
Abstract
Background
The coronavirus disease (COVID-19) pandemic imposed a major public health impact. Septic shock is one of the frequent complications encountered among critically ill COVID-19 patients, leading to poor healthcare outcomes. This study aimed at assessing the magnitude of septic shock and its associated factors.
Methods and materials
An institution-based cross-sectional study was conducted retrospectively on 242 randomly selected COVID-19 patients admitted to three Addis Ababa COVID-19 care centers from September 2020 to October 2021. Septic shock was defined as a Sequential Organ Failure Assessment (SOFA) score ≥2 points and persisting hypotension requiring vasopressors to maintain a mean arterial pressure of ≥65 mmHg despite adequate volume resuscitation. Variables in the bivariate analysis were fitted to multiple regression analysis to eliminate confounders and determine independent risk factors for septic shock. In the multivariable analysis, statistical significance was declared at P < .05
Results
The prevalence of septic shock was found to be 39.3% (95% confidence interval [CI]: 33.1, 45.7). Advanced age (≥60 years) [AOR = 7.9; 95% CI: 2.3, 26.8], intensive care unit stay above 7 days [AOR = 6.2; 95%CI: 2.1, 18.7], invasive ventilation [AOR = 10; 95% CI: 3, 37], and chronic obstructive pulmonary disease (COPD) [AOR = 18; 95% CI: 7, 45] were significantly associated with increased septic shock among COVID-19 patients. Meanwhile, diabetes [AOR = 0.24; 95% CI: 0.08, 0.71] and cardiovascular diseases [AOR = 0.17; 95% CI: 0.07, 0.44] were associated with a decrease risk of septic shock.
Conclusion
The prevalence of septic shock in critically ill COVID-19 patients was high and a major concern in this study, and it is independently associated with advanced age, prolonged stay in the intensive care unit, and COPD. Based on these findings, healthcare professionals should closely monitor and manage patients with COVID-19 who have a history of COPD, are older, or prolonged intensive care unit (ICU) stays to prevent septic shock and improve patient outcomes.
Introduction
The coronavirus disease (COVID-19) pandemic that ensued from the novel coronavirus outbreak in December 2019 induced rapid changes in the healthcare environment (Kim et al., 2022; Shigute et al., 2020). It gradually became a global health crisis due to a rapid increase in confirmed cases worldwide. World Health Organization (WHO) reported more than 469.3 million confirmed cases and 6.1 million deaths because of COVID-19 worldwide in March 2022 (Agarwal & Reed, 2021). World Health Organization reported 11,453,505 confirmed cases and 252,449 deaths of COVID-19 in 55 African countries on April 15, 2022 (WHO, 2022). According to the WHO report, Ethiopia recorded 470,232 coronavirus cases and 7,509 deaths on April 9, 2022 (WHO, 2022). Sepsis and septic shock are associated with high mortality and morbidity in developing countries (Dünser et al., 2006). Even with the declining trends of sepsis in developed countries, it is still a leading cause of non-cardiac death in critically ill patients (Hotchkiss & Karl, 2003; Martin et al., 2003; Vincent et al., 2009). Existing evidence showed that the mortality rate of critically ill COVID-19 patients with septic shock was higher than non-COVID-19 patients admitted to the intensive care unit (ICU) with septic shock (Heubner et al., 2022).
Based on the sepsis-3 consensus, sepsis is defined as an acute change in total sequential organ failure assessment (SOFA) score of ≥2 points secondary to infectious causes (Dugar et al., 2020; Singer et al., 2016). Septic shock occurs in a subset of patients with sepsis. Septic shock is defined by a Sequential Organ Failure Assessment (SOFA) or quick Sequential Organ Failure Assessment qSOFA score ≥2 points and persisting hypotension requiring vasopressors to maintain a mean arterial pressure of ≥65 mmHg and a serum lactate level greater than 2 mmol/L (18 mg/dL) despite adequate volume resuscitation of 30 mL/kg bolus of crystalloids (Alhazzani et al., 2021; Dugar et al., 2020; Singer et al., 2016). Although the exact pathophysiology of septic shock among COVID-19 patients is not explained, it is hypothesized to be linked to the over-expression of pro-inflammatory cytokines, which is triggered by activation of nuclear factor-kappa B activation as a primary response to infection (Cecconi et al., 2028; Faix, 2013; Li et al., 2020). The administration of empiric antibiotics in the absence of bacterial infection could lead to the formation of inflammatory storms either directly by enhancing cytokine secretion or indirectly by triggering the release of gut endotoxins (Bellinvia et al., 2020; Hantoushzadeh et al., 2020; Rogers et al., 1985).
Even though developed countries have access to infrastructure for advanced management of septic shock, the mortality rate among patients with COVID-19 has not been encouraging, and it may worsen in countries with limited resources and weak health infrastructure (Lakoh et al., 2020). A study conducted in South Korea showed that the mortality rate of septic shock increased after the COVID-19 pandemic (24.8–35.8%) (Kim et al., 2022). The study conducted at the University of Sierra Leone showed the mortality rate among the study participants was 29.8% (Lakoh et al., 2020).
Consequently, septic shock is associated with negative health outcomes and increased complications including acute kidney injury (Olanipekun et al., 2022; Raza et al., 2020; Zarbock et al., 2014), thromboembolic complications (Chang, 2019; Tufan et al., 2021), and multiorgan failure (Birhanu et al., 2022; Hassanein et al., 2020), which in turn increases demand for mechanical ventilation (Olanipekun et al., 2022), hemodialysis and prolonged Intensive Care Unit stay up to death (Al Mutair et al., 2021; Chen et al., 2022; Heubner et al., 2022). Management of septic shock could also result in increased healthcare costs (McBride et al., 2019; Thomas et al., 2022; Van den Berg et al., 2022) because it requires high-cost resources in terms of manpower, space, medications, and equipment.
Review of Literature
Globally the prevalence of septic shock among non-COVID-19 patients was 11 per 100,000 (Jawad et al., 2012). The study in Lisbon, Portugal showed that the prevalence of septic shock in COVID-19 patients was 33% (Cidade et al., 2021). The scoping review of research conducted at the University of Sierra Leone College of Medicine and Allied Health Sciences revealed that the prevalence of septic shock ranges from 4% to 28.9% (Lakoh et al., 2020). A previous study conducted in Mosco revealed that septic shock was reported in about 19.9% of COVID-19-confirmed patients (Glybochko et al., 2021). The prevalence of septic shock among non-COVID-19 patients in Addis Ababa, Ethiopia was 26.5% (Mulatu et al., 2021).
Preliminary studies documented several factors that were associated with an increased prevalence of septic shock among COVID-19 patients admitted to the intensive care unit (ICU). These include patient age, comorbidities (coronary heart disease, atrial fibrillation, type 2 diabetes, chronic obstructive pulmonary disease [COPD], and malignant tumors), mechanical ventilation time, and hospital and ICU stay (Glybochko et al., 2021; Silva et al., 2022; Yao et al., 2021).
Studies examining the occurrence, and variables associated with septic shock are scarce yet the the devastating health consequences that septic shock causes in COVID-19 patients. The researchers were unable to find any published or unpublished studies that addressed this topic of interest among COVID-19 patients in Ethiopia. Therefore, the purpose of this study was to determine the prevalence of septic shock in COVID-19 patients as well as its associated factors.
Methods and Materials
Study Area and Period
The study was conducted in Addis Ababa COVID-19 centers from September 2020 to October 2021. There are three COVID-19 care centers in Addis Ababa, Ethiopia (Millennium COVID-19 Care Center, Eka Kotebe Hospital, and Field Hospital). Millennium COVID-19 care center was the largest care center in terms of both capacity (with greater than 1,000 inpatient beds) and equipment. Eka Kotebe Hospital has 600 beds, including 16 ICU beds. In the Field, a hospital was established with the help of the World Health Organization for temporary use during the COVID-19 pandemic. It had served more than 200 patients and had about 20 ICU beds. The study was conducted from September 2020 to October 2021.
Study Design
An institution-based retrospective cross-sectional study was conducted.
Source of Population
All COVID-19 patients admitted to the ICU settings of the Addis Ababa COVID-19 care centers were considered the source population.
Study Population
All patients with age greater than or equal to 18 years old and all recordings of critically ill COVID-19 patients admitted to the ICU settings of Addis Ababa COVID-19 care centers were the study population.
Inclusion Criteria
All patients with age greater than or equal to 18 years old and with complete recordings were included.
Exclusion Criteria
All ICU patients who had incomplete data were excluded.
Sample Size Determination and Sampling Technique
The required sample size was determined using the single population proportion formula by taking the following assumptions: prevalence of septic shock = 20% from the previous study conducted in China (Zhou et al., 2020), 95% confidence level (Z = 1.96), and 5% margin of error (d), which yields 242. After adding 5% of the sample size for the non-response rate, the calculated sample size was 254.
Sampling Techniques
A total of 1,423 patients were admitted to the ICU of all centers (722 in the Millennium, 423 in the Eka Kotebe Hospital and 278 in the Field Hospital) during the study period. The calculated sample size was proportionally allocated to each hospital based on the total number of ICU registries (144 charts from Millennium, 87 charts from Eka Kotebe Hospital, and 42 charts from Field Hospital). Then, the samples were selected using a systematic random sampling technique by selecting every other case. The first case was selected by using the lottery method (Figure 1).

Flow chart showing sampling procedure of COVID-19 patients with septic shock at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).
Operational Definitions
Data Collection Tools and Quality Assurance
The data collection checklist was designed from previous literature (Glybochko et al., 2021; Silva et al., 2022). It was formulated in English and validated by intensivists and critical care seniors. Data were collected using a pretested and structured checklist. All available relevant data sources including the COVID-19 registry, triage report, patient charts, and reporting formats were used to collect the data. The checklist encompasses questions to assess sociodemographic characteristics, comorbidities, laboratory investigation findings, complications, and management given at the center. One week before the data collection, the checklist was pre-tested on 5% (13) of the samples. A 1-day training was given for five data collectors (B.Sc. nurses) and two supervisors (M.Sc. nurses). Data were evaluated and crosschecked for completeness daily.
Data Processing and Analysis
Data were cleaned, coded, and entered using Epi data version 4.4, and it was exported to SPSS version 25 for analysis. Cross-tabulation was done for the exploration of the data, to clear missing values, and to determine the number of expected events per cell. Binary logistic regression was used for the analysis of the data. Model fitness was checked using the Hosmer and Lemeshow test (P = .872). Variables with a P-value of .2 in the bi-variable analysis were identified and fitted to the final model to identify the independent effects of each variable on the outcome variable. An adjusted odds ratio (aOR) with 95% confidence intervals (CIs) was computed to identify the presence and strength of associations, and statistical significance was declared at P < .05.
Ethical Consideration
Ethical clearance was obtained from Saint Paulo's Millennium Medical Hospital and Medical College institutional review board (IRB) (protocol number = PM23/799). Permission for data collection was received from the executive director and clinical director. Patient consent was waived since the study was conducted retrospectively from patients’ charts. The responsible bodies at each intensive care unit and liaison office were informed about the objective of the study. The study was conducted per the declaration of Helsinki. Confidentiality was assured by data coding and aggregate reporting.
Results
Two hundred and fifty-four charts of patients with COVID-19 patients from September 2020 to October 2021 were reviewed. Of these, 242 fulfilled the inclusion criteria.
Socio-Demographic Characteristics
The study findings showed that 134 (55.4%) study participants were males. Moreover, the mean age of patients was 60 years (SD = 15 years). One-hundred and forty (57.9%) of the patients were aged greater than 60 years. On the other hand, 78.1% of the study participants reside in urban areas (Table 1).
Distribution of Sociodemographic Characteristics of COVID-19 Patients with Septic Shock at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).

Description of Chronic Medical Illness among COVID-19 Patients
The study findings revealed that 189 (78.1%) patients had at least one comorbidity. Among those, 65 (34.4%) had septic shock. Conversely, 20.4% (30/147) of patients without comorbidities developed septic shock. On the other hand, the commonest comorbidities recorded were hypertension (44.6%), diabetes mellitus (73.6%), and congestive heart failure (62.8%). Among patients with comorbidities, almost half of them had two or more comorbidities (Table 2).
Distribution of Chronic Medical Illnesses among COVID-19 Patients with Septic Shock at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).
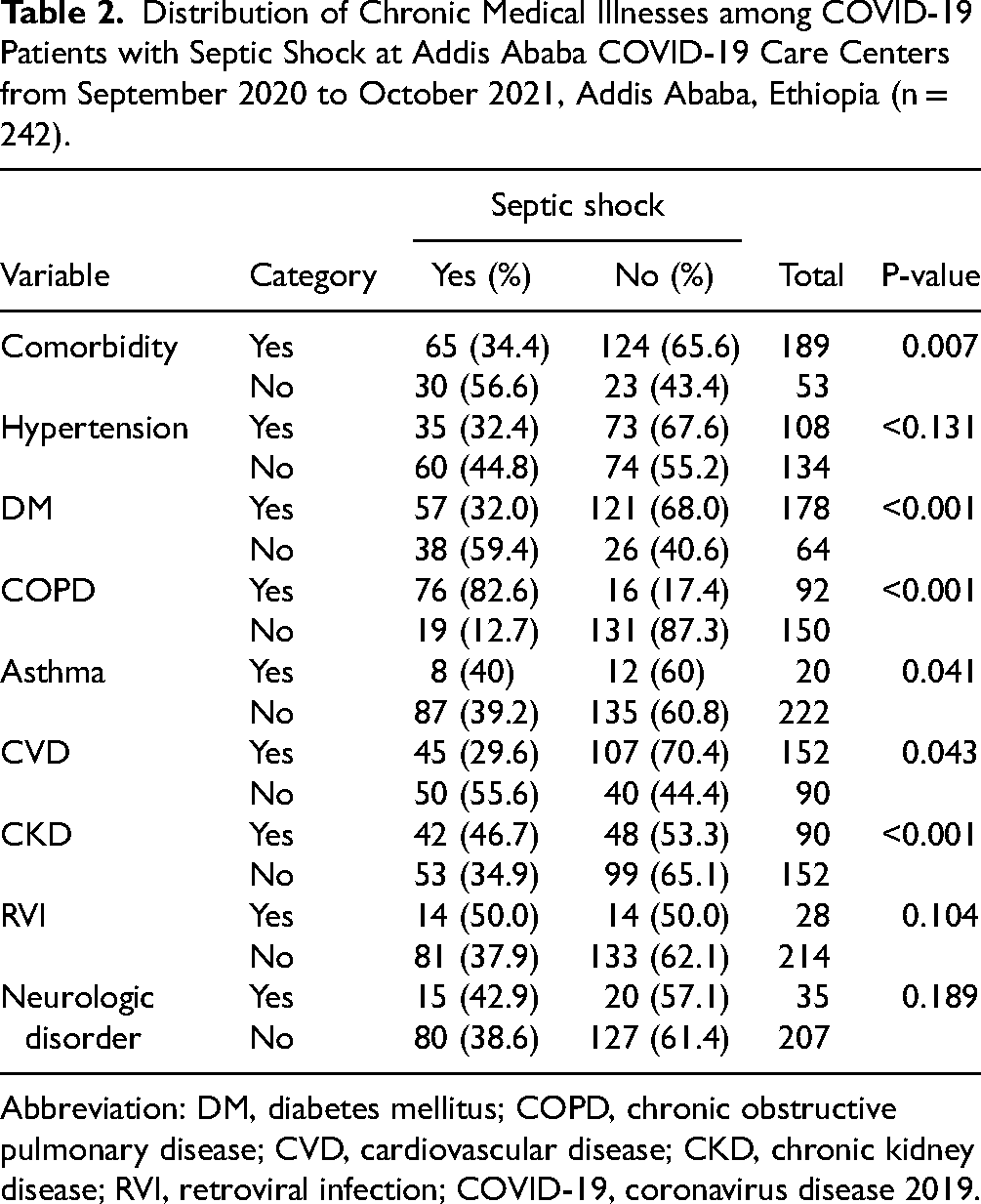
Abbreviation: DM, diabetes mellitus; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; CKD, chronic kidney disease; RVI, retroviral infection; COVID-19, coronavirus disease 2019.
Baseline Laboratory Findings Among COVID-19 Patients With Septic Shock
Regarding the baseline laboratory findings, the most frequently recognized abnormalities in this study were leukocytosis (50.4%), hyponatremia (43.8%), hyperkalemia (27.3%), thrombocytopenia (59.1%), and hyperbilirubinemia (81%). Moreover, 99 (41%) patients were identified with an elevated serum creatinine clearance (Cr > 1.2 mg/dL) at admission (Table 3).
Distribution of Baseline Laboratory Findings among COVID-19 Patients with Septic Shock at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).

Abbreviation ICU-intensive care unit, WBC-White blood cells, BUN-blood urea nitrogen, COVID-19-coronavirus disease 2019.
Prevalence of Septic Shock and Management Intervention
Out of 242 study participants, 95 (39.3%) were diagnosed with septic shock. Of those, 80% were admitted with severe or critical COVID-19 illness. According to the study result, the majority of patients (50.4%) had an infection of the chest focus. Furthermore, almost half of the study participants (117/242) had new-onset organ failure. Of those, 37.6%, 31.6%, 13.7%, and 12% had respiratory failure, acute kidney failure, acute hepatic failure, and cardiac failure respectively. More than three-fourths of patients with septic shock received vasopressor therapy such as noradrenaline, adrenaline, dopamine, and dobutamine
Presentation of Clinical and Management-Related Factors among COVID-19 Patients with Septic Shock at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).

Factors Associated With the Prevalence of Septic Shock
In the bivariate logistic regression analysis, sex, age, comorbidities (HTN, DM, CVD, COPD, RVI, and CKD), ICU stay, severity, and invasive ventilation had a P-value of less than .20 and transferred to the final model for confounder adjustment.
According to the result of multivariable analysis, after controlling other factors (confounders), age, ICU stays, comorbidities (DM, COPD, and CVD) and intubation had a statistically significant association with the magnitude of septic shock with COVID-19 patients.
COVID-19 patients aged greater than or equal to 60 years were eight times more likely to develop septic shock compared to patients aged less than 60 years (AOR = 7.9; 95% CI: 2.3, 26.8). COVID-19 patients who stayed in ICU for longer than 1 week were six times more likely to acquire septic shock compared to their counterparts (AOR = 6.2; 95% CI: 2.1, 18.7). The odds of acquiring septic shock among intubated patients were ten times higher than those who were not intubated (AOR = 10; 95% CI: 3.0, 37). COVID-19 patients diagnosed with COPD were 18 times at increased risk of septic shock than their counterparts (AOR = 18; 95% CI: 7, 45). Diabetic patients were 76% less likely to have septic shock compared to their counterparts (AOR = 0.24; 95% CI 0.08, 0.71). COVID-19 patients with cardiovascular diseases were 83% less likely to develop septic shock compared to patients without CVD (AOR = 0.17; 95% CI: 0.07, 0.44) (Table 5).
Bivariate and Multivariable Analysis for Factors of Septic Shock among COVID-19 Patients at Addis Ababa COVID-19 Care Centers from September 2020 to October 2021, Addis Ababa, Ethiopia (n = 242).

Abbreviation: cOR, crude odds ratio; aOR, adjusted odds ratio; CI, confidence interval; HTN, hypertension; DM, diabetes mellitus; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; CKD, chronic kidney disease; RVI, retroviral infection; ICU, intensive care unit; COVID-19, coronavirus disease 2019.
Discussion
This study was used to assess the prevalence of septic shock and the associated factors among ICU patients evaluated at the COVID-19 centers in Addis Ababa, Ethiopia. According to this study's findings, the prevalence of septic shock was 39.3% (95% CI: 33.1, 45.7). Age, comorbidities (COPD, DM, and CVD), ICU stay, and intubation status were identified as associated risk factors of septic shock.
This finding was comparable to the reports of a study conducted in Portugal, Lisbon, in which 33% of patients had septic shock (Cidade et al., 2021). The increment in septic shock among COVID-19 patients could be due to the prolonged stay in the ICU. COVID-19 patients admitted for longer periods in the ICU require prolonged respiratory support and ICU care. Therefore, patients might be exposed to infection and develop septic shock (Cidade et al., 2021; Kim et al., 2022). However, it was higher than the figures documented in Sierra Leone (28.9%) (Lakoh et al., 2020) and Shenzhen, China (25.7%) (Yao et al., 2021). The difference might be due to the short study period and small sample sizes applied by the previous studies.
COVID-19 patients above the age of 60 years were eight times more likely to develop septic shock compared to patients aged less than 60 years (AOR = 7.9; 95% CI: 2.3, 26.8). This agreed with the study conducted in Sierra Leone and Moscow, Russia (Glybochko et al., 2021; Lakoh et al., 2020). A possible justification could be the diminished immune defence mechanism with advanced age. Besides, the elderly are at higher risk of acquiring comorbid medical conditions that will, in turn, increase the risk of infection progression (Zhao et al., 2019).
COVID-19 patients who stayed in ICU for longer than one week were six times more likely to acquire septic shock compared to their counterparts (AOR = 6.2; 95%CI: 2.1, 18.7). This finding was conformable to the study conducted in Lisbon, Portugal, and South Korea (Cidade et al., 2021; Kim et al., 2022). With prolonged hospital stays, especially in the ICU settings, the chance of acquiring septic shock could be high since patients are critically ill (suppressed immunity), making them prone to complications. Furthermore, the risk of hospital-acquired infections may also increase with prolonged ICU stays (Ali et al., 2018).
The odds of acquiring septic shock among intubated patients were ten times elevated compared with those who were not intubated (AOR = 10; 95% CI: 3.0, 37). Earlier studies evidenced that invasive ventilation remains a high-risk procedure for the development of sepsis and septic shock in critically ill patients. Invasive ventilation during the COVID-19 era was frequently associated with clinical deterioration and cardiovascular failure (Darreau et al., 2020; Yang et al., 2021).
COVID-19 patients diagnosed with COPD were 18 times at increased risk of septic shock than their counterparts (AOR = 18; 95% CI: 7, 45). COPD patients require mechanical ventilation more frequently and have longer ICU stays. Consequently, these could be associated with a higher incidence of bacterial infection and septic shock (Rello et al., 2006).
Diabetic patients were 76% less likely to have septic shock compared to their counterparts (AOR = 0.24; 95% CI: 0.08, 0.71). This result contradicts the findings of a study conducted in Moscow, Russia that reported patients who had comorbidities were at higher risk of developing septic shock than those without comorbidities (Glybochko et al., 2021). The probable justification might be due to the devastating effect of stress hyperglycemia among non-diabetic patients diagnosed with septic shock, which could outweigh the effect of diabetes on septic shock. The effect of insulin therapy on pro-inflammatory cytokines could also provide protection. Studies documented that insulin plays an anti-inflammatory role by preventing immune system over-activation (Honiden & Gong, 2009; Schuetz et al., 2011). To support this idea, all diabetic patients included in our study received insulin therapy. Furthermore, an indolent inflammation due to diabetes differs from an inflammatory response resulting from sepsis (Goldfine et al., 2011).
COVID-19 patients with cardiovascular diseases were 83% less likely to develop septic shock compared to patients without CVD (AOR = 0.17; 95% CI: 0.07, 0.44). This finding was similar to the study conducted in Moscow, Russia (Glybochko et al., 2021). CVD is one of the factors that compromise the immune system. This could be because of the prompt attention given to patients with comorbid conditions such as CVD, which could enable early detection and management before the occurrence of complications like septic shock. Conversely, patients without comorbidities are often recognized late in the disease course mostly after acquiring advanced disease, and even after complications developed. Even the COVID-19 management guideline recommended the presence of pre-existing diseases such as DM and CVD to be used as severity criteria during the COVID-19 severity classification; which means no mild classification was applicable for such patients. This could contribute to halting the possible complications timely. Otherwise, it is undisputed that patients with CVD are at an increased risk of infection and are highly prone to septic shock (Arnautovic et al., 2018).
Strength and Limitations
Despite the study forwarding relevant points, it has certain limitations. First, serum lactate level was not considered in the definition of septic shock in this study. Second, the effect of some inflammatory markers such as
Implications for Practice
By recognizing and addressing risk factors such as advanced age, prolonged ICU stay, invasive mechanical ventilation, and COPD early on, healthcare professionals can potentially improve patient outcomes and reduce the incidence of septic shock. This has significant implications for health policy and the provision of high-quality ICU care, as it may lead to the development of targeted interventions and protocols aimed at preventing and managing septic shock in COVID-19 patients. Furthermore, the study's insights have to transform clinical practice by emphasizing the need for proactive risk factors assessment and management, ultimately enhancing patient care across critical care settings. By integrating these findings into clinical guidelines and protocols, healthcare providers can work towards improving the overall management of septic shock in COVID-19 patients.
Conclusion
The study findings revealed a higher prevalence of septic shock among COVID-19 patients in the ICU. Receiving invasive mechanical ventilation, prolonged ICU stay, advanced age, and COPDs were associated with an increased risk of septic shock. Conversely, the presence of diabetes and CVD was associated with a minimal risk of acquiring septic shock. Hence, it is essential to put specific strategies to manage and halt the identified factors to minimize the prevalence of septic shock among COVID-19 patients.
Footnotes
Acknowledgements
Data collectors, supervisors, staff, and administrators were appreciated for providing the necessary preliminary information. The authors would also like to thank the Ethiopian Ministry of Health and Saint Paulos Millennium Medical College for pursuing this chance.
Abbreviations
Authors’ Contributions
KGT generated the concept and developed the proposal. MGT, MSM, & TMA designed the study and developed the data extraction tool. KGT, TMA, AHS, MAM, EGM, WCZ & HAB participated in data collection and supervision. MSM and TMA performed the statistical analysis, interpreted the findings, and drafted the manuscript. MGT, MSM, & KGT edited and formatted the manuscript for publication. All the authors read, critically revised, and approved the final version of the manuscript. Finally, all the contributors agreed to be equally accountable for every aspect of the work.
Data Sharing Statement
Additional data that support the findings of this study are accessible upon reasonable and legal request and can be shared.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.