical Sciences.
Consent to Participate
Before participating in the study, each participant was informed about the study protocol and provided verbal and written informed consent.
Author Contributions
FY and AAP did conceptualization, data curation, investigation, writing—original draft.
HS-N did formal analysis, methodology, writing—original draft, writing—review and editing.
SG did data curation, methodology, writing—original draft, writing—review and editing.
AA did conceptualization, investigation, methodology, supervision, writing—original draft, writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.