
Abstract
Introduction
Emergencies are increasingly prevalent, necessitating specialized management to address significant social disruption. Effective management of health emergencies requires resilience from governments and health institutions, as these emergencies are becoming more common and have wide-ranging consequences on health, society, and the economy. Due to the interconnected nature of our global society, events in one location can have international or even global impacts, as demonstrated by the COVID-19 pandemic.
Objective
This study aims to assess disaster management preparedness among nurses and physicians during pandemics.
Methods
This study used an online survey conducted in late 2022 to collect primary data through a purposive sampling method, involving both government and private hospitals in Palestine. The participants included 512 nurses and 241 physicians from various hospital units.
Results
The findings indicate varying levels of knowledge among participants, with a significant portion (67%) reporting no prior experience with real disaster situations. Additionally, 63% lacked prior disaster response experience. Regarding training courses, 17.8% of nurses and physicians prioritized emergency preparedness, trauma mass casualty response, and triage disaster management systems. Despite some understanding of disaster management, the study emphasizes the importance of hospital managers implementing national standards, engaging healthcare professionals in continuous education, and addressing gaps in perceived competence.
Conclusion
While participants demonstrated some knowledge of disaster management, the study suggests the importance of hospital managers adopting national standards, engaging healthcare professionals in continuous learning activities, and addressing perceived competence gaps.
Introduction
The occurrence of health emergencies has risen significantly, resulting in considerable social disruptions and requiring specialized management. Effective handling of these emergencies demands a high level of preparedness and resilience from both governments and health institutions. These disasters, which are becoming more frequent, have severe health, social, and economic impacts (Abed et al., 2021). In our interconnected world, incidents in one area often have global repercussions, as seen in recent events. Key elements of emergency management include centralized governance, coordination, resource allocation, and preparedness at all levels. However, the emergency response can be influenced by various factors, including specific strengths and weaknesses unique to Palestine (Khirekar et al., 2023).
The Palestinian healthcare system faces challenges related to access, impacted by geographic and political factors, including checkpoints and restrictions affecting certain populations. Health insurance coverage varies based on employment status, economic means, and specific policies. Nurses receive formal education ranging from diploma programs to master's degrees, adhering to international standards. Disaster management preparedness training in nursing and medical curricula varies across institutions, underscoring the importance of such training in regions prone to disasters. Data on foreign-born nurses in Palestine are not readily available, with workforce demographics influenced by migration policies and international collaborations (Anera, 2020).
Palestine has experienced various health crises due to the Israeli occupation, frequent invasions, house demolitions, and epidemic diseases, including the ongoing COVID-19 pandemic (Hejaz, 2020). In response to COVID-19, the Palestinian Ministry of Health (MOH) developed and enforced preventive measures, with oversight from government agencies, especially the MOH. Researchers highlight the importance of crisis responsiveness and the government's dedication to managing the pandemic outbreak (Sham et al., 2018). Moreover, studies have recorded the challenges posed by disasters in recent years (Al Khalaileh et al., 2012; Bond & Tichy, 2007), which present significant difficulties for health organizations and communities in their response efforts (Total Disaster Risk Management-Good Practice, 2005).
Disasters cause severe disruptions to community functioning that surpass the community's ability to manage with its own resources. These disruptions can stem from natural or technological hazards and are influenced by factors affecting a community's exposure and vulnerability (IFRC, 2023). Disasters lead to loss of life, damage to public infrastructure, and significant interruptions in healthcare delivery systems, hindering proper responses to disaster victims (World Health Organization, 2019). Addressing the negative impacts of these disasters requires effective management strategies (World Health Organization, 2019). Consequently, disaster management demands collaboration from various organizations (Bly et al., 2021).
The initial phase in disaster management is preparedness, which involves proactive measures taken before an incident occurs. This stage encompasses the creation of warning systems, organization of evacuation and transportation logistics, stockpiling essential supplies such as food and water, conducting disaster simulations and drills, and developing comprehensive management plans.
The second stage, mitigation, involves actions designed to lessen the impact of a disaster. These measures encompass hazard and risk assessment, vulnerability analysis, resource allocation, and cross-training of staff. The third stage is the response phase, which involves the rapid implementation of disaster plans, activation of incident command systems, mobilization of staff, distribution of kits and equipment, patient treatment, and provision of additional relief measures such as food and shelter. The final stage, recovery, focuses on restoring human well-being and rehabilitating structures and services, aiming to return to a predisaster state, which can take from a few weeks to many years (Restore Your Economy, n.d.).
Healthcare providers, especially those organized in hospitals, are often the primary responders in a crisis. Effective disaster response depends on thorough preparedness and the availability of necessary resources (Pourhosseini et al., 2015). Nurses and physicians play critical roles in disaster management by promptly identifying and addressing needs (World Health Organization, n.d.). Comprehensive disaster management preparedness, including education programs, drills, and exercises, is essential for building confidence and professional expertise. Integrating disaster management into undergraduate health curricula can also enhance readiness (Bond & Tichy, 2007).
Recent studies have shed light on the disaster management capabilities of private hospitals. For instance, a study by Azarmi et al. (2021) found that private hospitals often have more flexible policies but face challenges in resource allocation compared to public hospitals. Another study by Alruwaili et al. (2021) highlighted the importance of tailored training programs in private settings to address specific vulnerabilities. For that reason, the study aims to assess disaster management preparedness among nurses and physicians during pandemics.
Review of Literature
A comprehensive literature review was conducted to assess the state of research on nurses’ and physicians’ experiences with disaster management preparedness during disease outbreaks. The review, which spanned from January 2020 to June 2024, utilized multiple search engines including PubMed, Scopus, and Google Scholar. The focus was to identify studies addressing disaster management preparedness specifically in the context of Palestine.
Despite the extensive global research on disaster management preparedness among healthcare professionals, there is a noticeable scarcity of studies that focus on physicians’ experiences in disaster management within Palestine. This research gap prompted the authors to explore this topic further.
At the end of 2019, a novel coronavirus causing widespread illness and fatalities was identified in Wuhan City, Hubei Province, China. The WHO classified this outbreak as a “global pandemic” and worldwide concern.” The COVID-19 pandemic reached Palestine in early 2020, with initial cases in Bethlehem linked to tourists from affected countries. The number of infections rose daily, documented by the MOH. The rapid and extensive nature of the global pandemic has significantly strained hospital resources and services (Abed et al., 2021). This increasing frequency of disasters underscores the importance of disaster management preparedness.
Frontline healthcare professionals in hospital departments play a critical role in disaster response, leveraging their knowledge and expertise to fulfill this crucial duty. They also contribute to disaster management preparedness by raising public awareness of disaster risks and providing emergency care. Essential crisis management skills are necessary for healthcare professionals to effectively handle disasters. However, studies indicate that healthcare professionals often lack adequate preparation for disaster-related duties (Azizpour et al., 2022).
The findings of this study, which aim to address this gap, provide valuable insights into the current state of disaster management preparedness among healthcare practitioners in Palestine. Specifically, the study seeks to compare the levels of preparedness between nurses and physicians using the Disaster management Preparedness Evaluation Tool (DPET). This tool is designed to assess healthcare providers’ knowledge of disaster management preparedness. The guiding research question for this study is: “What is the knowledge of disaster management preparedness among nurses and physicians in Palestine?”
Methodology
For this study, we employed a cross-sectional online survey as the selected research design, with eligible participants responding to a self-administered questionnaire that incorporated a mix of structured and open-ended questions, as utilized in a prior investigation (Farghaly et al., 2022). Utilizing a survey questionnaire proved efficient and cost-effective in swiftly gathering a substantial amount of data. Online survey administration offered convenience to busy professionals such as nurses and physicians, allowing them to complete the questionnaire at their own pace. Despite reduced researcher control, participant anonymity was enhanced, fostering more honest responses. The study encompassed all governmental and private hospitals in Palestine, including various units such as intensive care, medical and surgical departments, outpatient clinics, emergency departments, maternity wards, and pediatric and neonate wards. All hospitals in Palestine, both public and private, were included in the study rather than selecting a sample. This comprehensive approach was chosen to ensure that the data accurately reflected the disaster management preparedness across the entire healthcare system. The study was conducted in Palestine, a region with unique geographic, political, and socioeconomic challenges that significantly impact its healthcare system. The Palestinian healthcare system comprises both public and private hospitals, which are distributed across urban and rural areas. These hospitals face various obstacles, including limited resources, political instability, and frequent health emergencies.
The purposive selection of these units was driven by the elevated potential risk during the COVID-19 outbreak. The target study population comprised nurses and physicians (N = 647) with over years of experience, spanning various clinical departments. Inclusion criteria specified participants with nursing diplomas, bachelor's, master's, or PhD degrees for nurses, and physicians possessing bachelor's degrees or higher in their specialties. Participation in the study was voluntary, and the response rate was 85.9%, with 647 nurses and physicians returning completed questionnaires.
The primary tool for data collection was an online self-administered questionnaire, comprising both structured and open-ended questions. This design facilitated standardized data collection while allowing for spontaneous, detailed responses where necessary. Hosted on Google Docs, the questionnaire utilized in this study is based on the DPET, initially developed by Bond and Tichy (2007). The validity and reliability of the DPET have been established through verification in multiple countries, including those in Asia and the Middle East (Bond & Tichy, 2007).
The survey was conducted over two months, from September to October 2022, and distributed to nurses and physicians through their hospital official websites using Google Forms. To ensure a representative sample, the survey was disseminated through professional healthcare networks, associations, and institutions. No login with unique email IDs was required to encourage candid responses and maintain participant anonymity. The questionnaire, which took approximately 15 min to complete, assessed various stages of the disaster management process and was available in Arabic.
A pilot study involving 10% of the sample was conducted to confirm the clarity and feasibility of the study tools. All participants were Arabic speakers, and the Arabic version of the questionnaire, previously validated in a Jordanian study, was utilized. The reliability of the questionnaire was tested using Cronbach's alpha coefficient. The DPET tool comprised 45 items on a 5-point Likert scale, assessing various stages of disaster management. Average scores were calculated for each stage, and the total scale score indicated overall management preparedness. After data collection, the raw data underwent revision, coding, and processing using SPSS V23. Descriptive statistics, independent samples t-tests, Pearson correlation tests, Cronbach's alpha tests, and ANOVA tests were utilized for statistical analyses.
Results
Table 1 provides an overview of the demographic profile of 647 nurses and physicians who participated in this study. The sample's demographic profile includes gender, age, marital status, education level, employment status, workplace type, and years of experience. The data indicate that the sample was predominantly male (62.1%), aged 30–39 years (42.8%), and predominantly married (67.7%). In terms of education, most held a bachelor's degree (63.2%), followed by those with a master's degree (21.9%). Regarding employment status, most participants were employed full time (82.5%), with the majority working in governmental hospitals (58.7%). Participants’ years of experience varied, with 39.8% having 10–19 years of experience.
Demographic Characteristics of the Sample (N = 647).

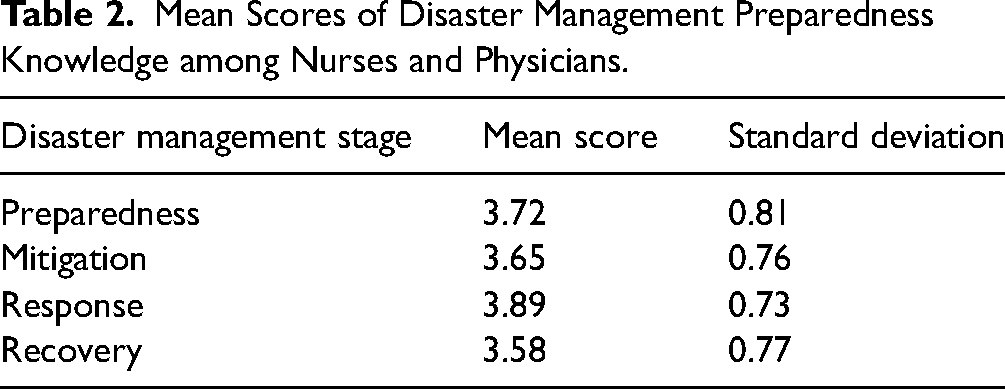
To assess the knowledge of disaster management preparedness among nurses and physicians, Table 2 displays the mean scores for the various stages of preparedness: preparedness, mitigation, response, and recovery. The results showed that the overall knowledge of disaster management preparedness among nurses and physicians was moderate. The highest mean score was found in the response stage (M = 3.89, SD = 0.73), followed by preparedness (M = 3.72, SD = 0.81), mitigation (M = 3.65, SD = 0.76), and recovery (M = 3.58, SD = 0.77).
Mean Scores of Disaster Management Preparedness Knowledge among Nurses and Physicians.
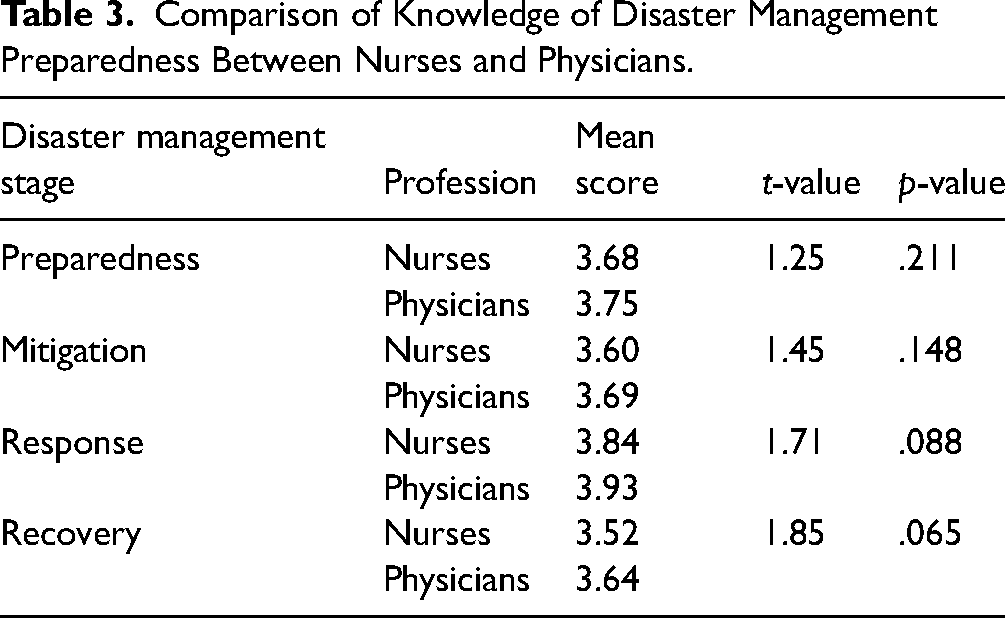
In Table 3, the t-values signify outcomes of an independent samples t-test, assessing knowledge score means between nurses and physicians across various disaster management preparedness stages. Correspondingly, the p-values measure the likelihood of observing such results, or more extreme, assuming the null hypothesis holds true, with lower p-values indicating stronger evidence against the null hypothesis. Across the preparedness, mitigation, response, and recovery stages, the analysis reveals no statistically significant disparity in disaster management preparedness knowledge between nurses and physicians. Despite some results nearing significance, particularly in the response and recovery stages, their values remain above the conventional threshold of 0.05. Consequently, while trends hint at potential distinctions, notably in the response and recovery stages, these disparities do not attain statistical significance.
Comparison of Knowledge of Disaster Management Preparedness Between Nurses and Physicians.
The study participants highlighted several areas where they felt a need for additional training in disaster management preparedness. Table 4 provides a detailed distribution of these training needs among nursing staff and physicians.
Training Needs Distribution among Study Subjects.

The most frequently identified training needs were in the areas of Disaster Management Systems, with 27.27% of nursing staff and 38.65% of physicians indicating a need for further education in this area, totaling 30.88% overall. Training for External Disasters and Man-Made Disasters (including Terrorist Attacks Management and Evacuation Plans) was noted by 22.73% of nursing staff and 28.99% of physicians, representing 24.71% of all participants. COVID-19 Health Disaster management preparedness was also a significant area of concern, with 18.18% of nursing staff and 24.15% of physicians expressing a need for more training, totaling 20.08%. Additionally, 25.00% of nursing staff and 28.99% of physicians identified Fire and Safety Management as a key area for improvement, amounting to 26.25% overall. First Aid was deemed necessary by 29.55% of nursing staff and 38.65% of physicians, making it the most commonly identified training need at 32.43%. Lastly, training on the Policy of Disaster Management/Supply Chain Disaster Management was needed by 22.73% of nursing staff and 24.15% of physicians, totaling 23.16%.
In the disaster management preparedness stage, there was a significant positive relationship between the knowledge of nursing staff and physicians and various demographic and work-related characteristics, all showing p < .001. Both groups demonstrated significant associations between their knowledge of the disaster management preparedness stage and factors such as age, level of education, working units, and years of experience (all p < .001). The correlation coefficient for the level of education and knowledge of the disaster management preparedness stage is 0.79, indicating a strong positive correlation, suggesting that individuals with higher education levels tend to have greater knowledge of disaster management preparedness. Similarly, during the disaster mitigation/response stage, there was a significant positive relationship between the knowledge of nursing staff and physicians and their age, level of education, working units, and years of experience (p < .001). The coefficients for the disaster mitigation/response stage (0.72) and disaster recovery stage (0.75) also indicate strong positive correlations. Additionally, a positive relationship was found between the knowledge of nursing staff and physicians and age, level of education, working units, and years of experience (p < .001). The correlation coefficients for working units and knowledge of disaster management stages are 0.74 for the disaster management preparedness stage, 0.67 for the disaster mitigation/response stage, and 0.71 for the disaster recovery stage. These coefficients indicate strong positive correlations, suggesting that specific working units of individuals are significantly associated with management stages (see Table 5).
Correlation Between Study Subjects’ Demographic and Work-Related Characteristics and Their Knowledge of Disaster Management Preparedness Stages.

*Statistically significant at p ≤ .0.
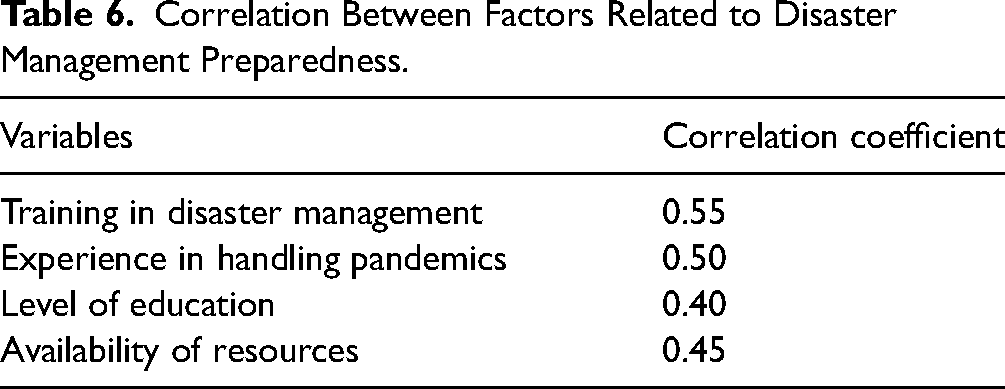
The correlation coefficients indicate relationships between various factors related to disaster management preparedness among healthcare professionals during pandemics. A coefficient of 0.55 between these factors suggests a moderate to strong positive relationship (see Table 6).
Correlation Between Factors Related to Disaster Management Preparedness.
Government hospitals had higher preparedness (M = 3.75, SD = 0.79) and response (M = 3.92, SD = 0.70) scores compared to private hospitals (preparedness: M = 3.64, SD = 0.85; response: M = 3.80, SD = 0.75). However, private hospitals scored higher in mitigation (M = 3.70, SD = 0.78) and recovery (M = 3.62, SD = 0.74). Significant differences were found in preparedness (t(645) = 2.14, p = .03) and response (t(645) = 2.01, p = .045) stages. Training needs were higher in private hospitals for disaster management systems (38.65%) and first aid (38.65%) (see Table 7).
Comparison of Disaster Risk Management Preparedness Between Government and Private Hospitals.
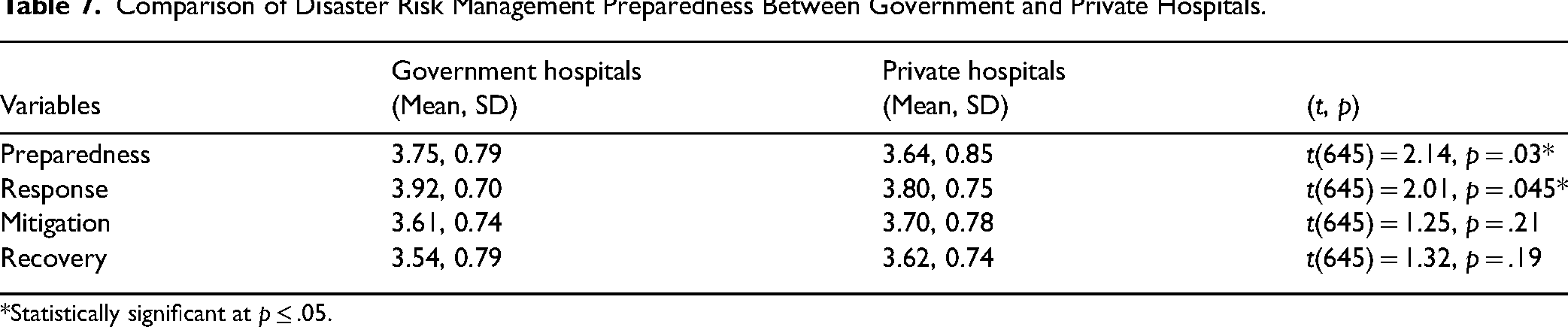
*Statistically significant at p ≤ .05.
The regression analysis shows how much these factors predict disaster management preparedness among healthcare professionals during pandemics. The significant beta coefficients and low p-values indicate that training in disaster management, experience in handling pandemics, level of education, and availability of resources “the extent to which necessary materials, equipment, personnel, and financial assets are accessible and can be utilized to achieve specific objectives or tasks” are significant predictors of disaster management preparedness (see Table 8).
Predicting Disaster Management Preparedness among Healthcare Professionals During Pandemics.

The correlation and regression analyses specifically linking these factors to disaster management preparedness among healthcare professionals during pandemics demonstrate statistically significant relationships, with higher levels of training, experience, education, and availability of resources associated with better disaster management preparedness.
Discussion
The results of this study reveal that participants possessed a moderate level of knowledge regarding disaster management preparedness, with an overall mean score of 3.58 ± 0.63. Notably, high scores were observed in the disaster management preparedness stage, indicating some understanding of essential disaster management practices. This finding aligns with the observation that a significant proportion of participants had not experienced real disaster situations, though many had received prior disaster management training.
The study did not extensively address the content of disaster management education in nursing and medical school curricula or the extent of disaster preparation training provided in workplaces. This limitation mirrors findings from other research, which indicates that while healthcare professionals generally exhibit satisfactory knowledge of disaster management preparedness, gaps remain. For instance, studies by Farghaly et al. (2022) and Nofal et al. (2018) reported average perceived knowledge scores among healthcare professionals, while research from Iran indicated lower perceived preparedness levels (Chegini et al., 2022).
It is crucial to contextualize these findings within the broader framework of disaster management challenges, especially given the unique circumstances in Palestine. The absence of references to published WHO reports on the current healthcare disaster situation in Palestine is a notable gap. These reports highlight critical issues such as resource shortages, violence, and the impacts of ongoing conflicts on health professionals. Despite not being a pandemic, the current situation in Palestine represents a severe disaster scenario, and understanding how health professionals are navigating these challenges is vital.
Moreover, resilience is an important aspect of disaster management that was not discussed. Resilience allows healthcare professionals to anticipate, plan, and recover from disasters effectively. This concept is particularly relevant as healthcare workers in Palestine, as well as globally during the COVID-19 pandemic, have demonstrated remarkable adaptability and endurance in the face of crises. Research on resilience, such as that conducted during the COVID-19 disaster, emphasizes the need for ongoing support and training to enhance the ability of healthcare professionals to manage and recover from emergencies (Balut et al., 2022; Goniewicz et al., 2020).
The study also revealed significant variations in knowledge based on factors such as education level, years of experience, and work environment. Intensive care unit nurses and physicians with higher education levels and more experience demonstrated better preparedness scores, likely due to their exposure to critical care scenarios. This finding is consistent with other studies indicating that healthcare professionals in high-stress environments often have better disaster management preparedness (Simpson et al., 2022).
Conversely, some studies have found no significant correlation between nurses’ demographic characteristics and their disaster management preparedness levels. Nevertheless, participants clearly identified a need for training in various areas of disaster management, including Emergency Situations Preparedness, Disaster Management Systems, and COVID-19 Health Disaster management preparedness (Mosleh et al., 2021).
In Egypt, the importance of comprehensive disaster planning and training is well-documented, emphasizing the need for hospitals to have robust plans for both internal and external disasters (Ghoneim, 2021). Similarly, nurses’ confidence in handling large-scale emergencies tends to be higher when they have practical experience in such situations. This underscores the need for thorough training and education, as nurses play a crucial role in emergency response through activities such as contact tracing, vaccine administration, and public education (Zarea et al., 2020).
The International Nursing Coalition for Mass Casualty Education has identified essential elements for integration into nursing curricula to build confidence in emergency response capabilities (International Nursing Coalition for Mass Casualty Education, 2018). Incorporating these elements into training programs is vital to ensure that healthcare professionals are prepared to handle emergencies effectively.
Overall, the study highlights the importance of continuous education and training in disaster management for healthcare professionals, considering the unique challenges and resilience demonstrated by those working in disaster-affected regions.
Conclusions
Both nurses and physicians expressed concerns about a lack of training, the absence of strategic and operational plans, and their unfamiliarity with roles, procedures, and assignments in catastrophic circumstances due to severe gaps in emergency preparedness knowledge.
Future longitudinal, experimental, and multisite investigations involving medical staff in Palestine are necessary. The proposed future research aims to evaluate the effectiveness of disaster management interventions, focusing on their impact on the knowledge, skills, and preparedness of medical staff. Additionally, longitudinal studies will explore the evolution of disaster management knowledge over time, identifying factors influencing retention or decline. Another area of investigation involves understanding the preferences of nurses and physicians in disaster management education, examining factors such as format, frequency, and content delivery.
Limitations of the Study
However, there are a few limitations to consider. First, because the study sample was selected using an online questionnaire based on convenience, the generalizability of the results is limited. Second, since the current findings rely on self-reported data, participants may not feel motivated to provide truthful or accurate responses. Finally, it is important to note that no directionality or causal relationship can be inferred because this study only demonstrates relationships between study variables.
Implications for Practice and Management
The findings from this study indicate that managers who facilitate regular real disaster training for nurses and physicians can expect greater effectiveness in disaster management. By providing support for ongoing training and preparedness initiatives, healthcare organizations can enhance their ability to respond to and manage real health-related disasters more effectively. Furthermore, the results of this research can serve as a valuable guide for healthcare administrators in establishing national health standards and protocols. This includes developing strategic and operational plans to ensure an adequate number of qualified personnel are trained and prepared for disaster and emergency situations. Additionally, fostering a culture of preparedness within healthcare organizations will be essential for improving overall response capabilities. Overall, these insights can inform decision-making and resource allocation to strengthen disaster management preparedness and response efforts within healthcare systems.
Key Messages
What is Already Known on This Topic?
Disasters and public health emergencies have been increasing in frequency and severity globally, with significant health, social, and economic consequences.
Palestine has experienced several health disasters, including the COVID-19 pandemic, which requires effective management and preparedness.
Healthcare providers, such as nurses and physicians, play a vital role in disaster management, but their preparedness and knowledge levels vary.
What This Study Adds
This study assesses and compares the knowledge of disaster management preparedness among nurses and physicians in Palestine during disease outbreaks.
It utilizes the DPET, a specific tool designed to measure healthcare providers’ knowledge of disaster preparedness.
By examining the knowledge levels of healthcare providers, this study adds to the existing literature on disaster preparedness among nurses and physicians, particularly in the context of Palestine.
How This Study Might Affect Research, Practice, or Policy
The findings of this study will contribute to our understanding of nurses’ and physicians’ preparedness for disaster management in Palestine.
It will shed light on the current knowledge levels and identify areas that need improvement in disaster preparedness among healthcare providers.
The results may inform future research on enhancing disaster management training and education for nurses and physicians in Palestine.
The study's findings can guide policymakers and healthcare institutions in developing strategies to improve disaster preparedness and response in the region.
Footnotes
Authors’ Contribution
IA initiated the study and collected the data. IA, along with MS, drafted the manuscript and approved the final version submitted for publication. Both IA and MS agree to be accountable for all aspects of the work, ensuring that questions related to accuracy or integrity are appropriately addressed and resolved. MS, KS, and AA made significant contributions to the design, analysis, and interpretation of the data for this study. Additionally, MS, KS, and AA provided critical revisions to the manuscript for important intellectual content. IA have reviewed and approved the final version submitted for publication. IA also agrees to be accountable for all aspects of the work, ensuring that any questions related to accuracy or integrity are properly investigated and resolved.
Ethical Approval and Consent to Participate
The ethical approval was obtained to conduct the study from “Nablus University for Vocational and Technical Education (NU-VTE)” (Reference No: Nrs. September. 2022/1). We affirm that all methods adhered to relevant guidelines and regulations. The study was voluntary and no anticipated risks. The study preserves the confidentiality and the participants have the right to withdraw at any time. By agreeing to participate, the participants assigned the informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.