
Abstract
Background
Sleep is essential for physiologic function and mental health stability, which promotes recovery from severe illness. However, poor sleep quality is a common complaint in the critical care unit. In intensive care units (ICUs), physical aspects of patient care are often prioritized over humanized aspects of care.
Objective
To assess the level of sleep quality and its associated factors among adult patients admitted to critical care units in Addis Ababa.
Method
A cross-sectional study design was conducted in three selected public hospitals. Over 4 months of the period we consecutively collected data among ICU patients, who were oriented to time, person, and place on the day of discharge. A modified freedman self-reporting and personal characteristics questionnaire was used. The data were entered into Epi-data version 4.4.6.0 and analyzed with SPSS 25. Both bivariate and multivariate analyses were conducted. A P-value of <.05 indicated statistical significance, and an adjusted odds ratio with a 95% confidence range was used to show the strength of the association.
Result
Of the total 102 participants, 57.8% of ICU patients had poor sleep quality. Four variables were identified as significant associations with poor sleep quality among ICU patients. These included elderly age (adjusted odd ratio [AOR] = 3.4; 95% confidence interval [CI]: 1.42, 7.93), comorbidity (AOR = 2.5; 95% CI: 1.24, 9.03), light exposure (AOR = 2.0; 95% CI: 1.16, 5.11), and the monitor's alarm (AOR = 1.7; 95% CI: 1.04, 8.23) were identified as significant association factors for poor sleep quality.
Conclusion and recommendation
Poor sleep quality was a major concern for ICU patients in this study. Elderly individuals, those with comorbidity, light exposure, and monitor alarms have been associated with poor sleep quality. Reducing nighttime light and adjusting alarm settings may significantly improve sleep quality, resulting in better recovery results in critical care units.
Introduction
Sleep is a cyclical state characterized by temporary unconsciousness, during which cognitive and sensory links to external stimuli are greatly decreased. It is made up of alternating phases of nonrapid eye movement and rapid eye movement sleep, which normally occur four to six times every night, with each cycle lasting around 90‒100 minutes. Overall, adults require approximately 7‒8 hours of sleep to maintain optimal health and functioning (Grimm, 2020; Patel et al., 2024).
An intensive care unit (ICU) is an extremely complicated environment in which critically ill patients are handled with intensive care monitoring and invasive devices (Elliott et al., 2011). However, poor sleep quality is a common complaint in critical care units (Brito et al., 2020; Dorsch et al., 2019). Patients also experience sleep disruption after they have been transferred from an ICU to a recovery room (Altman et al., 2017). Sleep disturbances substantially influence patients’ recovery from chronic diseases, especially in critical care settings. Disrupted sleep is associated with a variety of negative effects, including immunological dysfunction, decreased wound healing, and higher susceptibility to infections, which can impede recovery processes (Altman et al., 2017; Garbarino et al., 2021). Furthermore, sleep disturbance has an impact on the body functions that are critical to returning to a normal health state, including respiratory muscle weakness, cardiovascular effects resulting in hypertension, heart failure, and stroke, and hormonal changes resulting in insulin resistance in diabetics (Delaney et al., 2015; During & Kawai, 2017; Singh et al., 2022).
Review of Literature
A systematic review showed that about 66% of ICU patients experience poor sleep quality during their ICU stay (Shih et al., 2023). Studies revealed that the prevalence of poor sleep quality among ICU patients was significantly higher in different settings, in Australia 64% (Bihari et al., 2012), Iran 55% (Adib-Hajbaghery et al., 2012), Poland 50.1% (Lewandowska et al., 2019), India, 47% (Naik et al., 2018), and China 46.1% (Zhang et al., 2013). Furthermore, very little research has been conducted in Africa; a study of ICU patients in South Africa found that 70.6% of participants had poor sleep quality (Ehlers et al., 2013). Furthermore, in Egypt, a study conducted using the Freedman questionnaire found that 48% of ICU patients reported poor sleep quality (Magdy et al., 2019). Poor sleep quality is a significant public health concern in Ethiopia (Abate et al., 2024; Edmealem et al., 2024). However, there is limited data on sleep quality among critical care unit patients in Ethiopia.
Previous studies identified several factors that have been associated with poor sleep quality among critical care unit patients. These include elderly age, gender, environmental noise, heart monitoring alarms, light exposure, nursing care activities, pain and discomfort, stress and anxiety, frequency of admission, procedure and intervention, severity of illness, medication, bedside phone calling, medical conditions, and mechanical ventilation (Adell et al., 2021; Ahn et al., 2023; Bihari et al., 2012; Ding et al., 2017; Silva et al., 2024; Sundstrøm et al., 2021).
To our knowledge, no adequate studies have been undertaken to evaluate sleep quality among critical care unit patients in Addis Ababa. Hence, this study aimed to assess the level of sleep quality and identify its associated factors among adult patients in critical care units at selected public hospitals. By identifying key factors affecting sleep, this study aimed to lay a framework for encouraging preventative measures to improve patient recovery and general health. Improved sleep care may significantly contribute to better clinical outcomes, increasing recovery.
Methods
Study Design
A cross-sectional study was conducted among ICU patients who were admitted to ICUs. The study was conducted in the ICUs of selected public hospitals in Addis Ababa, the capital city of Ethiopia. The city has about 12 public hospitals. For this study, three public hospitals with advanced ICU services, large patient flow, and well-recorded systems were purposefully selected. These hospitals included the Alert Comprehensive specialized Hospital, Tikur Anbesa Specialized Hospital, and Saint Peter Specialized Hospital. The study period was from February 1 to June 30, 2020, by administering a self-rating Freedman sleep quality assessment questionnaire among ICU patients who were admitted to the selected public hospitals in Addis Ababa. The data were collected prospectively for 4 months.
Sample
All adult patients who were admitted to ICUs of public hospitals in Addis Ababa were included in the sample.
Study Population
The study included all patients admitted to ICUs from February 1 to June 30, 2020, at the selected public hospitals in Addis Ababa. A convenience sampling technique was used to recruit the participants.
Eligibility Criteria
Inclusion
This study included adult ICU patients (aged 18 and above) who had been hospitalized for at least two nights and were completely oriented to location, person, and time. This criterion ensured that participants received adequate exposure to the ICU setting, allowing for a more realistic assessment of how protracted stays affect sleep quality and mental orientation. By mandating this minimal stay, the study may be able to better capture the impacts of ICU ambient elements such as noise, light, and frequent medical interventions, all of which are well-documented disruptors of sleep patterns in critical care settings. Limiting the study to patients discharged between February 1 and May 30, 2020 ensures a consistent cohort that captures data relevant to that time period while avoiding variation caused by shifts in ICU procedures or seasonal changes.
Exclusion
Individuals with moderate-to-severe dementia, who had previous sleep disorders, did not speak the Amharic language, and were transferred to other facilities while unconscious were excluded from the study.
Sample Size Determination
The required sample size was determined using the single population proportion formula by taking the following assumptions: estimating proportion = 50%, 95% confidence level (Z = 1.96), and 9.7% margin of error (d) due to time and budget constraints, which yields 102. Convenience sampling was used in selecting patients who are easily accessible based on the inclusion criteria until fulfill the required sample size. This approach makes sure that every eligible patient is considered, resulting in a comprehensive and representative cohort for the study.
Sampling Technique
Of the 297 total patients admitted to the ICU during the data collection period, 102 were included by the convenient sampling technique because they met the inclusion criteria and agreed to participate in the study after receiving informed consent from the data collectors of each ICU. Study participants were screened every morning from Monday to Friday, starting from 8:30 to 12:30 a.m., at each ICU at the time of discharge (Figure 1).

Schematic representation of ICU patients’ screening, enrollment, and participant in Freedman sleep quality questionnaire performed at the three ICUs in Addis Ababa, Ethiopia, 2020. ICU = intensive care unit.
Operational Definition
The operational definition of the Freedman sleep quality scale was used to categorize as good and poor sleep quality. This questionnaire assesses sleep quality and its disruptions among ICU patients. Patients rated their sleep on a 1 to 10 scale (1 = poor, 10 = excellent) both at home and in the ICU (Freedman et al., 1999). This assessment was repeated throughout their ICU stay. Daytime sleepiness was also rated on a 1 to 10 scale (1 = unable to stay awake, 10 = fully alert). Environmental factors were evaluated for their impact on sleep disruption. These included noise, light, nursing interventions, diagnostic tests, vital sign checks, blood draws, and medication administration. Specific ICU noises, such as telemetry alarms, ventilator sounds, pulse oximetry, staff communications, Intravenous pump alarms, suctioning, doctor's beepers, and TV/phone noise, were also assessed for their disruptive effects. Finally, sleep quality can be considered good if they report being satisfied with their sleep in the previous night. This is confirmed by a Freedman Sleep Quality Scale score of 7 or above (Freedman et al., 1999). A patient is considered to have poor sleep quality if they report being dissatisfied with their sleep the night before. This is confirmed by a Freedman Sleep Quality Scale score of less than 7 (Bihari et al., 2012; Freedman et al., 1999).
Data Collection Tools
The data was collected using a structured questionnaire based on a modified version of the Freedman sleep quality questionnaire (Freedman et al., 1999). Data was collected using a pretested, self-administered questionnaire and chart review (for clinically related variables). It was a self-rated scale with four major sections: demographics, clinical features, sleep quality components, and sleep-disrupting factors. All sleep quality questions in the questionnaire were graded on a 10-point scale from 1 (bad) to 10 (excellent), as was daytime sleepiness (1 = unable to remain awake; 10 = fully alert) during the duration of their ICU stay, as well as on the first day, midway, and end of their stay in the ICU. On a 10-point scale, participants rated many environmental factors that impact their sleep quality as disrupted (1 = no disruption, 10 = significant disturbance). The tool was verified with Cronbach's alpha global value of .933 (Adell et al., 2020).
Data Quality Control
Predata collecting training was provided for three BSc nurse data collectors, and adequately designed data collection equipment was constructed to ensure data quality. Three BSc nurses were assigned from each ICU to distribute the questionnaire daily for ICU patients. A pilot study of 15 questionnaires was done at Saint Paul's Millennium Medical College before 1 week of actual data collection. The primary investigator ensured that all data was complete on each data-collecting day.
Data Process and Analysis
The data was checked for completeness, cleaned, coded, and imported into Epi-Data Manager (version 4.4.6). The data was then analyzed with SPSS (version 25). The study variables were reported with descriptive statistics (frequency and percentage) for categorical variables and summary statistics (mean and standard deviation) for continuous variables.
We used a binary logistic regression to determine the association between each independent variable and the dependent variable. Adjusting for potential confounders, the multivariate analysis included variables with a P <.25 at a 95% confidence level from the bivariate analysis. We used the standard error to conduct a multicolinearity test to determine the linear connection between independent variables. Multicolinearity was checked using variable inflation factors, with a mean value of 1.32. We used the Hosmer–Lemeshow goodness-of-fit test to check model fit. The omnibus test was significant (P <.001), which showed the model was fitted. During the multivariate analysis, we evaluated the adjusted odds ratio with a 95% confidence interval (CI) to find associated factors for poor sleep quality among ICU patients. Variables with a P <.05 and a 95% CI were shown to be significantly associated with poor sleep quality. The final data was presented as text, tables, and figures.
Results
A total of 102 patients were eligible and participated in the study (Figure 1). The participants’ mean age was 43.3 (SD ± 13.7) years. About 53% of the study participants were female, and 60.8% were under 60 years old. Regarding the residence of participants, 62.7% of the participants were urban, and the remaining 37.3% were rural. Of the total participants, nearly 54% of them were married, and only 30% of the study participants graduated from college. Furthermore, about 32% of the study participants’ occupations were merchants (Table 1).
Distribution of sociodemographic characteristics among ICU patients of public hospitals in Addis Ababa, Ethiopia, 2020.

Note. ICU = intensive care unit.
Sociodemographic Characteristics
Clinical-Related Characteristics
In this study, the mean length of stay in the ICU was 16.2 days + 3.27 SD. Almost one-third of respondents had a history of ICU hospitalization, with 66.7% experiencing extended stays (≥15 days). Only 21.6% of the study participants were brought to the ICU as a result of trauma, whereas 60% were hospitalized for medical reasons. Furthermore, 33.4% of the ICU patients had at least one comorbidity, with cardiac disease, diabetes, and hypertension being the most common. Furthermore, 33.4% of ICU patients had at least one comorbidity, with the most common being cardiac disease, diabetes mellitus, and hypertension (22.5%, 18.6%, and 14.7%, respectively). About 40.2% of the study participants received a mechanical ventilation during ICU stays (Table 2).
Distribution of clinical variables among ICU patients of public hospitals in Addis Ababa, Ethiopia, 2020.

Note. ICU = intensive care unit.
Environmental and Physiological-Related Factors
Based on the Freedman sleep quality scale on a 10-point scale, participants rated many environmental factors that impact their sleep quality as disrupted (1 = no disruption, 10 = significant disturbance). Accordingly, we categorized the 10-point scale into two categories: those who rated the score ≤5 on the Freedman sleep disruption factors were categorized as “no,” indicating it did not disrupt the sleep quality. In contrast, the ICU patients who rated >5 for the Freedman sleep disruption factors were categorized as “yes,” showing the factors significantly cause sleep disruption.
More than half (52%) of the participants rated the monitor alarm as a disrupting factor in sleep quality in the ICU. Nearly 30% of the participants reported that bedside phone calls disrupted sleep among ICU patients. The majority (57%) of the participants believed that talking was a significant cause of sleep quality. Furthermore, 37% of the participants also reported that doctors or nurses’ papers, pagers, and phone calls disrupted their sleep quality during their ICU stay. The most frequent causes of sleep disruption were light, pain, noise, and medication administration (71.6%, 63.7%, 61.8%, and 54.9%, respectively) (Table 3).
Distribution of noises and environmental factors that disrupt sleep quality of intensive care unit patients at public health in Addis Ababa, Ethiopia, 2020.

The most significant environmental-related self-reported factors affecting sleep quality among ICU patients were noise, pain, doctor/nurse activities, and light, with mean scores of 6.7, 5.6, 5.2, and 5.1, respectively (Figure 2). Furthermore, in terms of noise-related sleep disturbance factors, monitor alarms, talks, and phone calls were the most significant noise sources (Figure 3).

Mean patient perceptions of sleep-disrupting factors in adult ICU patients at public hospitals in Addis Ababa, Ethiopia, 2020. 1 = None significant and 10 = Significant sleep-disrupting factors. ICU = intensive care unit.
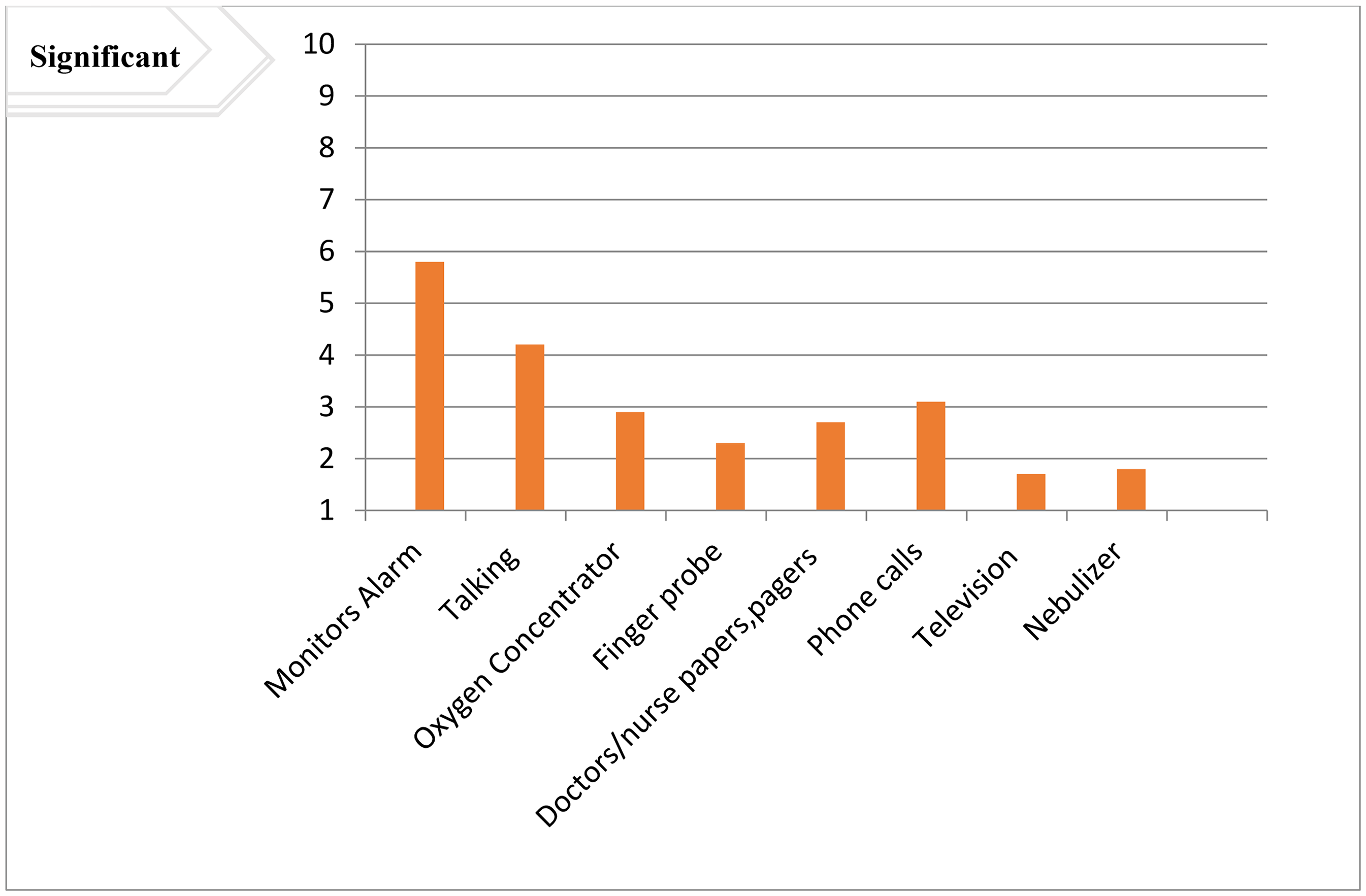
Mean patient perceptions of noise sleep-disrupting factors in adult ICU patients of public hospitals in Addis Ababa, Ethiopia, 2020. Noise disruptions are rated on a scale of 1 (no disruption) to 10 (significant sleep disruption). ICU = intensive care unit.
Prevalence of Sleep Quality
The study found that 57.8% of ICU patients reported poor sleep quality (95% CI: 48.4, 64.9). The majority of individuals, around 74.5%, reported satisfactory sleep quality at home. This showed that there was a substantial difference in sleep quality. The study found that sleep quality in the ICU was considerably worse than at home, with a mean score of 4.9 ± SD 1.2 (P = .002) (Figure 4).

Comparison of patients’ perceived sleep quality between home and intensive care unit in Addis Ababa, Ethiopia, 2020.
Risk Factors Associated with Poor Sleep Quality
In bivariable logistic regression analysis, factors were found to be statistically significant for poor sleep quality among ICU patients. These factors, including age, residence, previous ICU hospitalization, comorbidity, length of stay, mechanical ventilation, light, pain, anxiety, and monitor alarm, were candidates for multivariable logistic regression analysis, all variables with a P-value <.25. After accounting for potential confounders, four variables were identified as having statistically significant associations with poor sleep quality among ICU patients. These included elderly age, comorbidity, light exposure, and the monitor's alarm, which were found to have a significant association with ICU patients’ poor sleep quality (Table 4).
Bivariate and multivariate logistic regression analysis of patients admitted to intensive care units at public hospitals in Addis Ababa, Ethiopia, 2020 (n = 102).

Note. AOR = adjusted odd ratio; COR = crude odd ratio; ICU = intensive care unit; 95% CI = 95% confidence interval.
*Statistically significant.
Accordingly, the odds of poor sleep quality were three times higher among patients with an age greater than or equal to 60 years compared to those below 60 years (adjusted odd ratio [AOR] = 3.4; 95% CI: 1.42, 7.93). Patients who had at least one comorbidity were 2.5 times more likely to have poor sleep quality as compared to their counterparts (AOR = 2.5; 95% CI: 1.24, 9.03). The study participants who faced light exposure were two times more likely to experience poor sleep quality compared to their counterparts (AOR = 2.0; 95% CI: 1.16, 5.11). Furthermore, patients who believed the monitor alarm was the source of sleep disruption were 1.7 times more likely to have poor sleep quality than those who did not believe it was a disrupting factor (AOR = 1.7; 95% CI: 1.04, 8.23) (Table 4).
Discussion
This study assessed sleep quality and the associated factors among ICU patients at public hospitals of Addis Ababa, Ethiopia. According to this study's findings, 57.8% of the participants had poor sleep quality with (95% CI: 48.4, 64.9). Elderly age, comorbidity, light exposure, and the monitor's alarm were identified as associated factors of poor sleep quality among ICU patients.
The result of this study was comparable with that of a previous study in Iran, in which 55% of the ICU patients had poor sleep quality (Adib-Hajbaghery et al., 2012) and a study in Australia, 56% of ICU patients reported poor sleep quality (Martinez et al., 2021). The current study was also in line with a previous study in Poland, which reported that 50.1% of ICU patients experienced poor sleep quality (Lewandowska et al., 2019). However, the result of the current study was lower than that of a study conducted in South Africa, in which 70.6% of ICU patients reported poor sleep quality and this finding is also lower compared to the systematic and meta-analysis pooled prevalence of sleep disruption in the ICU patients, which reported 66% (Shih et al., 2023). This might be due to the difference in the short study period and the small sample size applied to the previous study (only 34 participants were included). Furthermore, the results of the current study were higher than those of the reported findings in China (46%; Zhang et al., 2013) and India (47%; Naik et al., 2018). This variation might be due to the small sample size and the difference in the study settings, and study population; the previous studies included the nurses’ point of view.
The ICU patients above the age or equal to 60 years were three times more likely to have poor sleep quality compared to patients under 60 years (AOR = 3.4; 95% CI: 1.42, 7.93). This finding was conformable to the study in Germany (Lemola & Richter, 2013) and north India (Naik et al., 2018). According to previous studies, people over 60 are more likely to have poor sleep quality than younger individuals (Corbo et al., 2023; Ryden & Alessi, 2022). A possible justification could be the increment of age is associated with hormonal changes that affect the sleep quality, including a reduction in melatonin production, which controls sleep cycles. This is supported by previous literature (Schlemmer et al., 2015).
The ICU patients who had at least one comorbidity were 2.5 times more likely to have poor sleep quality as compared to their counterparts (AOR = 2.5; 95% CI: 1.24, 9.03). This finding was in agreement with a previous study in Australia (Dagnew et al., 2024). Furthermore, a study in Tunisia found a high association between comorbidity and poor sleep quality (Moussa et al., 2023). This could be because patients with multiple comorbidities frequently take a variety of drugs, some of which might cause sleep disturbances. For example, many antidepressants or chronic pain drugs might cause daytime drowsiness and nighttime sleeplessness. Multiple health disorders might cause more stress and anxiety about one's health, making sleep more difficult. Worrying over controlling these situations might lead to racing thoughts and difficulties relaxing, making it hard to fall asleep (Dagnew et al., 2024; Novak & Lev-Ari, 2023).
The current study revealed that patients who faced light exposure were two times more likely to experience poor sleep quality compared to those with reducing light exposure (AOR = 2.0; 95% CI: 1.16, 5.11). This finding was also in line with the previous study conducted in Australia (Miranda-Ackerman et al., 2020; Siraji et al., 2023). The possible justification might be due to light has an important role in regulating the body's circadian rhythms, which control sleep and wake cycles. In the ICU, exposure to bright light, particularly at night, can cause misalignment of these rhythms, making it difficult to fall asleep and stay asleep.
Furthermore, patients who believed that monitor alarms were a source of sleep disturbance were 1.7 times more likely to experience poor sleep quality than those who did not identify alarms as a sleep-disturbing factor (AOR = 1.7; 95% CI: 1.04, 8.23). This finding contrasts a previous study conducted in Poland, which found no relationship between ventilator alarms and poor sleep, which patients rate as a sleep-disturbing factor. The variation might be due to the difference in the categorizing approach of the freedman self-rating on a 10-point scale for environmental factors. However, further research is needed to evaluate the relationship between monitor alarms and poor sleep quality among ICU patients. This study provides future researchers with baseline information, particularly in Ethiopia.
Limitation and Strength
Despite the relevance of this study's findings, which can contribute to improvements in the healthcare services in the ICU, it has notable limitations. The primary limitation is the data point is relatively small, which may restrict the generalizability of the results. Additionally, the absence of qualitative data to provide multiple perspectives further limits the depth of understanding. Another, limitation of this study was the COVID-19 pandemic, which caused disruptions in collecting data and limited access to participants since they were isolated. Nonetheless, these findings can serve as a valuable starting point for future, larger-scale studies that could address these limitations and offer more robust insights.
Implication for Practice
The findings highlight the importance of targeted interventions to enhance sleep quality among ICU patients, particularly those who are older or have comorbidities. To reduce disruptions, practical approaches might include limiting nocturnal light exposure and modifying alarm settings. Implementing a quiet, low-light environment can assist elderly people and others with health difficulties sleep better. By addressing these changeable environmental elements, ICU teams can improve patient comfort, potentially enhancing recovery outcomes and ICU care quality.
Conclusions
The magnitude of poor sleep quality among ICU patients was a major problem in the current study. Patients with elderly age and comorbidity have been identified as independent predictors of poor sleep quality in the ICU. In addition, patients who were exposed to light and monitor alarms reported poor sleep quality in the ICU. Implement strategies to reduce light exposure during the night and customize alarm settings could improve sleep quality. By following these recommendations, healthcare personnel may greatly enhance sleep quality for ICU patients while addressing the barriers provided by age, comorbidities, light exposure, and monitor alarms. This comprehensive approach not only improves patient comfort; but also promotes improved recovery outcomes in critical care.
Footnotes
Acknowledgments
The authors would like to thank data collectors, supervisors, and the respective hospitals involved in this study for their valuable contributions. The authors also want to appreciate Addis Ababa University, College of Medicine and Health Science for offering the chance and sponsor this study.
Ethical considerations
Ethical clearance was obtained from the Research Committee of Addis Ababa University College of Medicine and Health Science, Department of Emergency Medicine, with Ref. no. EMCM/022/2020. Written consent was obtained from each participant. The letter of permission was written by the College of Medicine and Health Science Research directorate office for each hospital. A formal written letter was provided for each hospital. All information was kept confidential, and no individual identifiers were collected.
Authors’ Contributions
TMA, BMK, and AW participated in the study conception and design as well as in interpretation of data. KGT, TSA, EGM, and AHS participated in editing the manuscript and advised during data analysis. TAW and TMA performed the statistical analysis, as well as drafted and reviewed the manuscript. TMA and BMK edited the manuscript and prepared it for publication. All authors read and approved the final manuscript and agreed to submit the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed are available in the article.