
Abstract
Background
Given the recency of the COVID-19 pandemic, few studies focus on the challenges frontline healthcare providers (HCPs) face in Saudi Arabia. There aren't many studies that specifically address the difficulties Saudi Arabia's frontline nurses confront due to the COVID-19 pandemic's recent onset.
Objective
This study was conducted to assess the concerns, perceived impact, and preparedness of nurses during COVID-19.
Method
Five hundred and thirty-four nurses participated in this cross-sectional and descriptively planned research on nurses in a tertiary healthcare setting in the Kingdom of Saudi Arabia. The study was conducted between July and October 2020, during the second wave of the virus outbreak. Participants in this study were nurses working in the acute healthcare setting. These nurses spoke English well. A 38-item anonymous self-structured survey that was previously utilized in research was adopted.
Results
On concerns over working and nonworking conditions, the responses confirm the findings of similar studies globally. Most respondents were concerned about their susceptibility to COVID-19 infection and reported feeling more stressed at work. The majority of nurses (96.88%) confirmed the presence of an infection control committee in their hospitals, emphasizing the importance of a strong organizational structure. Among the findings are the respondents’ strong sense of confidence regarding their own readiness and the readiness of their organizations. A significant association was observed between nurse's assessments of the effect of COVID-19 on their professional and personal life, as classified by age and job title.
Conclusion
Despite their and the institution's readiness, most nurses who replied to the survey questionnaire expressed work and nonwork-related worries. To effectively manage the effects of COVID-19, operational planning and execution in healthcare institutions must consider psychosocial counseling, epidemiological education, and environmental control training for HCPs.
Introduction
The World Health Organization reported the new coronavirus (COVID-19) occurrence in the Hubei province in China before the end of 2019 (Salzberger et al., 2020). The appearance and spread of COVID-19 indicated a new pandemic, which demanded the immediate attention of governments and health agencies worldwide (Sohrabi et al., 2020). Managing the growing demand for healthcare services will be the most significant challenge. Healthcare services will be better able to handle the influx if there is a high degree of readiness (Cutter, 2008). Healthcare workers (HCWs) are primarily affected by the COVID-19 pandemic and need to be protected since they are more susceptible to viral infection because of constant exposure (Smith, 2020).
The COVID-19 epidemic caused psychological health problems and anguish in the medical profession, particularly nurses. Despite having a sufficient understanding of COVID-19, more than 50% of respondents reported experiencing mental health problems, including anxiety (Alsharif, 2021). Due to the nature of their jobs, frontline healthcare providers (HCPs) encountered several difficulties during this pandemic (Alsulimani et al., 2021). When an underlying organic ailment existed, being female and having family obligations enhanced the chance of suffering from mental effects. Additional risk factors were the worry about contracting an illness, a lack of personal protective equipment (PPE), and close contact with COVID-19 (De Kock et al., 2021). HCWs had worries and apprehensions about working with COVID-19 patients who are highly contagious. The panelists liked the bulk of institutional readiness, although they were worried about PPE availability and continued supply (Alreshidi et al., 2020).
Review of Literature
The initial wave of COVID-19 caused a lot of emotional hardship for the healthcare workforce. Emotional responses, coping strategies, and stresses differed by health care position, but some experiences and reactions were consistent across groups (Rose et al., 2021). HCPs, particularly female nurses and frontline HCWs, who were directly involved in the diagnosis, treatment, or provision of nursing care to patients with suspected or confirmed COVID-19, experienced depression, anxiety, insomnia, and distress in hospitals with fever clinics or wards for COVID-19 patients (Lai et al., 2020). In addition to the family members and society's perceived shame, which heightened negative consequences, most notably stress and isolation, was the dread of the unknown or contracting an infection. Coping mechanisms differed among physicians, nurses, and other HCWs and the various sociocultural contexts (Cabarkapa et al., 2020).
The present epidemic is reenacting the same situation. In Saudi Arabia, COVID-19 has grown to be a critical element that may negatively impact the nation's infrastructure for public health preparedness. HCPs are at risk and concerned about getting infected with novel coronaviruses (Abolfotouh et al., 2020). HCPs were said to have experienced work-related stress in 2003 during the acute respiratory syndrome (SARS) epidemic, largely because of the healthcare system's strain (Koh et al., 2003; Tam et al., 2004). The largest HCWs in the healthcare system are mostly nurses fighting the epidemic on the front lines (World Health Organization, 2020). Many nurses worry about their work and its personal effects while carrying out their professional responsibilities in times of crisis (Chiang et al., 2007; Koh et al., 2012). According to recent research in china, during the COVID-19 epidemic (Hu et al., 2020), nurses experienced mental health challenges, especially burnout and fear.
In reaction to COVID-19, Saudi Arabia equipped both public and commercial institutions to manage the pandemic. Saudi Arabia prepared governmental and private organizations to handle the epidemic in response to COVID-19. To regularly track national and worldwide updates, track contacts, screen the population, create awareness, and take appropriate measures to stop the spread of this illness, Saudi authorities built a governance framework made up of responsible committees. With the preparedness, restrictions, and precautions, Saudi Arabia successfully limited the spread of SARS-CoV-2. The number of deaths was not very high compared to other countries, highlighting the excellent care in hospitals in Saudi Arabia (Khan et al., 2021). This was demonstrated by Saudi Arabia, which implemented preventative measures and decreased infection and mortality rates in the region by 27% compared to other nations, where the death rate varied from 10% to 73% (Adly et al., 2020). However, a study has to be initiated to examine the concerns of the nurses who were the frontline care providers during the pandemic. The current study aimed to examine the general concerns about COVID-19 among nurses in Saudi Arabia, as well as their opinions of its effects and levels of readiness.
Method
Study Design
The study adopted a descriptive, cross-sectional study design to assess nurses’ concerns, perceived impact, and preparedness during COVID-19.
Study Setting and Participants
The study was conducted in a tertiary healthcare setting that offers various healthcare services to the population around the Riyadh region. With a total bed capacity of about 1,000, it is one of the Middle East's largest and fastest-growing medical complexes. The study was conducted between July and October 2020, during the second wave of the virus outbreak.
The population is about 3,000 nurses working in the healthcare setting. The participants were 534 nurses selected by convenience sampling technique. Nurses working in the setting for more than 6 months, fluent in English, and available during the data collection period were considered the participants of this study. Nurses who were unwilling to participate and the new nurses were excluded from the study.
Study Instrument
Data were collected using a structured self-administered questionnaire. An anonymous self-structured questionnaire was adopted in a previous study (Wong et al., 2008). The 38-item questionnaire was structured under three dimensions as follows:
Dimension 1: Work-related concerns and nonwork-related concerns, with eight and four items, respectively
Dimension 2: Perceptions of the impact of the pandemic on personal life and work, with 10 items
Dimension 3: Personal preparedness and that of the institutional workplace, with 16 items
A 6-point Likert scale was adopted to classify responses (strongly disagree, disagree, not sure but probably disagree, not sure but probably agree, agree, and strongly agree). A total of 534 HCPs participated in the research. The questionnaire responses were categorized into positive strongly agree, agree, and probably agree) and negative (strongly disagree, disagree, and probably disagree).
While analyzing the results, the overall alpha coefficient value was 0.827, indicating that the questionnaire used in this study was reliable. Also, Cronbach's alpha values for individual dimensions were reported to be 0.637, 0.860, 0.778, and 0.839, respectively, for Dimensions 1, 2, and 3 (itemized above).
Data Collection
The researcher provided the participants with explanations of the purpose of the research. The nurses received detailed information regarding the study's methodology. The participants’ consent was acquired before collecting the data, and the nurses were encouraged to participate, and the data were collected.
Data Analysis
The data was analyzed using SPSS Version 22.0 (SPSS Institute, Chicago, IL, USA). During statistical analyses, the scale was dichotomized into positive response (strongly agree, agree, and probably agree) and negative response (strongly disagree, disagree, and probably disagree). Descriptive statistics were employed to investigate the demographic characteristics of the HCPs and their corresponding responses across each dimension of the questionnaire. The participants’ demographic data and responses to each dimension were presented using frequency and percentage. The Cronbach-alpha reliability test was used to determine the reliability and validity of the questionnaire. Chi-square test was utilized in the bivariate analysis process to examine the association between demographic variables and different dimensions of the questionnaire. Specifically, the test was applied to determine the significant level of association between variables (age group and job title) with perceptions of the impact on personal lives and work among HCPs during COVID-19. The level of significance for the analysis was set at p < .05.
Ethical Considerations
The Institutional Review Board of the study setting granted ethical permission for this study (IRB Log No: 20-183), which adhered to the Declaration of Helsinki's principles. Potential participants were given explanations of the study's objectives before enrollment. All participants received guarantees of anonymity, confidentiality, and the freedom to withdraw at any time.
The nurses received detailed information regarding the study's methodology. The participants’ consent was acquired before data collection, and the nurses were encouraged to participate. The data were collected from the nurses working in the setting for over 6 months.
Results
Demographic Characteristics
The demographic characteristics reveal that the majority of the nurses were predominantly female (90.3%), married (59.4%), aged between 26 and 40 years (63.9%), non-Saudi (96.4%), qualified as registered nurses 372 (69.7%) and living alone (64%; refer Table 1).
Frequency and Percentage of Demographic Characteristics of HCPs.
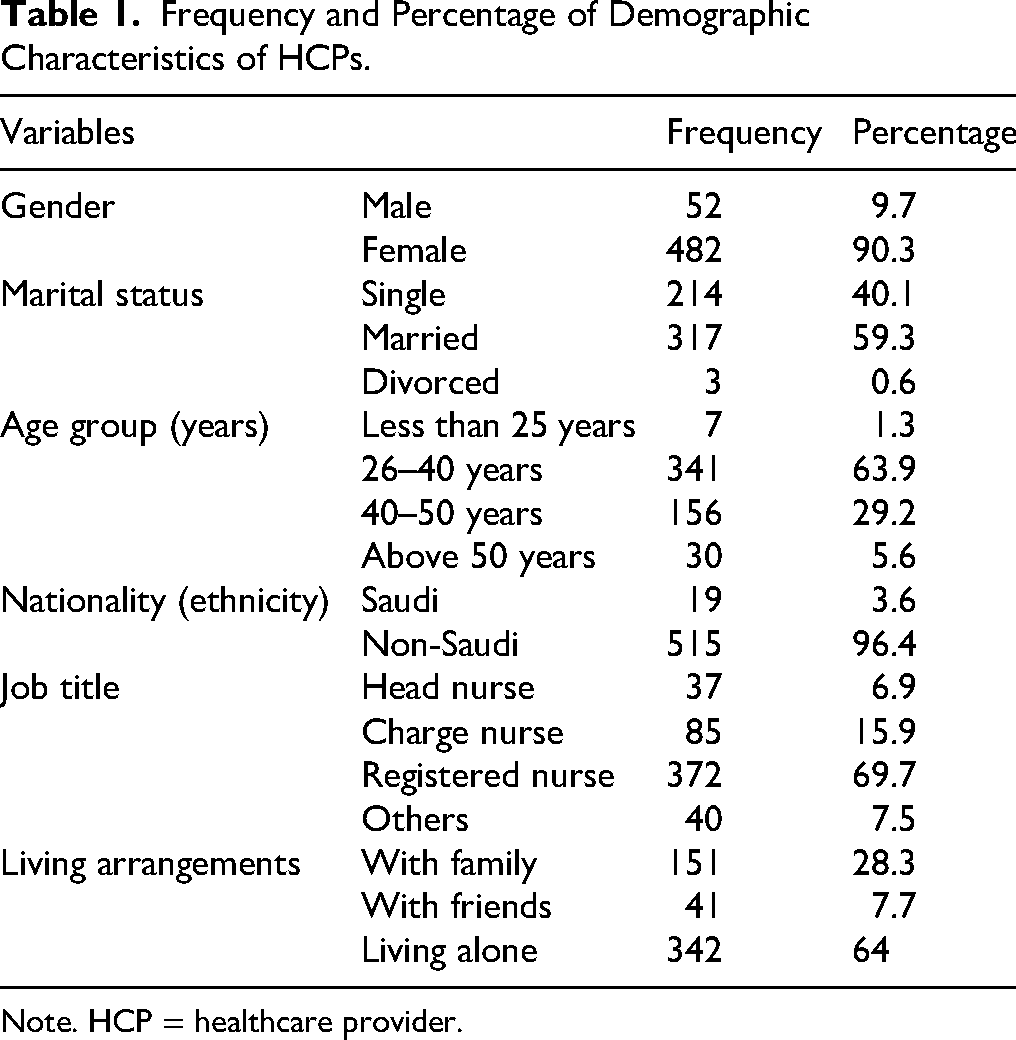
Note. HCP = healthcare provider.
Table 2 is a statistical summary of the responses of HCPs to questions used in the questionnaire under Dimensions 1 (Work-related concerns) and 2 (Perceived Impact on Personal Life and Work).
Concerns Regarding COVID-19 Pandemic.

Work-Related Concerns
On work-related concerns, 93.63% of respondents expressed concerns over their vulnerability through exposure to patients with COVID-19 infection (5.3 ± 1.1). 89.7% were afraid of falling ill with the coronavirus (5.1 ± 1.3). However, only 35.2% expressed any unwillingness to care for patients with coronavirus infection (3.0 ± 1.4), and 18.54% said they might look for another job (2.4 ± 1.3).
Nonwork-Related Concerns
On nonwork-related concerns, 97.19% of respondents felt that relations, dependents, and friends were worried for their (respondents’) health (5.4 ± 0.8). 88.95% of the respondents felt stressed over the possibility that people important to them in their personal lives could be at risk of viral infection (5.1 ± 1.2). Most respondents were concerned about their colleagues, friends, and spouses (Table 3).
Preparedness for COVID-19.

Chi-Square Association With Demographic Variables.
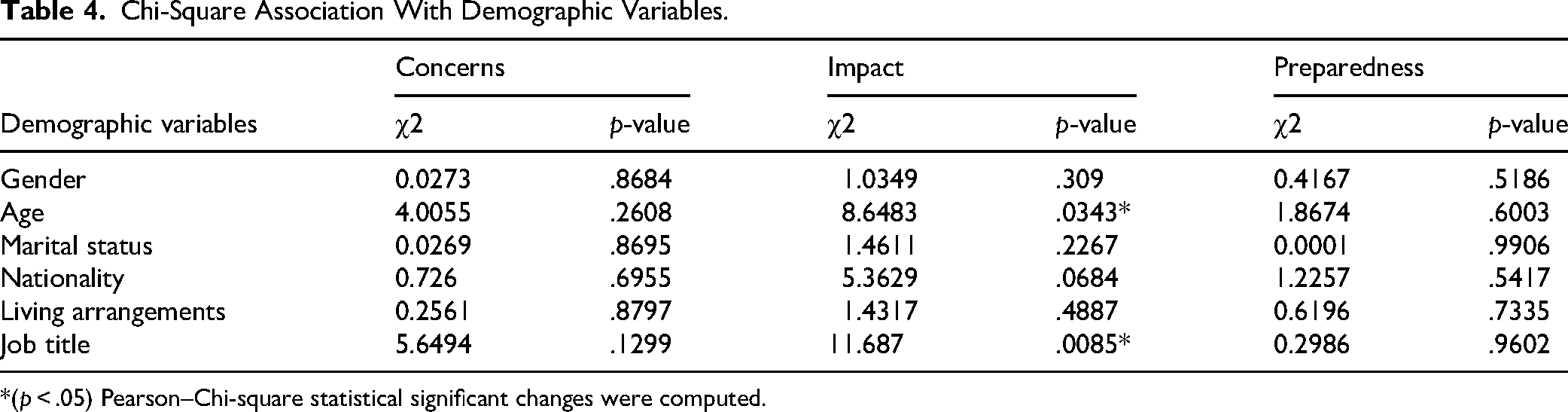
*(p < .05) Pearson–Chi-square statistical significant changes were computed.
Impact of the Pandemic on Their Personal Lives and Work
Concerning perceptions of the impact of the pandemic on their personal lives and work, 69.85% of the respondents felt greater stress at work than before (4.2 ± 1.5). 62.73% of the respondents felt that acquaintances might distance them on account of where they worked (3.8 ± 1.5), and 28.46% of the respondents said they would prefer to conceal disclosing the nature of their job to people they came into contact with (2.8 ± 1.5; Table 3).
Nurses and Institutional Preparedness
The data in Table 3 represent the nurses’ perceptions of institutional preparedness during the pandemic. The majority of nurses (96.88%) confirmed the presence of an infection control committee in their hospitals, emphasizing the importance of a strong organizational structure. Additionally, 92.51% of the staff received infection control training, indicating that comprehensive training measures were taken to ensure staff readiness (5.3 ± 0.9 and 5.1 ± 1.0, respectively).
Among the findings are the respondents’ strong sense of confidence regarding their own readiness and the readiness of their organizations. 88.2% of the respondents felt adequately prepared on a personal basis, while 89.3% expressed the view that their institutions could handle the pandemic. The majority of the responses reported being knowledgeable about someone to rely on for guidance with PPE usage and felt adequately trained in PPE application. Interestingly, only 41.01% purchased flu medication in the preceding 6 months (Table 3). The statistic results suggest that HCPs adopt varying approaches to preventive measures.
A Chi-square analysis was conducted to determine if demographic variables were associated with nursing concerns and preparedness during the COVID-19 pandemic. Interestingly, the Chi-square results showed no significant association between the demographic variables measured, such as gender, marital status, nationality, living arrangements, and nurse concerns and preparedness during COVID-19. Notably, a significant association was found between nurses’ age group and their job title during the pandemic, suggesting that these factors affected nurses’ experiences during COVID-19 (Table 4, Dimension 2).
Discussion
The global health care systems are impacted, and frontline HCWs—especially nurses—face numerous difficulties as a result of this crisis or pandemic. They are at the risk of exposure and contracting the disease. This study examined nurses’ perceived concerns, perceived impact, and preparedness among nurses during COVID-19 pandemic.
According to this survey, nurses in Saudi Arabia have worries about their working and nonworking environments, how it will affect their personal life, and how well they are equipped on an individual and institutional level to deal with the current COVID-19 epidemic. Most respondents were women, married, and between the ages of 26 and 40; these findings are consistent with earlier data collected during the SARS epidemic (Chung et al., 2005; Koh et al., 2012). HCWs in the United States reported having concerns about exposure to the illness and perceived the need for psychological support (Balicer et al., 2006). Prior research has demonstrated that most HCWs indicated a high-risk perception at work (Hope et al., 2011; Shaw et al., 2006). Several HCPs at the “front line” believed infection from pandemic diseases was an unavoidable occupational hazard (Koh et al., 2012; Martin et al., 2013). The current findings on worries at work are consistent with earlier research on HCPs during pandemics.
Prior research has documented the psychological discomfort experienced by frontline HCPs (Conversano et al., 2020). This fact raises the specter of increased infections among HCPs and the impact this could have on the people close to them. In line with this possibility, the present study showed that people close to the respondents were worried about the respondents’ health. In turn, HCPs feared that they were placing people close to them at greater risk of infection (Lam & Hung, 2013). Further, more than half of the respondents accepted the resignation of colleagues out of an understanding of their colleagues’ predicament of fear and anxiety (Ehrenstein et al., 2006). The present findings during the ongoing COVID-19 pandemic in Saudi Arabia thus corroborate previous results on nonwork-related concerns during pandemics elsewhere.
This study supports the findings of other studies (Huang, Lin et al., 2020; Wu et al., 2009) regarding how HCPs perceive the pandemic's effects on their personal and professional life. According to a recent survey, nurses experienced stress at work due to high workloads and a lack of personnel (Huang, Xu, & Liu, 2020). HCPs also indicated fear about their own and their families’ social rejection. Another similarity between accounts from the COVID-19 outbreak and those from the SARS pandemic is that HCPs who were clearly in uniform for their jobs reported experiencing stress symptoms (Wu et al., 2009).
The majority (96.88%) of HCPs who replied said that their hospital had an infection-control committee when asked about the COVID-19 pandemic's readiness (5.3 ± 0.9). Infection control training was provided to 92.51% of the responders (5.1 ± 1.0). While 89.3% of HCPs believed their institutions were equally prepared, 88.2% of HCPs said they were individually equipped to manage the catastrophe. This is in line with WHO guidelines (Wong et al., 2008), which stress the importance of preparing strategies to deal with the effects of pandemic breakouts. The current study provided documentation of institutional readiness, consistent with findings from a prior study showing that participants valued most areas of institutional readiness for the COVID-19 pandemic (Alreshidi et al., 2020).
Additionally, most respondents stated that they could depend on someone in the last 6 months if they required suitable PPE instruction on using PPEs or were unsure how to use their own. However, only 41.01% of the respondents bought flu medication in the past 6 months. The results of this research are consistent with those of earlier ones (Hope et al., 2011; Wong et al., 2008). Despite the chance of contracting an illness, nurses’ readiness to do their duties in the event of a pandemic shows a strong commitment to patient care (Hope et al., 2011).
Finally, none indicated demographic characteristics were associated with nurses’ worries and readiness for COVID-19. However, there was a substantial correlation between the factors of age group and job title and assessments of how the epidemic affected their personal and professional life. This discovery supports the findings of a prior investigation on pandemics (Balicer et al., 2006).
Strengths and Limitations
Only the nurses in the acute health care context, in Riyadh, Saudi Arabia, were included in this study. Cross-sectional surveys with self-administered questionnaires, like the one employed here, have limitations regarding recollection, framing, and rating bias. One should also be aware that the data in this study are self-reported and, to some degree, rely on the honesty and recollection of the participants. It is advised that more studies be done to generalize the results using a broader sample of nurses working at various hospitals around the KSA. In addition, medical professionals such as pharmacists and other HCPs may be included in future research. Despite these limitations, this study provides insight into the frontline nurses’ concerns, perceived impact, and preparedness during COVID-19.
Implications for Practice
Although there have been other studies on HCWs during a pandemic, this one focused on the concerns of the nurses, who are the front-line HCWs and play a crucial role in containing the disease. This also provided evidence of people's and organization's readiness during the pandemic. It is important for nurses to learn how to be resilient, supported, and ready to deal with a pandemic. In its research setting, the study provides baseline data that managers can use to develop system-wide initiatives to address the concerns of healthcare practitioners. Additionally, institutions—particularly those in the healthcare industry—need to be ready to handle such a disaster.
Conclusion
The COVID-19 epidemic has presented a significant challenge to mental health; the majority of study has concentrated on mental health disorders among healthcare personnel during this time. Nonetheless, this research adopted a distinct approach to investigate nurses’ concerns, perceived impact, and preparedness during COVID-19. This study discovered that despite their own and their institution's readiness, most nurses who answered the survey questionnaire had work- and nonwork-related worries. Most nurses who answered the poll thought that their jobs included a lot of personal danger. HCPs experience both physical and emotional tiredness in emergency circumstances. These worries were described as the dread of being sick and dealing with more duties and stress. The second wave of the viral outbreak coincided with the time our study was done, and our findings may shed light on the concerns, perceived impact, and preparedness of nurses working in an acute healthcare environment that served as a COVID center for the area during COVID-19. Therefore, measures must be put in place to minimize the overall impact of pandemics on nurses, as well as provisions for the mental support of nurses in pandemic preparedness. These interventions may include counseling, the supply of personal protective equipment, morale-boosting incentives, instruction in infection prevention, and environmental controls.
Footnotes
Acknowledgment
The authors express their sincere gratitude to the nurses who volunteered to participate and to the Research Center of King Fahad Medical City for providing essential research services and financial support for this study.
Ethical Considerations
Approval for the study was obtained from the Nursing Research Committee and the hospital's Institutional Review Board under IRB Log Number 20-183. Participation in the study was purely voluntary. Confidentiality and anonymity were maintained throughout the study.
Author Contribution Statement
All the authors contributed to the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received a grant from the King Fahad Medical City/Riyadh research center (Grant No. IRF 021-028).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.