
Abstract
Introduction
The diaphragm is considered the main inspiratory muscle, and as such, its assessment is crucial in patients with respiratory pathology. It is known that the contractile capacity of a muscle is determined by strength, length, and the duration of contraction. Although transdiaphragmatic pressure is the gold standard test for its study, ultrasound has been confirmed as a useful tool in clinical practice. Thanks to it, both the strength (diaphragmatic thickness) and the length of movement (diaphragmatic excursion) can be evaluated. This study aims to investigate the relationship between the inspiratory time and the diaphragmatic contraction.
Design
Cross-sectional controlled study.
Methodology
Eighty healthy subjects, yoga practitioners, with no previous respiratory pathology participated in this study. They were asked to take three different types of deep breaths: diaphragmatic with nasal inspiration, pursed-lip inspiration, and ujjayi (nasal inspiration with slight contraction of the glottis). The variables of thickness, excursion, and inspiratory contraction time were taken for each of them by ultrasound.
Results
Diaphragmatic contraction time is the only variable that shows a significant correlation with the other two. Thus, the correlation between inspiratory time and diaphragmatic thickness is significant (p < .001) for the three breaths: diaphragmatic (0.60), ujjayi (0.67), and pursed lips (0.39) and the correlation between inspiratory time and diaphragmatic excursion is significant for diaphragmatic breaths (−0.24, p = .035) and ujjayi (0.27, p = .017), but not in pursed lips (−0.01, p = .90).
Conclusion
The inspiratory contraction time and the diaphragmatic excursion are two essential variables in the dynamic functional evaluation of the diaphragm, compared to the diaphragmatic thickness measurement that only reports its strength.
Key Points
– The inspiratory contraction time and the diaphragmatic excursion are two essential variables in the dynamic functional evaluation of the diaphragm.
– Diaphragmatic thickness is a static value that only reports its strength.
Introduction
The diaphragm, recognized as the key muscle for inhalation, plays a crucial role in evaluating respiratory function. In conjunction with tests like spirometry, diaphragmatic ultrasound has become an indispensable tool in clinical practice, aiding both in exploration and diagnosis of respiratory conditions (Diaz Sánchez et al., 2019). It offers advantages over other invasive techniques such as measurement of transdiaphragmatic pressure (Fayssoil et al., 2018): it is easier to perform at the bedside, painless, fast, noninvasive and free of ionizing radiation (Gil-Rodríguez et al., 2022).
Review of Literature
When assessing the contractile capacity of a muscle, three key parameters must be considered: strength, range of motion, and contraction duration. Ultrasound, using its two imaging modes, allows for real-time evaluation. In B-mode, it provides structural insights, such as muscle thickness at rest, which correlates with body mass and weight, and after inspiration, which reflects muscle strength (Fogarty et al., 2018). M-mode, on the other hand, assesses the dynamic movement of connective tissue within the muscle over time (Ortega-Santamaría et al., 2023). This movement, referred to as diaphragmatic excursion, represents the distance the diaphragm travels during contraction and descent during inspiration (Boussuges et al., 2020). It is correlated with the MIP and MEP (Qaiser et al., 2020; respiratory mouth pressure parameters) and the volume of air mobilized, as supported by spirometry.
Ranges have been established to define normal diaphragmatic function using ultrasound evaluation. Regarding its resting thickness measured at the end of a nonforced expiration, normal values are considered to be between 2 and 3 mm. A resting thickness of less than 2 mm suggests atrophy (Acosta et al., 2018; Inci et al., 2024; Yao et al., 2024). Diaphragmatic excursion is considered functional when it ranges from 1 to 2.5 cm during tidal volume (Boussuges, Finance, et al., 2021) and from 4 to 11 cm during maximal inspirations, depending on the physical characteristics of the individual (Testa et al., 2011). These values vary according to the evaluation position (supine or seated; Boussuges, Rives, et al., 2021).
But what about the variable of contraction duration? Although a comprehensive muscle assessment should also include contraction time, this aspect is relatively underexplored in diaphragmatic ultrasound. It is a simple measure, as it only requires measuring the duration of the inspiratory phase in M-mode, from the start of inspiration until it reaches its peak (Richard, 2017). This metric is commonly employed in fields such as pelvic floor studies(Matsunaga et al., 2022) where muscular fatigue correlates with the incapacity to sustain a contraction over an extended period (Enoka & Duchateau, 2008). A muscle with less strength tires more quickly, struggling to maintain activity over prolonged periods and potentially failing to perform its intended function, which, in the case of the diaphragm, is to ensure inspiration and the entry of air into the lungs.
Under normal conditions, an adult is considered to breathe about 12 times per minute (Webster & Karan, 2020), a figure that drops to four or 10 for deep and slow breaths (Russo et al., 2017). This variability in timing is possible due to voluntary breath control, which allows for the modulation of both the intensity and duration of breathing (Nair et al., 2017), and, above all the composition of the diaphragm that allows it to contract at different speeds (Brown et al., 2022).
Diaphragm is made up of muscle fibers: types I, IIa, IIx, and IIb. Each of these is activated depending on the required contraction speed. For example, during a slower basal breath, the types I and IIa fibers are mainly activated, while for greater efforts such as coughing or sneezing in which explosive force is needed (more force in less time), type IIx or IIb fibers contract. It is considered that in a spontaneous respiratory cycle, 40% of the activated fibers in the diaphragm are types I and IIa, with only 5% being type IIx or IIb (Brown et al., 2022). In other words, slow-twitch fibers predominate, requiring more time to contract (longer inspiratory duration) and being more resistant to fatigue.
Likewise, the diaphragm is frequently evaluated both during an inspiration at tidal volume and during a deep inspiration or the sniff test (rapid nasal inspiration; Chow & Hatem, 2022). The main difference between each of them is the duration of the inspiratory time and therefore the speed at which the diaphragm contracts. A value that is rarely used in routine ultrasound examinations, but which indirectly informs us of its strength (Varón-Vega et al., 2021).
The aim of this study is to investigate the relationship between inspiratory time and diaphragmatic contraction (thickness and excursion) and to determine its utility in the functional assessment of the diaphragm.
Material and Method
Design: A nonrandomized cross sectional-controlled study, analysts blinded to the data, carried out between the months of February and September 2022. The study by Trevisan et al. was used for the calculation of the sample size, 80 healthy subjects who met the inclusion/exclusion requirements participated in this study.
Research question: Investigate the effect of inspiratory time on diaphragmatic contraction.
Method: Participants were fasting for the previous 2–3 hr and resting for 10 to 30 min before taking the measurements of height, weight, and age. After, they answered the GPAQ questionnaire on physical activity. Each participant was required to perform three different maximal breathing techniques: diaphragmatic nasal inspiration, pursed-lip mouth inspiration, and nasal inhalation with slight contraction of the glottis (ujjayi yoga breathing). These three breaths were selected because they are performed with slow inspirations, primarily engaging the diaphragm.
Evaluator followed the real-time ultrasound imaging protocol for ultrasound measurements by physiotherapists: three evaluations were taken, pausing 30 s between each repetition, and the average of the three was calculated (Trevisan et al., 2015).
Assessments were consistently conducted by the same evaluator, ultrasound technique expert, with 2 years of experience, under the same conditions and with the same US machine with probes of 2–6 and 6–15 MHz (LOGIQ S7 Expert, GE Healthcare, Chicago, IL, USA). The participants were lying in a supine position, with the legs bent at 30° (Richard, 2017).
Ultrasonic Variables
The first ultrasound measurement was the diaphragmatic thickness. This evaluation is normally taken on the right hemidiaphragm as it is more accessible with the hepatic window, in front of the spleen window (on the left side). All measurements were made at the same point, the intersection between the ninth intercostal space and the midaxillary line, thanks to a longer linear probe at 10–12 MHz (Richard, 2017).
Diaphragm thickness was measured using B-mode US imaging, at two points in time: on a nonforced expiration, at rest (representing the functional residual capacity) and on a maximum inspiration (total lung capacity). The distance between the pleural line and the peritoneal line, both at their innermost part was measured (Crimi et al., 2018).
The second ultrasonographic measurement was the excursion of the diaphragm. On this occasion the 3.5 MHz convex probe (Richard, 2017) was placed following the mid-clavicular line, below the right costal, cranially oriented. We looked for the highest diaphragmatic position, because it is the part of the diaphragm that produces the greatest craniocaudal excursion (Jousela et al., 1994).
The excursion of the diaphragm is measured with M-mode technique, the distance from the highest point of the diaphragmatic dome (end-maximal inspiration, in total lung capacity; Crimi et al., 2018) to the lowest point, which is achieved with the end of each inspiration, in functional residual capacity (Jones et al., 2017; Testa et al., 2011).
The last ultrasonic measurement was the diaphragm contraction time: the same image was used as in the measurement of diaphragmatic excursion, using as reference the starting point of inspiration and the point of maximum inspiration. It was measured in seconds (Richard, 2017).
The calculation of all the measurements and their analysis was carried out thanks to the ImageJ software. Figure 1 shows a comparison of the variables studied in each of the breaths on the ultrasound images.

Ultrasound image of diaphragmatic thickness (top) and excursion and contraction time (bottom) during diaphragmatic breathing (left), pursed lips (center), and ujjayi (right).
Inclusion/exclusion criteria: Healthy subjects, yoga practitioners, aged between 18 and 65 and who did not meet any of the following exclusion criteria (any previous respiratory pathology, thoracic deformities, neuromuscular diseases, treatment with corticosteroids, muscle relaxants and/or barbiturates in the last week, any episode of allergy or thoracic/abdominal surgery in the last 3 weeks (Fayssoil et al., 2018; Trevisan et al., 2015).
The local Research and Ethics Committee of the UAM approved the study protocol with code CEI-120-2409 and registered in Clinical Trials No. NCT05330026. The study was conducted in accordance with the principles described in the Declaration of Helsinki, and all participants signed the consent to participate voluntarily.
Statistical analysis: Categorical variables (sex and smoker) were described with frequencies and percentages, and quantitative variables with mean and standard deviation due to the symmetry on the data distribution. Scatter plots and Pearson's correlation coefficient have been used to study the degree of linear relation between the variables thickness, excursion, and diaphragmatic contraction time. Absolute agreement intraclass correlation coefficient was calculated from a two-way random effects ANOVA. Correlations are reported with the coefficient and the p-value. Linear regression models are no calculated because we cannot establish that one variable is the response and the rest the predictors. The significance level was set at 0.05. The IBM® SPSS version 29 program was used (SPSS® Inc., Chicago, IL, USA).
Results
Eighty subjects participated in the study, whose demographic variables are shown in Table 1. The variables of thickness, excursion, and diaphragmatic inspiration time were measured with each of the breaths (Tables 2 and 3) and when analyzing the correlations (Table 4) between the variables, it was observed that the only variable that shows a statistically significant correlation with the other two is inspiratory time. Thus, it can be seen that the correlation between inspiratory time and diaphragmatic thickness is significant for (p < .001) for the three breaths: diaphragmatic (0.60), ujjayi (0.67), and pursed lips (0.39).
Demographic Variables.

Results From Ultrasound Variables (Thickness, Excursion, and Inspiratory Time) During Diaphragmatic Breathing, Pursed Lips Breathing (LPB), and Ujjayi.

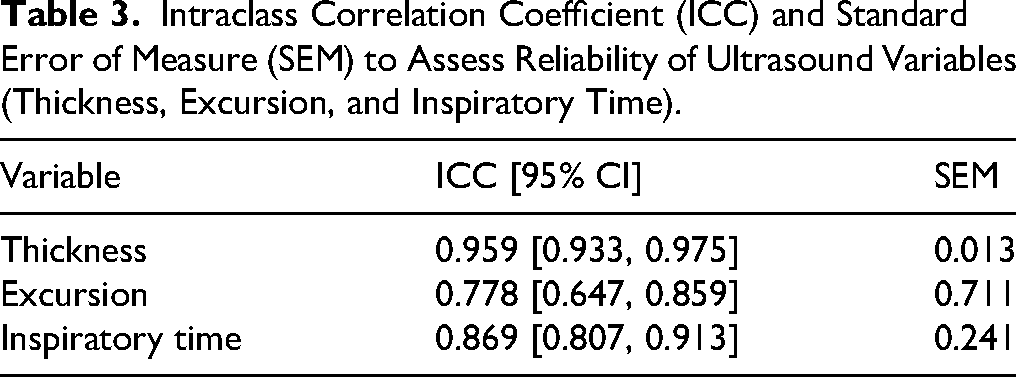
Intraclass Correlation Coefficient (ICC) and Standard Error of Measure (SEM) to Assess Reliability of Ultrasound Variables (Thickness, Excursion, and Inspiratory Time).
Correlations Between the Variables of Thickness, Excursion, and Inspiratory Time During Diaphragmatic Breathing, Pursed Lips Breathing (LPB), and Ujjayi.

When analyzing the correlation between inspiratory time and diaphragmatic excursion, it is significant for diaphragmatic respirations (−0.24 p = .035) and for ujjayi (0.27 p = .017) but not for pursed lips (−0.01 p = .90).
Finally, it should be noted that there was no correlation between the variables of diaphragmatic thickness and excursion in any breath: diaphragmatic (−0.15 p = .194), ujjayi (0.21 p = .064), and pursed lips (−0.14 p = .226).
Discussion
This study demonstrates the interest of the inspiratory time variable in the analysis of diaphragm functionality and its relationship with diaphragmatic thickness and excursion in long and deep inspirations.
Functional tests, such as spirometry or diffusion capacity have been used for decades to help diagnose and monitor the progression of lung diseases, as well as their response to treatment (Stanojevic et al., 2022). They provide information about the functionality of the respiratory system dynamically versus more static tests, such as a chest X-ray. Something similar happens in ultrasound of the diaphragm, since it allows us to take a dynamic measurement, the diaphragmatic excursion, and a more static one, the thickness.
Thickness gives us information about the strength (Fogarty et al., 2018), because the diaphragm, like all striated muscles, has the characteristic of increasing in volume when contracting, due to the creation of actin and myosin bridges (Pham & Puckett, 2022). This, together with the fact that it remains active throughout inspiration, would explain why in this study the correlation is positive between time and thickness, that is, the longer the duration of inspiration, the greater the diaphragmatic thickness. In addition, it cannot be forgotten that it is composed of Type I fibers, muscle fibers specially designed to resist long contractions and has a higher density of mitochondria and therefore, a higher oxidative capacity (Plotkin et al., 2021).
But thickness is not only determined by muscle contraction, but also depends on anthropometric measurements such as height, sex, or weight (McCool et al., 1997). This would explain the results of other studies (Dos Santos Yamaguti et al., 2008; Souza et al., 2014) in which after a specific training of the inspiratory musculature, the improvement in the excursion was not so important, despite the increase in thickness. The researchers observed the same in this study, as there is no significant correlation between excursion and thickness, or in other words, an increase in thickness does not always translate into an improvement in diaphragmatic excursion.
While it is true that the measurements of this study were taken in healthy subjects, there is a study in COPD patients in which it is concluded that diaphragmatic dysfunction is more related to mobility restriction than to muscle thickness (Ogan et al., 2019). This could be justified on one hand because the increase in diaphragmatic thickness in these patients is more attributed to an increase in fatty tissue rather than muscular fibers (Ostadan et al., 2023). On the other hand by the breathing used by this type of patient (pursed lips) which leads to an activation of the sternocleidomastoid (Kang et al., 2018; Shiraishi et al., 2023). Just like in this study, which is the only breath in which there is no correlation between the diaphragmatic excursion and the duration of inspiration. It has been observed that in mouth breaths there is a greater activation of the accessory muscles, mainly scalenes and sternocleidomastoid muscles (da Fonsêca et al., 2020; Medeiros da Fonsêca et al., 2022) and therefore, a greater increase in thoracic volume compared to abdominal volume.
If the focus is now on the key variable of this study, the diaphragmatic contraction time, it is known that a strong diaphragm is not only measured in power but also in resistance. When measuring the diaphragmatic thickness and excursion variables during a sniff test or a deep inspiration or at tidal volume by ultrasound, it is observed that they are greater in a deep inspiration than in a tidal volume (Yamada et al., 2017). So it can be deduced that the duration of inspiration influences both values in pulmonary and extrapulmonary respiratory diseases, such as neuromuscular diseases (Di Costanzo et al., 2023; Ruggeri et al., 2020).
Slow, directed breathing is one of the most commonly used techniques in respiratory physiotherapy. It aims to increase inspiratory volume and, above all, to increase inspiratory time (Chukwu et al., 2022). This creates a laminar flow that improves alveolar ventilation (Mendes et al., 2021) and abdominal displacement (Parreira et al., 2005), resulting in an increase in diaphragmatic excursion.
In this study, it was obtained that, in maximal inspirations, the increase in inspiratory time did not lead to a greater increase in diaphragmatic excursion. The reason is that this variable, as its name suggests, refers to the descent of the diaphragm muscle and has an anatomical limit in the viscera of the abdominal cavity (Bordoni & Zanier, 2013). Once reached, if inspiration continues, that is, if the diaphragm continues to contract, the rest of the inspiratory muscles (sternocleidomastoid, scalenes, and external intercostals) come into action (Acosta et al., 2018). This was observed by Wang et al. (2009) in their study, by comparing the data obtained with ultrasound (excursion) and plethysmography (abdominal, middle, and upper thoracic volume) in healthy subjects. They demonstrated the direct relationship between the descent of the diaphragm and abdominal volume (94–95% of maximum capacity) and that once its maximum was reached, the medium (3%) and high (1–2%) thoracic volumes also increased, due to the action of the accessory muscles.
Returning to the results of this study, as described above, it is observed that in maximal inspirations an increase in the thickness of the diaphragm does lead to a greater increase in inspiratory time. So perhaps if Dos Santos Yamaguti et al. (2008) and Souza et al. (2014). If they had measured the duration of inspiration, they would have observed that despite no change in diaphragmatic excursion, participants were able to maintain longer breaths. That is why relying only on diaphragmatic excursion as an evaluation of the diaphragm is a mistake, since the diaphragm is also stronger when it can maintain its contraction for longer.
Conclusions
The time of inspiratory contraction and the diaphragmatic excursion are two essential variables in the dynamic functional evaluation of the diaphragm, providing information about its strength and contraction resistance, compared to the measurement of diaphragmatic thickness, which is solely an anatomical parameter.
Strengths and Limitations
This is the first article that demonstrates the relationship between inspiratory time and diaphragmatic thickness, using ultrasound. This would imply that, in clinical practice, it would only be necessary to measure contraction time and diaphragmatic excursion to evaluate diaphragm functionality, without the need to assess thickness. This approach offers the advantage of saving time, as both variables can be measured during a single inspiration using the convex probe.
Despite following the ultrasound protocol for diaphragm evaluation, this technique is still evaluator dependent. Therefore, all the measurements, as well as the analysis of the images, were carried out by the same person. The participants were all healthy subjects, so the values obtained from each of the variables were within the normal range. It would be interesting to carry out this study with patients who have followed a specific training of the inspiratory muscles and see the effects on inspiratory time. The chosen position for measurements (supine position, with the legs bent at 30°) is very helpful for locating the diaphragm by relaxing the abdominal muscles but may also limit its descent, thus reducing its excursion.
Implications for Nursing Practice
Although ultrasound is not available in all workplaces, it has become a very useful tool in diaphragmatic assessment. It offers advantages for both patients (nonionizing, no prior preparation, and no adverse effects) and therapists, primarily physical therapists and nurses, since it can be performed without medical supervision, unlike other methods such as spirometry or transdiaphragmatic pressure.
Supplemental Material
sj-docx-1-son-10.1177_23779608251337591 - Supplemental material for Inspiration Time: The Ultrasound Variable Necessary to Study the Diaphragm Functionality. A Cross-Sectional Controlled Study
Supplemental material, sj-docx-1-son-10.1177_23779608251337591 for Inspiration Time: The Ultrasound Variable Necessary to Study the Diaphragm Functionality. A Cross-Sectional Controlled Study by Teresa E Fernández-Pardo, Maria Jesús Rodríguez-Nieto, Mercedes Furió-Valverde, María García-Arrabé, Ana Mallo-Lopez, Ignacio Mahillo-Fernández and Germán Peces-Barba Romero in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608251337591 - Supplemental material for Inspiration Time: The Ultrasound Variable Necessary to Study the Diaphragm Functionality. A Cross-Sectional Controlled Study
Supplemental material, sj-pdf-2-son-10.1177_23779608251337591 for Inspiration Time: The Ultrasound Variable Necessary to Study the Diaphragm Functionality. A Cross-Sectional Controlled Study by Teresa E Fernández-Pardo, Maria Jesús Rodríguez-Nieto, Mercedes Furió-Valverde, María García-Arrabé, Ana Mallo-Lopez, Ignacio Mahillo-Fernández and Germán Peces-Barba Romero in SAGE Open Nursing
Footnotes
Ethics Considerations and Consent to Participate
The local Research and Ethics Committee of the UAM approved the study protocol with code CEI-120-2409. The study was conducted in accordance with the principles described in the Declaration of Helsinki, and all participants signed the consent to participate voluntarily.
Consent for Publication
All authors and participants consent the publication.
Author Contributions
Teresa E Fernández-Pardo: conceptualization, methodology, investigation, and writing—original draft; María Jesús Rodríguez-Nieto: supervision, validation, writing—reviewing and editing; Mercedes Furió-Valverde: conceptualization, and writing—review and editing; María García-Arrabé: methodology, investigation, and writing—review and editing; Ana Mallo-López: writing—review and editing; Ignacio Mahillo-Fernández: formal analysis; Germán Peces-Barba Romero: supervision, validation, and writing—reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Datasets supporting the reported results are available upon request to the first author.
Study Approval Number
NCT05330026.
Use of AI Software
The authors declare no use of AI software.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.