
Abstract
Introduction
Childbirth self-efficacy has repeatedly been shown to raise satisfaction with childbirth, reduce the need for analgesic, and promote the use of different childbirth alternatives. However, the measures to improve the childbirth self-efficacy had rarely been investigated among Egyptian primiparous women.
Aim
The aim of this study is to evaluate the effectiveness of childbirth self-efficacy enhancing classes on labor length and outcomes among Egyptian primiparous women.
Methods
A quasi-experimental research approach was carried out on prospective, consecutive sample of 148 pregnant women at the end of pregnancy. A prenatal education study group (n = 74) and a control group receiving standard antenatal care (n = 74) make up the first and second groups, respectively. Between October 2021 and October 2022, the study was conducted at the antenatal clinic. The following four tools were employed to fulfill the study's objective: A structured interviewing form, a childbirth self-efficacy inventory, a follow-up checklist for monitoring maternal and neonatal outcomes during labor, and three antenatal education sessions to boost childbirth self-efficacy are all examples of tools that can be used. All statistical analyses were performed using SPSS for windows version 20.0
Results
Approximately 68.9% of women in the experimental group gave birth vaginally, compared to 29.7% of those in the control group with (p = .001), according to the study's findings. In the experimental group, regular labor took an average of 8 to 12 h, but it took more than 12 h in the control group. Birth weight (>3000g) in the experimental group compared to (2000–3000 g) in the control group, as well as the Apgar score at 1 min and 5 min, were highly statistically significance between two groups with (p = .001). The means±SD of the childbirth self-efficacy result scores were better in the study group than in control groups regarding length of delivery and vaginal delivery (248.2 ± 19.4 versus 144.6 ± 21.6 and 250.1 ± 18.2 versus 137.9 ± 21.5, respectively).
Conclusion
According to the findings of this study, antenatal education classes have a real chance of assisting primiparous women in increasing their childbirth self-efficacy and improving maternal and neonatal outcomes.
Introduction
The woman's self-efficacy for labor has a major role in her ability to use coping mechanisms during labor. A woman's personal assessment of her own abilities or confidence in her ability to handle labor and to carry out the necessary behaviours throughout labor and delivery is known as childbirth self-efficacy. The impression of pain during childbirth depends heavily on one's belief in one's capacity to handle labor. A woman's self-efficacy plays an important role in how she experiences childbirth. Women, who are more assured in their capacity to control their labor experience better labors, suffer less pain, and use analgesia less frequently (Cunqueiro et al., 2017).
Review of Literature
Self-efficacy in coping with labor refers to a woman's belief in her ability to handle labor discomfort throughout the labor and delivery stages. It has two components: first,
Self-efficacy in managing labor is the measure of a woman's belief in her ability to regulate the behaviors needed to successfully master childbirth (Yuksel & Bayrakci, 2019). The experience of giving birth is influenced by a woman's sense of her skills, not just in terms of how well she manages physically but also in terms of how she thinks and feels about this experience. Additionally, it has a significant impact on the decision of whether to give birth naturally or by a caesarean section, not only for the current pregnancy but also for following pregnancies. Also, mothers’ greater confidence and calm have been shown to positively affect children's mental health outcomes. Thus opening the possibility that higher maternal childbirth self-efficacy could strengthen children's well-being (Tilden et al., 2016).
Researchers have researched a range of strategies, including educational initiatives, to advance the physical and mental health of women. It was found conventional methods to educating expectant mothers about childbirth did not significantly enhance their psychological wellbeing or labor outcomes. In order to make the best choices about the manner of delivery, develop the skills necessary for childbirth and pain management, and prepare for motherhood, women frequently require antenatal skills based childbirth education programs (Howarth & Swain, 2019).
In study conducted by Taheri et al. (2014), mean scores of childbirth in intervention group were reduced and expectation and childbirth self-efficacy had a significant increase after intervention (P < .05). In this study, 71.4% of mothers in intervention group and 53.8% of control mothers naturally delivered their children. Most of intervention group mothers desired to deliver through cesarean and had more fear (P < .001) but lower childbirth expectation (P > .05) and self-efficacy (P < .001) than those who chose normal method.
In particular for primiparas, midwives and/or healthcare professionals should discover ways to support pregnant women's self-efficacy in managing labor pain. It is possible to reduce the need of epidural anaesthesia and encourage primiparas to participate more actively in childbirth by implementing measures to boost self-efficacy and prepare them for the management of labor pain. Programs to help women prepare for childbirth may boost their confidence in their ability to deal with labor pain (Huang et al., 2024). When uterine contraction emerges, a good sense of childbirth control can help pregnant women control pain, establish a positive psychological state and enhance their enthusiasm, participation, and intelligence in medical decision-making (Saiman et al., 2020).
Nurses can increase pregnant women's self-efficacy in a variety of ways. Research has indicated that among them, childbirth education classes have the ability to lower stress associated with the processes of pregnancy, childbirth, and parenthood in addition to improving pregnant women's self-efficacy in managing labor pain. Prenatal education is a tool for assisting future mothers in making safe decisions before and during labor, using labor pain management techniques, and using techniques for postpartum care, infant care, breastfeeding, and motherhood (Schwartz et al., 2015).
The aim of prenatal care is to ensure the health of both mother and child and a happy birthing experience. A mother and her baby could suffer long-lasting mental and physical scars if they don't receive high-quality care during childbirth, especially if it's their first labor. This could lead them to reject the treatment that is being offered. In other words, persuade her to choose cesarean section during her subsequent pregnancy or to abstain from having any more children (Cook & Loomis, 2012). Thus, the purpose of this study was test the effect of childbirth self-efficacy enhancing classes on labor outcome among Egyptian primiparous women.
Materials and Methods
Study Design
This quasi-experimental research approach was used in this study.
Study Setting
The study was performed at antenatal clinic. From Saturday through Thursday, the antenatal clinic was opened daily from 9 a.m. to 2 p.m.
Research Hypotheses
The level of childbirth self-efficacy will be higher in experimental group than in control group.
Pregnancy outcomes will be better for women and newborn in experimental group than in control group.
Sample
A prospective, consecutive sample of 148 pregnant women was recruited at the end of pregnancy, at gestational weeks 28–42. These cases were recruited from all cases admitted to antenatal clinic in the period from 1st of October 2021 to the end of to October 2022
Based on data from literature (Taheri et al., 2014), considering level of significance of 5%, and power of study of 80%, the sample size can be calculated using the following formula:


Inclusion/Exclusion Criteria
Only primiparous women were invited to participate in order to prevent the impact of a previous birth experience on their degree of self-efficacy during childbirth. Additionally, only regular and singleton pregnancies were included. The participating women accepted to provide written informed consent and could read and write.
Medical reasons for caesarean sections (prior caesarean, dystocia, fetal distress, and breech presentation), premature births or emergency caesarean deliveries, and situations in which the mother refused to participate were among the exclusion criteria. Pregnant women with mental disorders history had been excluded from this study.
Data Collection Tools
After receiving informed consent, data was gathered through in-person interviews. The following tools were employed by the researcher during the interview to gather data:
Prior to the approaching childbirth, the
Validity of Questionnaire
The researcher reviewed the local and international literature to get more knowledge about the study and also designed the study tools. Five obstetrics and gynecological nursing specialists evaluated the instruments for content validity. The recommended modifications were made, and the final form was ready for use.
Data Collection Procedure
The researcher visited the study site throughout the study period and checked the registration book to find pregnant women who fit the inclusion criteria. Each woman was individually met by the researcher, who thoroughly explained the purpose of the study to win their acceptance and their written consent. The entire set of instructions for the data collection tools was provided. The study's recruitment process began with the use of tools 1 and 2, the
A comprehensive prenatal education classes with 270 h of teaching was made available to them. There were three weekly sessions of 90 min each.
Outline for a 3-Week Antenatal Class Series.

Designed by researchers of the main manuscript: this table designed according to education classes that given to pregnant women.
The researcher returned to the labor and delivery unit after finishing the three sessions with the women in the antenatal education group and learning the date, time, and location of labor from the participants’ contacts. During labor and delivery, the researcher was present with each participant (from the antenatal education and control groups) to assess the length and result of the labor as well as the self-efficacy of the women giving birth using the CBSEI.
Institutional Review Board Approval and Informed Consent
Oral and written consent was taken from women who wanted to participate in this research. All procedures, including the human members, were in accordance with the ethical principles of the institutional and/or national research committee as well as the 1964 Helsinki Declaration and its later corrections, or tantamount moral measures. The study was affirmed by Research Ethics Committee with the ethical code Zu.Nur.REC #:0055.
Statistical Analysis
All statistical analyses were performed using SPSS for windows version 20.0 (SPSS, Chicago, IL). Continuous data were normally distributed and were expressed in mean ± standard deviation (SD). Categorical data were expressed in number and percentage. One-way analysis of variance (ANCOVA) test was used for comparison among more than two for variables with continuous data. Chi-square test was used for comparison of variables with categorical data. The reliability (internal consistency) test for the questionnaires used in the study was calculated. Statistical significance was set at p < .05.
Results
According to their demographic factors, the examined women are distributed as shown in Table 2. It demonstrates that there was a significantly different mean age between the two groups (P = .007*). Additionally, there was no noticeable difference between the secondary education levels of the 50.0% of women in the control group and the 56.8% of women in the study group. The same table showed that, with no statistically significant difference, nearly two thirds (64.9%) of the women in the experimental group were housewives, with 43.2% of them came from urban areas, compared to 35.1% in the control group.
Number and Distribution of the Demographic Characteristics of the Egyptian Primiparous Women.

Table 3 demonstrates that there was a statistically significant difference in the obstetrical histories of the two groups. Compared to one-third (31.1%) in the control group, over two-thirds of the women (63.5%) in the experimental group had three or more prenatal visits. In the experimental group, 68.9% of women gave birth vaginally compared to 29.7% of women in the control group. Compared to more than 12 h in the control group, the experimental group's average length of normal labor was 8 to 12 h. A statistically significant difference in the frequency of intra-partum problems between the study and control groups is also shown in this table (p = .001).
Number and Distribution of the Obstetric History of the Egyptian Primiparous Women.

There was a statistically significant difference between the study and control groups in terms of birth weight (>3000 g) in the experimental group compared to (2000–3000 g) in the control group, according to Table 4, which contrasts the neonatal outcomes of two groups. Additionally, this data demonstrates that there was a very statistically significant difference in Apgar scores between the study and control groups at 1 and 5 min (p = .001). Admission to the NICU was more frequent in the experimental group (2.7%) than in the control group (64.9%).
Number and Distribution of the Newborn Outcome of the Egyptian Primiparous Women.

The scores obtained by the study and control groups at the pretest and posttest for childbirth self-efficacy are shown in Figure 1 together with their respective means and standard deviations. In terms of the pretest, there were significant differences in the means of childbirth self-efficacy scores between the study's antenatal education and control groups (p = .015*). On the posttest, there were, however, very significant differences between the two groups (p = .001). These data clearly demonstrate that the study education group had higher means for childbirth self-efficacy scores.
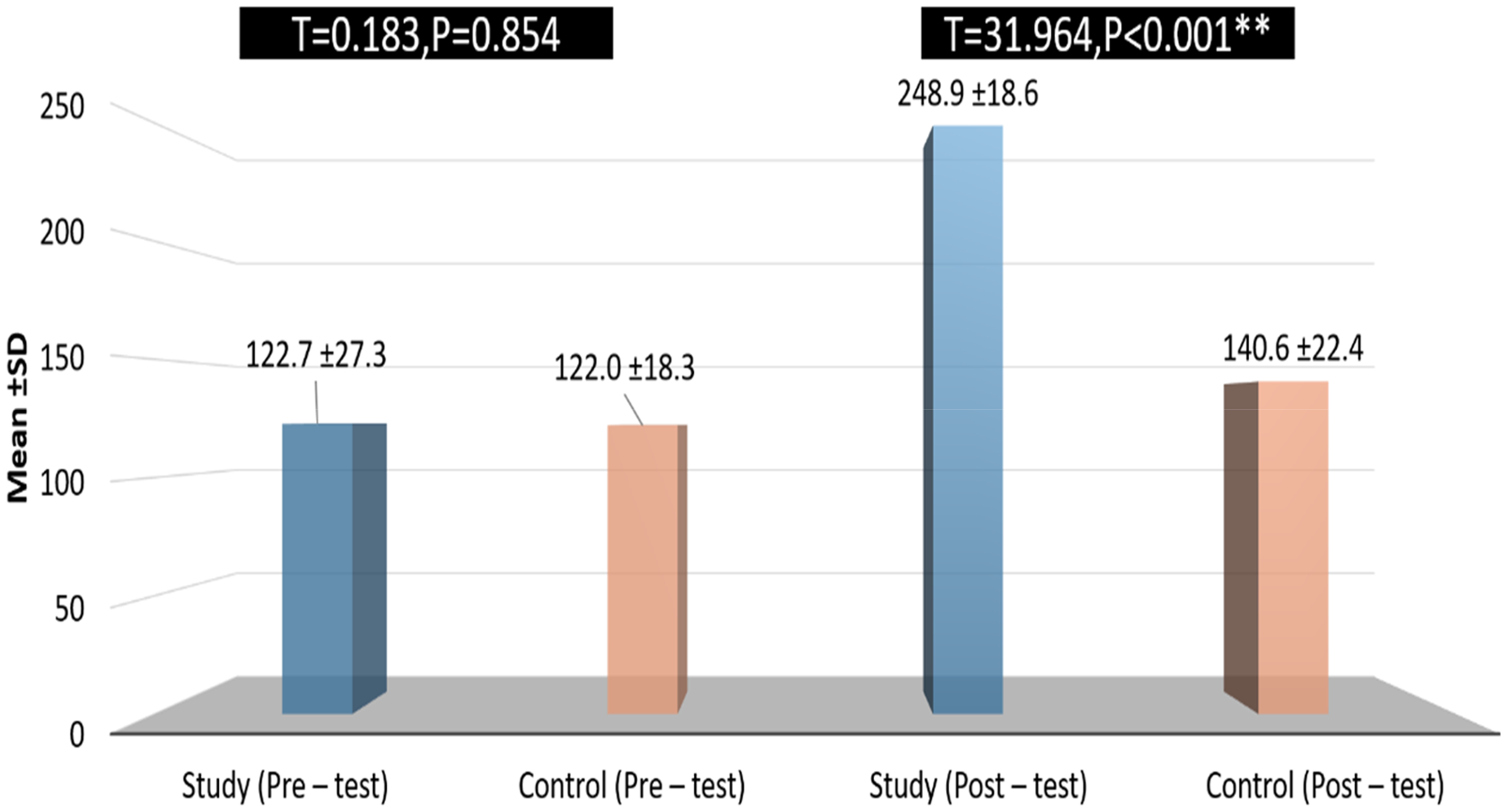
Comparison between childbirth self-efficacy scores between study and control groups.
Additionally, we performed a one-way ANCOVA analysis of variance to investigate the relationship between two factors (labor time and delivery method) and confidence in one's ability to give birth to a child (Table 5). The interaction between labor length and childbirth efficacy for the study group was statistically significant (F = 1.466, p = .038). The research group's participants had high levels of childbirth self-efficacy and had vaginal deliveries (T = 0.799, p = .047), demonstrating that there were statistically significant differences in the types of deliveries and childbirth self-efficacy.
Association Between the Obstetric History and Childbirth Self-Efficacy Domains and Scores at Post-Intervention.

Subjects were split into two groups for the purposes of Table 6, which examines the impact of childbirth self-efficacy on fetal outcomes (the study group and the control group). We subsequently made the decision to perform a one-way between-groups analysis of variance (ANOVA) and a student's t-test to compare the outcomes of the two groups of women's fetuses. A significant correlation between admission to the NICU and levels of childbirth self-efficacy was shown by the analysis of variance (p = .034). Finally, in the intervention group childbirth self-efficacy had a significant increase after childbirth self-efficacy enhancing classes than in control group (p < .001) (Table 7).
Association Between the Newborn Outcome and Childbirth Self-Efficacy Domains and Scores at Post-Intervention.

Correlation Between the Childbirth Self-Efficacy Scores of the Egyptian Primiparous Women.

Discussion
In the current study, we investigated the effectiveness of childbirth self-efficacy-enhancing classes on labor length and outcomes among 148 Egyptian primiparous women. Also, this study hypothesized that, the pregnancy outcomes would be better for women and newborn in experimental group who attending the educational classes. The study results revealed that antenatal education classes have a real chance of assisting primiparous women in increasing their childbirth self-efficacy and improving maternal and neonatal outcomes. This leads to acceptance of this hypothesis.
This quasi-experimental study looked at how antenatal education classes that increased self-efficacy affected labor duration and outcomes for Egyptian primiparous women. The study's objectives and hypotheses were fulfilled by the study's results, which showed an increase in Egyptian primiparous women's confidence in their ability to successfully carry out coping behaviours after childbirth as a result of attending antenatal education sessions. In the control group, which included 74 women, standard clinical treatment was provided. For the experimental group, which attended 3 sessions of antenatal education classes, 74 more women were recruited (Gluck et al., 2020).
In a recent randomised controlled study, Cankaya and Simsek (2021) looked into the impact of prenatal courses given to primiparous women on fear of birth, childbirth self-efficacy, depression, anxiety, stress, and mode of delivery. According to the findings of this study, a 4-week antenatal education programme given to pregnant women increased childbirth self-efficacy while decreasing birth fear, depression, anxiety, and stress both during pregnancy and postpartum. Antenatal education as well urges women to give birth vaginally.
One other study conducted by Hassanzadeh et al. (2019), between regular and irregular attenders, primiparous women's childbirth knowledge and satisfaction with childbirth h preparation classes were compared, with the findings showing that regular attendance at childbirth preparation classes is associated with higher women's knowledge, which can help primiparous women meet their learning needs, decrease maternal deaths, and improve maternal health.
According to the current study, 29.7% of women in the control group gave birth vaginally, compared to 68.9% of women in the experimental group. These results are consistent with Ricchi and colleagues’ (2020) finding that C-section rates were found to be lower among women who attended childbirth education classes than among women who did not, as well as with Gluck and colleagues’ (2020) finding that childbirth education attendees had higher rates of normal vaginal deliveries and lower rates of instrumental deliveries.
The current investigation discovered a significant difference between the study and control groups in terms of newborn outcomes, with the study group performing much better in terms of newborn admissions to the NICU and the control group had no newborns admitted to the NICU. In line with Ellis and Roberts (2020), there was a statistically significant difference between the study and control groups, with the study group having better fetal outcomes, according to studies by Ashour et al. (2021), Riley et al. (2020), and Bradford et al. (2019).
Participants in this study who attended childbirth classes experienced shorter labors on average than those who did not, which was statistically significant. Compared to more than 12 h in the control group, the experimental group's average length of usual work was 8 to 12 h. According to the researchers, having self-efficacy during labor results in decreased discomfort, worry, and tension. Compared to Duncan et al., these findings are different (2017). The severity of uterine contractions, the woman's pelvic and soft tissue structures, the size of the fetus, and other significant psychological elements like stress and anxiety may all have an impact on how long labor lasts, according to previous study.
Regarding the study groups’ average scores on the pretest and posttest measures for self-efficacy and outcome expectancy, the study showed that the mean scores of both outcome and self-efficacy expectancies did not significantly differ between the control and prenatal education groups at pretest (El-Kurdy et al., 2017). At the posttest assessment, there were very substantial differences between the two groups. Clearly, the prenatal education group had a higher mean score for both pregnancies.
This could be because women who attended antenatal education classes learned how to develop self-reliance during labor and gained practical skills that increased their self-confidence and decreased their fear throughout the childbirth process. This is in agreement with El-Kurdy et al. (2017), who studied the effect of the application of antenatal education on childbirth self-efficacy for Egyptian primiparous women in Egypt.
Strength and Limitations
One of the strengths of the study is the inclusion of women living in rural areas in addition to urban. The target population in this study was primiparous women who need more attention and had lack of knowledge regarding applying of childbirth self-efficacy measures during birth. One of the limitations of this study is small sample size and also, scares of previous study concerning the Effect of childbirth self-efficacy-enhancing classes on labor length and outcomes among Egyptian primiparous women.
Conclusions
The study's findings indicate that antenatal education classes offer a real chance for assisting primiparous women learn how to raise their level of self-efficacy during childbirth.
The study's findings showed how antenatal education sessions can enhance women's confidence in their ability to give birth, and there was a statistically significant difference between the two groups in terms of delivery method, intra-partum problems, and neonatal outcomes.
Finally, all the study results that have been presented are crucial, especially for developing nations like Egypt where antenatal education is not a part of routine antenatal care.
Implications for Clinical Practice
According to this study, women with higher self-efficacy levels engaged in more coping mechanisms throughout delivery, gave the childbirth process a higher rating, and experienced much higher levels of postpartum satisfaction. Nurses and midwives could determine which pregnant women won't give birth naturally through the vaginal canal by asking them how confident they are in their capacity to handle the traumatic experience of labor. Our work contributes to improving pregnant women's self-efficacy and coping, which helps to support efforts made by medical professionals to raise satisfaction with the delivery experience.
Recommendations
Based on the study findings, the study is recommending the following:-
Planning and implementing prenatal education programs as a crucial part of the normative antenatal care at associated public hospitals. A more satisfying delivery will result from creating and implementing childbirth education classes in the third trimester of pregnancy, especially for primigravidas, to encourage their self-control during labor. Creating and disseminating a thorough, updated booklet of childbirth education that is appropriate for and tailored to Egyptian women's culture through independent and connected Egyptian antenatal clinics.
Supplemental Material
sj-docx-1-son-10.1177_23779608241288755 - Supplemental material for Effectiveness of Childbirth Self-Efficacy Enhancing Classes on Labor Length and Outcomes among Egyptian Primiparous Women: A Quasi-Experimental Study
Supplemental material, sj-docx-1-son-10.1177_23779608241288755 for Effectiveness of Childbirth Self-Efficacy Enhancing Classes on Labor Length and Outcomes among Egyptian Primiparous Women: A Quasi-Experimental Study by Azza Ibrahim Abd El-Kader in SAGE Open Nursing
Footnotes
Acknowledgment
The author wants to thank the directors of health centers for everything they do. We want to express our gratitude to every one of our patients who took the time to respond to our inquiries.
Author's Contributions
A.I.A.E-K.; administrated education classes about dental health care for pregnant women, contributed extensively in interpretation of the data and the conclusion and she is a corresponding author. Also, she conducted the overall supervision and provided the first draft of the manuscript before its publication, participated in all the steps of research.
Ethical Considerations
The study was affirmed by the Zagazig University-Faculty of Nursing Ethical Committee with the ethical code Zu.Nur.REC#:0055.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.