
Abstract
Introduction
Nurses play a vital role in ensuring effective patient care delivery and organizational productivity. Hence, it becomes imperative to prioritize their psychological well-being and explore how its impairment may be associated with their productivity loss.
Aims
The study aims to investigate the relationship between nurses’ psychological well-being and their work productivity loss by examining how nurses self-reported their own psychological well-being and work productivity loss.
Methods
A descriptive correlational design was conducted at an Egyptian university hospital. A convenience sample of 400 nurses completed two tools: (a) Outcome Questionnaire-45 was used to assess the psychological well-being of nurses and (b) the Work Productivity and Activity Impairment – General Health Questionnaire was used to measure nurses’ work productivity.
Results
Among the 400 surveyed nurses, 66.7% reported overall poor psychological well-being. Regarding work productivity loss, 22.8% of nurses missed an average of 974.81 work hours due to absenteeism, and 62.0% lost an average of 10,630 work hours due to presenteeism. Additionally, 75.5% experienced impaired daily living activities. Approximately 13.4% of total working hours were missed due to health problems or psychological distress. Regression analysis revealed that poor psychological well-being significantly predicts work productivity loss, accounting for 2.0% of absenteeism, 11.0% of presenteeism, 17.0% of daily activity impairment, and 9.0% of overall productivity loss, with the model being significant (p < 0.01).
Conclusion
Nurses often experience poor psychological well-being and distress that hinder their daily activities and cause work productivity loss. Therefore, hospital management should prioritize improving nurses’ physical and mental health and bolstering their self-efficacy and resilience to minimize the effects of symptom distress on productivity. Investing in nurses’ well-being through managerial caring, organizational support, and fostering a supportive work environment are vital strategies for promoting quality patient care and enhancing their work productivity.
Introduction
Nurses, the largest group in the healthcare workforce, are vital to hospitals, providing continuous care and coordination with other professionals to ensure comprehensive patient support (Abou Hashish et al., 2024; Araújo-dos-Santos et al., 2018). Their productivity is crucial for patient outcomes, quality of care, and the overall functioning of healthcare facilities (WHO, 2017). However, nurses face significant challenges, including high stress, fatigue, burnout, and mental health issues, which can adversely affect their well-being, performance, and productivity (Abou Hashish & Atalla, 2023; Alsayed et al., 2022).
Recent research has shed light on the prevalence of common mental and psychological concerns among nurses, with depression, distress, and anxiety emerging as predominant concerns (Rezio et al., 2022). These concerns have been identified as the main causes of long-term work incapacity in developed countries, with projected productivity losses estimated at around US$16 trillion by 2030 (Mat et al., 2021). Another research study highlighted the significant impact of nurses’ psychological well-being on their performance and that nurses encounter various challenges, such as heavy workloads and insufficient resources, which affect nurses’ well-being and productivity (Flaubert et al., 2021). Stress, anxiety, and associated symptoms such as sadness, insomnia, and cognitive dysfunction often arise when work demands exceed workers’ adaptability, leading to substantial productivity losses (Santos et al., 2022).
Therefore, addressing nurses’ psychological well-being is paramount for maintaining their productivity and ensuring optimal patient care delivery within healthcare settings (Flaubert et al., 2021). Nevertheless, limited evidence exists on the relationship between nurses’ psychological well-being and productivity loss, particularly in the Arabian and Egyptian contexts. This study aims to bridge this gap. The findings of this study could offer empirical evidence to improve nurses’ health and work productivity through targeted interventions for those working while ill, thereby enabling them to provide quality patient care.
Literature Review
Psychological well-being is usually conceptualized as some combination of positive affective states, such as happiness and functioning with optimal effectiveness in individual and social life. For nurses, it refers to the perceptions of how the quality of nurses’ lives could affect their physical, emotional, and social functioning (Fawzy et al., 2023). It represents an optimal state of positive psychological functioning, facilitating individuals’ adaptive capacity, particularly when influenced by workplace factors (Joshanloo, 2018). To comprehensively assess nurses’ psychological well-being, the current study examined three key dimensions identified by Lambert et al. (1994); social role (SR) functioning, interpersonal relationships (IRs), and symptom distress (SD).
Social role functioning is a type of social support that represents the experience of being loved, valued, respected, and cared about by others who are present in one's life. It measures the employees’ work relations and leisure activities (Lambert et al., 1994; Matavovszky et al., 2024). Recent research has underscored the necessity of recognizing and respecting the importance of social relationships in organizational contexts to promote healthier environments. Thus, sustaining positive IRs is an additional way of evaluating nurses’ satisfaction with their relationships—particularly those with friends and family (Garmendia et al., 2023; Matavovszky et al., 2024). Symptoms distress, on the other hand, arises from various general emotional and lifestyle pressures, as well as subjective discomfort or dysfunction. This distress is an indicator of poor psychological well-being resulting from the interaction between an individual and their work environment, which the person appraises as taxing or exceeding their resources and endangering their well-being (Teo et al., 2023). In trying to answer why people stay healthy instead of getting sick, as in the case of a dominant pathogenic condition, Lambert et al. (1994) developed the Outcome Questionnaire (OQ-45)/Life Status Questionnaire (LSQ) to assess nurses’ perceptions of their psychological well-being about these three subscales and determined a cutoff point score for the questionnaire. If the participant's responses increase more than or exceed this point, it implies an increased level of psychopathology and that the participant has a high psychological distress problem (Lambert et al., 1994; Lambert et al., 2004).
Nurses face high levels of daily stress and emotional pressure, which directly impacts their health and reduces their work performance and productivity (Abou Hashish & Atalla, 2023; Dall'Ora et al., 2020). An increasing body of evidence suggests both direct and indirect impacts of psychosocial factors on nurses’ metrics such as absenteeism, sickness absence, and overall productivity loss (Li et al., 2019). However, further research studies are needed to comprehensively grasp how specific workplace and individual factors, such as the health and well-being of employees, influence nurses’ outcomes including their productivity loss (Melnyk et al., 2018).
Work productivity is the second variable in this study. For any professional group, including nurses, productivity is a key measure of professional development. Productivity reflects the ability to transform resources (input) into services and products effectively and efficiently while making the best use of the workforce and resources. Work productivity has previously been studied in terms of absenteeism, workability, and competence (Li et al., 2019; Reilly et al., 1993). However, Reilly et al. (1993) developed a specific measurement of work productivity named the Work Productivity Activity Impairment – General Health (WPAI-GH), which is a well-validated tool to measure the work productivity losses resulting from health problems. They identified four dimensions for measuring work productivity: absenteeism, presenteeism (work effectiveness), work productivity loss (altered workload), and activity impairment.
Absenteeism is a feature of productivity loss, defined as the inability to report to work, whether planned or unplanned, due to personal issues or illness for one or more expected workdays (or shifts). It is commonly used to refer to the number of missed workdays for employed people. Absenteeism can serve as a suitable criterion for assessing the health and well-being of a society's system, while also offering a valuable tool for analyzing the physical and mental health of employees and healthcare providers (Rabarison et al., 2017). Unplanned absenteeism among nurses seems to be a complex issue influenced by multiple factors and is worrisome because of its impact on the day-to-day management of human resources and associated with extra costs ultimately affecting the provision of safe care (Ticharwa et al., 2019).
The global shortage of nurses has underscored the significant impact of nurse absenteeism. In Europe, absenteeism has led to reduced patient satisfaction and substantial healthcare costs. In Africa, it contributes to job dissatisfaction, increased workloads, and nurse turnover (Mbombi et al., 2018). In Asia, factors such as poor human resource management, job stress, and burnout are major contributors to absenteeism (Elbarazi et al., 2017). In Saudi Arabia, nurses average 0.62 days of absence per month, costing about $4 million annually, with absences often linked to psychosocial factors (Al Ismail et al., 2023). Additionally, hospital absenteeism results in a yearly productivity loss of $425,749, primarily due to minor ailments and workload-related fatigue (Shdaifat et al., 2023).
Presenteeism refers to working while experiencing health issues, which leads to decreased labor intensity and productivity. Factors predicting presenteeism include depression, work stress, high job demands, and a sense of being irreplaceable (Li et al., 2019; Shan et al., 2021). This phenomenon negatively impacts the quality of nursing care, job satisfaction, and job preference, and results in both direct and indirect organizational losses (Zhang et al., 2017). Prior studies have highlighted presenteeism serves as a risk factor for subsequent absenteeism and represents the largest portion of total health-related costs. Additionally, presenteeism is associated with reduced individual health, job dissatisfaction, high job burnout, and poor work performance (Li et al., 2019; Shan et al., 2021). In North Carolina, nurses’ presenteeism is estimated to cost between $2 and $13 billion annually (Letvak et al., 2012).
Both absenteeism and presenteeism contribute to a loss of work productivity, reflecting a reduction in workload and an increase in overall work impairment (Reilly et al., 1993). Daily activity impairment measures the extent to which productivity is restricted in performing regular daily activities (Trotter, 2008).
Significance of the Study
Previous literature indicates that health-related productivity loss is influenced by absenteeism (missing work), presenteeism (working while unwell), and the inability to perform work due to illness (Yaghoubi et al., 2022). In the context of Egyptian nurses, significant findings warrant further investigation. For example, Arafa et al. (2003) reported that 21.67% of nurses exhibited moderate to severe psychological symptoms on the General Health Questionnaire. Ahmed et al. (2023) found that 84.0% of nurses experienced sickness presenteeism, with two-thirds (65.2%) having a moderate perception of presenteeism. Additionally, Ali et al. (2019) discovered that over two-thirds of staff nurses had low productivity level, and nearly one-fifth had moderate productivity level.
In other contexts, Shdaifat (2023) reported a productivity loss of USD 605,283 due to presenteeism among nurses. Yaghoubi et al. (2022) conducted a systematic review showing that presenteeism led to productivity losses ranging from USD 2,000 to USD 15,541 per healthcare employee annually. The review also found that absenteeism costs exceeded presenteeism costs, with figures of USD 463 and USD 340 per person, respectively. Silva-Costa et al. (2020) found that 10.17% of nurses had compromised overall productivity, with a 32.8% prevalence of presenteeism. Older studies, such as Letvak et al. (2012), highlighted that presenteeism often leads to increased patient falls and medication errors, diminishing service quality, with annual per capita economic losses ranging from USD 1,346 to USD 9,000.
Hence, it becomes crucial to investigate and address the health issues contributing to presenteeism, absenteeism, and activity impairment to enhance organizational productivity (Li et al., 2019). Psychology research further emphasizes that employees with mental health concerns often result in financial costs for organizations, including expenses related to medical services and lost productivity (Reilly et al., 1993). Melnyk et al. (2018) highlighted that workplace challenges faced by nurses have significant implications for their health and overall well-being, ultimately affecting their professional performance and the quality of care provided to patients. Consequently, there is increasing attention on nurses’ psychological well-being and the potential negative outcomes of psychosocial risks at work.
Despite increased attention, few studies have comprehensively examined the combined impact of nurses’ psychological well-being and work productivity. Existing literature highlights the adverse effects of workplace stress on nurses’ psychological health, including burnout, compassion fatigue, trauma, depression, and anxiety (Abou Hashish & Atalla, 2023; Juvé-Udina et al., 2020). Li et al. (2019, 2022) found that presenteeism increases fatigue, leading to job burnout, and productivity loss. Roelen et al. (2014) assessed sickness absence as an indicator of productivity, while Letvak et al. (2012) explored presenteeism's impact on quality of care and costs. Research shows a strong correlation between job burnout, fatigue, sickness presenteeism, and productivity loss (Aboagye et al., 2019; Ferreira et al., 2019; Zhang et al., 2020).
To the researchers’ knowledge, no prior investigation has explored the direct relationship between nurses’ productivity loss and their psychological well-being in the Egyptian context. Understanding how nurses self-report their psychological well-being and productivity loss could inform strategies to enhance their productivity. This study might help hospital management recognize the importance of nurses’ psychological well-being and identify variables associated with work productivity, enabling the development of interventions to promote nurses’ well-being and enhance their productivity.
Developed Conceptual Framework
Based on the previous conceptualization of the study variables, we developed the following framework (Figure 1) and a related hypothesis to validate whether outcome measures of psychological well-being could be related to nurses’ work productivity loss among nurses. This study attempts to examine this assumption by correlating the OQ scores of psychological well-being with measures of work productivity loss using the WPAI-GH.

Conceptual framework illustrating the potential relationships between nurses’ psychological well-being and work productivity loss.
Thereupon, we hypothesized that:
Hypothesis 1(H1): Impairment in nurses’ psychological well-being is associated with a loss in their work productivity.
Aim of the Study
The study aims to investigate the relationship between nurses’ psychological well-being and their work productivity loss by examining how nurses self-reported their own psychological well-being and work productivity loss.
Methods
Research Design, Setting, and Sampling
A descriptive-correlational study was conducted in all inpatient medical care units, surgical care units, and critical care units at Alexandria Main University Hospital. The STROBE cross-sectional reporting guideline was followed. The target population consisted of 600 nurses employed in the hospital, who were potential respondents of the questionnaire. Eligible participants were registered nurses with at least one year of work experience, willing to participate. Exclusion criteria included newly hired and student nurses, individuals with severe mental illness or taking psychotropic drugs, and nurses on leave during the investigation who declined to participate. Consequently, the final potential population size was 462. The sample size was determined using the Raosoft sample size calculator, resulting in a minimum recommended sample size of 210, with a margin error of 5, a 95% confidence interval, and a significance level of p-value ≤0.05. The researchers aimed to include all eligible and willing nurses to achieve the required sample size; therefore, they distributed a total of 462 questionnaires. Ultimately, a convenience sample of 400 nurses completed and returned the final questionnaires, resulting in a response rate of 86.6%.
Data Collection Instruments
Data were collected using two primary tools:
1. The OQ-45 / LSQ was developed by Lambert et al. (1994) and adopted by the current researchers. It is a validated, 45-item questionnaire that assesses nurses’ perceptions of their psychological well-being to three subscales, namely: SR-9 functioning items, IR-11 items, and SD-25 items. The responses were measured on a 5-point Likert scale and ranged from never (0) to almost always (4). The responses to the negatively worded items have been reverse coded, and scores on the overall scale were tallied. The overall score ranges from 0 to 180; the higher scores represent increasing levels of psychopathology. The cutoff point score for the total subscales score was 63, where a score of 63 or more implied a participant has a high psychological or distressing problem. The cutoff scores for the subscales are 12 for SR, 15 for IR, and 36 for SD.
The OQ-45 is a valuable outcome measure that has become one of the most frequently used by practitioners in the USA to measure clinical outcomes. It has also been translated into several languages, including Japanese, Korean, Italian, French, Portuguese, German, and Dutch (de Jong et al., 2007; Lambert et al., 1994; Lambert et al., 2004). The Cronbach's alpha (α total) for the 45-item full scale in our sample is 0.90, demonstrating a high level of internal consistency. For the SD subscale, the Cronbach's alpha is 0.88, while the IR subscale has an alpha of 0.76, and the SR subscale has an alpha of 0.73. These results are comparable to the original questionnaire developed by Lambert et al. (2004), where αSD was 0.91, αIR was 0.74, and αSR was 0.71. This result indicates that our reliability value of the scale aligns well with the original measures, confirming its robustness and suitability for our study.
2. Work Productivity and Activity Impairment – General Health questionnaire, developed by Reilly et al. (1993), has been adopted by the current researchers to measure how nurses self-report their work productivity loss. The WPAI-GH consists of six questions asked about Q1: current employment; Q2: hours missed due to health problems; Q3: hours missed due to other reasons, Q4: hours actually worked; Q5: the degree to which health affected productivity while working; and Q6: the degree to which health affected productivity in regular unpaid activities. The recall period for questions 2–6 reflected the previous seven days immediately before data collection for each participant. Responses to questions 5 and 6 were measured using a Likert scale ranging from “no effect on work” (0) to “completely prevented from working” (10). Four main outcomes or dimensions were generated from the WPAI-GH and expressed in percentages by multiplying the following score by 100 for all participants. The scores of the tool were expressed in impairment percentages, with higher scores reflecting decreased productivity. This calculation was done against the total work hours per week. For instance, a presenteeism score of 50% suggests that 50% of the time spent at work is impaired.
-Obtaining a score for each scale involves a series of formulas. Four outcomes were derived, as follows:
Absenteeism (work time missed due to health problems—the number of days missed from the workplace in the last 7 days) = Q2/ (Q2 + Q4). Presenteeism (percentage of impairment while working due to health problems—working when sick or not feeling well) = Q5/10. Overall Work Productivity Loss (absenteeism + presenteeism) = Q2/ (Q2 + Q4) + ((1 - Q2/ (Q2 + Q4)) × (Q5/10)). Activity impairment (other than work—work missed due to health problems) = Q6/10.
For identifying nurses’ responses to the six questions of the WPAI-GH (see Supplementary File 1 for Tables A1–A6).
To identify the percentage of missed hours from total nurses’ working hours, the total hours that should have been worked by nurses during the studied week were first calculated by multiplying the mean of working hours for all nurses by the total number of nurses (42.07* 400 = 16,828) (Reilly et al., 1993) (see Supplementary File 1 for Table A4).
In addition to the tools mentioned above, the participants’ demographic and professional information included their age, gender, educational level, working unit, years of experience, and the shift they worked during the week before the data collection.
Validity and Reliability
The English instruments were translated into Arabic to align with the cultural and educational context of nurses in Egypt and the Arab context. Subsequently, bilingual experts translated them back into English. The authors and a panel of expert members reviewed the backtranslations to ensure accuracy. Following deliberation and resolution of any discrepancies, a consensus was reached among the authors and experts on the final versions in both Arabic and English. Face and content validity were evaluated by a panel of five experts, which included a nurse researcher, a manager, and three academic members. Each expert was individually provided with the questionnaires to assess their face validity, content validity, and fluency. They were instructed to evaluate the instrument's item relevance, comprehensiveness, and clarity. All experts unanimously agreed that none of the items were difficult to comprehend. While some items required minor modifications or revisions, none were eliminated.
To better align with the Egyptian cultural context among nurses, a few statements in the OQ-45 tool were rephrased. For example, “I use alcohol or a drug to get going in the morning” was modified to “I use stimulant beverages such as coffee or drugs to get going in the morning.” The Content Validity Index was calculated at 0.82, indicating a good level of agreement among the experts (Polit & Yang, 2016). In addition, a pilot study involving 40 nurses was conducted to gather feedback and ideas regarding the questionnaire. However, no changes were deemed necessary based on the participants’ input, resulting in the finalization of the tool. Furthermore, the internal consistency of the OQ-45 and WPAI-GH scales was assessed during the pilot study using Cronbach's alpha. The results indicated high reliability for both tools, with coefficient values of 0.90 and 0.88, respectively.
Data Collection
Following approval from the hospital's administration and before data collection, written informed consent to participate in the study was obtained, and participants were informed of the study's purposes and their ethical rights. The researchers distributed the Arabic questionnaires in paper form to nurses who agreed to participate in the study, along with its instructions. Participants were asked to give their responses to the previous week's status to complete the questionnaire after receiving it. Each questionnaire form was assigned a code number to facilitate tracking and completion in case of missing data. The researchers agreed with nurses for one week to fill out the questionnaires and then visited the units to collect the completed ones, which were often left with the unit nurse manager. Questionnaire data were collected over four months (from March 2022 through the end of June 2022).
Data Analysis
The collected data were revised, coded, and entered into the statistical software program SPSS, version 24. Data were cleaned for any missing data before analysis. The mean score and standard deviation were used to describe the scaled data, while the frequencies and percentages were used to describe the categorical data. Cronbach's alpha reliability coefficient was used to measure the internal consistency of the tools. A Linear Mixed Model was used to test the correlation between latent variables (psychological well-being) and each of the outcome variables (work productivity). All statistical analyses were done using 2-tailed tests and an α-error of p-value ≤0.05.
Ethical Considerations
The study was approved by the Ethical Committee of the Faculty of Nursing, Alexandria University (IRB00013322-February 2022). Following approval from the hospital's administration and before embarking on data collection, written informed consent was obtained from participants after explaining the aim of the study and assuring confidentiality of the obtained data, securing anonymity, and respecting privacy. Participants were informed that they could opt out of the study at any time.
Results
Participants’ Characteristics
Table 1 showed the highest percentage of nurses (45.0%) were in the age group of 20 to less than 30 years old, and 33.8% were between 30 and less than 40 years old, with a mean age of 33.05 years and a standard deviation of 8.66. About 98.0% of nurses were female, and 66.5% were married. About 61.8% of nurses had a diploma from secondary technical nursing schools, and 22.5% had a bachelor's degree in nursing science. Additionally, 23.0% of nurses had more than 20 years of experience, and 22.5% had between 5 and less than 10 years of experience. Furthermore, 81.5% of nurses had varying shift assignments.
Nurses’ Demographic and Professional Characteristics (N = 400).
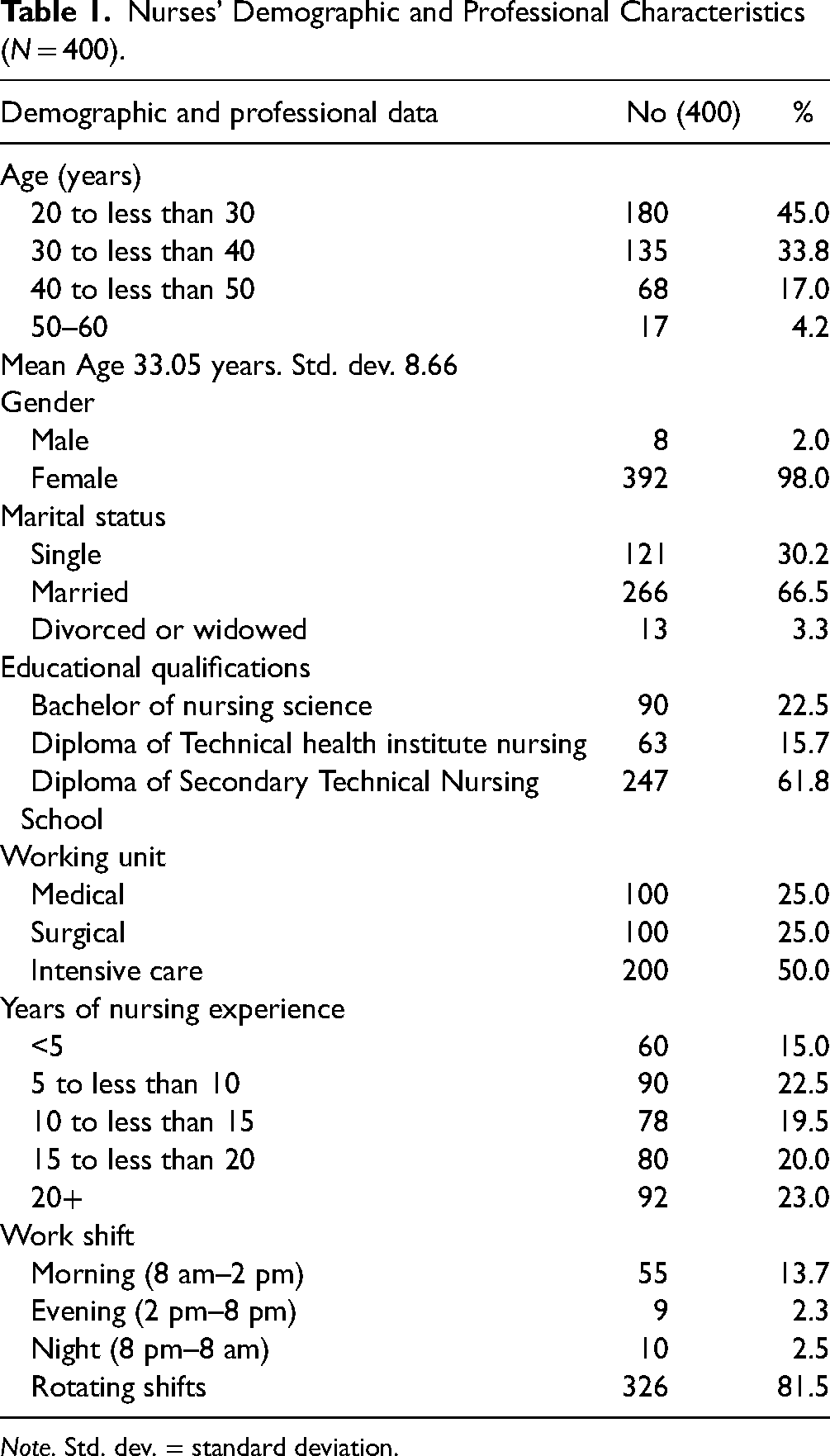
Note. Std. dev. = standard deviation.
Nurses’ Psychological Well-Being
Based on the analysis, the results showed that 66.7% of nurses had an overall poor psychological well-being, especially those who had a score of 63 or more with a mean of 71.82 (Std. Dev. 21.18). Also, most nurses (84.7%) had high SR functioning impairment (those who had 12 scores and more) with a mean of 16.20 (Std. Dev. 4.65) followed in descending order by 66.7% experiencing poor IRs (those who had 15 scores and more) with a mean of 17.27 (Std. Dev. 5.49) and 45.5% had symptoms of distress (those who had a 36 or more score), with a mean of 33.78 (Std. Dev. = 12.20) (Table 2, Figure 2).

A descriptive analysis of overall nurses’ psychological well-being and its dimensions.
Nurses’ Perception of Their Psychological Well-Being (N = 400).

Note: Std. dev. = standard deviation.
Work Productivity Loss
Out of the 400 nurses studied, 91 of them, accounting for 22.8%, reported missing an average of 974.81 of their work hours in the studied week due to health problems, representing their absenteeism. On the other hand, a total of 248 nurses, representing 62.0% of the total, reported losing an average of 10,630 of their work hours due to their presenteeism (attending work while they were ill). Furthermore, 67.7% of nurses addressed overall work impairment as a result of WPAI-GH due to absenteeism and presenteeism combined and 75.5% of nurses’ regular daily living activities had been impaired due to their health problems (Table 3, Figure 3). See Supplementary File 1 (Table A1–A6) for the detailed responses to the six questions of WPAI-GH.

Percentage of nurses’ work productivity loss per working week.
Nurses’ Work Productivity Loss Per Working Week.

Number and Percentage of Missed Work Hours
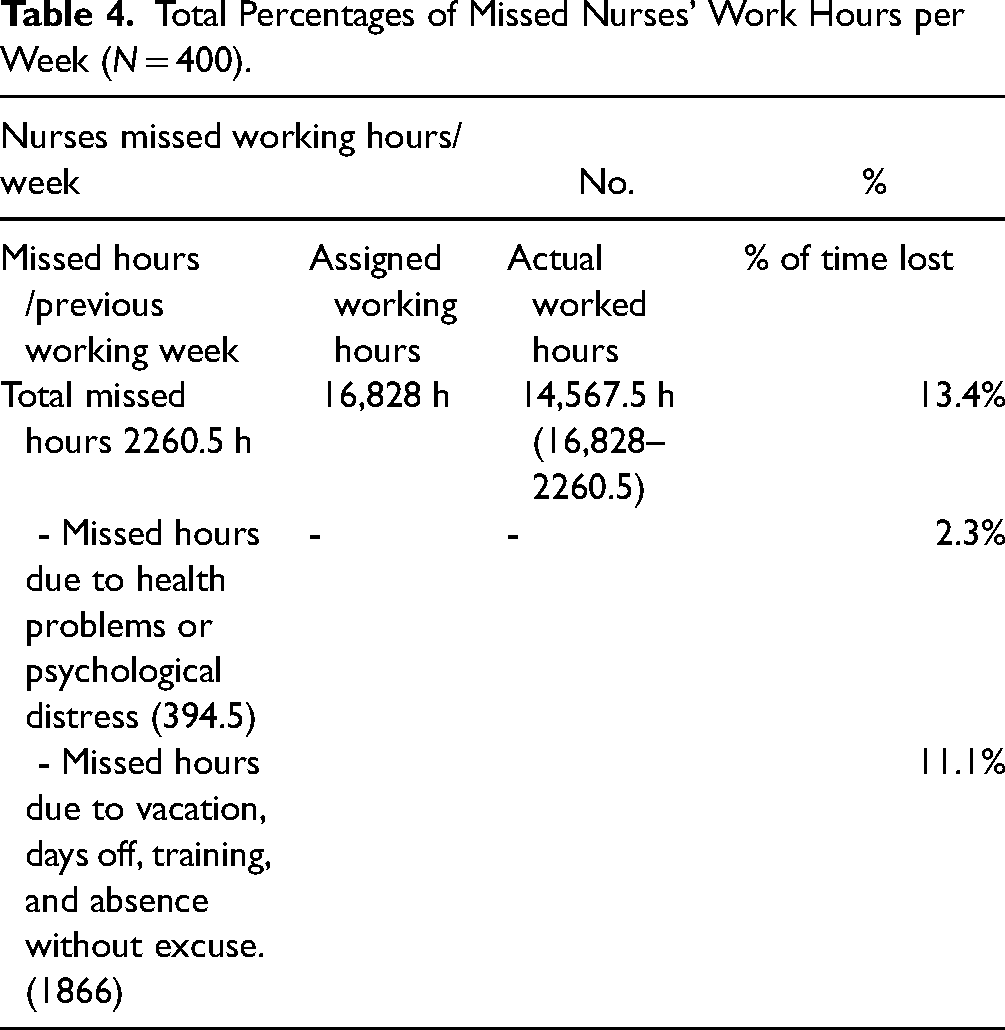
The total number of hours that were supposed to be worked by nurses during the study week was 16,828 h (400 nurses *42.7 h). At the same time, the missed nurses’ work hours during their previous working week are equal to 2260.5 h. The missed hours were derived by calculating the total missed hours due to health problems and psychological distress (394.5 h per week) plus the total missed hours due to other reasons such as vacation, days off, training, and absence without excuses (1866 h per week). So, the final actual hours worked by nurses during the studied week are the result of subtracting the assigned working hours from the actual working hours (16,828–2260.5 = 14,567.5 h) representing 86.6% of total nurses’ work time while 13.4% of nurses’ time was missed (Table 4).
Total Percentages of Missed Nurses’ Work Hours per Week (N = 400).
Correlation and Regression Model of the Relationship Between Psychological Well-Being and the Work Productivity Outcomes of Nurses
Table 5 shows the regression model results that illustrate the relationship between nurses’ overall psychological well-being (the independent variable) and their work productivity (the dependent variable). The regression coefficient determination shows that overall nurses’ psychological well-being can cause a variance and predict about 2.0% of nurses’ absenteeism, 11.0% of nurses’ presenteeism, 17.0% of nurses’ daily activity impairment, and 9.0% of nurses’ overall work productivity loss with significant F-models and p-value ≤0.05.
Regression Models of the Relationship Between Overall Psychological Well-Being and the Work Productivity Outcomes of Nurses (N = 400).

r = Pearson correlation coefficient; R2 = regression coefficient; F = F-test.
* Significant at p ≤ 0.05.
Furthermore, the finding of the mixed linear regression model reveals that in predicting nurses’ work productivity outcomes, the symptoms distress subscale of psychological well-being has the most significant power in predicting absenteeism (β = −.17, t = −2.33), presenteeism (β = .17, t = 2.42), nurses’ daily activities impairment (β = .26, t = 3.94), and overall work productivity loss (β = .18, t = 2.63) followed by SR functioning (p ≤ 0.05). See Table 6 for the detailed values.
Mixed Linear Regression Models of the Relationship Between Nurses’ Psychological Well-Being Domains and the Different Work Productivity Outcomes (N = 400).

t = t-test value.
*Statistically significant at * Significant at p ≤ 0.05.
Discussion
Perceived Levels of Nurses’ Psychological Well-Being
The present study aimed to investigate the relationship between nurses’ psychological well-being and their work productivity loss by examining how nurses self-reported their own psychological well-being and work productivity loss. In terms of descriptive analysis of self-reported data, the findings revealed that most nurses exhibited poor psychological well-being, indicating significant distress. Additionally, a substantial proportion reported high SR functioning impairment and poor IRs. Furthermore, near half of nurses exhibited symptoms of distress.
These findings highlight widespread psychological challenges among nurses. The prevalence of poor psychological well-being among nurses is a multifaceted issue influenced by various factors within their work environment and personal experiences. Stressful work conditions, including high patient-to-nurse ratios and emotionally demanding tasks, contribute to feelings of overwhelm and burnout. Organizational factors such as lack of support and limited growth opportunities exacerbate these challenges. Individual characteristics and coping mechanisms also play a role in determining nurses’ mental resilience (Alsayed et al., 2022; Rezio et al., 2022; Santos et al., 2022). Moreover, IRs among nurses are complex and multifaceted, suggesting the need for further investigation into their impact on work productivity. Likewise, Mahvar et al. (2020) highlighted various elements influencing the development of interpersonal communication culture, while effective workplace communication relies on nurses’ utilization of workspace and work patterns. Additionally, professional and occupational relationships among nurses contribute to therapeutic performance and the delivery of high-quality care.
The current findings mirror previous research that has consistently highlighted poor psychological well-being among nurses, along with increased levels of compassion fatigue, depression, and burnout. In the United States, Kim et al. (2021) demonstrated that nurses are grappling with poor mental health, as evidenced by the majority reporting moderate to high levels of stress. Within the same setting of the current study, Abou Hashish and Atalla (2023) revealed that the highest percentage of nurses reported a moderate level of compassion fatigue and burnout, suggesting a significant risk or potential for impaired well-being. Their findings indicate a concerning level of emotional exhaustion and potential burnout among nurses, potentially stemming from the pressures of the work environment and personal experiences. Also, the findings align with those of Li et al. (2022), who observed moderate to high levels of burnout, and secondary traumatic stress among Chinese nurses. This correspondence suggests a shared pattern of emotional experiences and challenges within the nursing profession across different cultural contexts, highlighting the urgent need for support and interventions to address their well-being.
Reported Nurses’ Work Productivity Loss
Moving to productivity loss, the current study revealed that about one-quarter of nurses reported an average of 974.81 work hours missed due to absenteeism, and near to-third lost an average of 10,630 work hours due to presenteeism. Additionally, the majority of nurses experienced impairment in their daily activities due to health issues, resulting in a loss of significant portion of their work hours. Similar to previous studies, the time lost due to presenteeism exceeded that of absenteeism. Compared to previous studies, Silva-Costa et al. (2020) revealed a significant portion of nurses reported compromised overall productivity, with a notable prevalence of presenteeism. In Dyrbye et al. (2019), it was reported that many nurses missed work in the past month due to personal health issues. Additionally, Burmeister et al. (2019) conducted a study involving a substantial number of nurses from multiple countries, revealing that the prevalence of missing work over the past three months varied significantly, with a considerable portion among nurses working in the United States. Similarly, Rantanen and Tuominen (2011) found that a substantial fraction of nurses worked while ill in the preceding weeks, leading to a notable reduction in their work capacity compared to their usual state.
The reported levels of absenteeism, presenteeism, and impaired daily living activities among nurses stem from the demanding nature of their work, long hours, high patient-to-nurse ratios, and physically and emotionally taxing situations (Dall'Ora et al., 2020). Nurses often work despite being unwell due to their critical role in patient care, leading to presenteeism, reduced productivity, and potential compromises in patient safety (Shan et al., 2021).
The Relationship Between Nurses’ Psychological Well-Being and Work Productivity Loss
The study found a significant correlation between impaired psychological well-being and work productivity loss among nurses. Regression analysis indicates that poor psychological well-being is associated with increased absenteeism, presenteeism, and daily activity impairment, partially supporting the hypothesis that diminished psychological health negatively impacts productivity. Distress and SR impairment emerged as key predictors of these productivity issues, with distress having the most substantial effect. However, these factors collectively explain only a small portion of the overall variance in work productivity loss.
These findings are consistent with previous research, which has demonstrated that psychological factors such as stress, depression, and anxiety negatively affect work performance and increase absenteeism and presenteeism among healthcare professionals, including nurses (Bamforth et al., 2023; Flaubert et al., 2021). The prevalence of impaired daily living activities among nurses underscores the significant impact of work-related stressors on their personal lives. Factors such as high workload, excessive emotional exhaustion, and chaotic work environments with insufficient psychological support likely exacerbate productivity loss. Literature suggests that working despite illness or health issues results in poorer physical and mental health outcomes, decreased job satisfaction, increased burnout, and diminished work performance, all contributing to economic costs (Evans-Lacko & Knapp, 2016; Shan et al., 2021).
In comparison with other studies, Silva-Costa et al. (2020) reported a higher prevalence of presenteeism among nurses, with a correlation observed between presenteeism and a higher level of common mental disorders. Tokac and Razon (2021) found a moderate positive correlation between poor mental health indicators, such as anxiety, depression, burnout, insomnia, and work impairment. Similarly, Li et al. (2022) highlighted these symptoms of distress, like job burnout, can lead to increased fatigue, sickness presenteeism, and productivity loss among nurses. Bubonya et al. (2017) demonstrated a direct relationship between mental health status and reduced work productivity through presenteeism and absenteeism. Like Kruk et al. (2018), nurses in the present study may face challenges in maintaining their SRs and IRs. These studies collectively illustrate the significant impact of poor mental health on work productivity, presenteeism, absenteeism, and the ability to maintain SRs and IRs among nurses.
Speaking about the correlation among the variable dimensions, SD emerged as the most significant predictor of work productivity loss and impairment, followed by the SR scale of the OQ. This contrasts with Allred (2012) and Trotter et al. (2009), where the SR scale was a significant predictor of presenteeism, overall work impairment, and activity impairment, suggesting a correlation between higher absenteeism and greater overall work impairment. Our results suggest that general mental health issues, as captured by SD, may encompass a broader range of challenges than the SR scale, which specifically assesses disturbances in work and leisure (Trotter et al., 2009). Additionally, the findings indicate that nurses’ overall poor psychological well-being has a minimal predictive effect on absenteeism compared to other outcomes.
Surprisingly, the results revealed a negative correlation between SD and absenteeism. The economic status of nurses often plays a crucial role in influencing their absenteeism behavior. Concerns about losing valuable fringe benefits can deter nurses from taking sick leave, leading them to prioritize attendance at work even when experiencing symptoms or distress. Similarly, Ose et al. (2022) linked this discrepancy to organizational policies and culture, suggesting that financial consequences might discourage participants from taking sick leave, thereby increasing presenteeism and subsequent productivity loss. Additionally, Burmeister et al. (2019) found that full-time nurses, those working overtime, and those perceiving inadequate staffing in their units were more likely to report absenteeism.
This result matches with Parli (2018) suggests that economic crises, along with restructurings, downsizings, financial concerns, and fears of dismissal due to absence, influence employees’ decisions to work despite ill health. Presenteeism, or working while sick, is found to have higher economic costs compared to absenteeism due to sickness. Factors such as sick pay regulations, weak protection against dismissal, and inadequate confidentiality of health data contribute to increased presenteeism. This highlights the need for a human-rights-based approach to human resource management, crucial from both employees and public health perspectives (Aldoghan & Elrayah, 2021).
From the perspective of the current authors, the combination of these factors highlights the need for targeted interventions to address workload pressures, improve workplace support systems, promote overall well-being among nurses, and ensure a sustainable and effective nursing workforce. In this context, Kamel and Abou Hashish (2015) stressed the importance of recognizing the relationship between employee well-being, working conditions, satisfaction, and productivity. They advocate for proactive measures to address factors contributing to nurses’ poor well-being, such as high work demands and inadequate leadership. In addition, cultivating a positive work environment, providing organizational support, and adopting empowering and caring leadership styles are essential strategies for fostering positive attitudes and work behaviors among nurses. These approaches can enhance nurses’ well-being, engagement, and performance (Abou Hashish et al., 2024; 2023; Elliethey et al., 2024; Mohammad et al., 2023).
Strengths and Limitations of the Study
The study has notable strengths, including its original nature in Egypt, as the first to explore the link between nurses’ subjective well-being and work productivity loss. A rigorous methodology, employing validated instruments and expert review, enhances the credibility of the findings. Practical implications highlight the importance of addressing nurses’ well-being to improve productivity and patient care quality. However, limitations include the cross-sectional design, limiting causal inference, and the focus on a single hospital, limiting generalizability. Also, subjective measurements may introduce potential response bias inherent in self-reported data collection methods. While integrating productivity with economic indicators is beneficial, objective factors may be overlooked. Addressing these limitations in future research would enhance understanding of the relationship between nurses’ well-being and their work productivity.
Implications of the Study
The current study proposes vital recommendations for practice and management, education and professional development, and future research:
Implication for Practice and Management: To improve nurses’ psychological well-being and mitigate its negative impact on work productivity, hospital and nursing management should implement initiatives that promote quality of work life, effective coping strategies, resilience building, and social support. This may include:
- Fair work policies that ensure equitable workloads and reasonable working hours. - Work–life balance initiatives such as flexible scheduling and adequate time off. - Counseling services to provide emotional support and professional guidance. - Training programs focused on stress management and resilience. - Clinical supervision and mentoring to offer ongoing professional support. - Peer support groups foster a sense of community and shared understanding among nurses. - Efforts to reduce the stigma around mental health disclosure and accessing support are crucial for fostering healthier working cultures. This can be done by: - Creating an open and supportive environment where nurses feel safe to discuss their mental health. - Encouraging leaders and managers to model healthy behaviors and mental health openness. - Developing policies that protect nurses from discrimination based on mental health conditions.
Implication for Education and Professional Development: Educational / training departments should advocate for better organizational support for nurses’ well-being and promote evidence-informed self-care and mental well-being strategies in training programs. This can be achieved by: Integrating mental health education into nursing curricula; offering workshops and seminars on coping strategies and resilience and providing resources for self-care and stress management techniques.
Implication for Future Research
Future research should utilize qualitative methods to explore the reasons for high psychological impairment among nurses. This could involve in-depth interviews or focus groups to gain deeper insights into the personal and professional factors contributing to their stress and well-being. Another study could investigate the role of nurse managers in promoting psychological health and productivity. Understanding how managerial support and leadership styles impact nurse well-being could inform targeted interventions. Moreover, comprehensive studies employing regular panel surveys with validated measures can provide valuable insights into staff mental health trends over time. These studies can also assess the effectiveness of various interventions, helping to refine and improve support strategies.
Conclusion
In conclusion, the current study highlights the effect of impaired nurses’ psychological well-being in predicting productivity loss. Poor psychological well-being among nurses correlates with decreased work productivity, manifesting in higher rates of presenteeism, impairment of daily activities, and overall work productivity loss (absenteeism and presenteeism). These findings highlight the importance of addressing nurses’ psychological health to maintain optimal productivity levels. Moreover, by focusing on nurses in the Egyptian context, the study contributes valuable empirical data from a culturally diverse population, complementing past research primarily conducted in European and American settings. Moving forward, this research serves as a reference point and lays the groundwork for future investigations into the relationship between psychological well-being and productivity loss among nurses.
Supplemental Material
sj-docx-1-son-10.1177_23779608241285400 - Supplemental material for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study
Supplemental material, sj-docx-1-son-10.1177_23779608241285400 for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study by Azza Hassan Mohamed Hussein, Ebtsam Aly Abou Hashish and Boshra Mostafa Younes in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241285400 - Supplemental material for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study
Supplemental material, sj-docx-2-son-10.1177_23779608241285400 for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study by Azza Hassan Mohamed Hussein, Ebtsam Aly Abou Hashish and Boshra Mostafa Younes in SAGE Open Nursing
Supplemental Material
sj-doc-3-son-10.1177_23779608241285400 - Supplemental material for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study
Supplemental material, sj-doc-3-son-10.1177_23779608241285400 for The Relationship Between Nurses’ Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study by Azza Hassan Mohamed Hussein, Ebtsam Aly Abou Hashish and Boshra Mostafa Younes in SAGE Open Nursing
Footnotes
Acknowledgment
The authors would like to express our thanks to all the participants who agreed to be included in the study.
Authors’ Contribution
AH and EA conceived the presented idea. AH and EA developed the theory and performed the computations. AH and EA verified the analytical methods. AH and EA wrote, edited, and reviewed the main manuscript. AH and EA planned and encouraged BY to collect data and AH and EA supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Committee of the Faculty of Nursing, Alexandria University (IRB00013322-February 2022).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.