
Abstract
Introduction
The evolving landscape of healthcare in Jordan presents unique challenges and opportunities for nursing professionals. With a focus on critical care nurses, understanding the dynamics of professional autonomy and professionalism within this context is crucial for advancing nursing practice and improving patient care.
Objectives
This study aimed to investigate the relationships between perceived nursing professional autonomy and professionalism among critical care nurses in Jordan.
Methods
A descriptive correlation design was used among critical care nurses from five major Jordanian governmental hospitals. A total of 227 questionnaires were distributed, with a final sample size of 200 participants. Data were collected between August and September 2023. Professional autonomy and professionalism were measured using the Dempster Practice Behaviors Scale and the Nurses' Professionalism Inventory, respectively. We used the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines in the current study.
Results
The study revealed moderate levels of perceived professional autonomy (mean DPBS total score: 103.94) and professionalism (mean NPI total score: 119.12) among participants. A significant positive correlation (r = .49, p < .001) was observed between these two constructs. However, demographic and work-related factors showed minimal influence on these perceptions.
Conclusion
The study highlights the importance of professional autonomy and professionalism in improving nursing care in Jordan. It recommends targeted approaches like ongoing education and supportive workplace policies to bolster these aspects. These findings have significant implications for nursing policy and education across various healthcare settings.
Keywords
Introduction
In contemporary medical disciplines, professionalism and ethical conduct are paramount, ensuring that healthcare practitioners treat their patients with dignity, respect, fairness, and sound judgment (Varkey, 2021). Nursing professionalism is an important part of the nursing profession that ensures quality patient care and ethical practice, and it should be used to determine how individuals receive care in all healthcare systems (Bani-Hani & Hamdan-Mansour, 2021). Professional autonomy has been recognized as an essential component of nursing practice, and the nursing profession places a premium on it (Fitzgerald, 2020; Pursio et al., 2021). Critical care nurses were selected for this study due to their crucial role in high-stakes patient care, which demands a significant degree of autonomy, highlighting the unique requirements of critical care and the importance of autonomy in their professional practice (Taleghani et al., 2023).
Review of the Literature
Professionalism refers to the behavior, qualities, and/or objectives that distinguish a profession and typically defines practices that are required of its members (Fitzgerald, 2020). Attitudes, knowledge, and behaviors that demonstrate a multidisciplinary approach to the laws, concepts, and standards that underpin good clinical practices are manifestations of professionalism (Kaya & Boz, 2019).
Although, professionalism is exceedingly difficult to quantify. An in-depth analysis of both the overall profession and the individual behaviors that form professionalism is essential to improve nursing professionalism (García-Moyano et al., 2019). Miller et al. (1993) developed the Behavioral Inventory for Professionalism in Nursing to assess professional behaviors among nurses using Miller's Professionalism Model.
Professionalism in nursing requires a combination of knowledge and skills, dedication to compassion, caring, and strong moral values; ongoing self- and other-development; accountability and responsibility for incisive practice; and showing a collaborative and flexible attitude (Tola et al., 2020). Nurses who adhered to practice guidelines and displayed technical (psychomotor) proficiency exemplified professionalism (Grande et al., 2022). Autonomy is the main element of professional practice and professionalism in nursing (Rouhi-Balasi et al., 2020).
Professional autonomy is defined by Skår (2010) as having the authority and freedom to act in alignment with one's professional knowledge base. Self-determination theory (SDT) posits that autonomy is a fundamental human need that enhances motivation and engagement (Deci & Ryan, 2000). Professional autonomy in nursing is also defined as independence in patient treatment and the capacity to use clinical decision-making and clinical judgment (Roshanzadeh et al., 2018). It benefits both caregivers and patients, boosts nurses’ job satisfaction (Labrague et al., 2019), improve nurse-physician collaboration and team spirit, reduce emotional stress and intention to leave (Laurs et al., 2020), and improve patient care quality and safety (Lee & Choi, 2019). Studies also found association between nurses’ professional autonomy and patients’ mortality rates and risk of complications (Rao et al., 2017). Professional autonomy empowers nurses to make sound choices in order to establish and maintain patient safety, enhance care quality, retain nurses in their field, and guarantee job satisfaction (Mert &Türkmen, 2020; Rouhi-Balasi et al., 2020). On the other side, nurses’ professional autonomy is hampered by a lack of institutional support, inadequate incentives, and a lack of participation in professional groups (Pursio et al., 2021). When professional autonomy is insufficient, it is frequently linked to reasons such as inadequate workplace guidelines (Abdolmaleki et al., 2018), and the medical profession's common domination within healthcare system (Germov, 2019).
Nursing professionalism and professional autonomy represent fundamental elements within the healthcare framework, profoundly impacting the delivery of high-quality healthcare services (Rouhi-Balasi et al., 2020; Shohani et al., 2018). There are some factors that influence professional autonomy and professionalism such as individual characteristics, including gender and the specific clinical specialty; for example, gender may influence autonomy in clinical decision-making (Maharmeh, 2017), and certain clinical specialty within nursing may offer varying degrees of autonomy, thereby affecting professionalism (Pursio et al., 2021). The workplace conditions, including nurse-patient ratios, workload, and resources, play a pivotal role in determining the extent to which nurses can exercise their professional autonomy and professionalism. In settings with optimal conditions, nurses may find it easier to engage in autonomous decision-making and maintain high levels of professionalism (Labrague et al., 2019). Supportive leaders who encourage autonomy and provide opportunities for professional growth can foster a culture of professionalism among nursing staff (Yuk & Yu, 2023).
The relationship between autonomy and professionalism is not clearly understood by the researchers; however, problem-solving skills act as mediators between professional autonomy and job satisfaction, influencing professionalism (Bayer et al., 2023). A qualitative meta-synthesis study for 13 articles found that the professional autonomy is a developmental achievement rooted in patient-centered competence and self-reliance, enabling healthcare professionals to create optimal care plans that enhance patient health through informed decision-making and effective collaboration with team members. This autonomy also fosters job satisfaction and professionalism, with problem-solving skills playing a key role in strengthening these connections (Rouhi-Balasi et al., 2020). Nurses with strong problem-solving abilities are more likely to effectively address clinical challenges, make autonomous decisions, and maintain professionalism in their practice. The multifaceted relationship between these two concepts, particularly in the context of critical care nursing in Jordan, is not well understood (Maaitah et al., 2019). Given the crucial role that critical care nurses play in Jordanian healthcare settings, the extent of this problem is extensive (Donovan et al., 2018). This study aims to investigate the relationships between perceived nursing professional autonomy and professionalism among critical care nurses in Jordan. Understanding this relationship is crucial for advancing nursing practice and improving patient care in Jordan's evolving healthcare landscape.
Methods
Design
The study employed a descriptive correlation design to answer the research questions. We used the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines in the current study.
Research Questions
The current study addressed the following research questions:
What are the levels of nursing professionalism perceived by Jordanian critical care nurses? How do Jordanian critical care nurses evaluate their nursing professional autonomy? What is the association between perceived nursing professionalism and nursing professional autonomy among Jordanian critical nurses? What sociodemographic and work-related factors predict the perceived levels of nursing professionalism and nursing professional autonomy? Are there differences in perceived nursing professionalism and professional autonomy based on the sociodemographic and work-related factors?
Sample and Setting
The study used a convenience sampling technique to recruit participants. The study was conducted at five large Jordanian governmental hospitals. The hospitals were selected based on specific criteria, that is: availability of a critical care unit, adequate sample size, accreditation by the Healthcare Accreditation Council and representation of the diverse geographical areas across Jordan. This ensured a comprehensive and representative sample for the study.
The sample size calculation was conducted using G power analysis, the medium effect size of 0.15; the desired statistical power, set at 0.8; The number of predictors in the regression model was determined to be 13; the significance criterion was set at p-value < .05. Based on these parameters, G power analysis estimated that a minimum sample size of 131 participants was required to achieve the desired statistical power. However, to increase power, an additional number of participants was added to the calculated sample size. The final required sample size was determined to be around 200 participants.
To ensure a fair and unbiased recruitment of participants from the five governmental hospitals in Jordan, a quota recruitment technique was employed. The sample size from each hospital was determined based on the number of critical care nurses available: Princess Basma Hospital with 30 nurses, Al-Basheer Hospital with 160 nurses, Al-Badiah Hospital with 25 nurses, Almafraq Hospital with 45 nurses, and Prince Faisal Hospital with 50 nurses. In the study, which included five hospitals, the sample size for each was calculated based on their individual critical care nurse populations. To determine the sample size for each hospital, these proportions were applied to the estimated total sample size of 209 participants (Albasheer Hospital = 108; Almafraq Hospital = 31; Prince Faisal = 34 participants; Prince Basma Hospital = 20 participants; and Albadiah Hospital = 17 participants).
Inclusion/Exclusion Criteria
The inclusion criteria were: Registered critical care nurses who are registered with the Jordan Nursing Council, who are currently working in the intensive care units at the governmental hospitals, with a minimum of 1 year of experience in critical care settings and who have at least 1 year of experience in providing direct patient care at the bedside. Nurses who did not meet the inclusion criteria and nurse managers were excluded from the study.
Measurements
The following instruments were used to collect data:
1. The sociodemographic data sheet was used in collecting essential sociodemographic information from the study participants. It encompassed a range of demographic variables, including age, gender, educational attainment, marital status, years of experience in critical care units, overall years of experience in the nursing profession, current unit assignment, and the type of shift duty (e.g., fixed day shift, day-night shifts, ABC shifts). Moreover, data about work status were also collected; such as the name of the hospital, previous work experience outside the Jordanian Ministry of Health, previous experience in other health sectors outside Jordan, previous experience in sectors unrelated to direct nursing care, and participants’ intentions to leave nursing career. 2. The Dempster Practice Behaviors Scale (DPBS) was used in this study to measure professional autonomy. The DPBS is a 30-item questionnaire that consists of four subscales: Readiness, Empowerment, Actualization, and Valuation. The subscale of readiness includes 11 items and examines the participants of skills, competence, and mastery. The empowerment subscale owns seven questions to assess the legitimacy of the performer. The actualization subscale holds nine items that investigate decision-making, accountability, and responsibilities. The valuation subscale has three questions to evaluate the value, worth, merit, and usefulness. This questionnaire used a 5-point Likert scale (1 = “not at all true”; 2 = “slightly true”; 3 = “moderately true”; 4 = “very true”; 5 = “extremely true”). The scores for each subscale are calculated by summing the scores of the items in that subscale. The total score is the sum of the four subscale scores. The higher the total score, the higher the perceived level of professional autonomy. The total summed scores of nurses’ professional autonomy ranged from 30 to 150. The total score of 30–70 is considered low autonomy, 70–110 as moderate autonomy, and 110–150 as high autonomy (Dempster, 1990). Dempster (1990) reported an overall internal consistency reliability of 0.95 for the DPBS. The subscale reliabilities ranged from 0.77 to 0.95 (Dempster, 1990). Overall, in the current study the DPBS is a reliable (0.77 to 0.95) and valid instrument for measuring professional autonomy among nurses. 3. The Nurses’ Professionalism Inventory (NPI): It is a comprehensive assessment tool consisting of 28 items distributed across five subscales: accountability, self-improvement, professional attitude, advancement of the nursing profession, and professional membership. Each item is rated on a 6-point Likert scale, ranging from 1 (strongly disagree) to 6 (strongly agree), with higher scores indicating a greater level of agreement with the statement. The internal consistency reliability, measured using Cronbach's alpha, ranged from 0.84 to 0.90, indicating strong internal consistency within each subscale (Ichikawa et al., 2020). The instruments used in this study were validated with the current data, the reliability analyses were conducted, yielding Cronbach alpha of 0.81 in the current study. This confirms the reliability of the instrument in the Jordanian context.
The pilot study to evaluate the clarity of the survey items, identify any potential areas of confusion, estimate the time required for completion, and gauge the participants’ overall experience with the questionnaire was done for 20 participants who were subsequently excluded from the final analysis. A few modifications were done with maintaining the conceptual meaning to ensure the effectiveness and reliability of the survey for the main study.
Ethical Considerations
The current study was conducted in compliance with all enacted regulations, including the Declaration of Helsinki, and the local regulations. The study received ethical approval from the Institutional Review Boards (IRBs) of the primary investigator's university and the participating hospitals. Study permissions were obtained from the respective hospital administrations. Participants were informed about the study's purpose, procedures, and their rights, and written informed consent was obtained from all participants.
The data collection process for the study involved several meticulous steps. After securing hospital entry approvals, the researcher approached the heads of selected departments within these hospitals. During these interactions, the study was introduced in detail, highlighting its purpose and significance. The department heads were asked for their assistance in identifying eligible participants based on the inclusion criteria of the study. Subsequently, the researcher visited the selected departments to meet potential participants. During these visits, eligible participants were approached at their convenience and were provided with a comprehensive explanation of the study. Along with the verbal explanation, they received a cover sheet detailing the study's objectives and procedures and a consent form. This process ensured that participants were fully informed about the study before deciding to participate.
Participants who expressed interest in the study were then given a survey package. They were instructed to complete the surveys at their convenience and return them to a specified box located at the office of each unit head. The data collection process spanned 2 months, from August to September 2023. During this period, the researcher made repeated visits, a total of seven times, to the departments to facilitate the distribution and collection of survey packages.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 27. Descriptive statistics (mean, standard deviation, proportion, and frequency) were used to describe the demographic characteristics of the participants, as well as the level of nursing professional autonomy and nursing professionalism. Pearson correlation analysis was used to assess the association between nursing professional autonomy and nursing professionalism. One-way analysis of variance (ANOVA) was conducted to assess the differences in mean scores of dependent variables based on independent categorical variables with more than two levels on nursing professionalism (such as job titles or education levels). Additionally, independent t-tests were employed to ascertain whether there were significant gender differences in nursing professionalism scores. Multiple linear regression analysis was used to identify the predictors of nursing professional autonomy and nursing professionalism. The significance criterion was set at p < .05.
Results
Sample Characteristics
In this study, a total of 227 questionnaires were distributed to eligible participants of Jordanian critical care nurses. Out of those, 211 questionnaires were returned, demonstrating a high response rate (93%). However, during the data cleaning process, 11 questionnaires were excluded due to incompleteness, which left a final questionnaire set of 200 for analysis. The Kolmogorov–Smirnov test was conducted to assess the normality of the data. The test statistic (D) was found to be 0.087, with a p-value of .23. Since the p-value was greater than .05, we fail to reject the null hypothesis, indicating that the data follows a normal distribution.
Table 1 provides a detailed reflection of the demographic and work-related characteristics of the participants; the participants ages ranging from 24 to 50 years, the average was 34.24 years (SD ± 6.17). Their experience levels ranging from a minimum of 2 years to a maximum of 18 years with the average of experience in CCU was 7.69 years (SD ± 3.94). Meanwhile their experience in nursing profession ranged from 2 to 20 years, with an average of 9.17 years (SD ± 4.55). Additionally, most of the participants had no previous experience in other health sectors outside Jordan (83.5%, n = 167). The majority of participants (62%, n = 124) were females, and most of them being married (57%, n = 114). The majority (80%, n = 160) were holding a Bachelor degree. Quarter of participants were working on Al-Basheer Hospital (25%, n = 50). In regards to the distribution of participants across different units, around half of them (47.5%, n = 95) worked in Medical ICU. Participants’ type of working shift highlights that 19.5% had a fixed day shift. Around one-third of the participants (35%, n = 70) said they have considered leaving their profession.
Socio-Demographic and Work-Related Characteristics of the Participants (n = 200).

n = number, % = percentage.
Research Questions Results
The Level of Perceived Nursing Professionalism Among Jordanian Critical Care Nurses
The mean scores for most items ranged between 3.79 and 4.44; indicating that nurses have a positive attitude towards their professional identity and responsibilities. Nurses strongly agreed with statements that emphasized their accountability within the nursing profession, such as being aware of their answerability as nurses (mean = 3.79) and maintaining a professional responsibility when making decisions (mean = 4.22). Moreover, nurses demonstrated commitment to self-improvement and continuous learning, as indicated by their agreement with statements related to reflective practice, research engagement, and knowledge sharing.
Notably, nurses also recognized the importance of their roles in society, with a mean score (mean = 4.03) on the item emphasizing the significance of their work to society. This finding suggests that nurses in critical care units acknowledge their contributions to healthcare and their role in upholding patient rights and dignity.
The total score for the NPI ranges between 28 and 167, with a mean score of 119 (SD ± 23.81). The total score offers an overall perspective on the perceived nursing professionalism among the study participants. For subscales, the results showed that nurses scored, on average, 32.59 (SD ± 7.77) for accountability, 34.62 (SD ± 7.24) for self-improvement, 21.46 (SD ± 4.76) for professional attitude, 17.47 (SD ± 3.99) for advancement, and 12.99 (SD ± 3.09) for professional membership (see Table 2).
Descriptive Statistics for Each Item in the NPI Scale.

The Level of Perceived Nursing Professional Autonomy Among Jordanian Critical Care Nurses
The results of the study revealed that critical care nurses, on average, displayed moderate to high levels of perceived nursing professional autonomy. The mean scores for most items of the scale fell within the range of 3.26 to 3.85, suggesting that nurses generally agreed with statements indicating a feeling of autonomy and independence in their professional roles. Some of the highest mean scores were observed for items related to nurses taking responsibility for their actions (mean = 3.26), having developed an image as independent professionals (mean = 3.44), and basing their actions on the full scope of their knowledge and abilities (mean = 3.56). These findings emphasized the nurses’ feeling of accountability, independence, and confidence in their professional roles.
However, there were a few items that received lower mean scores, indicating some challenges to perceiving professional autonomy. Notably, the item related to being constrained by bureaucratic legalities received a relatively lower score (mean = 2.38), suggesting that administrative and legal constraints may hinder nurses’ perceived autonomy. Similarly, the item regarding having too many routine tasks to exercise independent action also received a lower score (mean = 2.27), pointing to potential workload-related limitations.
The DPBS total score range from 71 to 122, with a mean score of 103.94 (SD ± 11.65). This cumulative score indicates that the total perception of professional autonomy among critical care nurses in Jordan. The results showed that nurses’ average scores are 37.89 (SD ± 6.77) for readiness, 23.49 (SD ± 3.02) for empowerment, 32.47 (SD ± 4.99) for actualization, and 9.87 (SD ± 1.42) for valuation. These subscale scores offer insights into the various facets of autonomy perception among the nurses, with readiness and actualization scoring relatively higher than empowerment and valuation (see Table 3).
Descriptive Statistics for Each Item in the DPBS Scale and its Subscales.

DPBS = Dempster Practice Behaviors Scale.
The Relationship Between Perceived Nursing Professional Autonomy and Nursing Professionalism Among Jordanian Critical Care Nurses
Table 4 shows a statistically significant positive correlation (r = .49, p < .001) between professional autonomy and professionalism. This finding indicates that as nurses perceive higher levels of professional autonomy in their practice, tend to exhibit a stronger sense of nursing professionalism. Additionally, a positive and statistically significant correlations have been found between each professionalism subscales (dimensions) and perceived nursing professional autonomy. Nurses who reported a greater sense of autonomy also tended to exhibit higher levels of accountability, self-improvement, professional attitude, advancement, and active participation in professional membership organizations (see Table 4).
The Association Between Professional Autonomy and Nursing Professionalism.
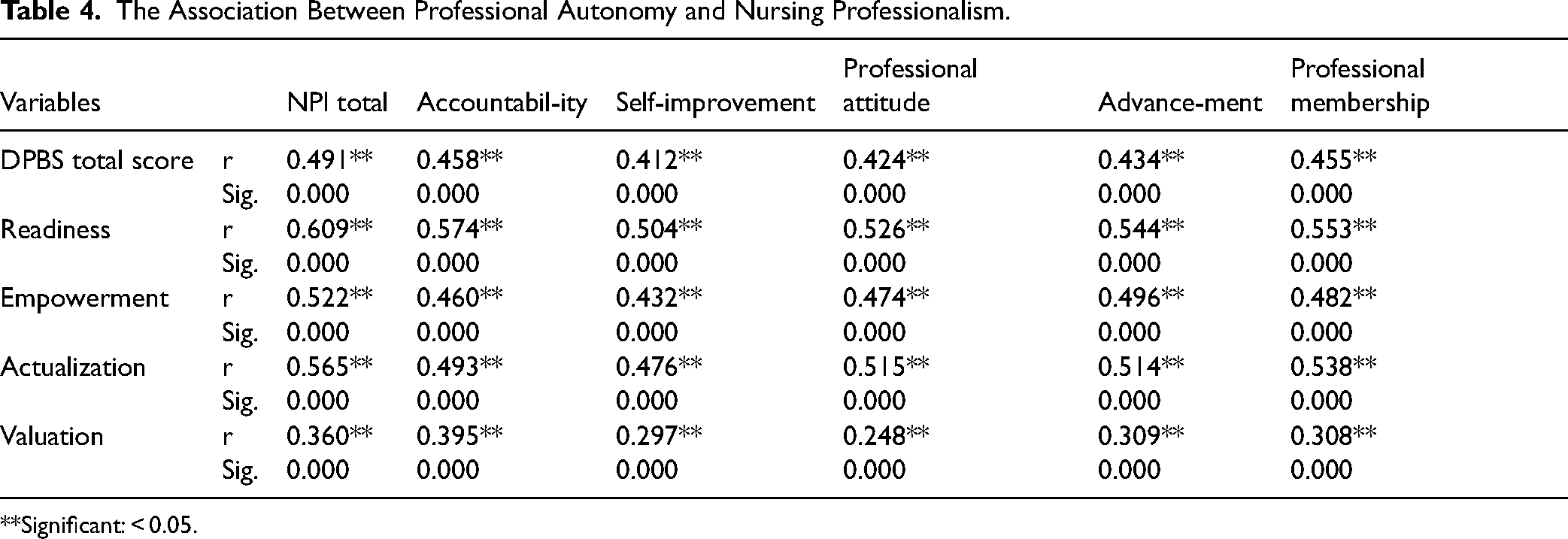
Significant: < 0.05.
The Predictors of the Perceived Levels of Nursing Professional Autonomy and Nursing Professionalism
The results reveal that the DPBS Total Score has a significant negative relationship with nursing professionalism, as evidenced by its unstandardized coefficient of −0.480 (p = .02) (Table 5). This suggests that higher scores on the DPBS Total Score, representing greater perceived nursing professional autonomy, are associated with lower scores on the NPI total score, indicating lower levels of nursing professionalism.
Predictors of Nursing Professionalism Among Jordanian Critical Care Nurses.

Among the DPBS subscales, Readiness has a strong positive relationship with nursing professionalism, with an unstandardized coefficient of 1.556 (p < .001). This suggests that nurses who report higher readiness levels, as measured by the DPBS, tend to have higher levels of nursing professionalism (p = .024). Similarly, DPBS Actualization has a positive relationship (p = .004). Valuation has a positive relationship with nursing professionalism (p = .008). These findings suggest that nurses who perceive higher levels of empowerment, actualization, and valuation in their professional roles tend to have higher levels of nursing professionalism.
The Differences in Perceived Professional Autonomy and Professionalism Levels Based on Participant's Demographic and Work-Related Variables
The findings showed that there is no statistically significant difference in perceived professionalism between based on gender (p = .88), marital status (p = .48), previous experience outside the Jordanian Ministry of Health (p = .99), previous experience in health sectors outside Jordan (p = .665) and the intention to leave the nursing profession (p = .74). However, participants lacking unrelated work experience in healthcare displayed higher levels of perceived professionalism in comparison to those who did not have (p = .04) (see Table 6).
Variations in Perceived Professionalism Level Based on Socio-Demographic Characteristics.
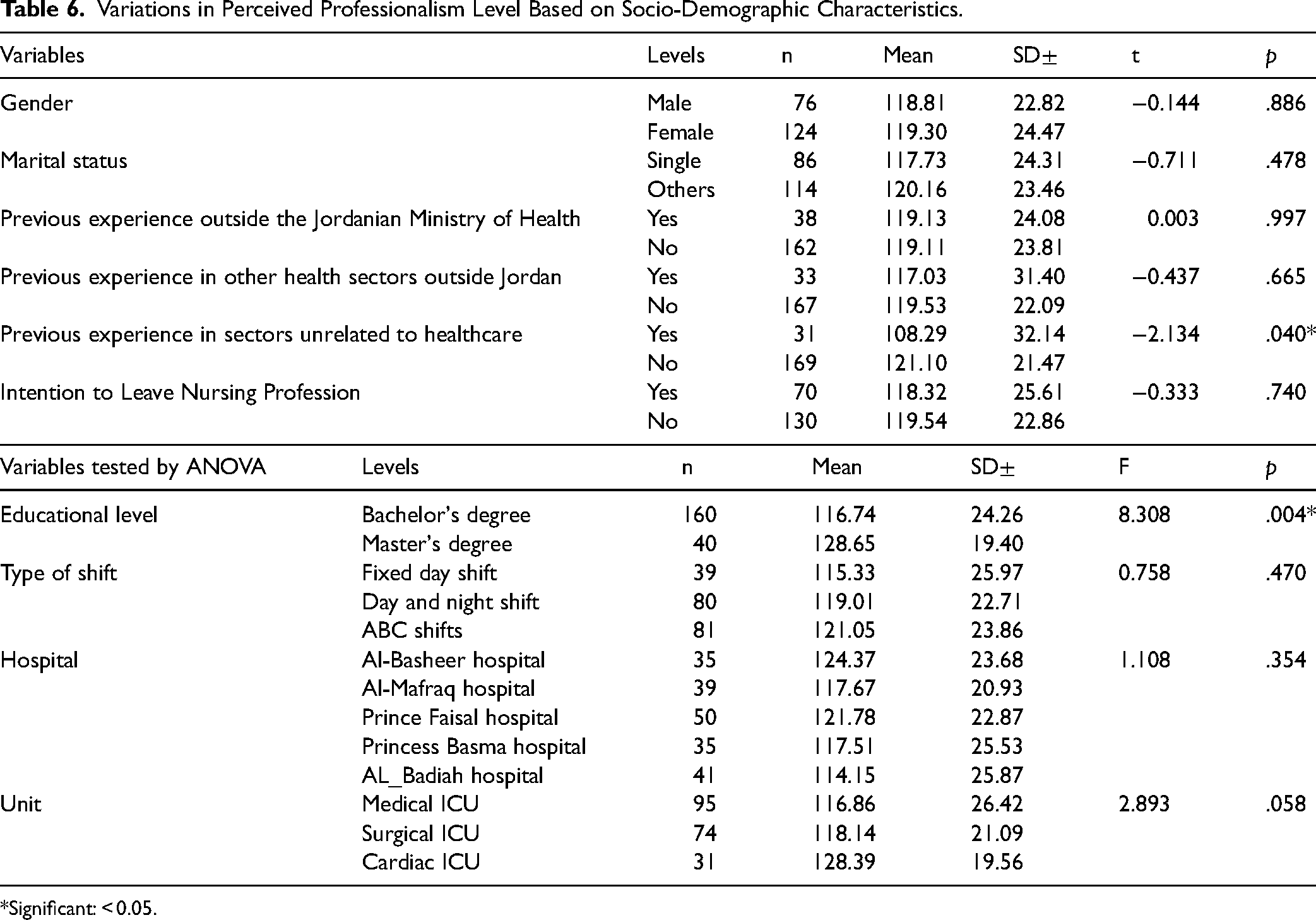
Significant: < 0.05.
A statistically significant difference in perceived professionalism levels was found across educational levels (F = 8.308, p = .004). Our findings revealed that there is no statistically significant difference in perceived professionalism levels among different shift types and different hospitals and different types of ICUs (see Table 6).
There is a statistically significant difference in perceived autonomy levels between nurses with and without previous experience in sectors unrelated to healthcare, with those without unrelated experience having higher autonomy levels (t = −2.340, p = .024) (see Table 6). The results of the one-way ANOVA (F = 4.177, p = .04) indicate that there is a statistically significant difference in perceived autonomy levels based on educational level. Specifically, nurses with a Master's Degree had significantly higher perceived autonomy compared to those with a Bachelor's Degree. But no statistically significant difference was observed for the rest of the variables (see Table 7).
Variations in Perceived Autonomy Levels Based on Socio-Demographic Characteristics/Tested by t-test and ANOVA.
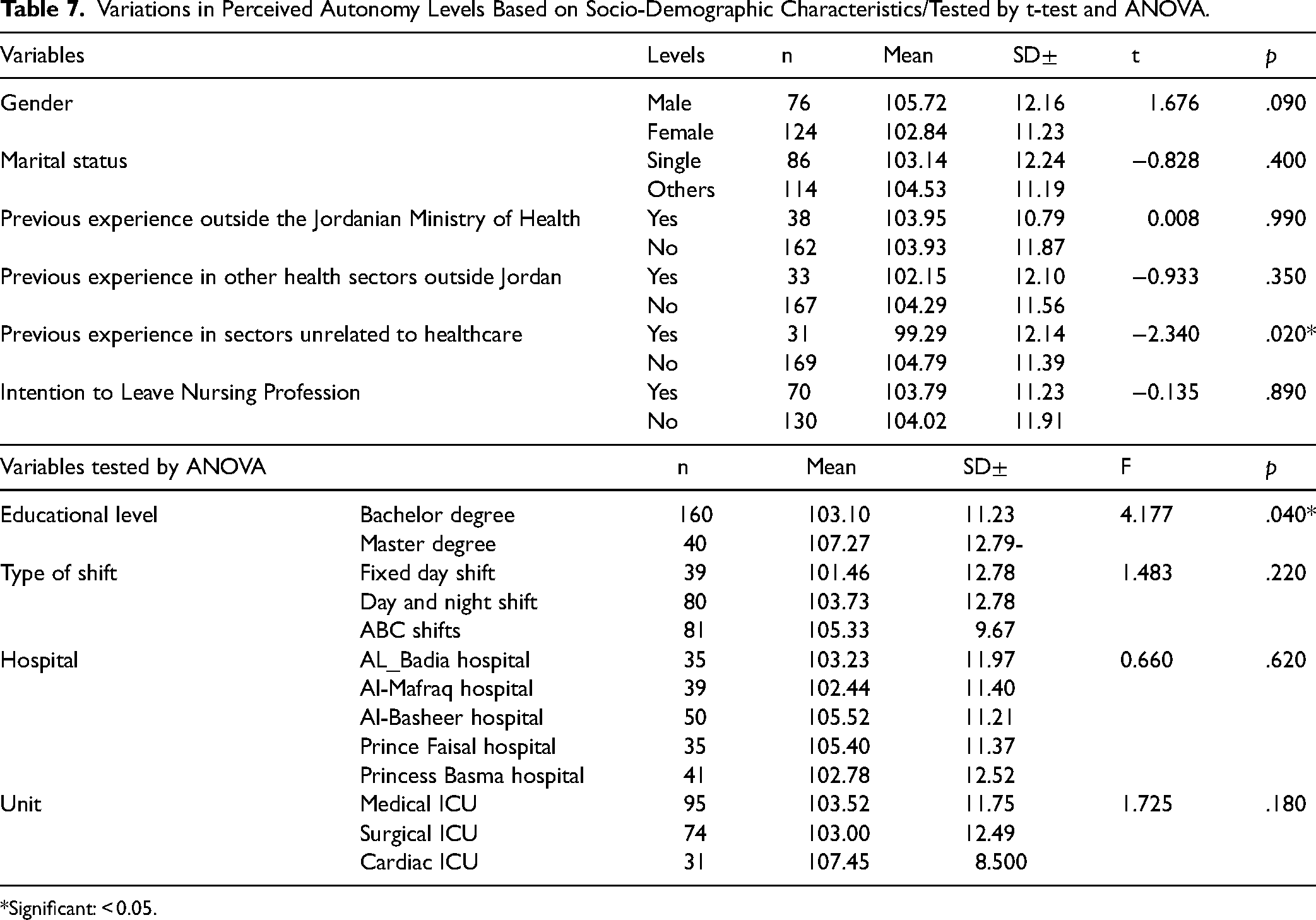
Significant: < 0.05.
Discussion
The results of the current study indicated a generally moderate to high level of perceived nursing professional autonomy among the participants, alongside a moderate perception of nursing professionalism. Notably, a significant positive correlation was found between perceived professional autonomy and nursing professionalism. However, the study revealed a complex relationship between the overall scope of professional autonomy and professionalism. While individual components of autonomy—such as readiness, empowerment, actualization, and valuation—positively predicted professionalism, higher overall autonomy scores were intriguingly associated with lower professionalism. This finding suggests that excessive autonomy without adequate support or guidelines may lead to deviations from professional standards, warranting further investigation. The findings align with and contrast existing literature in nursing practice, that is, studies by Rouhi-Balasi et al. (2020) and Oshodi et al. (2019) emphasize the crucial role of autonomy in enhancing patient care standards and applying professional knowledge. These studies mirror our results, indicating a parallel recognition of autonomy's importance across various healthcare contexts. Conversely, the moderate level of perceived professionalism among Jordanian critical care nurses presents a nuanced view when compared to international studies. Research conducted in Western contexts, such as those by Fitzgerald (2020) and Lee et al. (2019), highlights a pressing need for increased professionalism in nursing, often pointing to a gap between existing practices and ideal standards. This discrepancy may stem from cultural differences, where Western healthcare systems often emphasize individualistic practices and stringent professional standards, while Eastern contexts, including Jordan, may prioritize collective values and professional identity shaped by cultural and institutional influences. The moderate levels of perceived professional autonomy and professionalism can be attributed to several factors supported by existing research. Educational and training programs in Jordan, as discussed by Al-Dweik and Ahmad (2019) and Suliman and Aljezawi (2018), play a pivotal role in equipping nurses with the necessary skills and knowledge to exercise autonomy and professionalism. Moreover, evolving healthcare policies in Jordan have emphasize the significance of nursing roles in patient care, which may influence the perceptions of professional autonomy and professionalism (Suliman & Aljezawi, 2018). These findings have substantial implications for nursing practice and policy in Jordan. Moderate levels of perceived professional autonomy and professionalism among nurses are likely to translate into more effective patient care, as autonomous nurses are better positioned to make critical decisions and advocate for their patients.
The observed positive correlation between perceived professional autonomy and professionalism in Jordanian critical care nurses is consistent with previous studies (Labrague et al., 2019; Shohani et al., 2018). This relationship can be understood through the lens of self-determination theory (SDT). SDT (Deci & Ryan, 2000) provides a useful framework for understanding the relationship between autonomy and professionalism. According to SDT, autonomy enhances intrinsic motivation, which is essential for professional development. Pursio et al. (2021) also noted that autonomy significantly predicts nursing professionalism. Given this context, nursing education programs in Jordan should focus on fostering students’ sense of autonomy and decision-making skills, as suggested by the studies of Eid et al. (2018) and Park and Jeong (2021). Additionally, creating workplace culture that supports and values autonomy and professionalism are critical (Bakar et al., 2022). Healthcare institutions in Jordan should strive to empower nurses to exercise their judgment and make decisions, necessitating not only policy changes but also a cultural shift within healthcare settings.
The study's findings regarding the lack of significant influence of certain demographic and work-related factors on perceived autonomy and professionalism among Jordanian critical care nurses present a contrast with expectations based on existing literature. Western studies have indicated that demographic factors such as age, gender, and years of experience affect perceptions of professional autonomy and professionalism (Kim-Godwin et al., 2010; Pursio et al., 2021). However, in the current study, these factors did not indicate an influence. This discrepancy may arise from the standardized nature of nursing education and training in Jordan (Al-Dweik & Ahmad, 2019; Suliman & Aljezawi, 2018) and highlights the need for further analysis of the unique healthcare environment in Jordan.
Overall, these findings underscore the importance of cultural context in shaping perceptions of professional autonomy and professionalism and suggest avenues for further research to enhance nursing practice in Jordan.
Strengths and Limitations
The current study boasts several notable strengths, primarily in its comprehensive exploration of nursing professionalism and autonomy within the critical care context in Jordan and our findings. Additionally, the chosen instruments, DPBS and NPI, fit well within the context of Jordanian critical care nursing. Their validity and reliability in this setting support the robustness of our findings. However, the study is not without limitations. The focus on a single country's healthcare system may limit the applicability of the findings to other contexts with different cultural and institutional dynamics. Additionally, the cross-sectional nature of the study restricts the ability to capture changes over time. Furthermore, using self-reported questionnaires restricts the generalizability of the current study. In cultures with hierarchical medical structures, where physicians often hold predominant authority, nursing autonomy can be somewhat constrained. This limitation may manifest in nurses’ decisions and judgments being overshadowed by medical directives, thereby inhibiting their full professional autonomy.
Implications for Practice
The findings of this study have significant implications for nursing practice and policy in Jordan. Enhancing professional autonomy and professionalism among nurses can lead to improved patient care outcomes. Strategies such as ongoing education, supportive leadership, and policy reforms are recommended to foster these aspects. Recognizing the cultural and institutional context in Jordan is crucial in implementing these changes. At the institutional level, creating a supportive and empowering work environment is a key requirement. This involves establishing policies and practices that recognize and encourage nurse professional and autonomy. For policymakers and educators, the emphasis should be on integrating concepts of autonomy and professionalism into nursing curricula and policy frameworks. This study opens several avenues for future research. Future studies could benefit from employing qualitative methodologies, such as in-depth interviews or focus groups, to gain richer, more nuanced insights into how nurses perceive and experience professional autonomy and professionalism in their day-to-day practice. Another area for further research is the longitudinal analysis of changes in perceptions of professional autonomy and professionalism over time. The role of technology in nursing practice is another potential area for future research. With the increasing integration of technology in healthcare, studies could explore how technological advancements are impacting nursing autonomy and professionalism.
Conclusion
This study revealed moderate levels of perceived professional autonomy and professionalism among Jordanian critical care nurses, with significant positive correlations identified between these constructs. Demographic and work-related factors exhibited minimal impact, indicating that other elements might be more influential. The results emphasize the need to promote professional autonomy and professionalism to improve nursing care in Jordan. Future research should explore underlying factors and consider interventions to enhance these aspects of nursing practice.
Footnotes
Acknowledgments
We thank all participants in this study for their time and efforts. The publication fee of this article was funded by College of Nursing, Qatar University.
Author Contributions
Based on the CRediT (Contributor Roles Taxonomy) guidelines, the author contributions for the manuscript are as follows: Alaa Mefleh Al-sbehat: conceptualization, data curation, writing—original draft. Nidal Eshah: methodology, supervision, writing—review & editing. Ahmad Rayan: formal analysis, visualization, writing—review & editing. Ahmad H. Abu Raddaha: investigation, resources, writing—original draft. Omar Al Omari: validation, project administration, writing—review & editing. Fadwa Alhalaiqa: software, data curation, writing—original draft. Each author has contributed to at least two roles, with one being either writing—original draft or writing—review & editing, in accordance with the authorship criteria outlined by CRediT.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Zarqa University and the Ministry of Health Research Ethics Committees (approval no. 25/2022 and 10457 respectively) on June 15, 2023/July 2, 2023.
Funding
The authors received no financial support for the research, and authorship of this article.