
Abstract
Wolff-Parkinson-White (WPW) syndrome produces repolarisation electrocardiogram (ECG) changes that can both mimic and mask myocardial infarction. Concurrent presentation with both conditions can cause extreme difficulty with ECG interpretation. We present a case of a 46-year-old man, with WPW ECG and concurrent inferior ST-elevation myocardial infarction.
Introduction
Wolff-Parkinson-White (WPW) syndrome is the most common form of ventricular preexcitation. Due to alterations on ventricular intramural conduction and repolarisation, electrocardiogram changes can mimic that seen in myocardial infarction, and diagnosis in the presence of both conditions can be difficult. Differentiation of WPW patterns from actual infarction could thus prove difficult. We report an interesting case where the WPW pattern on ECG could have potentially masked the diagnosis of an acute myocardial infarction.
Case report
A 46-year-old male presented with first onset central chest pain at rest. It lasted for 30 min and was associated with mild dyspnea. The patient denied palpitation, diaphoresis, syncope and fever. He is an active cigarette smoker with a 20-pack-year smoking history. He has no past medical history or family history of sudden cardiac death or heart disease. In addition, a previous health screen and exercise stress test 4 years ago was unremarkable. He was not taking any medication or over the counter supplements.
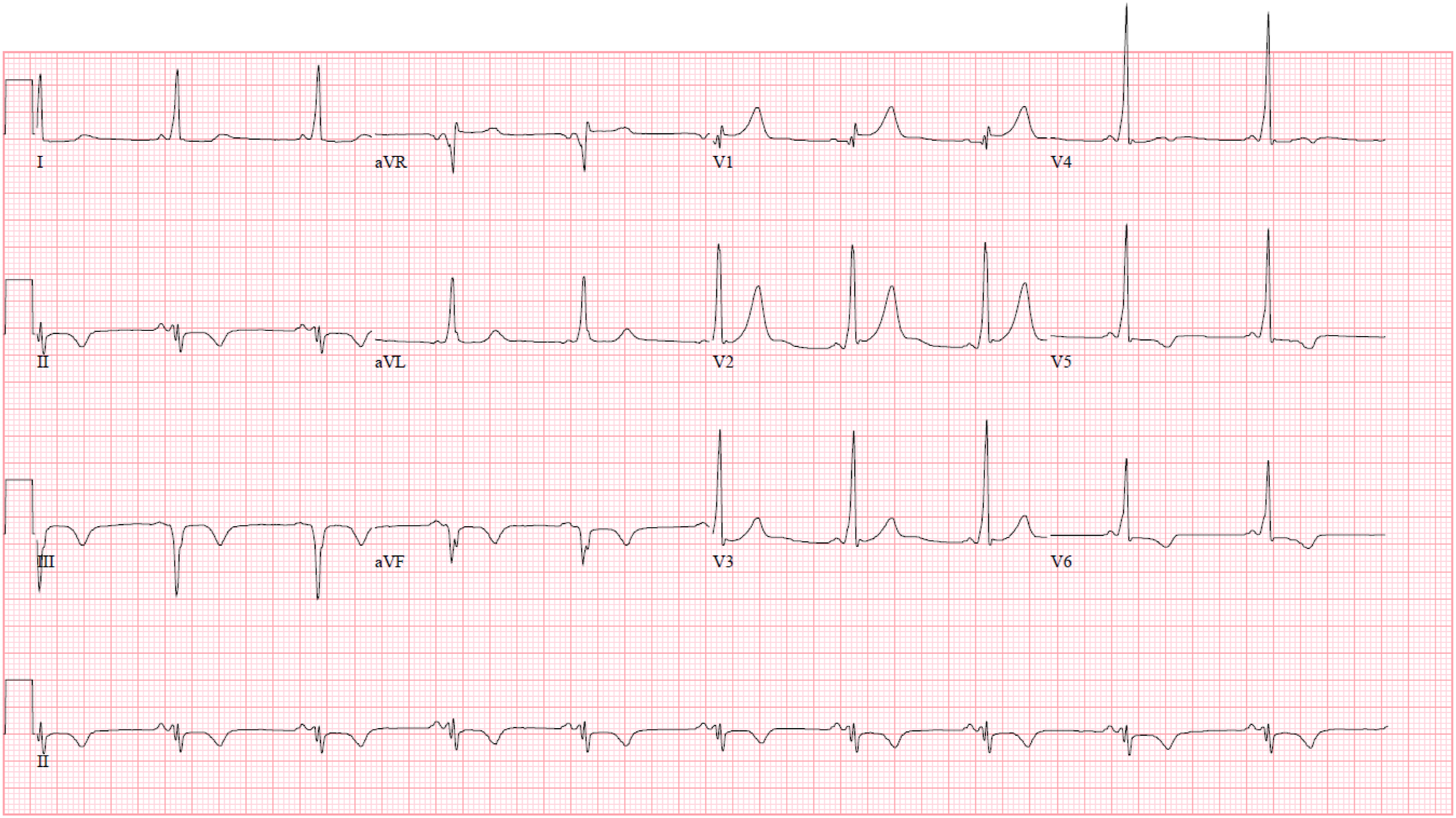
On arrival to hospital, the patient was afebrile, with blood pressure of 135/88 mmHg, heart rate of 85 beats per minute, respiratory rate of 16 per minute and oxygen saturation of 98% on room air. Physical examination was unremarkable. Cardiac auscultation revealed normal first and second heart sounds with no murmurs. Initial electrocardiogram (ECG) revealed sinus rhythm, short PR interval, delta wave, 1 mm ST elevation and biphasic T waves in V5–6 and inferior leads (Figure 1). In addition, there were 1 mm ST depressions and T inversions in lead I and aVL. Laboratory results revealed normal electrolytes, renal, liver panel and thyroid function. High-sensitive troponin I level on presentation was 45 ng/L and peaked at 8274 ng/L (normal range 0–18 ng/L). Lipid panel showed elevated LDL-C of 4.3 mmol/L, triglycerides 10 mmol/L and HDL-C 0.9 mmol/L. Chest radiography showed no consolidation or pleural effusion. His reverse-transcription polymerase chain reaction for COVID-19 was negative. Initial electrocardiogram showing sinus rhythm, short PR interval, delta wave, 1 mm ST segment elevations and biphasic T inversions in V5-6 and the II, III and aVF, 1 mm ST segment depressions in I and aVL.
Coronary angiogram showed double vessel disease with acute occlusion of the left circumflex artery (LCx) and 90% stenosis in the proximal right coronary artery (RCA) (Figure 2(a) and (b)). Primary percutaneous coronary intervention (PCI) was done with placement of a drug-eluting stent in LCx (Figure 2(c)). Staged PCI was performed to his RCA 3 days later. Transthoracic echocardiogram showed left ventricular ejection fraction of 55% with normal wall motion. Inpatient telemetry did not reveal any significant arrhythmia. A repeat ECG on day 5 of hospitalisation showed resolution of ST segment changes in the inferior leads, I and aVL (Figure 3). (a) Coronary angiogram revealing acute occlusion of the left circumflex artery. (b) There was a 90% stenosis in the proximal right coronary artery. (c) Successful re-establishment of blood flow with implantation of a drug-eluting stent in LCx. Repeat electrocardiogram was done on day 5 of hospitalization showing sinus rhythm, delta wave and resolution of ST segment changes in V5-6, II, III, aVF, I and aVL.
The electrophysiology team was consulted, and impression was that of WPW pattern ECG. The patient was subsequently discharged well on day 6 of hospitalization, and was scheduled for an outpatient exercise stress test, for further risk stratification.
Discussion
The appearance of delta wave in WPW can mimic ischemia by producing pseudo-infarct Q waves in the corresponding leads. Goldberger et al. demonstrated that concordant Q/T waves were highly suggestive of primary ischemic changes. 1 This unique pattern have been described in identifying ischemia among patients with hypertrophic cardiomyopathy, left ventricular hypertrophy and paced rhythm. 2 AMI and WPW pattern ECG may present simultaneously and represent a lethal event. 3 At times, the electrocardiographic diagnosis of myocardial infarction can only be made from normally conducted beats. In addition, presence of fragmented QRS complexes increases the specificity for infarction to 96%.4,5
Coronary artery vasospasm and Takotsubo cardiomyopathy are key differential diagnoses to consider in this case. Thus, invasive coronary angiogram remains the gold standard in evaluating coronary anatomy. Peri-myocarditis also needs to be excluded in the setting of raised troponin, wall motion abnormalities and patent coronaries. Benign repolarization ECG pattern remains largely a diagnosis of exclusion.
Depolarization abnormalities on ECG are usually associated with repolarization changes. They include bundle branch blocks, intraventricular conduction delays and pre-excitation. 6 Early repolarization ECG pattern has been previously reported as well.7,8
In our case, despite the ECG changes, the combination of angina, significant cardiovascular risk factor of smoking and elevated troponins raises the suspicion of an acute myocardial infarction. This highlights the importance of identifying the ECG subtleties in the appropriate clinical situation. Identification of concordant Q/T wave changes in WPW pattern is an important but often overlooked feature. In certain cases, serial ECG and troponin evaluation may be required to aid in the diagnosis. Once confirmed, definitive therapy such as cardiac catheterization and if required, PCI, should be performed. In our patient, coronary catheterization revealed a 100% acute occlusion of the LCx, which is the culprit vessel contributing to his symptoms and ECG abnormalities.
The patient was reported to have an unremarkable exercise stress test a few years prior to his current event. Not uncommonly, the delta wave may “manifest” intermittently. Intermittent loss of pre-excitation on ECG and abrupt loss of pre-excitation during exercise are the best predictors of low risk WPW. 9 The disappearance of delta wave during symptomatic stimulations indicates that the accessory pathway is unable to conduct in the antegrade fashion, and this puts the patient at a lower risk of tachyarrhythmia. 10 Management of asymptomatic WPW remains debatable, and, catheter directed radiofrequency ablation is of Class IIA based on the latest guidelines. 11
Conclusion
AMI is an important cause of chest pain in WPW. This case illustrates how ST segment elevation acute myocardial infarction can be masked in the presence of WPW pattern ECG. Having a high index of suspicion, along with careful and systematic interpretation of the ECG and consideration of its differentials are essential in securing an accurate diagnosis in patients with WPW pattern ECG.
Footnotes
Author contributions
SW: Drafting the manuscript, acquisition of data. SS: drafting the manuscript. JL: supervision and critical revision of manuscript. SW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.