
Abstract
Introduction
Rapid and reliable peripheral IV access is essential for many patients admitted to the emergency department (ED) to ensure administration of life-saving medications, and successful intravenous cannulation can significantly affect patient care.
Objective
The objective of this study was to assess the impact of a continuous needle tracking system on the accuracy, speed, and quality of ultrasound-guided peripheral venous catheter insertions.
Methods
A convenient sample study based on the study setting using simulated tissue was conducted with 49 US-based ED nurses to compare the insertion of a midline catheter using traditional ultrasound guidance versus an advanced needle-tracking technology along with ultrasound guidance. The purpose of this evaluation was to assess the impact of continuous needle tracking system. Informed consent was obtained from all individual participants involved in this study. All participants were made aware that the results may be published. There was no IRB approval for this study. All sources were properly disclosed within the text.
Results
The addition of the advanced needle-tracking technology significantly reduced total insertion attempts, insertion time, backwall penetrations, and redirects (probes to hit the target vein), while improving image clarity and confidence for participants.
Conclusion
The innovative needle-tracking system evaluated in this pilot study has the potential to improve emergent difficult vascular access. EDs should assess the value of this technology to potentially improve the management of difficult intravenous access patients in their settings.
Keywords
Introduction
Acutely ill patients admitted to the emergency department (ED) usually require at least one fast and reliable peripheral intravenous (PIV) access device to allow the administration of urgent and life-saving medications, and to optimize the evaluation and stabilization of critically ill patients. Obtaining vascular access in a timely manner is essential, and successful intravenous (IV) cannulation is a factor that significantly impacts patient care. Furthermore, delays in the establishment of vascular access may impede diagnostic testing, including laboratory analysis and radiology evaluation, prevent the efficient treatment of patients, and slow ED throughput (Scoppettuolo et al., 2016).
Review of Literature
Difficult intravenous access (DIVA), defined as requiring two or more IV attempts or the use of a vascular access rescue method to establish IV access, is a frequent challenge in the ED, affecting nearly one in every nine adults in an urban ED for a variety of reasons (Fields et al., 2014). One of the variables found to be predictive of DIVA was the inability of healthcare providers to detect a dilated vein by palpating and/or visualizing the extremity (van Loon et al., 2019). The typical palpation IV insertion time has been reported as 2.5 to 12.6 min, with patients with DIVA requiring as much as 125 min (Costantino et al., 2005; Lapostolle et al., 2007; Piredda et al., 2017). As a result, DIVA patients may be subjected to numerous IV placement attempts by multiple practitioners, which not only causes significant pain to the patient but also consumes considerable resources and time (Fields et al., 2014; Witting, 2012).
DIVA may lead to serious consequences. Patient pain and overall suffering are increased by repeated attempts to obtain venous access, which in turn may increase the risk of subsequent complications (Abolfotouh et al., 2014; Gorski et al., 2021; Hawes, 2007). Difficult access also leads to delays in the administration of medications, partial or total loss of a prescribed dose, and the need to place central venous lines, representing a greater risk for patients (Gorski et al., 2021). Moreover, it may cause an increase in material use, nurse time, costs associated with complications, and length of stay (Hawes, 2007).
Ultrasound (US) guidance for vascular access has been in clinical practice for more than 30 years and has been increasingly utilized for target vessel visualization to minimize complications and increase success rates during vascular cannulation. Multiple studies have demonstrated significantly increased safety, effectiveness, and efficiency of US-guided vascular access, as compared to cannulation by anatomical landmarks and/or acoustic Doppler (Privitera et al., 2022; Vezzani et al., 2013).
Consensus statements recommend the use of US-guided PIV placement as a safe alternative to palpation IV technique to establish vascular access, especially in patients with DIVA (Lamperti et al., 2012; Spencer & Bardin-Spencer, 2019). The adoption of US-guided techniques has been shown to reduce the number of punctures and time needed to achieve vascular access, and to increase patient satisfaction (Franco-Sadud et al., 2019; van Loon et al., 2018).
While real-time US needle guidance optimizes the probability of needle placement in the vessel upon first pass, minimizing the risk of complications (Chapman et al., 2006), in true clinical practice, it is not always possible to achieve this ideal (Spencer & Bardin-Spencer, 2019).
The introduction of continuous needle tracking as an adjuvant to US-guided vascular access has been proposed to provide greater control in guiding the needle from insertion to vein and may augment the US-guided technique (“AIUM practice guideline for the use of ultrasound to guide vascular access procedures,” 2013). According to the American Institute of Ultrasound in Medicine, using needle localization and guidance products that do not make it difficult to move the needle may make vascular access procedures safer and easier for providers and patients (“AIUM practice guideline for the use of ultrasound to guide vascular access procedures,” 2013).
Methods
Design
A pilot simulation study evaluated the CueTM Needle-Tracking System (Becton Dickinson, Franklin Lakes, NJ), a newly introduced needle-tracking system. The system tracks needle position, depth, and trajectory, highlights when the needle is centered in the target vein, and superimposes this tracking on the US image. In the pilot simulation study, the CueTM system was used with the Site-Rite® 8 ultrasound system (Becton Dickinson, Franklin Lakes, NJ) to insert a PowerGlide ProTM Midline Catheter (Becton Dickinson, Franklin Lakes, NJ) into a gel test block with a metallic target imbedded in it to represent the target vein.
Research Question
What is the impact of a continuous needle tracking system on the accuracy, speed, and quality of ultrasound-guided peripheral venous catheter insertions?
Sample
Participants were recruited from among attendees at the Emergency Nursing 2019 Meeting (October, 2019, Austin, TX), and included 49 US-based ED nurses.
Inclusion/Exclusion Criteria
The inclusion criteria required participants to have placed 10 PIV catheters in the past 60 days and placed <15 US-assisted vascular access devices in the past 60 days. Each participant received the same training on the use of the CueTM system. The testing sequence was randomized for each participant.
Ethical Considerations
This simulation-based study was completed by healthcare providers to indicate accuracy measurements (e.g., insertion time in seconds) and self-reported estimates (e.g., perceived confidence). No patient data were collected, and the study was conducted in accordance with the Declaration of Helsinki ethical principles for medical research (World Medical Association, 2013) and the US Office of Human Research Protections guidance (Subpart A of 45 CFR Part 46: Basic Health and Human Services Policy for the Protection of Human Subjects, 2018); informed consent was obtained from participants as evidence of their agreement to voluntarily participate in this study. Participants also consented to the release of information obtained due to their participation, and were informed that the study sponsor would not reveal identifying information in any publication resulting from the study. Therefore, an ethical committee was not consulted. All data were deidentified before performing any analyses.
Tests and Procedures
In the accuracy test, participants inserted the midline catheter into a gel test block with a metallic target imbedded in it to represent the target vein. Each participant made six attempts to contact the metallic target—three with the assistance of the CueTM Needle-Tracking System (the intervention) and three with traditional US techniques using Site-Rite® 8 ultrasound system (the control). Outcomes were recorded as the distance in millimeters from the target, as indicated by the puncture of the embedded plastic sheet surrounding the metallic target. The plastic sheet embedded in the phantom target was changed between participants/and intervention with each participant.
In the insertion and timing test, participants used the provided US unit to make six successful catheter insertions—three in the intervention group and three in the control group.
Each participant made as many attempts as needed to successfully insert six catheters; the time required for all attempts was recorded, starting from the time the participant verbally indicated they would puncture the test block until they self-reported that their attempt was complete. At completion of the attempt, the time required (in seconds) and the outcome (success/failure) were recorded. Additional attempts followed failed insertions until success was achieved. The number of additional attempts and the time required were recorded.
Additionally, a proprietary software program (CueTM Needle-Tracking System technology) for data capture was used on each attempt. This data capture provided screen captures at 3 Hz with associated needle tracking data for the evaluation of backwall penetration events. Needle tracking data were recorded for each attempt and the software identified redirects and deflections, as the operator probed to find the vein.
Outcomes and Statistical Analyses
The primary outcomes constituted accuracy measurements recorded as 0.01-mm increments, insertion time in seconds, number of deflections, number of redirects, number of attempts (or first stick success rate), and backwall complications. All the primary outcomes data for the intervention and control arms were recorded during three repeated observations in trials 1, 2, and 3 of this study.
The secondary outcomes constituted the self-reported estimates of the clarity of needle tip location (“How clear was the needle tip location?”) and perceived confidence (“How confident were you during insertion?”). Responses were reported on a Likert scale of 1 (“Extremely unclear”) to 7 (“Extremely clear”). All secondary outcomes for the control and intervention groups were collected from the respondents at the end of the study.
Descriptive statistics were calculated for all the primary and secondary outcomes. Median and standard deviations (SDs) were reported for the continuous variables, and frequency/percentages were reported for the categorical variables. Wilcoxon signed rank tests were conducted to compare the medians of the accuracy measurements, insertion time, deflections, and redirects. Chi-square and Fisher's exact tests were conducted to compare all the categorical variables including number of attempts, backwall complications, clarity, and confidence.
Eight regression models were designed to analyze the associations between all the outcome variables and treatment effect. For each regression model, the dependent variable constituted one of the outcome variables and the independent variable constituted an indicator variable for the treatment effect.
To account for the dependency of repeated measures within each participant and trial, mixed effect models were found to be a good fit for four outcomes: accuracy measurements, insertion time, deflections, and redirects. The treatment effect was considered the fixed effect, and the participant number and trial number were the random effects.
For the accuracy measurements and insertion time, a linear mixed effect model was used. Both outcome variables did not have a normal distribution; therefore, a log transformation was conducted for the analysis. The estimates were then converted back to the exponential form and presented in this study. For deflections and redirects, a generalized negative binomial mixed effects model was used, and the estimates were presented as incidence rate ratios (IRR).
The number of attempts was analyzed using Poisson regression and the estimates were presented as IRR. The backwall penetrations variable contained a large number of zeroes, therefore, zero-inflated negative binomial regression was used for this variable and the estimates were presented as IRR. Ordered logistic regression was used to model clarity and confidence, and the estimates were presented as odds ratios (ORs). Statistical significance was measured at p-value ≤.05. All the analyses were conducted using SAS Enterprise Guide and STATA MP 15.
Results
Primary Outcomes
The overall median accuracy measurement of the sample was 2.23 mm from target (SD = 3.11). There was no significant difference in the accuracy measurements for the control (2.40 + /−3.06 mm) versus intervention method (2.08 + /−3.18 mm; Table 1). Insertion time difference might be less if training and experience with US-guided midline insertion were included. Training and experience may also influence avoidable complications, such as penetration of the back wall (Table 2).
Descriptive Statistics for the Control and Intervention Methods.
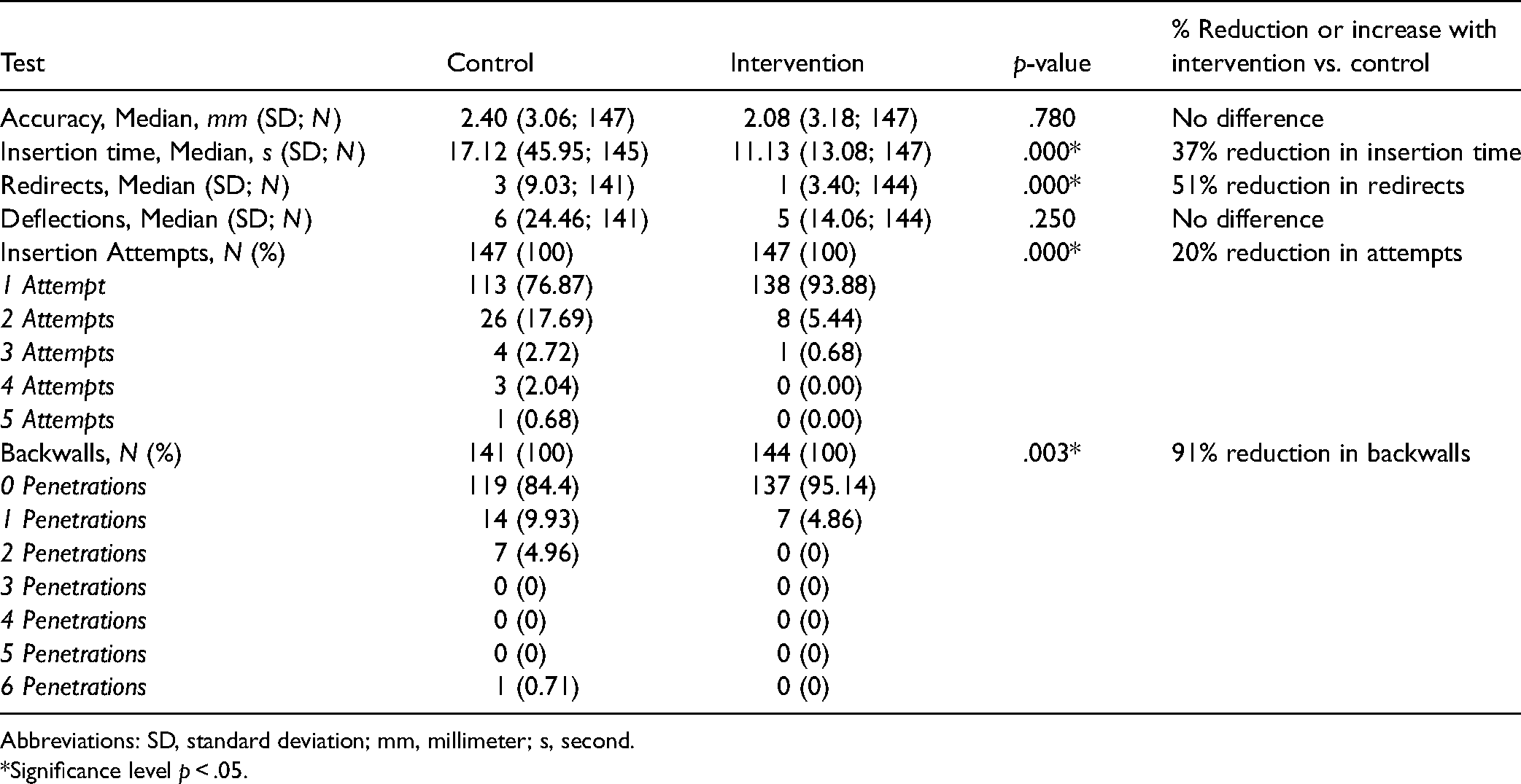
Abbreviations: SD, standard deviation; mm, millimeter; s, second.
*Significance level p < .05.
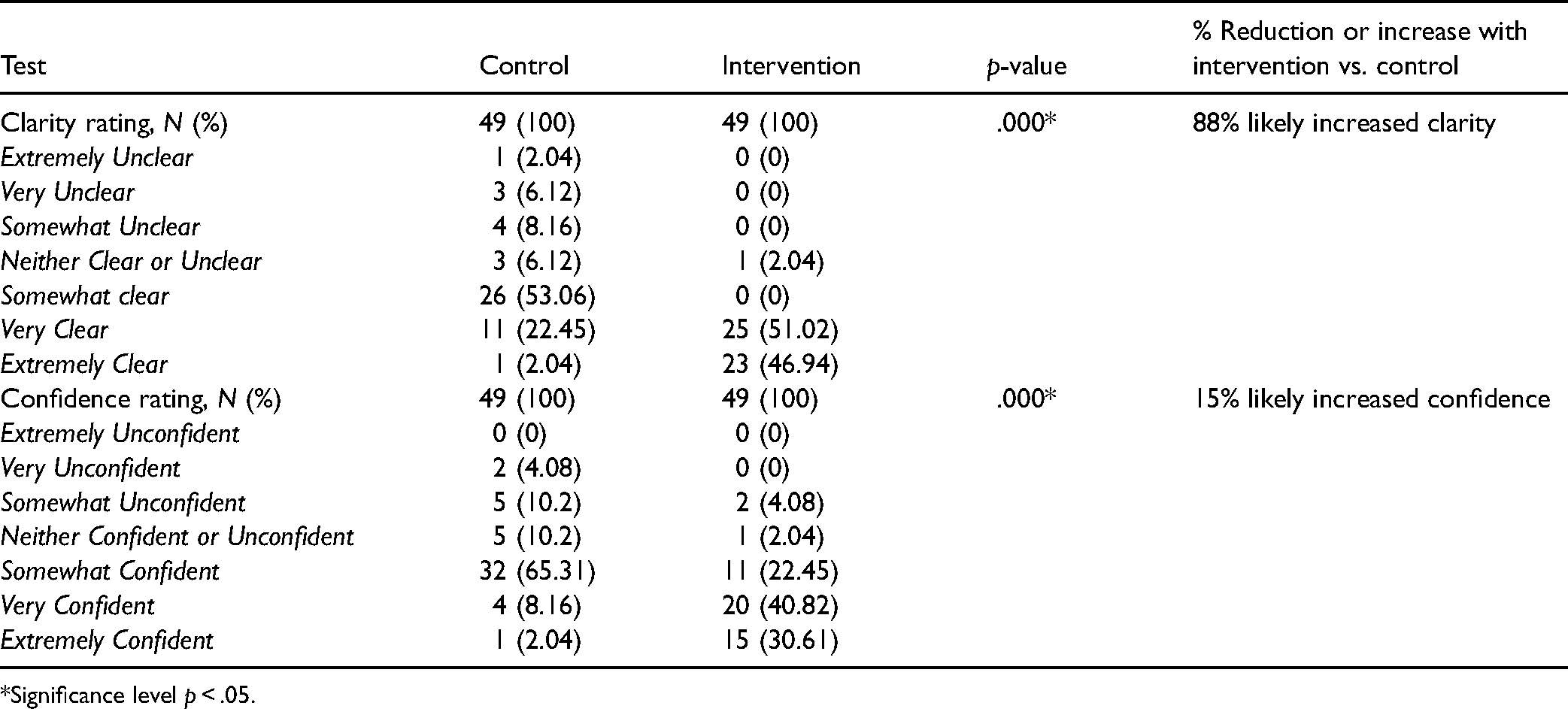
Nurses Self-reported Estimates of the Clarity of Needle Tip Location and Perceived Confidence for the Control and Intervention Methods.
*Significance level p < .05.
The median insertion time was statistically higher for the traditional method versus Cue (17.12 vs. 11.13, p = .000). According to the regression model shown in Table 3, as compared to the control method, the insertion time for the intervention attempts decreased by 37% (95% CI: 0.537–0.737, p = .000).
Regression Models Assessing the Association Between the Outcome Variables and the Treatment Effect (Control vs. Intervention).

Abbreviations: CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio.
*Significance level p < .05.
The median number of deflections of the overall sample was 6 (SD = 19.92) and no significant differences were found between the two methods.
The median number of redirects was significantly higher for the method utilizing US when compared to the intervention (3 vs. 1, p = .000). Also, the regression model in Table 3 suggests that compared to the traditional method, the number of redirects decreased significantly by a factor of 0.494 for intervention method (95% CI: 0.381–0.640, p = .000). In other words, the intervention attempts had 51% fewer redirects compared to the control method.
The number of attempts was significantly different for control versus intervention, with 94% of intervention insertions having first-stick success (number of attempts = 1) versus 77% for the control method. According to the regression model in Table 3, the number of attempts decreased by a factor of 0.805 for the intervention as compared to control (95% CI: 0.653–0.993, p = .043).
Backwall penetrations were significantly greater with the control method versus the intervention method, with zero penetrations recorded for 95% of the intervention attempts versus 84% of the control attempts. According to the regression model, the expected rate of backwall penetrations would decrease by a factor of 0.09 for the intervention (95% CI: 0.0162–0.512, p = .007). In other words, the intervention method had 91% fewer backwall penetrations compared to the control method.
Secondary Outcomes
The self-reported measures of needle location clarity showed significant differences between the control and intervention methods with approximately 98% reporting a needle location clarity of Very Clear or Extremely Clear with the intervention method as compared to 25% of the control method. Also, the regression model in Table 3 showed that the perceptions of high needle clarity were 88 times greater with the intervention method than with the control method (95% CI: 18.73–411.37, p = .000).
The self-reported measures of confidence during insertion showed significant differences between the control and intervention methods with approximately 72% reporting a confidence rating of Very Confident or Extremely Confident with the intervention method as compared to 10% of the control method. Also, the regression model in Table 3 showed that the odds of having a higher confidence rating were 15 times greater with the intervention method versus the control (95% CI: 5.82–39.50, p = .000).
Discussion
In this pilot study, the accuracy of needle placement in the target vein was similar with Cue™ system and traditional US guidance, suggesting that experienced emergency nurses can get relatively close to a target with either method after comparable training, even when adopting this new technology. The new technology did not reduce the existing accuracy of the US trained nurses using this method (these nurses have been trained but have only placed <15 catheters utilizing US).
First-stick success in the ED is important when IV access is required to deliver life-saving treatments. First-stick success was significantly more frequent, while total attempts and insertion time were significantly reduced by the addition of the Cue™ system. This improvement may enable faster time to treatment, more efficient through-put in the ED, and may offer an improved patient experience.
Backwall events where the needle penetrates through the backwall of the vessel were significantly reduced with the CueTM system. This reduces the risk of extravasation and bruising, and could impact IV dwell time and patient satisfaction.
Redirects, or probes to hit the target vein, were significantly reduced with the CueTM system, which has potential implications for time-to-treatment and provider efficiency, and could impact patient satisfaction.
Self-reported image clarity and operator confidence among participants also improved with the CueTM system, which may contribute to provider satisfaction. The ability to see the needle tip is critical to insertion attempts, especially for DIVA patients.
Strengths and Limitations
This pilot study has limitations based on the small number of participants; however, the statistically significant preliminary results suggest that hospital EDs may want to conduct local studies to determine the role of advanced needle-tracking systems in their armamentarium for vascular access.
The clinicians who participated in this study had limited use of US, having placed less than 15 catheters utilizing US technology prior to enrollment in this study. This may be considered a limitation in experience but also shows the ease of use with the CueTM Needle-Tracking System.
Another limitation is the use of a convenience sample and recruitment at a conference where the sample of clinicians was close at hand. These nurses were experienced emergency room clinicians with limited US experience.
Implications for Emergency Clinical Practice
In the high-pressure setting of the ED, rapid venous access may be required for life-saving interventions. Every factor that contributes to the accuracy and speed of venous access, as well as clarity and confidence for nurses, particularly when faced with DIVA patients, can affect patient outcomes. US guidance to insert midline catheters is useful and may be further enhanced when paired with a needle-tracking system.
Conclusions
This pilot study demonstrated that when a needle-tracking system was paired with US guidance, it reduced the number of attempts and time to successful insertion, and penetration of vessel backwall, and improved operator's confidence and perception of needle clarity. These preliminary data suggest that this innovative needle-tracking technology represents an important advance in the practice of vascular access. As the American Institute of Ultrasound in Medicine suggested, needle localization and guidance products may make vascular access procedures safer and easier for clinicians. In this pilot study, the CueTM Needle-Tracking System demonstrated more rapid and accurate vascular access. Education and training are key in the success of any new technology and should be included with any new or upgraded procedure.
Footnotes
Acknowledgments
The authors recognize the valuable contributions of, Maureen Burger, Prachi Arora and Christine deVries, who are employees of Visante Inc and who helped with the writing and editing of this manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KA and KH report being employees of and own stocks in Becton, Dickinson and Company.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Becton, Dickinson and Company.