
Abstract
Introduction
Inadequate nursing management of critical area alarms negatively impacts patients’ health and increases the risk of adverse outcomes. There is a lack of studies examining clinical alarm management-related knowledge and practices among Palestinian critical care nurses (CCN) in the West Bank.
Objectives
This study aimed to assess CCNs’ knowledge and practices regarding clinical alarm management and identify associated demographic factors among Palestinian CCNs in Southern West Bank hospitals.
Methods
A cross-sectional study was conducted in critical care units of governmental and non-governmental hospitals in May 2024. A total of 155 nurses were recruited through convenience sampling. Data were collected using a self-administered questionnaire consisting of three sections: socio-demographic characteristics, knowledge of clinical alarms, and practices related to clinical alarm management. Data analysis was performed using SPSS.
Results
Of the 155 nurses, 60.6% experienced a lack of alarm-related training. Only 16.1% of the participants demonstrated good knowledge and 35.5% had good practices. Nurses with Master`s degree or higher showed significantly better knowledge (p < 0.001). Younger, less-experienced, female, single nurses, who received alarm-related training, had better practices (p < 0.05).
Conclusion
The critical gaps in nurses’ knowledge and practices concerning clinical alarms demand immediate attention. Educational and training initiatives are essential for improving alarm management for enhancing patient safety.
Introduction
Clinical alarms are audible or visual signals from critical care devices to notify healthcare professionals, including critical care nurses (CCNs), that something is wrong with the patient or the patient's condition has changed (Cho et al., 2016). These include physiological cardiac monitors, mechanical ventilators, infusion pumps, syringe pumps, and oxygen saturation devices (Morton & Thurman, 2023). Alarm limits refer to the lowest and highest values, which are set based on the patient's baseline so that when the patient's values move outside of these limits, an alarm is triggered and CCNs are notified of the change in the patient's physiological condition, thus a nursing response is needed (Fujita & Choi, 2020).
Nurses must possess the necessary knowledge to appropriately customize and set devices in critical care units (CCUs), enabling them to respond effectively to alarms and enhance patient care. This knowledge helps reduce the frequency of false alarms caused by technical errors, which can result in incorrect information being transmitted or displayed on patient monitoring systems (Ruppel et al., 2018).
Nurses’ practices in monitoring clinical alarms are closely linked to their level of knowledge and various socio-demographic characteristics (Ibrahim et al., 2023; Lee et al., 2021; Meng’anyi et al., 2017). Effective alarm management requires nurses not only to recognize alarm signals but also to interpret their urgency, reset parameters based on patient conditions, and ensure appropriate interventions are taken. Evidence suggests that higher educational preparation and prior training contribute to more accurate alarm setting and faster response, thereby enhancing patient safety and reducing preventable complications (Abdelhalim et al., 2019; Liao et al., 2022). Theoretically, the study is guided by the Job Demands–Resources theory and Cognitive Load Theory that describe how frequent alarms, interruptions, and high workload create increased cognitive load on nurses and, consequently, delayed responses or inappropriate silencing of alarms. When demands for work exceed resources like suitable staffing, training, and supportive technology, nurses are more vulnerable to alarm fatigue and poor alarm management practice (Claudio et al., 2021; Zhu et al., 2025). Therefore, this study aimed to assess CCNs’ knowledge and practices regarding clinical alarm management and identify associated demographic factors among Palestinian CCNs in Southern West Bank hospitals.
Review of the Literature
The literature reveals inadequate nursing knowledge and practices regarding clinical alarms internationally. Studies conducted in China and various African countries, including Kenya, Sudan, and Egypt underscore the widespread challenges in this area (Abdelhalim et al., 2019; Ibrahim et al., 2023; Liao et al., 2022; Meng’anyi et al., 2017). Kenya's study revealed that most CCNs (81.6%) required training in clinical alarm knowledge and practices (Meng’anyi et al., 2017). Similarly, an Egyptian study showed that over three-quarters of the nurses had unsatisfactory knowledge and practice regarding clinical alarms (Abdelhalim et al., 2019). Additionally, an investigation in Sudan revealed poor nursing knowledge of ventilator alarms (Ibrahim et al., 2023).
Beyond Africa and Asia, several studies from Europe and North America have reinforced the critical importance of clinical alarm management in ensuring patient safety. For example, research conducted in Ireland demonstrated that frequent false alarms and insufficient staffing were major contributors to alarm fatigue, with more than 80% of nurses reporting occasional disabling of alarms due to excessive non-actionable alerts (Casey et al., 2018). Similarly, in the United States, investigations revealed that nearly all intensive care nurses perceived false alarms as a common occurrence, which diminished their trust in monitoring systems and increased the likelihood of inappropriate alarm silencing (Sowan et al., 2015).
Despite extensive international research on clinical alarm management, no studies have examined Palestinian CCNs’ alarm management competencies, despite unique challenges of resource-limited settings, including staffing constraints, limited access to continuous professional development, and ongoing political instability affecting healthcare delivery. A lack of adequate knowledge and practice toward true alarms that require prompt intervention may contribute to increased risks of preventable complications and negative patient outcomes.
Aim of the Study
Assess CCNs’ knowledge and practices regarding clinical alarm management, and
Examine associations between demographic characteristics and alarm management competencies among nurses working in critical care settings in the southern West Bank.
Methods
Design and Setting
The study adopted a cross-sectional, descriptive correlational design. This study was conducted in the Southern West Bank of Palestine in governmental and non-governmental hospitals, which are equipped with CCUs, including Cardiac Care Units (CCUs), Intensive Care Units, Neonatal Intensive Care Units, and Pediatric Intensive Care Units.
Population and Sampling
Nurses working in CCUs in the Southern West Bank Hospitals were the target population. The accessible population comprised nurses working in CCUs at the selected governmental and non-governmental hospitals in the southern West Bank.
The G*power analysis program version 3.0.10 was used to calculate sample size, where the alpha = 0.05, the effect size = 0.3 (moderate), and the power = 0.90, thus, the required sample size was 144 participants
The inclusion criteria encompassed all nurses currently working in CCUs and available during the data collection period, capable of providing consent to participate in the study. Nurses in managerial positions (such as head nurses and directors) were excluded due to limited patient contact, and newly hired nurses with <1 year of experience in CCUs were excluded to minimize bias related to limited clinical exposure.
Instrumentation
A structured self-reported questionnaire was used for data collection. The questionnaire comprised three main sections: socio-demographic information, knowledge of clinical alarms, and nurses’ clinical alarm practices. The first section focuses on socio-demographic characteristics and includes age, gender, level of education, marital status, hospital type, experience in CCUs, and alarm-related training. These demographic variables were selected based on evidence from prior studies showing their potential influence on nurses’ knowledge and clinical alarm practices (Abdelhalim et al., 2019; Meng’anyi et al., 2017).
The second section assesses knowledge of clinical alarms using a tool developed by (Meng’anyi et al., 2017). The research team adapted this tool after necessary approval (supplementary file), where additional items were incorporated, resulting in ten items about clinical alarms. Responses for each item were true, or false, and I am unsure. The scoring system was as follows: correct answers received a score of one, and incorrect answers received a score of zero. The knowledge scores were converted into percentage scores by dividing the respondents’ results by the potential maximum scores and multiplying them by 100. The total score of each result was calculated using Bloom's cutoff point (Bloom, 1956). Participant scores of knowledge were categorized as follows: high level (80–100%), moderate level (60–79%), and low level (< 60%).
The third section refers to nurses’ practices when monitoring clinical alarms tool originally developed by (Meng’anyi et al., 2017). The responses were on a 5-point Likert scale, ranging from 5 (always) to 1 (never) to assess the frequency of performing nine specific actions related to clinical alarms. Scores were converted into percentage scores by dividing the respondents’ results by the potential maximum scores and multiplying by 100. Each respondent's total score was then calculated using Bloom's cutoff point (Bloom, 1956). Participant scores of practices were categorized as follows: good level (80–100%), fair level (60–79%), and poor level (<6 0%).
The validity of the questionnaire was evaluated using content validity, which was assessed using the content validity index. This validity process involved asking three highly experienced research professors and experts in CCN, patient safety, and nursing education. Based on their recommendations, minor wording modifications were made, and the revised instrument was reviewed again by the same experts to confirm the adequacy of content validity. After that, a pilot study was conducted on 17 nurses working in CCUs to assess its clarity, understandability, and feasibility. Based on the feedback from the pilot participants, some adjustments were made, including reorganizing the tables for improved clarity. To avoid any potential bias or contamination, the nurses who participated in the pilot study were excluded from further involvement. The reliability of the questionnaire was then assessed using Cronbach's alpha coefficient on the final sample, which was reported to be 0.734, indicating acceptable internal consistency.
Ethical Considerations
The approval to conduct this study was obtained from the national research committee at (Palestine Ahliya University) with reference NO# (CAMS/CCNA/30/524). Participants were informed about the voluntary nature of their participation. Informed consent was obtained from the participants. To ensure privacy during data collection, the process was conducted in a comfortable and private setting. Participants were also assured that all personal information would be protected, secured, and kept confidential.
Data Collection Process
After obtaining ethical approval, meetings were scheduled with head nurses in each selected hospital unit to explain the study's purpose and request a list of the unit's participants’ characteristics and experiences. Once participants were identified, they were asked to sign informed consent and complete a structured self-reported questionnaire at a time that was convenient for them during their working shifts in designated staff rooms to ensure privacy and minimal disruption to clinical duties. The investigator remained available to clarify any questions and verified completeness of responses before collecting the forms daily. To prevent the loss of questionnaires, the researcher was present while respondents completed them and collected all responses at the end of each working day. The principal investigator oversaw the distribution and collection of the questionnaires from the selected hospitals at over a 4-week period during May 2024. The questionnaires were completed in English and assigned unique codes to facilitate tracking.
Data Analysis
SPSS software version 26.0 was used for data entry and analysis. All questionnaires were checked for completeness. The normality of continuous variables was examined using the Shapiro–Wilk test and by visual inspection of histograms and Q–Q plots to ensure assumptions for parametric tests were met. Descriptive statistics including frequency, percentage, mean, and median were utilized. Inferential statistics, including one-way ANOVA and t-test, were used to analyze the difference in mean knowledge and practice related to clinical alarm across different socio-demographic characteristics. The Pearson correlation test was used to examine the relationship between knowledge of clinical alarms and practice in monitoring clinical alarms. Data were considered significant at a p-value ≤ 0.05.
Results
A total of 477 nurses were eligible across the selected CCUs. Since no published reports were available, data on the number of CCNs in the selected hospitals were obtained by directly contacting the nursing directors. Questionnaires were distributed to 180 nurses, and 155 were completed and returned, yielding a response rate of 86.1%.
The results revealed that 56.1% were males and 43.9% were females. The average age was 29.3 years. Regarding marital status, 62% of the participants were married. Additionally, 63.2% of respondents worked in non-governmental hospitals. A total of 41.3% of the participants had more than 6 years and 62.6% held Bachelor's degrees. Concerning alarm training courses, 60.6% had not received any alarm-related training courses (Table 1).
Socio-Demographic Characteristics of Respondents (N = 155).

Results revealed that the average knowledge score among nurses was 60.6%. Also, the distribution of knowledge levels among the participants showed that 16.1%, 51.0%, and 32.9% demonstrated high, moderate, and low levels of knowledge, respectively. Moreover, the average level of practice was 71%. Analysis of the distribution of practice levels revealed that 35.5%, 44.5%, and 20.0% of the participants demonstrated good, fair, and poor practices, respectively (Table 2).
The one-way ANOVA results showed no statistically significant differences in clinical alarm knowledge based on age, marital status, and experience. Additionally, there was no statistically significant difference in knowledge based on gender, working hospital, and alarm-related training. However, the one-way ANOVA showed a significant difference in knowledge mean based on the level of education (F (2, 152) = 11.128, p < 0.001). The post-hoc test revealed that nurses with Master's degrees had significantly higher knowledge mean than those with Diplomas or Bachelor's degrees (p < 0.001). This finding suggests that higher levels of education were associated with greater knowledge and understanding of clinical alarm among CCNs (Table 3).
Clinical Alarm Knowledge and Practices Among Participants (N = 155).

Comparison of Clinical Alarm Knowledge by Selected Socio-Demographic Variables.
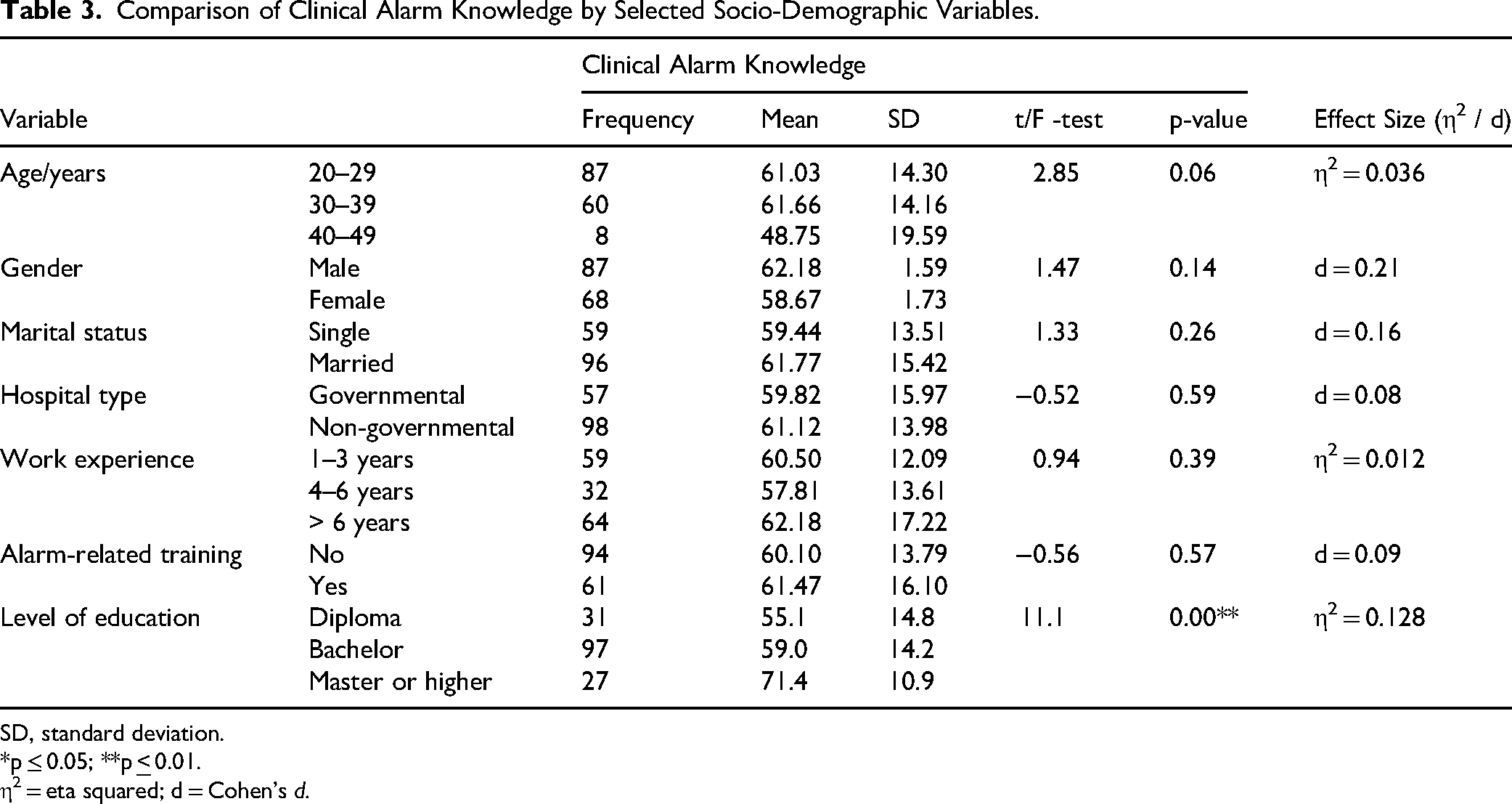
SD, standard deviation.
*p ≤ 0.05; **p
η2 = eta squared; d = Cohen's d.
Table 4 presents clinical alarm practices based on demographic factors. Concerning age, the results of one-way ANOVA revealed a significant difference in the mean practice of the participant across their age groups (F (2, 152) = 7.27, p = 0.001). Post-hoc Scheffe test indicated that nurses aged 40–49 exhibited significantly lower practice levels than those in the 20–29 age group (p = 0.002) and the 30–39 age group (p = 0.029). Regarding gender, the t-value of −2.45 indicates that the mean for males (M = 68.5, SD = 14.6) was significantly lower than for females (M = 74.2, SD = 14.0) with a p = 0.015. Therefore, females tend to have a higher mean practice score compared to males in the population. Concerning marital status, the one-way ANOVA revealed a significant difference in practice mean across their marital status (F (2, 152) = 4.19, p = 0.017). The post-hoc Scheffe test indicated that married nurses exhibited significantly lower clinical alarm practices than single nurses (p = 0.021). Therefore, single nurses tend to have higher clinical alarm practices than married.
Comparison of Clinical Alarm Practices by Selected Socio-Demographic Variables.

SD, standard deviation.
*p
η2 = eta squared; d = Cohen's d.
Concerning hospital type, the mean for nurses working in governmental hospitals (M = 66.6, SD = 14.6) was significantly lower than for nurses working in non-governmental hospitals (M = 73.7, SD = 14.0). This difference is statistically significant with a two-tailed p = 0.003. Therefore, nurses working in non-governmental hospitals had a higher mean of clinical alarm practices than governmental hospital nurses. Regarding years of experience, the one-way ANOVA revealed a significant difference in practice levels among nurses across their years of experience (F (2, 152) = 4.76, p = 0.01). The post-hoc Scheffé test revealed that nurses with 1–3 years of experience in CCUs demonstrated significantly higher practice levels compared to those with over 6 years of experience (p < 0.05). Additionally, there were no significant differences in practice levels among CCNs.
Regarding alarm training, the mean of practice among nurses who participated in alarm training programs (M = 74, SD = 14.1) was significantly higher than those who did not participate (M = 69, SD = 15.0). This difference is statistically significant with a p = 0.04. Therefore, the results suggest that participation in alarm training programs is associated with a notable improvement in the level of practice among nurses. Regarding scientific degree, the ANOVA results showed no statistically significant difference in practices based on educational levels. Also, no significant association was found between practices and knowledge regarding clinical alarms among the study participants (r = -0.037, p > 0.05).
Discussion
The present study involved 155 CCNs who were mostly young, bachelor-educated, and worked in non-government hospitals. Nurses had moderate knowledge (60.6%) and fair practice (71%), as reported in Egyptian and Kenyan studies (Abdelhalim et al., 2019; Meng’anyi et al., 2017). Higher education associated with enhanced knowledge, aligned with Ibrahim et al. (2023). Likewise, the relationships observed between practice and factors such as training, age, and gender are consistent with previous evidence presented by Liao et al. (2022) and Lee et al. (Lee et al., 2021). However, the lack of correlation between practice and knowledge is a clue towards contextual barriers such as workload, limited technology, and minimal chances for training, prevailing in resource-deprived Palestinian environments (Farajalla, 2025; Najjar et al., 2022; Qtait et al., 2025).
This study found that a low percentage of participants had good knowledge. Other previous studies found varying levels of knowledge in specific aspects of clinical alarms. For example, Liao et al. found that nurses scored highest on knowledge related to alarm signals but lowest on alarm classification (Liao et al., 2022). Similarly, Ramlaul et al. (2021) reported that 85.7% of respondents knew the purpose of clinical alarms, but only 45.1% felt confident in adjusting and monitoring these alarms. This study suggests that nurses may understand the basic principles of clinical alarms. In particular ventilator alarms, Ibrahim et al. (2023) found good ventilator alarm assessment knowledge.
In this study, it was found that nurses with a Master's or higher education level had stronger alarm knowledge. This result aligned with Ibrahim et al. (2023), highlighting the importance of promoting postgraduate education and continued professional development opportunities within clinical settings.
The current study revealed that around half of the nurses exhibited fair clinical alarm practices. This result aligns with Abdelhalim et al. (2019) who found that most healthcare professionals had unsatisfactory practice levels in managing clinical alarms. Additionally, Ibrahim et al. (2023) revealed poor management of ventilator alarms, underscoring the broader issue of inadequate alarm management practices in CCUs. The fair performance in monitoring clinical alarms suggests a basic proficiency but also indicates a need for improvement. Enhancing educational programs, increasing access to up-to-date technology, and providing targeted training on alarm management could help promote the standard of care and ensure more effective monitoring in CCUs (Lehet et al., 2023).
In the present study, scores on practice (71%) were higher compared to scores on knowledge (60.6%). Therefore, it appears that nurses can conduct routine activities for managing alarms on the basis of unit practice rather than knowledge for its own sake. There is evidence from other research studies that scores in practice were higher in comparison to scores on knowledge (Meng’anyi et al., 2017; Ramlaul et al., 2021).
There were significant differences between clinical alarm practices based on socio-demographic characteristics. This study found better clinical alarm practices among younger nurses (20–39 years). This study's findings might be interpreted as younger nurses trying to develop themselves to be enriched and updated by attending training courses to enhance their practices and skills (Lera et al., 2020). Also, young nurses could be better educated in performing practices due to the changing nursing curriculum (Lasater et al., 2021).
Furthermore, nurses with low experience (1–3 years) in CCUs performed better at managing alarms than those with more experience (> 6 years), indicating the possible impact of recent exposure to alarm events. In contrast, Liao et al. found no correlation between alarm behaviors and educational level (Liao et al., 2022). This study's finding suggests that senior nurses with more than 6 years of experience, who frequently face larger workloads or have more administrative responsibilities, may struggle to keep up with alarm management practices.
The study found that nurses who participated in alarm-related training programs demonstrated better clinical alarm practices emphasizing the importance of regular and specialized training programs. This result is consistent with Liao et al.'s (2022) findings revealed a relationship existed between clinical alarm behaviors and alarm-related training. The specialized training programs can enhance nurses’ professional values development, knowledge, skills, and practices and keep them up-to-date with new knowledge and practices (Mlambo et al., 2021; Subih et al., 2021).
Female nurses in the study were better in practice compared to their male counterparts, in accordance with Lee et al. (Lee et al., 2021). This difference may be related to variations in task engagement and adherence to safety procedures rather than inherent gender characteristics (Göktepe & Sarıköse, 2022). Female social and professional norms for being more meticulous and empathetic could help in better monitoring capabilities and appropriate responses towards alarms. When it came to the marital status, single nurses were better in practice levels compared to their married counterparts. According to Olivar (Olivar, 2025), single nurses show better commitment levels towards an organization, better adaptability, and better flexibility in terms of shift work, which could increase their concentration levels towards critical care activities. Collectively, these outcomes make it clear that factors associated with gender-related behaviors and individual life circumstances affect the performance level of nurses in handling alarms.
Additionally, it was found in this study that nurses in non-governmental hospitals performed better in alarms possibly due to differences in resources, work environment, nursing education, sufficiency of nursing staffing, and hospital policies (Ruppel et al., 2018). Also, this study had no significant relationship between educational level and alarm practices, indicating that educational level did not influence clinical alarm management practices, as evidenced in previous studies (Ibrahim et al., 2023; Liao et al., 2022; Ramlaul et al., 2021).
The knowledge-practice gap probably contributes to suboptimal practices. Emergency Care Research Institute determined failure to identify and respond to actual clinical alarms as one of the most significant issues in healthcare, ranking alert dangers as the top health technology hazards in 2012. Missed or neglected alarms remain a serious hazard to patient safety in clinical settings (Hyman, 2014; Tronstad et al., 2023), emphasizing the need for effective clinical alarm management (Lee et al., 2021).
The current study demonstrated no significant association between alarm knowledge and practices. Ibrahim et al. (2023) revealed that nurses had good ventilator alarm assessment knowledge but poor overall management of ventilator alarms. This study highlights the need for further investigation to understand the underlying factors contributing to disassociation between knowledge and practice, particularly across different alarm types. In contrast, a strong relationship was found in studies by Liao et al. (2022) and Abdelhalim et al. (2019). This variation in findings could be attributed to differences in study settings, sample characteristics, and assessment methods employed.
The results must be understood in the specific circumstances within the Palestinian healthcare system, which continue to operate under prolonged political instabilities and resource limitations (Alqaissi et al., 2025; Najjar et al., 2022). Restrictions on travel between cities and across borders further hinder CCNs’ access to international conferences, workshops, and advanced monitoring technologies (Najjar et al., 2022; Qtait et al., 2025). Limited access to international training, restricted movement for educational opportunities, and healthcare priorities focused on acute crisis management may explain the high rate of untrained nurses.
Less-experienced and younger nurses’ better performance could be the result of more recent exposure to newer monitoring systems and newer educational curricula, which are increasingly being utilized in Palestinian nursing educational institutions (Lasater et al., 2021; Mesk et al., 2025). The nurses who were employed in non-governmental hospitals also had better practice levels, perhaps because of greater resource availability, staffing sufficiency, and increased access to continuing professional development (Ruppel et al., 2018).
Hence, the strengthening of alarm-system education in undergraduate studies and in-service training is of paramount importance in the improvement of alarm response and patient safety in Palestinian CCUs.
Strength and Limitation
This study represents the first investigation in Palestine of CCNs’ knowledge and practices regarding clinical alarms, as well as the barriers they face. It addresses a significant gap in the literature by offering valuable insights into clinical alarm management, a largely unexplored area in the region. Notably, it highlights critical barriers that hinder effective responses to clinical alarms, providing a foundational basis for future research in this important field.
However, there are some limitations to consider. As a cross-sectional study, it cannot establish cause-and-effect relationships. Additionally, the use of a self-administered questionnaire restricts the depth of data collection; incorporating an observational instrument could enhance data quality. Furthermore, the study's focus is confined to nurses in CCUs in the southern West Bank, limiting its applicability to other healthcare staff and settings. Future research should aim to include a broader range of nurses across the country and various wards.
Implications for Practice
The findings of this study can assist policymakers and hospital administrators in developing comprehensive educational programs focused on clinical alarm management to enhance nurses’ knowledge and practical skills. Hospitals should implement structured annual refresher training for all CCNs. It is also crucial to provide adequate support resources, a conducive work environment, and sufficient staffing to ensure prompt responses to alarms. Integrating alarm management into undergraduate curricula and continuous professional development programs would ensure sustainable skill acquisition. In resource-limited Palestinian hospitals, cost-effective approaches, such as simulation-based workshops using existing monitors, peer-led bedside demonstrations, and online microlearning modules, are highly feasible. Furthermore, additional research should be conducted to improve alarm management in CCUs, focusing on the effectiveness of targeted training programs, the impact of staffing levels on alarm responses, and strategies to minimize false alarms.
Conclusion
This study highlights crucial gaps in knowledge and practices related to clinical alarm management among CCNs in Southern West Bank hospitals. Key findings indicated that while nurses had a moderate level of knowledge about clinical alarms, many demonstrated fair to poor practices in responding to them. Notably, higher educational attainment correlated with better knowledge levels. The study also points to demographic factors such as age, gender, marital status, and hospital type influencing alarm management practices. To enhance patient safety, the study underscores the need for focused interventions, including comprehensive training programs and strategies to address the identified barriers. By improving clinical alarm management, hospitals can foster timely and accurate responses, ultimately benefiting patient outcomes.
Footnotes
Acknowledgments
The author thanks the nurses who participated in this study.
Ethical Considerations
The approval to conduct this study was obtained from the national research committee at (Palestine Ahliya University) with reference NO# (CAMS/CCNA/30/524). Participants were informed about the voluntary nature of their participation. Informed consent was obtained from the participants. To ensure privacy during data collection, the process was conducted in a comfortable and private setting. Participants were also assured that all personal information would be protected, secured, and kept confidential.
Consent to Participate
Written informed consent was secured from all study participants.
Consent for Publication
Not applicable. This manuscript does not contain any individual person's data in any form (including individual details as name, images, or videos).
Author Contributions
FF and AB designed the study and provided the data. FF and AA conducted data analyses and prepared tables. All authors wrote the main manuscript text and AB supervised the study and provided valuable comments during the drafting of the manuscript. AA and MM edited the manuscript and provided valuable comments. All authors reviewed and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data are available from the corresponding author upon reasonable request.