
Abstract
Background
Vitamin D deficiency is a great problem worldwide. Vitamin D plays an essential role in calcium and bone metabolism. Diabetic nephropathy (DN) is a dangerous kidney-related complication of type 1 diabetes (T1D).
Aim of the study
To evaluate levels of Vitamin D3 in pediatric patients with T1D and DN; to study the dependence between the Vitamin D level and main clinical and laboratory parameters of the disease, that is, duration, complications episodes, albuminuria levels, glomerular filtration rate (GFR).
Material and methods
A survey of 72 children with T1D and DN aged 3–17 years was done. Complex examination including conventional methods (physical examination, blood pressure measurement, blood tests, study of urinary sediment, renal ultrasound, etc.) was done for all patients. Data was processed using GraphPad Prism 9.0 Software for Windows (USA, San Diego, CA). p-values <.05 were considered statistically significant.
Results
Majority of patients from T1D group have normal value of Vitamin D, only 27.7% of children have Vitamin D insufficiency. In contrast, in children from DN group only 16.7% of children have Vitamin D insufficiency and 83.3% have Vitamin D deficiency. Vitamin D serum level negatively correlates with disease duration and albuminuria level in the group with DN. Serum levels of Vitamin D positively correlate with GFR in patients with T1D. Patients with DN who had a duration of T1D for 10 years and more have a higher progression rate to Vitamin D deficiency as compared to those who have a T1D duration of less than 10 years.
Conclusions
The authors conclude that Vitamin D has a direct relationship with functional disorders with DN, that is, albuminuria, GFR, kidney function. Further investigations of Vitamin D supplementation on different stages of the ND development and progression are needed.
Introduction
Vitamin D is a lipid-soluble, secosteroid hormone. Vitamin D plays a crucial role a numerous physiological functions. Numerous acute and chronic conditions, including problems with calcium metabolism, autoimmune disorders, certain malignancies, types 1 and 2 diabetes mellitus, cardiovascular disease, and infectious diseases have been linked to Vitamin D insufficiency or deficiency. Today, Vitamin D deficiency is recognized as a global epidemic (Zmijewski, 2019).
The main factor contributing to Vitamin D insufficiency is inadequate sun exposure. For kids and adults of all ages, it has been and still is the main source of Vitamin D. Vitamin D is fundamentally important for maintaining calcium homeostasis (Lindblad et al., 2014; Zmijewski, 2019) (Figure 1).

Chemical Structures of Vitamin D2 (A) and Vitamin D3 (B).
To evaluate the Vitamin D status in humans, the 25(OH)D measurement in blood is commonly used method (Jukic et al., 2018; Lindblad et al., 2014). The following scale was used to evaluate the results: >30 ng/mL (>75 nmol/L)—sufficient, 20–30 ng/mL (50–75 nmol/L)—insufficient, 10–20 ng/mL (25–50 nmol/L)—deficient, and <10 ng/mL (<25 nmol/l)—severe deficient.
Vitamin D receptors (VDR) are expressed in all types of human cells. VDR and Vitamin D regulate multiple biological processes through the gene regulation (Mendis, 2017; Zmijewski, 2019). Vitamin D and its role in understanding the basic processes of kidney and cardiovascular diseases pathogenesis are crucial for further treatment strategies (Cieślińska et al., 2018; Jacqueline & Manson, 2012; Koroshi & Idrizi, 2011).
The aim of the study was to evaluate levels of Vitamin D3 in patients with type 1 diabetes (T1D) and patients with T1D and developed diabetic nephropathy (DN); to explore the relationship between the disease's primary clinical characteristics and laboratory markers (duration, complications episodes, albuminuria levels, blood pressure, GFR) and Vitamin D levels in children with T1D and patients with T1D and developed DN.
Material and Methods
A survey of 72 kids (33 boys and 39 girls) with T1D and DN, aged 3–17 years was conducted. Informed consent was obtained from all patients and their families. The study was approved by the hospital local ethics committee. All informed consents were signed by children (≥12 years old) themselves and/or by their parents and kept in medical records. Study was conducted at Clinical Pediatric Hospital № 6, which houses Clinical Base of Bogomolets National Medical University Department of Pediatrics № 4. Every patient receives a thorough evaluation that includes the usual procedures (physical examination, blood pressure measurement, blood tests, analysis of urine sediment, renal ultrasonography, etc.). All patients were seen every 3 months and all were on multiple flexible dosing intervals of insulin treatment. Chronological age, diabetes duration, weight, height, body mass index (BMI), blood pressure, Hb1Ac, serum cholesterol, DKA episodes were recorded during each visit to hospital. Boys’ and girls’ BMI values were evaluated using WHO BMI-for-age z-scores for both genders. Children were considered to have a normal body weight once their weight-for-height z-scores observed within the interval 0 to < ± 1. Based on the basic clinical data, all patients were divided into groups (Table 1).
Clinical Characteristics of Patients.

**p < .001
Glomerular filtration rate (GFR) was used to assess kidney function. Schwartz formula for children and adolescents from 1 to 17 years old used:
eGFR = 0.413 × (height/Scr) if height is expressed in centimeters OR 41.3 × (height/Scr) if height is expressed in meters
eGFR (estimated glomerular filtration rate) = mL/min/1.73 m2
Scr (standardized serum creatinine) = mg/dL
Urinary albumin excretion was measured in 24-h urine collection samples using basic conventional technique established in Clinical Pediatric Hospital №6. Vitamin D3 levels were studied using ELISA assay and commercially available kit (Vitamin D3 [human] ELISA kit [BioVision, USA]).
The data presented are as means ± SEM and as frequencies and percentages when appropriate. Analysis of variance followed by the post-hoc Kruskal–Wallis test for multiple comparisons was used to test significance of differences. Pearson correlation was used to analyze the relationships between several factors. The fraction developing macroalbuminuria at different times for different subgroups was assessed with Kaplan–Meier plots and compared by Gehan–Breslow–Wilcoxon test. Data were processed using GraphPad Prism 9.0 Software for Windows (USA, San Diego, CA). p-values <.05 considered statistically significant.
Results
Clinical Characteristics of Patients
The study covered analysis of data from 2015 to 2020 including children with T1DM followed in the endocrinology unit. All patients were divided into three groups. Control group included 27 healthy children (12 boys and 15 girls). Group entitled T1D were patients included into the study after the onset of T1D with up to 1 year of the disease duration. The average disease duration in T1D group was 11.2 months. Patients with T1D who also had DN made up the group called DN group. The duration of DN in this group was at least a year and longer. In the DN group, the mean value of T1D course was 6.15 years. The criteria for including and excluding patients from the study are listed in the Supplemental Material.
The authors show that in the control group, the GFR value was 104.44 ± 3.95% mL/min/1.73 m2. In contrast, the T1D group value was 131.25 ± 3.74% mL/min/1.73 m2 which is statistically different as compared to control group value (p < .01). The GFR level in the DN group was higher as compared to control group value (112.44 ± 3.02 mL/min/1.73 m2 vs. 104.44 ± 3.95% mL/min/1.73 m2, p < .01) and lower as compared to T1D group value (p < .05).
Blood pressure changes in children with T1D as well as in the group with DN was evaluated. Children in the T1D group had considerably lower systolic blood pressure than children in control group—96.22 ± 3.8 mmHg and 113.34 ± 0.18 mmHg, respectively (p < .01). DN group value was significantly higher as compared to control group and patients with T1D (p < .01). Diastolic blood pressure values were similar in the control group and group of patients with T1D—67.2 ± 1.25 and 64.3 ± 1.45 mmHg, respectively. However, the DN group value was higher than in control group and in T1D group (p < .01).
Vitamin D in Children With T1D and Early DN
All patients from the control group, T1D, and DN groups had their Vitamin D blood levels tested. Normal level of Vitamin D were defined as ≥30 ng/mL, Vitamin D insufficiency—21–29 ng/mL, deficiency ≤20 ng/mL, respectively. Endogenous levels of Vitamin D3 synthesis are season-dependent. Due to this reason, the study was done during the period from September to February. The patients with the lowest levels of Vitamin D3 were those who had DN. In the control group, Vitamin D3 was detected at level 35.75 ± 0.29 ng/mL, in patients with T1D—32.0 ± 0.83 ng/mL (p > 0.05), in patients with DN—18.94 ± 0.26 ng/mL (р<.0001 as compared to control group) (Figure 2A). Interestingly, in the T1D group 27.7% of children had Vitamin D insufficiency and 72.3% had normal levels of Vitamin D (Figure 2B). In contrast, in the DN group 16.7% of children had Vitamin D insufficiency and 83.3% had Vitamin D deficiency (Figure 2C).

(A) Vitamin D levels in children with T1D, early DN, and control group. Subgroups of patients with Vitamin D insufficiency and Vitamin D deficiency in children with (B) T1D and (C) DN.
Correlation Analysis of Vitamin D and Basic Clinical Parameters in Children With Early DN
A correlation analysis was used to assess the relationship between serum Vitamin D levels, clinical and laboratory parameters, such as GFR, albuminuria, and disease progression. Vitamin D levels and disease duration were found to be negatively correlated in a group of DN patients (R = −.51, р<.05) (Figure 3). Average disease duration in children with DN was 6.15 years.

Correlation between serum levels of Vitamin D3 and disease duration in children with DN.
All patients included into the group with DN had albuminuria documented at least at level 30–300 mg/24 h. A DN diagnosis was made based on the discovery of microalbuminuria or macroalbuminuria in at least two of the three samples for every kid in the DN group. Follow-ups were done every 3 months.
In was found that Vitamin D3 serum levels negatively correlated with albuminuria levels in patients with DN (R = −.52, р<.001) (Figure 4). In contrast, no dependence between the two parameters were found in T1D group.
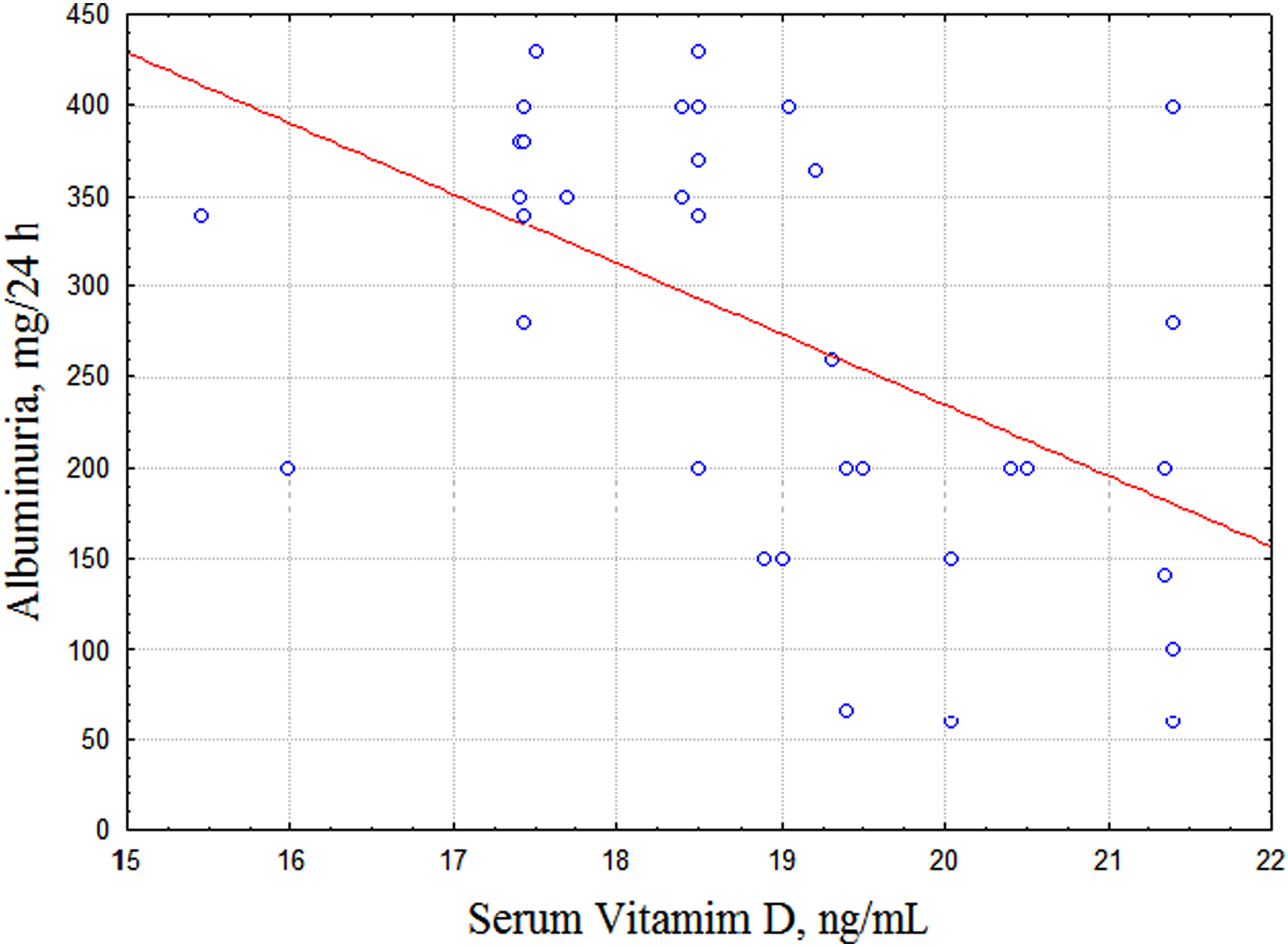
Correlation between serum levels of Vitamin D3 and albuminuria levels in children with DN.
Results of the study show that children with T1D have significantly higher level of GFR as compared to the control group and group with DN. A correlation analysis was performed to assess the relationship between Vitamin D levels and GFR. We found that Vitamin D3 serum levels positively correlated with GFR in patients with T1D (R = .59, р<.05) (Figure 5). However, there was no relationship between serum Vitamin D levels and GFR in a group with DN.
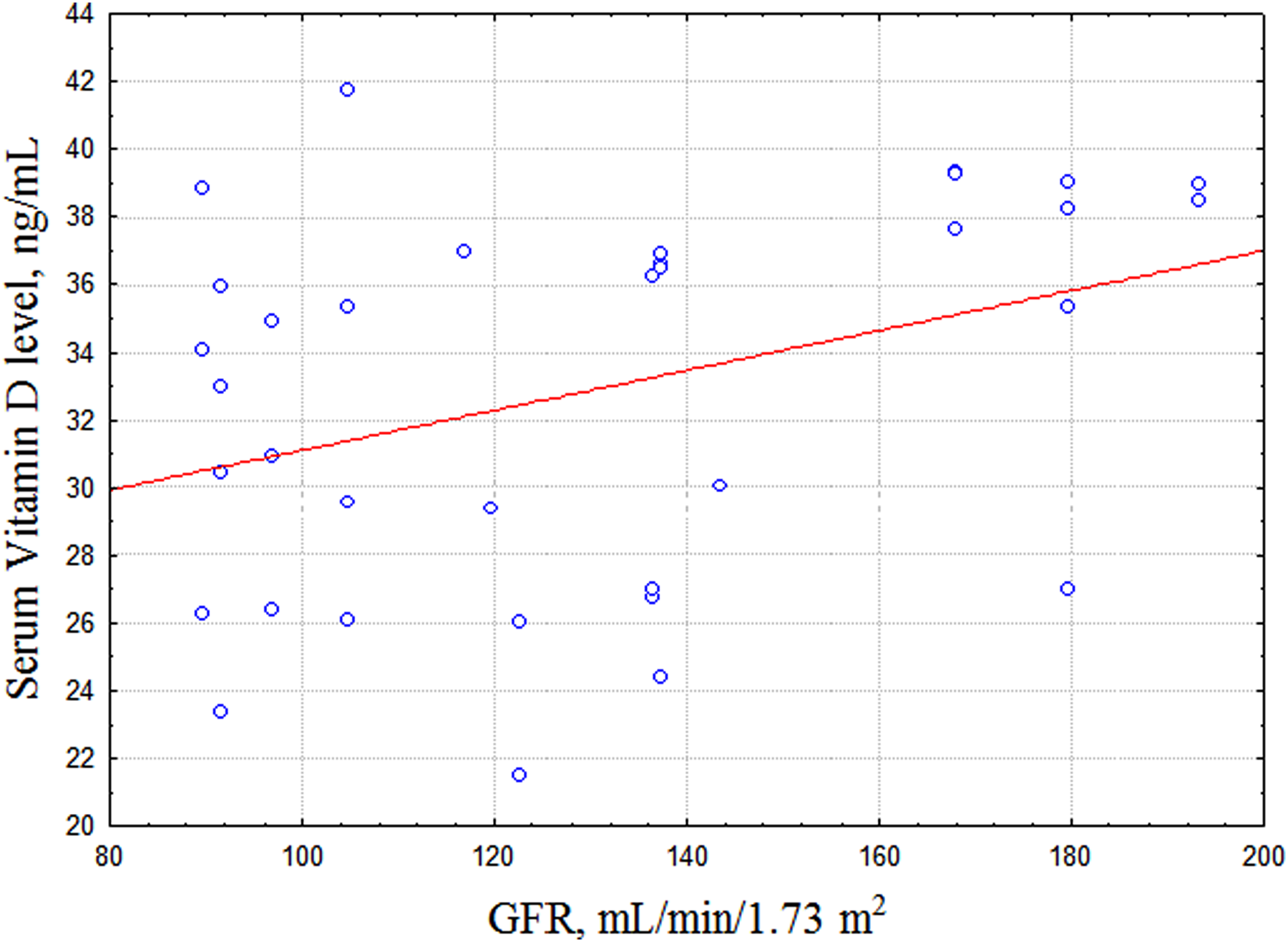
Correlation between serum levels of Vitamin D3 and GFR in children with T1D.
Finally, Kaplan–Meier estimated the fraction developing Vitamin D deficiency at different times for each subgroup and used a Gehan–Breslow–Wilcoxon test to measure statistical significance among the two groups was done. The statistical results showed that patients with DN who have T1D for 10 years or more have a shorter time to develop a Vitamin D deficiency than children with DN who had T1D for less than 10 years (p = .01) (Figure 6).

Time to develop a Vitamin D deficiency in children with DN and different duration of T1D.
Discussion
The wide tissue distribution of VDR suggests that the Vitamin D has additional physiological functions beyond calcium homeostasis. Epidemiological studies show that diabetes mellitus type 1 has prevalence in countries with lower winter ultraviolet exposure. Recent data support the hypothesis that Vitamin D supplementation in early childhood may prevent the onset of diabetes mellitus type1 (Corica et al., 2019).
It has been demonstrated using an in-vivo model that 1.25(OH)2D or its analogs have the ability to lower proteinuria levels due to the preservation of podocyte structure and to lower TGF-1 levels. It is known about the inverse association of circulating Vitamin D levels with blood pressure (Koroshi & Idrizi, 2011).
VDR have also been identified in pancreatic β-cells. Vitamin D deficiency has been shown to effect the insulin synthesis and secretion in animal models of type 2 diabetes. Several studies demonstrated that lower Vitamin D levels were associated with an increased risk of diabetes (Alam et al., 2016). A short-term supplementation with Vitamin D significantly improved function of beta cells; HbA1c levels were decreased (Alam et al., 2016; Devaraj et al., 2011; Gaddas et al., 2022; Joergensen et al., 2011; Satirapoj & Adler, 2014; Tonneijck et al., 2017).
The aim of current study was to evaluate the levels of Vitamin D3 in pediatric patients with T1D and DN; to study the dependence between the Vitamin D level and the main clinical and laboratory parameters of the disease, that is, duration, complications episodes, albuminuria levels, GFR.
The authors show that the majority of pediatric patients from the T1D group had a normal value of Vitamin D, only 27.7% of children had Vitamin D insufficiency. In contrast, in children from the DN group only 16.7% of children had Vitamin D insufficiency and 83.3% had Vitamin D deficiency.
Albuminuria is one of the most characteristic clinical signs of the DN. In the past, especially from the observations in patients with type 1 DM, the clinical stages of DN were considered to begin from early glomerular hyperfiltration, followed by the development of microalbuminuria, and macroalbuminuria (Lin et al., 2016). Results of the study show that Vitamin D serum levels negatively correlate with disease duration and albuminuria levels in children with DN. The authors speculate that the latter is a result of structural changes in kidney in response to persistent albuminuria, metabolic changes. This in turn disrupts Vitamin D kidney metabolism. Moreover, Vitamin D levels negatively correlate with the DN disease duration meaning the time-dependent effect of the mentioned above changes.
Hyperglycemia, as a hallmark of T1D, causes afferent arteriolar dilatation through the release of vasoactive mediators, such as insulin-like growth factor 1 (IGF-1), glucagon, nitric oxide (NO), vascular endothelial growth factor (VEGF), and prostaglandin leading to the GFR changes (Cheng & Harris, 2014; Shi et al., 2018).
The authors found that patients with T1D during the first year after the disease onset have increased GFR level as compared to control values. Meaning the GFR increase can be a “shock” reaction of the glomerular circulation in response to metabolic disorders: hyperglycemia, ketoacidosis, oxidative stress. Results of this study are in line with other research groups data. Tonneijck L. et al. (Tonneijck et al., 2017) reported a supraphysiologic elevation in GFR in 10%-67% of patients with T1D. This phenomenon, known as glomerular hyperfiltration, classically has been hypothesized to predispose to irreversible nephron damage, thereby contributing to initiation and progression of kidney disease in diabetes. The prevailing hypothesis is that hyperfiltration in diabetes precedes the onset of albuminuria and/or decline in renal function, and predisposes to progressive nephron damage by increasing glomerular hydraulic pressure and transcapillary convective flux of ultrafiltrate. Moreover, the purpose of the increased GFR in single remnant nephrons is to compensate for reduced nephron numbers (Brenner et al., 1996; Fattah et al., 2019
Results of the study show that pediatric patients with DN who had a duration of T1D 10 years or more had higher progression rate to Vitamin D deficiency as compared to those who had T1D duration less than 10 years. Several mechanisms have been discussed in the literature concerning the Vitamin D deficiency development in T1D. One of the possible mechanisms of Vitamin D deficiency in diabetics is decreased binding proteins. This phenomenon was shown in vivo (Kim et al., 2017). Later on, in humans, it has been found that the urinary loss of Vitamin D binding protein (VDBP) and diminished function of megalin or low-density lipoprotein-related protein 2 (LRP2), correlated with proteinuria (Thrailkill et al., 2011). Furthermore, it has been shown that level of T1D compensation, that is, DKA number, has an important effect on Vitamin D level. Vitamin D level can be lowered by acidosis (Iqbal et al., 2019).
In conclusion, serious health issues are linked to Vitamin D insufficiency and deficiency, particularly in children with T1D and DN. Early identification and treatment can prevent it. Consequently, the nurse practitioner should be knowledgeable with the risks of Vitamin D insufficiency in diabetic children and patients who could need diagnostic tests (children with early DN, children with T1D, and long disease duration). Endocrinology unit nurses can educate patients and/or their parents about the value of Vitamin D and can provide treatment for Vitamin D deficiency.
Conclusions
The researchers found that over the first year following the onset of the disease, serum Vitamin D levels in pediatric T1D patients tended to deficiency. The majority of patients from the T1D group had normal values of Vitamin D, only 27.7% of children had Vitamin D insufficiency. In contrast, in children from the DN group only 16.7% of children had Vitamin D insufficiency and 83.3% had Vitamin D deficiency.
Results of the study show that Vitamin D serum level negatively correlates with disease duration and albuminuria level in group with DN. Serum levels of Vitamin D positively correlate with GFR in patients with T1D. This trend was not observed in patients with DN.
Children with DN who have T1D for 10 years or more have a shorter time to develop a Vitamin D deficiency than children with DN who have T1D for less than 10 years. Further investigations of Vitamin D supplementation on different stages of the ND development and progression needed.
Strengths and Limitations of the Study
The study's strength is the way it illuminates crucial issues about Vitamin D insufficiency and deficiency in children with T1D and DN. The findings may be helpful for endocrinology unit nurses in terms of informing patients and/or their parents about the importance of Vitamin D and providing them with an accurate diagnosis and course of therapy for Vitamin D deficiency.
A potential limitation of this study is that the study did not take into account evaluation of specific markers of kidney injury—kidney injury molecule (KIM-1), gelatinase-associated lipocalin (NGAL), and other factors that can potentially play a role in Vitamin D networking in patients with DN. Another disadvantage of this study involves the limited number of patients included into the study.
Supplemental Material
sj-docx-1-son-10.1177_23779608221145122 - Supplemental material for To the Question of Vitamin D Network in Type 1 Diabetes and Diabetic Nephropathy in Children Nursed in Ukrainian Endocrinology Unit
Supplemental material, sj-docx-1-son-10.1177_23779608221145122 for To the Question of Vitamin D Network in Type 1 Diabetes and Diabetic Nephropathy in Children Nursed in Ukrainian Endocrinology Unit by Ievgeniia Burlaka and I.O. Mityuryayeva in SAGE Open Nursing
Footnotes
Acknowledgments
We acknowledge the assistance of Endocrinology Unit of the Clinical Pediatric Hospital №6 (Kyiv, Ukraine).
Author Contributions
B.Ie.A.: conceptualization, study design, review of literature, data analysis, manuscript preparation, manuscript submission. M.I.O.: conceptualization, study design, data analysis, manuscript writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study is a records data analysis. Local permission obtained from Clinical Pediatric Hospital №6 (Kyiv, Ukraine) was granted for records use. Written consent was obtained from mothers/caregivers and/or children.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.