
Abstract
Background
There are limited studies regarding physical activity, anxiety, and depression levels among patients with postacute myocardial infarction (AMI). This is a need for more research on physical activity, anxiety, and depression levels based on the type of AMI following hospitalization to develop interventions to improve these outcomes.
Objective
To compare physical activity behavior, anxiety, and depression levels among patients with post-ST-elevation myocardial infarction (STEMI) and post-non-ST-elevation myocardial infarction (NSTEMI) not involved in cardiac rehabilitation program following hospitalization.
Methods
A descriptive cross-sectional study design was employed with a convenience sample of 254 patients with post-AMI, 4 weeks after hospitalization. Participants, recruited from three hospitals in Jordan.
Results
The sample characteristics included the following: 140 males (54.3%), 120 married (47.2%), diagnosed with STEMI (n = 137, 53.1%) or NSTEMI (n = 117, 45.3%). And 41.3% of participants had moderate-to-severe anxiety level (General Anxiety Disorder-7 [GAD-7] > 10), while 22.0% had moderate to severe depression levels (Patient Health Questionnaire-9 [PHQ-9] > 10). Post-STEMI and post-NSTEMI participants had moderate levels of anxiety, with 14.39 (3.45) versus 13.37 (3.51); and depression levels of 12.66 (3.28) versus 12.22 (3.54), respectively. There was no significant difference in depression level between patients with post-STEMI and post-NSTEMI, but the former had statistically significant higher anxiety level than the latter. The mean self-reported exercise duration and exercise frequency of patients with post-STEMI were significantly higher than for their post-NSTEMI counterparts: 151.7 (76.33) versus 87.78 (37.62) minutes per week, and 2.92 (1.44) versus 1.97 (0.88) times per week (respectively). Furthermore, patients with post-STEMI had less mean sedentary time: 582.92 (128.92) and 641.54 (147. 27) minutes per day (p > .05) (respectively).
Conclusions
Healthcare providers have to consider the differences in physical activity behavior, anxiety, depression levels based on types of AMI when developing interventions and establishing cardiac rehabilitation program to improve physical activity behavior and reducing sedentary time.
Review of Literature
Acute myocardial infarction (AMI) is a leading cause of premature death and morbidity in the world and also a major contributor to cardiovascular diseases (CVD) and related mortality (Dani et al., 2022). In the United States there are an estimated 805,000 AMI incidents every year (approximately one every 39 s) (Virani et al., 2021). Improved post-AMI survival rates have been attributed to secondary prevention measures for patients who cannot attend cardiac rehabilitation, or as an adjunct to it (Jin et al., 2019). Cardiac rehabilitation programs support many patients to maintain moderate levels of physical activity (PA) required for improved cardiovascular health outcomes, and PA is a core element of the lifestyle management component of cardiac rehabilitation programs (Xing et al., 2020).
Randomized controlled trials demonstrate that cardiac rehabilitation programs lead to behavioral change and a significant improvement in PA levels among patients with CVD (Dibben et al., 2018). There is a strong empirical evidence in the literature concerning the numerous benefits of PA for patients with cardiac disease, including reduced cardiovascular mortality (Ekblom et al., 2018), and improved patient cardiac ejection fraction, exercise tolerance, and physical status (Zhang et al., 2018). Moreover, PA contributes to improve behavioral risk factors that may result in AMI, promotes exercise capacity, and elevates quality of life for patients with AMI (Xing et al., 2020). Any light or moderate PA can help reduce AMI fatalities (Peytz et al., 2019).
In order to improve cardiovascular health by 20% and reduce deaths from CVD and stroke by 20%, the American Heart Association identified seven key health factors and behaviors, dubbed “Life's Simple 7”: not-smoking, PA, healthy diet, body weight, control of cholesterol, blood pressure, and blood sugar (Tsao et al., 2022). In addition, the World Health Organization (WHO, 2020) international recommendations on PA and sedentary behavior is at least 150 to 300 min of moderate-intensity aerobic PA; or at least 75 to 150 min of vigorous-intensity aerobic PA; or an equivalent combination of moderate- and vigorous-intensity activity throughout the week. In addition, it is generally recommended to limit the amount of time spent being sedentary, replacing sedentary time with PA of any intensity (WHO, 2020). However, adherence to the international recommendations on PA and sedentary behavior have been disappointing. An estimated 46.6% of AMI survivors do not meet PA international recommendations 1 year after cardiac rehabilitation (Racodon et al., 2020).
Psychological symptoms such as anxiety and depression can help improve adherence to cardiac rehabilitation after AMI (Murphy et al., 2020; Rao et al., 2020). Previous studies have empirically demonstrated the positive effects of exercise-based cardiac rehabilitation on anxiety and depression with patients with AMI (Zheng et al., 2019). Allabadi et al. (2019) found that more than 50% of patients with AMI suffer from symptoms of depression, while 19.2% had severe-to-very severe anxiety. Another prospective longitudinal study revealed that baseline, 2 to 4, and 6 to 12 month prevalence rates among 911 patients with AMI were 22%, 17%, and 15% for depressive symptoms; and 43%, 28%, and 27% for anxious symptoms. Furthermore, anxiety also had a negative correlation with prognosis in patients with post-MI (Murphy et al., 2020). Many studies have shown that patients with post-MI with anxiety and depression have higher rates of hospitalization and recurrent cardiac events after acute hospitalization (Bai et al., 2021).
Depressive symptoms independently predict post-AMI complications among both men and women (AbuRuz & Al-Dweik, 2018). In addition, post-MI depression are significant risk factors for re-infarction and death (May et al., 2017). Another study examined the impact of depression on mortality post-AMI, reporting that mortality risk at 1 year of 33% in patients previously diagnosed with depression, as opposed to 26% in patients previously not diagnosed with depression; the mortality risk was 87% and 78% at 19 years after the AMI, respectively (Sundbøll et al., 2017).
Several studies have investigated psychological symptoms such as anxiety and depression and their association with PA among patients with post-AMI following hospitalization, and many researchers have investigated the determinants of PA and factors impacts on the adherence with healthy lifestyle among AMI. However, there is a gap in existing knowledge regarding whether there are differences in PA, sedentary time, anxiety, and depression levels among patients with post-ST-elevation myocardial infarction (STEMI) and their post-non-STEMI (NSTEMI) counterparts not involved in cardiac rehabilitation programs following hospitalization. Therefore, this study establishes baseline data about PA behavior, anxiety, and depression levels among post-AMI population in the Middle Eastern region. In addition, this study could help intervention developers when they need to establish cardiac rehabilitation program in order to improve PA behavior among patients with post-AMI. Therefore, the study aims to identify the differences in PA levels, sedentary time, anxiety, and depression levels among patients with post-STEMI and post-NSTEMI postdischarge.
Methods
Objective
The objective of this study is to identify the differences in PA levels, sedentary time, anxiety, and depression levels among patients with post-STEMI and post-NSTEMI not involved in a cardiac rehabilitation program 4 weeks following hospitalization in Jordan.
Research Question
Are there differences in PA levels, sedentary time, anxiety, and depression levels among patients with post-STEMI and post-NSTEMI not involved in a cardiac rehabilitation program 4 weeks following hospitalization in Jordan.
Design
The study utilized a descriptive, prospective, and cross-sectional design. The participants were recruited after 4 weeks of hospital discharge from outpatient departments (OPD) during their first-time appointments at cardiology clinics, after being diagnosed with AMI and admitted to Coronary Care Units (CCUs) in three major hospitals in Jordan.
Setting
The research was implemented at three main hospitals in Jordan, representing the major Jordanian healthcare sectors including: Jordan University Hospital, a Ministry of Health Hospital, and a private hospital. These hospitals receive patients’ referrals from other cities of Jordan, which improves the generalizability of the results and also increases the representativeness of the sample. The Jordan University Hospital is a tertiary main referral hospital with approximately more than 600 beds. It received patients from the majority of cities in Jordan based on a contractual agreement with Ministry of Health, and it also receives private patients (Jordanian Ministry of Health, 2016).
The Ministry of Health hospital studied in this article is a major part of the healthcare sector in Jordan, offering extensive health services to a large number of the Jordanian population, with 433-bed capacity (Jordanian Ministry of Health, 2016). The private hospital is considered as one of the major comprehensive and teaching hospitals in the country, with over 300 beds. There are no structured education or secondary prevention services for cardiac rehabilitation delivered in hospitals in Jordan to prepare patients with post-AMI for their subsequent self-care.
Sampling and Participants
The study employed a convenience sampling technique. G-power analysis was used to calculate the sample size (Faul et al., 2007). An α level of 0.05 and a power of 0.8 were required for a medium effect size of 0.25. Therefore, the calculation showed that 228 patients were enough number to meet objectives of the study. Moreover, an attrition rate of 10% were added, therefore the total needed sample size was 245 patients based on the calculation of power analysis. In purpose of improving clinical validity of the results, the study exceeded this number and recruited 254 patients.
The study assessed all patients who admitted to CCU after the cardiologist clinically confirmed first AMI (Virani et al., 2021). Inclusion criteria were aged ≥18 years old, patients did not involve in health intervention that aims to improve cardiovascular risk factors control, promote PA and increase compliance to health lifestyle, able to read, comprehend, and write in Arabic. Exclusion criteria were any comorbidity disease that might affect PA and patients who documented in their medical records any diagnosed with mental/ psychiatric disorders.
Data Collection Procedure
The data collection procedure was conducted in the cardiology clinics at the three studied hospitals. The involved CCU and OPD nurses were met by the principal investigator to explain the aims and methods of the study prior to collecting data. Verbal and written consent forms were provided from the patients before participating in the study in the medical wards where patients with post-AMI were transferred from CCU after being hemodynamically stable and receiving medications. The data collection procedure lasts six months, began in February and ends in August 2019.
The eligible, willing patients were asked by the principle investigator to meet them after 4 weeks during the follow-up appointments at the cardiology clinics, to complete filling out the questionnaires including: sociodemographic and clinical data sheet, the International Physical Activity Questionnaire—Short Form (IPAQ-SF), Patient Health Questionnaire-9 (PHQ-9), and General Anxiety Disorder-7 (GAD-7) Questionnaire (as described below), all of which were administered and collected from the participants on the same day in the OPD. In order to avoiding any missing response items, the collected data were checked before collecting the questionnaires from the participants, in case there was missing response items, the researcher reminded the participants if they would like to answer the not answered items. After that, the collected questionnaires were kept in locked cabinet, the principal researcher had the cabinet key only.
Ethical Consideration
Ethical approvals were obtained from involved Institutional Review Boards from involved hospitals and from Applied Science Private University (IRB. No. DRGS/2018-2019-11) in Jordan. All patients participated in the study voluntarily and provided verbal and a written consent informed. The investigation conforms with the principles and norms outlined in the Declaration of Helsinki in1995 (as revised in Edinburgh 2000) (General Assembly of the World Medical Association, 2014). The collected data were anonymous, coded, and were saved in password-protected computers. The principal investigator and co-authors can access the collected data only. All patients could take the decision to withdraw from the study without providing any reasons.
Measures
Sociodemographic and Clinical Data
Self-reported demographic data were completed by the patients, the data included their age, gender, employment status, marital status, and highest level of education. Clinical history data, including the type of AMI, body mass index (BMI), and diabetic and smoking status were obtained from patients’ medical records (with the permission of patients and hospitals).
General Anxiety Disorder-7
GAD-7 Questionnaire (Spitzer et al., 2006) was used to measure anxiety symptoms in primary care settings. The GAD-7 is used to measure the severity of generalized anxiety disorders and was also shown to be a reliable screening tool for post-traumatic stress disorder and panic, social anxiety. It is a 7-item self-report Questionnaire. The GAD-7 Questionnaire assesses how the participants have been affected by seven different symptoms of anxiety during the past 2 weeks with response options (Kroenke et al., 2010). Participants reported their anxiety level using a four-point Likert scale (0–3), ranging from 0 “Not at all” to 4 “Nearly every day.” The GAD-7 total score for seven items ranges from 0 to 21, with modified classification indicating levels of anxiety: mild (0–9), moderate (>9–15), and severe (>15). The mean score of the questionnaire items was calculated, with higher mean GAD-7 scores demonstrating patients’ greater anxiety level (Spitzer et al., 2006).
The GAD-7 Questionnaire has been found to be valid within large different populations in a primary care setting in multiple studies (Ahmad et al., 2017; Kroenke et al., 2010). GAD-7 Questionnaire has been found to be reliable by numerous studies (Dhira et al., 2021; Rutter & Brown, 2017; Spitzer et al., 2006; Villarreal-Zegarra et al., 2024), with excellent Cronbach's alpha of 0.92 (Spitzer et al., 2006). It has also been validated in psychiatric patients and patients in primary healthcare settings, and has been validated in various cultures (Delgadillo et al., 2012; García-Campayo et al., 2010; Sawaya et al., 2016). The research team used the Arabic version of GAD-7 Questionnaire, which has a good internal consistency, with a Cronbach's alpha of 0.76 (AlHadi et al., 2017).
Patient Health Questionnaire-9
The PHQ-9 is a nine-item self-report questionnaire used to assess and monitor depression severity. It was utilized as a screening tool for depressive symptom. However, is also used as a diagnostic measure of major depressive disorder (Kroenke, Löwe et al., 2010; Kroenke, Spitzer et al., 2001). PHQ-9 consists of nine items measuring depressive symptoms, corresponding to the diagnostic criteria for major depressive disorder (Kroenke et al., 2001). Participants report their depression level on four-point Likert scale (0–3), ranging from 0 “Not at all” to 3 “Nearly every day.” The PHQ-9 total score for the nine items ranges from 0 to 27. The total scores classify mild (0–9), moderate (>9–20), and severe (>20) depression.
The items on the PHQ-9 correspond to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria used to diagnose a major depressive episode (American Psychiatric Association, 2000). The PHQ-9 is shown to have high internal consistency (Cronbach's alpha between 0.86 and 0.88) (Kroenke et al., 2001) and high test–retest reliability (Chronbach's alpha between 0.84 and 0.95) (Kroenke et al., 2001). Many studies found the unidimensionality of the PHQ-9 although two-factor models were also supported (Williams et al., 2009).
The PHQ-9 found to be valid in psychiatric patients (Sun et al., 2020), patients with specific medical conditions (Molebatsi et al., 2020; Negeri et al., 2021). In addition, primary care patients and patients in general hospital settings (Molebatsi et al., 2020). It has also been translated into different languages and validated in various cultures (Martinez et al., 2023; Müller, Amberger et al., 2017; Müller, Hansen et al., 2024; Reich et al., 2018; Ukwaththage et al., 2023). The research team used the Arabic version of PHQ-9 Questionnaire, which has good internal consistency, and a Cronbach's alpha of 0.85 (AlHadi et al., 2017).
International Physical Activity Questionnaire—Short Form
The International Physical Activity Questionnaire (IPAQ) was developed in 1998 to facilitate investigation of PA based on a global standard (Craig et al., 2003). The IPAQ is the most commonly used PA questionnaire (van Poppel et al., 2010), with two versions available: the 31-item IPAQ long form (IPAQ-LF) and the nine-item IPAQ short form (IPAQ-SF).
The IPAQ-SF records the PA of four intensity levels: first, vigorous-intensity activity, second, moderate-intensity activity, third, walking, and fourth, sitting. The original authors of The IPAQ-SF recommended the “last 7 day recall” version of the IPAQ-SF for PA surveillance studies (Craig et al., 2003). The IPAQ-SF and its widely accepted high reliability, Cronbach's alpha ranged from 0.71 to 0.89 (Craig et al., 2003; van Poppel et al., 2010).
IPAQ-SF was used to determine the PA level among patients with post-AMI. It is a cost-effective method to assess PA among adult and elderly populations (Tomioka et al., 2011). The IPAQ-SF included questions about three specific types of activity undertaken in the three domains and sitting. The specific types of activity that are assessed are walking, moderate-intensity activities and vigorous intensity activities; frequency (measured in days per week) and duration (time per day) are collected separately for each specific type of activity. The vigorous intensity activities domain was not used in the study, because patients with post-AMI are advised to avoid vigorous-intensity activities during the early recovery phase. The IPAQ-SF is a commonly used, valid, and reliable questionnaire (Balboa-Castillo et al., 2023; Craig et al., 2003; Lee et al., 2011; van Poppel et al., 2010). In addition, it has been used previously among cardiac disease populations (Müller et al., 2017; Pfaeffli et al., 2013) and other populations such as respiratory diseases (Flora et al., 2023) and healthy adults (Dinger et al., 2006). The researchers used the Arabic version of the IPAQ-SF, which is a valid and reliable questionnaire, with a Cronbach's alpha ranging from 0.769 to 1.00 (Helou et al., 2018).
Data Analysis
All data were analyzed using SPSS version 22.0 (SPSS Inc., Chicago, IL). Descriptive statistics including frequency, percentage, central tendency (such as means), and dispersion measures (such as standard deviations and ranges) were used to describe data of the used questionnaires (including IPAQ-SF, GAD-7, PHQ-9, and the sociodemographic and clinical characteristics items). In addition, if there was no violation assumption found, the independent t-test was used for variables with two categories to compare continuous outcomes, such as the difference between PA level, PHQ, and GAD among patients with post-STEMI and post-NSTEMI. Data on vigorous-intensity activities was excluded from IPAQ-SF, because patients with post-AMI are not recommended to perform such exercise during the early recovery period.
Results
Sociodemographic and Clinical Data
Descriptive statistics were used to describe participants’ sociodemographic and clinical characteristics, as shown in Table 1. A total of 254 patients participated in this study, aged from 34 to 88 years, with a mean (SD) age of 58.48 (11.26) years. Just over half (55.1%) were male, and almost half (47.2%) were married. The mean (SD) BMI was 27.7 (2.21). Over half (50.8%) had diabetes and were cigarette smokers (52%). More participants were diagnosed with STEMI (n = 137, 53.1%) than non-STEMI (n = 117, 45.3%; Table 1).
Sample Characteristics: Sociodemographic and Clinical Data (N = 254 = 100%).
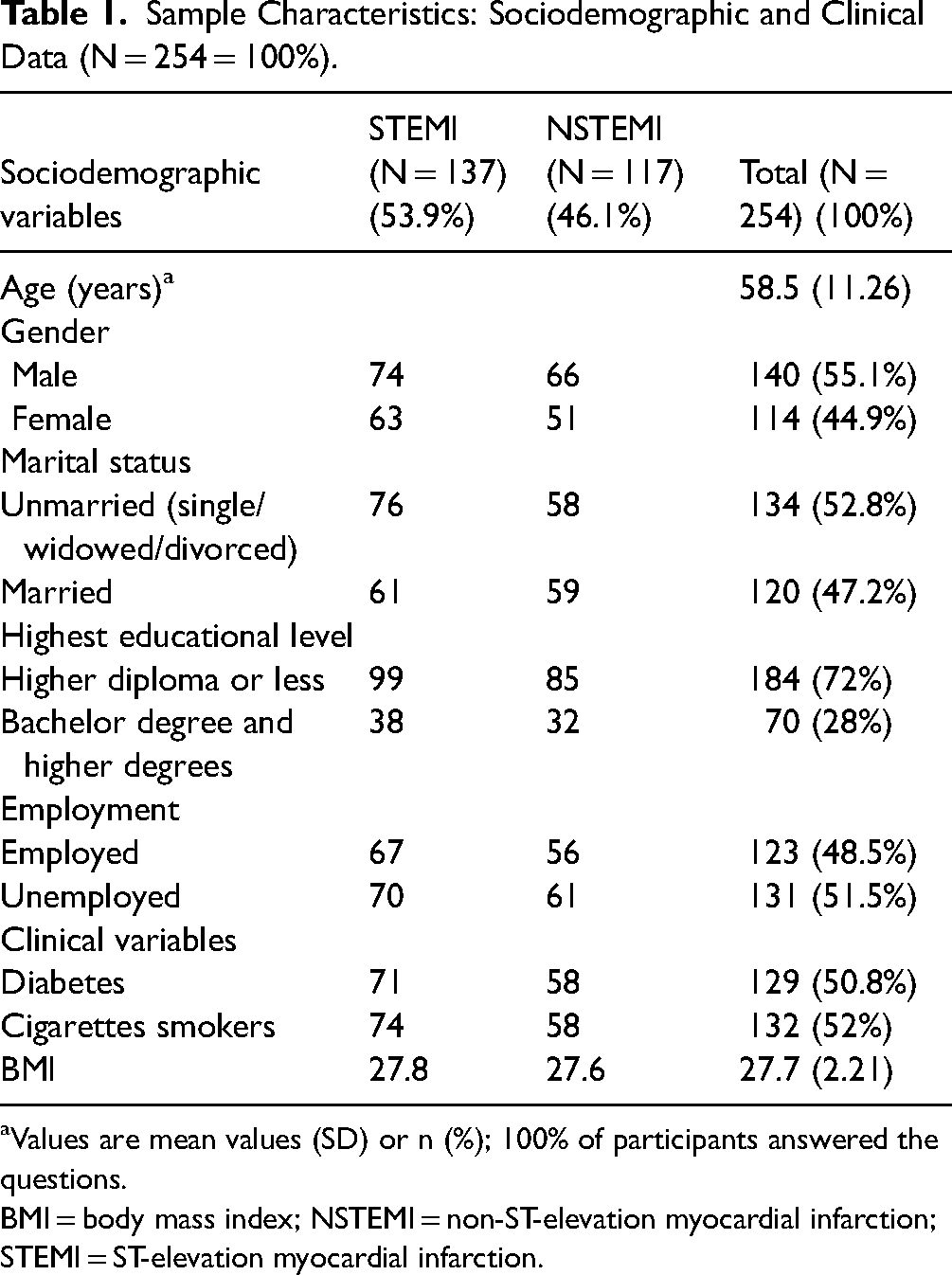
Values are mean values (SD) or n (%); 100% of participants answered the questions.
BMI = body mass index; NSTEMI = non-ST-elevation myocardial infarction; STEMI = ST-elevation myocardial infarction.
Anxiety and Depression Levels
The data analysis showed that 41.3% of patients with total post-AMI had moderate anxiety. In addition, 22.0% had moderate depression levels. In general level of anxiety and depression among patients with post-AMI were 13.92 (3.51) and 12.46 (3.4), respectively. Patients with post-STEMI and post-NSTEMI had moderate levels of anxiety (14.39 (3.45) vs. 13.37 (3.51)) and depression (12.66 (3.28) vs. 12.22 (3.54)) 4 weeks following hospitalization. However, there was no statistically significant difference in depression level between patients with post-STEMI and post-NSTEMI (p = .312). Statistically significant higher anxiety levels were reported among patients with post-STEMI than among post-NSTEMI (p = .02).
PA and Sedentary Period
The study findings showed that mean self-reported exercise duration in general for patients with total post-AMI was 122.28 (69.29) minutes per week. Statistically significant higher mean self-reported exercise duration was reported for patients with post-STEMI compared to patients with post-NSTEMI: 151.7 (76.33) versus 87.78 (37.62) minutes per week, respectively (p = .001; Table 2).
Anxiety, Depression, Exercise Duration and Frequency and Sedentary Time According to the Type of Acute Myocardial Infarction (Independent t Test).

Significant difference when p < .05; 100% of participants answered the questions.
AMI=acute myocardial infarction; NSTEMI = non-ST-elevation myocardial infarction; STEMI = ST-elevation myocardial infarction.
In general, the mean exercise frequency for patients with total post-AMI was 2.48 (1.3) times per week. Specifically, the mean of self-reported exercise frequency for patients with post-STEMI was statistically significant higher than for post-NSTEMI, with 2.92 (1.44) and 1.97 (0.88) times per week, respectively (p = .001; Table 2; Figure 1). Statistically significant higher mean self-reported sedentary time was recorded for patients with post-NSTEMI than for post-STEMI ones: 641.54 (147.27) and 582.92 (128.92) minutes per day, respectively (p = .001; Table 2).

Comparison between anxiety and depression among patients with post-AMI comparison between duration of exercise and sedentary time among patients with post-AMI. AMI=acute myocardial infarction.
Discussion
The current study explores differences in PA behavior, anxiety, and depression levels among patients with post-STEMI and post-NSTEMI not involved in cardiac rehabilitation program following hospitalization. Improving PA behavior, anxiety, and depression levels among patients with post-AMI are crucial outcomes of secondary prevention strategies (Dibben et al., 2018; Zheng et al., 2019). The study showed that there was a high level of sedentary periods per week and low PA levels in general, below the international PA recommendation guidelines, among patients with post-AMI. This result is consistent with another study which showed that patients with CVD had sedentary periods of 10.4 hours per day (Bakker et al., 2021).
Moreover, patients with post-NSTEMI were more sedentary than their post-STEMI counterparts, and had lower PA levels, affirming Charman et al. (2016) finding that patients with STEMI and NSTEMI spent more time sedentary and had low moderate-to-vigorous PA levels. Additionally, this study confirms prior investigations showing that patients with post-NSTEMI had lower PA levels and higher sedentary time (Shajrawi, Granat et al., 2021; Shajrawi, Khalil et al., 2021). The levels exhibited are below the international PA recommendation of at least 150 minute/week of moderate intensity or 75 minute/week of vigorous-intensity aerobic activity (or an equivalent combination), with muscle-strengthening activities at least 2 days/week (Virani et al., 2021).
Similarly, Matthias et al. (2018) indicated that the majority of patients with acute coronary syndrome were physically inactive, but they noted no significant differences in PA levels between patients with STEMI and NSTEMI. In the current study, the PA behavior level was congruent with the progressive increase of CVD risk factors and prevalence among the Jordan population. This may be attributed to many factors that affect PA behavior in the context of Jordanian population, such as the lack of a structured discharge education plan, and poor secondary prevention strategies in the healthcare sector (Eshah, 2013; Shajrawi, Granat et al., 2021). Moreover, there is poor knowledge regarding management of risk factors of CVD among patients with post-AMI. Therefore, serious steps to improve PA level of patients with post-AMI should be taken following hospitalization in the future.
The study showed there were moderate levels of depression, in addition to high levels of moderate to severe levels of anxiety among patients with post-AMI. There is strong evidence to supports these findings in the literature, showing that symptoms of depression and anxiety are more prevalent among cardiac patients (Allabadi et al., 2019). Moreover, the prevalence of anxiety and depression are consistent with the previous studies which shows that anxiety rates were 43% to 27% and depression rates were 22% to 15% during the first 12 months after an acute cardiac event (Murphy et al., 2020; Rao et al., 2020). In addition, a previous study revealed that increased incidence of MI is attributed to both depression and anxiety, about 52.83% and 58.49% participants suffered from anxiety and depression 2 weeks prior to their MI (Mal et al., 2019).
A recent meta-analysis study revealed that strong evidence that increased anxiety was linked with poor prognosis in patients with post-MI. In addition, the study revealed that patients with post-MI anxiety had a 23% increased risk of short-term complications and a 27% increased risk of adverse long-term prognosis compared to those without anxiety (Wen et al., 2021). The current study has added new knowledge about the differences in anxiety and depression levels based on types of AM (patients with STEMI vs. post-NSTEMI) following hospitalization.
Although there is no significant difference in depression level and significant difference in anxiety level based on the type of AMI, there is no relevant study in the literature regarding the depression level based on types of AMI to compare with. The literature showed that depression is associated with a higher risk of cardiovascular events and long-term mortality among cardiac patients (Martin-Subero et al., 2017; Takeji et al., 2021). On the other hand, these results showed that patients with post-STEMI had higher levels of anxiety level than patients with post-NSTEMI, but they have better PA levels and lower sedentary periods per week.
The study showed that patients with post-STEMI had a statistically significant higher PA duration and frequency than their post-NSTEMI counterparts, and significantly lower mean sedentary time. This may be attributed to the more aggressive treatment plan for patients with post-STEMI (Ahrens et al., 2019), and it may be a result of other psychological factors that affect patients’ health outcomes and PA, such as illness perception (Al-Smadi et al., 2017) and self-efficacy level (Shajrawi, Khalil et al., 2021). This result may demonstrate the probable impact of anxiety on PA behavior among patients with post-NSTEMI, which needs further investigation with consideration of cultural differences and other relevant contextual factors in the future.
Conclusions
Improving PA behavior, anxiety, and depression status are essential outcome for patients with post-AMI, particularly post-NSTEMI. Healthcare providers have to consider these differences in PA behavior, anxiety, and depression levels based on types of AMI to improve PA behavior and reducing sedentary time.
Strengths and Limitations
The study has many limitations: first, the short follow-up period of PA and anxiety and depression post-AMI, which can affect the implications and value of the study findings. Consequently, the study suggests that the results be considered carefully in context, especially as these findings are particularly related to the early recovery period following hospitalization. Second, using a self-reported PA questionnaire is prone to recall bias and could affect the findings. Third, absence of cardiac rehabilitation and/or cardiac disease self-management program may affect the findings of the study. Four, lack of qualitative component such as patient interviews could provide deeper insights into factors influencing, anxiety, and depression post-AMI. Finally, exploring potential mediating or moderating relationships between variables could offer a more nuanced understanding of the findings.
This study has two important strengths. First, it was conducted during the early recovery period, and it thus presents rich information regarding PA and anxiety and depression levels specific to this time, based on types of AMI. Second, the study was conducted in cardiology centers in multiple settings, which improves the clinical validity and generalizability of the findings.
The Implications of This Paper
Nursing leaders have to consider the differences in PA behavior, anxiety, and depression levels based on types of AMI when developing interventions to improve PA behavior and seek to realistically reduce sedentary time among patients with post-AMI, relative to their needs, abilities, and motivations, in a holistic and person-centered context. Healthcare policy makers need to consider screening programs for anxiety, depression, and PA levels among patients with post-AMI, in order to design appropriate interventions to encourage and improve PA behavior and establishing cardiac rehabilitation center. The integration of screening programs before providing secondary prevention services among patients with post-AMI in Jordan is strongly recommended.
Further studies to explain and interpret the mechanism that makes the differences in PA, depression, and anxiety among patients with post-AMI is warranted. Besides, studies to confirm the findings with different methodologies, such as using objective PA measurement devices (e.g., accelerometer or pedometer and heart monitoring), and adopt studies with longer follow-up period is strongly recommended.
Supplemental Material
sj-docx-1-son-10.1177_23779608241304478 - Supplemental material for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels
Supplemental material, sj-docx-1-son-10.1177_23779608241304478 for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels by Abedalmajeed Methqal Shajrawi, Hekmat Yousef Al-Akash, Ahmed Mohammad Al-Smadi, Rami Masa'deh, Mohannad Eid Aburuz, Heba Khalil, Issa Moh'd Hweidi and Ahmad Rajeh Saifan in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241304478 - Supplemental material for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels
Supplemental material, sj-docx-2-son-10.1177_23779608241304478 for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels by Abedalmajeed Methqal Shajrawi, Hekmat Yousef Al-Akash, Ahmed Mohammad Al-Smadi, Rami Masa'deh, Mohannad Eid Aburuz, Heba Khalil, Issa Moh'd Hweidi and Ahmad Rajeh Saifan in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608241304478 - Supplemental material for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels
Supplemental material, sj-docx-3-son-10.1177_23779608241304478 for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels by Abedalmajeed Methqal Shajrawi, Hekmat Yousef Al-Akash, Ahmed Mohammad Al-Smadi, Rami Masa'deh, Mohannad Eid Aburuz, Heba Khalil, Issa Moh'd Hweidi and Ahmad Rajeh Saifan in SAGE Open Nursing
Supplemental Material
sj-docx-4-son-10.1177_23779608241304478 - Supplemental material for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels
Supplemental material, sj-docx-4-son-10.1177_23779608241304478 for Postacute Myocardial Infarction Differences in Physical Activity Behavior, Anxiety, and Depression Levels by Abedalmajeed Methqal Shajrawi, Hekmat Yousef Al-Akash, Ahmed Mohammad Al-Smadi, Rami Masa'deh, Mohannad Eid Aburuz, Heba Khalil, Issa Moh'd Hweidi and Ahmad Rajeh Saifan in SAGE Open Nursing
Footnotes
Authors’ Contribution
AMS is the principal researcher and contributed to study conception and design and revising the manuscript final draft. HA was involved in writing the manuscript and revising the whole study manuscript; HK in reviewing the critical points in the research; RM in analyzing and interpreting the data; AS and MA in writing the manuscript; IH and ARS in supervising the work and revising the whole study manuscript.
Availability of Data and Materials
The data that support the findings of this study are available on request from the corresponding author.
Consent for Publication
All authors read and approved the final manuscript final draft. All listed authors meet the authorship criteria and that all authors are in agreement with the content of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval obtained from Applied Science Private University: IRB no. DRGS/2018-2019-11, Jordan University Hospital: IRB no. 2019/A-06-12; Ministry of Health Hospital: IRB no. 2019/8-16; Jordan Hospital: IRB no. 19-R10-012;All participants in the study gave their written consent to participate in the study.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.