
Abstract
Background
Food insecurity is a state in which people do not have both physical and economic access to sufficient food to meet their dietary needs. Food insecurity affects all nations despite that it is high in Africa, particularly in Ethiopia. There is limited information on the magnitude of food insecurity and its associated factors among lactating mothers in Ethiopia. Therefore, the purpose of this study was to determine the magnitude of food insecurity and associated factors among lactating mothers in Yirgalem Town, South Ethiopia.
Methods
A community-based cross-sectional study design was conducted on five randomly selected Kebeles and 557 lactating mothers who were selected using a simple random sampling technique from January 10 to April 30, 2022. The data were collected using interviewer administered questionnaires. Bi-variable and multivariable logistic regression analysis was used in the analysis. Family folder documentation was used to know the number of lactating mothers found in each Kebeles. Food insecurity was measured by household food insecurity access scale (version 3). Dietary diversity was assessed by the 24-hour dietary recall method.
Results
The magnitude of food insecurity among lactating mothers was 58.2%. Low minimum dietary diversity score, mothers with two and below antenatal care, mothers who had more than two children under 5 years, no home gardening practice, and having meals two and below were significantly associated with food insecurity.
Conclusion
The magnitude of food insecurity was 58.2% in the study area. Therefore, the agricultural and health sectors should work collaboratively to improve home gardening practices, dietary diversity practices and maternal health services are highly recommended to reduce food insecurity.
Introduction
Food insecurity is a state in which people do not have both physical and economic access to sufficient food to meet their dietary needs for a productive and healthy life (Coates et al., 2013). It also occurs when the availability, quality, and quantity of food are limited to being accessed in a socially acceptable manner that promotes and maintains the well-being of an individual (Leroy et al., 2015).
It is a global issue that impacts every country, regardless its wealth or standing. However, it has become more severe and prevalent in low- and middle-income nations in the past 20 years (Botreau & Cohen, 2019; Imran et al., 2014). Food insecurity has received increased attention worldwide (Endale et al., 2014).
Sustainable developmental goal two (zero hunger) targets make it imperative for countries to step up their efforts and create a world without hunger and malnutrition by 2030. However, the prevalence of food insecurity gradually increased (Ntwenya et al., 2015). Food insecurity has three categories: mildly food insecure, moderately food insecure, and severely food insecure (Coates et al., 2013).
An estimated 2.3 billion people in the world will face moderate-to-severe food insecurity in 2019. In Africa, food insecurity has increased significantly. It was 35.3% in 2013, 67.2% in 2014, and 92.0% in 2020 (De Cock et al., 2013; Grobler, 2014; Masa et al., 2020). In Ethiopia, food insecurity assessed from 2013 to 2020 has increased from 6.8% to 77% (Endale et al., 2014; Getacher et al., 2020; Tilksew & Fekadu, 2014).
Nutritional requirements increase during lactation because there is maternal tissue development specific to reproduction and infant growth (Chinnakali et al., 2014; Payne et al., 2016). Lactating mothers who live in food-insecure conditions are usually exposed to malnutrition (Chinnakali et al., 2014). Ethiopia is one of the developing countries that has a great challenge to meet food security (Audain, 2014; Getacher et al., 2020; Hirvonen, 2020; Sani & Kemaw, 2019). In Ethiopia, mothers are responsible for preparing and cooking food for all household members, and they are well aware of the absence of sufficient food for all members of the household. Therefore, lactating mothers are the best respondents for food insecurity studies.
Review of Literature
A cross-sectional study conducted in northeast Iran on food insecurity and associated factors among rural household's shows the prevalence of food insecurity was 40.9%. Mothers live in rural areas and who had no home gardening practice are more vulnerable to food insecurity (Gholami et al., 2013).
Another cross-sectional study conducted in Malaysia on the association between household food insecurity and adverse health outcomes in low-income households in rural areas of Malaysia shows the prevalence of food insecurity was 83.9%. Rural residence, low frequency of meals per day, and mothers who had no home gardening practice are some of the contributing factors to food insecurity (Ihab et al., 2012).
A cross-sectional study conducted in Tanzania on dietary patterns and household food insecurity in rural populations of the Kilosa district shows the magnitude of food insecurity was 80%. Mothers with poor dietary diversity practices and who consume alcohol were significantly associated with food insecurity (Ntwenya et al., 2015). A cross-sectional study was conducted in rural areas of Limpopo Province, South Africa on household food insecurity and associated factors among lactating mothers shows the magnitude of food insecurity was 53%. Lactating mothers with poor educational status, mothers who had no antenatal care, and rural residents were correlated with food insecurity (De Cock et al., 2013).
A systematic review and meta-analysis conducted in East Africa shows the pooled prevalence of urban household food insecurity was 60·91%. Mothers with low socio-economic status, large family size, and poor dietary diversity practices were significant factors of food insecurity (Gebremichael et al., 2022). A study conducted in East Ethiopia on factors influencing rural household food insecurity shows the prevalence of food insecurity was 57%, and large family sizes have a great contribution to food insecurity (Tilksew & Fekadu, 2014). Another cross-sectional study conducted in Ataye, North Ethiopia, shows the magnitude of food insecurity was 36.8%. Mothers who had no home gardening practice, low frequency of meals per day, and low minimum dietary diversity score were the factors that increased food insecurity (Getacher et al., 2020).
A study conducted in Jimma on factors associated with malnutrition among lactating women in subsistence farming households in Dedo and Seqa-chekorsa districts shows the magnitude of food insecurity was 6.8% (Arba, 2016). A cross-sectional study conducted in Farta district on the magnitude of food insecurity shows the magnitude of food insecurity was 70.7%. Lactating mothers had no income-generating activities (activities increase monthly or annual income), and those who had no home gardening practices were more susceptible to food insecurity (Endale et al., 2014).
Another community-based cross-sectional study conducted in the Benishangul Gumuz Region, north-western Ethiopia, on food insecurity shows the magnitude of food insecurity was 72%. Mothers with poor socio-economic status, large family size, and low frequency of meals per day have a greater contribution to the high prevalence of food insecurity (Guyu & Muluneh, 2018).
Food insecurity among lactating mothers may occur due to different reasons: such as poor socioeconomic status, large family size, absence of income-generating activities, poor dietary diversity practices, and a low frequency of meals per day (Asgharian Dastnaei et al., 2013; Endale et al., 2014; Getacher et al., 2020; Tilksew & Fekadu, 2014). Furthermore, mothers who had no home gardening practices and consumed alcohol contributed to the food insecurity of mothers (Getacher et al., 2020). However, there is limited information on food insecurity and its associated factors among lactating mothers in Ethiopia.
Objectives of the Study
To determine the magnitude of food insecurity and associated factors among lactating mothers in Yirgalem Town, South Ethiopia, 2022.
Methods
Study Area and Period
The study was conducted in Yirgalem town. It is 323.3 km away from Addis Ababa, which is the capital city of Ethiopia. It is 40 km away from Hawassa city, which is the regional city of Sidama. It has a latitude and longitude of 6°45″N 38°25″E and an elevation of 1776 m above sea level. The town has 13 Kebeles. There are one general hospital, two health centers, and 13 health posts.
Based on the Yirgalem town population statistics report for 2013 E.C., the town has an estimated total population of 83,205, of whom 40,437 are men and 42,768 are women. There are 12,988 children under 5 years old and 2,027 lactating mothers living in Yirgalem town (Office, 2021). This study was conducted in three urban and two rural randomly selected Kebeles from January to April 2022.
Study Design and Population
A community-based cross-sectional study design was conducted in Yirgalem Town from January 10 to April 30, 2022. All lactating mothers who live in the selected Kebeles of Yirgalem Town were our study population. Lactating mothers who lived for at least 6 months and above in the town were included, and lactating mothers who were unable to respond to an interview, severely sick mothers and mothers who did not volunteer to respond to the questionnaire were excluded from the study.
Sample Size Determination
The required sample size for this study was determined and calculated using a single population proportions formula with the following assumptions:

Sampling Techniques and Procedure

The sampling procedure of food insecurity and its associated factors among lactating mothers in Yirgalem Town.
Study Variables
Dependent variable: Food insecurity.
Independent variables: Socio-demographics factors: The place of residence, maternal age, marital status, maternal educational status, family size, number of children under 5 years, occupation of the mothers.
Health service utilization-related factors: having antenatal care, place of delivery, postnatal visit, and maternal history of illness, food source.
Feeding practices of the mothers related factors: minimum dietary diversity, nutritional knowledge, sources of food, home gardening practice, alcohol intake by the mothers, and income generating activities.
Operational Definitions
Knowledge of mothers about nutrition: It was computed based on six questions using a mean score. Mothers who scored above the mean cutoff point were considered to have good knowledge and coded as “1,” whereas those who scored below this cutoff point were considered to have poor knowledge and coded as “0” during analysis (Yabancı et al., 2014).
Kebeles: A small administrative unit in Ethiopia (kebele, 2022).
Health post: Basic public health services unit at the local level (Foreman, 2013).
Home gardening practice: The farming system involves growing fruits, vegetables, and herbs in the family home for personal consumption (Rammohan et al., 2019).
Food secure mothers: Mothers who have experienced none of the food insecurity conditions or have just been worried, although rarely, during the past 4 weeks (Asgharian Dastnaei et al., 2013).
Food insecure mothers: Mothers who are unable at all times to access food sufficient to lead an active and healthy life (includes all stages of food insecurity; mild, moderate, and severe) (Hussein et al., 2018).
Mildly food insecure mothers: Mothers who worry about not having enough food sometimes or often and/or are unable to eat preferred foods and/or eat a more monotonous diet than desired and/or some foods considered undesirable but only rarely (Hussein et al., 2018).
Moderately food insecure mothers: Mothers who sacrifice quality more frequently, by eating a monotonous diet or undesirable foods sometimes or often and/or have started to cut back on quantity by reducing the size of meals or number of meals, rarely or sometimes. However, they do not experience any of the three most severe conditions (Hussein et al., 2018).
Severely food insecure mothers: Mothers who have been forced to cut back on the meal size or the number of meals often and/or experience any of the three most severe conditions (running out of food, going to bed hungry, or going a whole day and night without eating), even as infrequently as rarely (Hussein et al., 2018).
Data Collection Methods and Instruments
The data collectors underwent a community-based face-to-face interview using a structured and pretested questionnaire. The lactating mothers were informed about the details of the research during the interview period. Two master-prepared health professionals from the Yirgalem town health office were recruited for the supervision of the data collection procedure.
Measurements
Household food insecurity was measured with the household food insecurity access scale (HFIAS) version 3. It is a structured, standardized, and validated tool developed mainly by Food and Nutrition Technical Assistance (FANTA III) to classify households as food secure or not (Coates et al., 2013; Wiesmann et al., 2009). The tool consists of nine questions that show the frequency of occurrence and measure the severity of food insecurity in the last 4 weeks in terms of Likert scale question responses (0 = never, 1 = rarely (1 or 2 times), 2 = sometimes (3–10 times), and 3 = often (>10 times)_.
The mothers were expected to answer these questions on behalf of all household members in their household. The tool was used to assess access to food for all household members at the time of data collection. The cumulative score of food insecurity among mothers determined through the nine items ranged from 0 to 27, and a higher score indicated that the household members experienced more food insecurity.
For analysis, all “yes” responses were coded in “1” and “no” responses were coded in “0,” and the responses were summed to obtain the household food insecurity status. The household food insecurity status, which had high internal consistency (Cronbach's α = 0.895), was further dichotomized as “food insecure” and “food secure” households, which were coded as “1” and “0,” respectively, for analysis.
Nutritional knowledge was assessed by asking mothers six questions about their knowledge of nutrition. It was computed, and mothers who properly answered three or more questions were “considered” knowledgeable. The mean score of the mothers who scored above the mean cutoff point was considered to have good knowledge and coded as “1,” whereas those who scored below this cutoff point were considered to have poor knowledge and coded as “0.”
The questions included mothers’ awareness about nutrition, dietary diversity practice and taking varieties of food groups, definitions of the term varieties and types of varieties of food groups, definitions of the term nutrition and malnutrition, causes of malnutrition, and consequences of malnutrition. The previous history of illness of mothers was assessed by self-reporting and asking them whether they faced any illness in the last time (Yabancı et al., 2014).
Data Quality Control
The questionnaire was translated back to English by independent language experts in both languages to ensure its consistency, and comparisons were made on the consistency of the two versions. Before the actual data collection was started, the questionnaire was pretested outside the selected Kebeles. Dale wereda, which is a neighboring wereda for Yirgalem town, was selected to conduct the pretest, and 5% (29) lactating mothers participated from two randomly selected Kebeles of Dale wereda to ensure the validity of the tool.
After the pretest was conducted, all necessary adjustments were made. The pretested and structured questionnaires were translated into the Amharic language used to collect the data. The training was given for two days on theoretical and practical aspects of data collection for five health extension workers and two supervisors.
The training was focused on the areas of interview techniques, ethical issues, and the rights of the participants, reading through all the questions and understanding them well, and ways of minimizing under-reporting or over-reporting and maintaining confidentiality. Interviews were conducted without the involvement of any person other than the respondent in the area of providing adequate confidentiality and privacy. The actual data collection was closely supervised by the principal investigator and the two supervisors. The collected data were cross-checked on each day of activity for consistency, missing data, and completeness.
Data Processing and Analysis
The principal investigator visually checked all the interview questionnaires before going in for analysis. EpiData version 4.6.0.0 software was used to code, enter, and clean the data, and after the completeness was checked, then exported and analysed with Statistical Package for Social Science (SPSS) Version 25 software. Simple descriptive statistics were performed to describe the demographic, socio-economic, and maternal-related characteristics of the respondents. Tables and figures were used to present the information of respondents.
The bi-variable analysis and crude odd ratio, along with a 95% confidence interval (CI), were used to see the association between each independent variable and the outcome variable. Independent variables with a value of P ≤ .25 were included in the multivariable analysis to control for confounding factors. Multi-collinearity was checked using standard errors (SE), and variables with an SE of ≥2 were dropped from the multivariable analysis to see the linear correlation among the independent variables.
The test coefficient of Hosmer–Lemeshow's goodness-of-fit model was used to test the fitness of the model. It was found to be insignificant with a large P-value (P = .760). The adjusted odd ratio (AOR) with a 95% CI was estimated by using multivariable logistic regression analysis to identify the associated factors of food insecurity. All tests were two-sided, and the level of statistical significance was declared with a value of P < .05.
Ethical Clearance and Considerations
Ethical approval was obtained from the Hawassa University, College of Medicine and Health Science Institutional Health Review Board. The participant's privacy and their rights during the interview were guaranteed, and written and signed informed consent was obtained from each respondent. Those who signed written consent only participated in the study, and the confidentiality of the respondent was maintained throughout the research process by giving a code to the participant. The participant had the right to withdraw from the study at any time.
Results
Sociodemographic Characteristics of Respondents
Out of 583 respondents, 557 lactating mothers participated in the study, with a response rate of 95.54%. The mean age of the mothers (±SD) was 28.87 (±5.83) years. Four hundred and twenty-seven (76.5%) lived in urban areas, and 28% (157) were in the age group of 25 to 30 years, and 482 (93.9%) were married. Twenty-two percent had no formal education and 352 (63.2%) were housewives (Table 1).
Sociodemographic Characteristics of Respondents in Yirgalem Town, South Ethiopia 2022 (n = 557).

Health Service Utilization of Mothers
More than half (53.3%) of mothers had four and above antenatal care. On the other hand, around 46% were delivered in the hospital, and 92.1% had a postnatal follow-up. Three-tenths of the mothers had an illness in the last 2 weeks (Table 2).
Health Service-Related Characteristics of Respondent in Yirgalem Town, South Ethiopia, 2022.

The main source of food for 75% of lactating mothers was covered purchasing, 36% of mothers had good nutritional knowledge, and half of the mothers (50.4%) had a high minimum dietary diversity (Table 3).
Food Source and Feeding Practice of Mothers in Yirgalem Town, South Ethiopia, 2022.

The Magnitude of Food Insecurity in Yirgalem Town
The magnitude of food insecurity in Yirgalem town was 58.2% with a 95% CI (53.9, 62.3) (Figure 2).
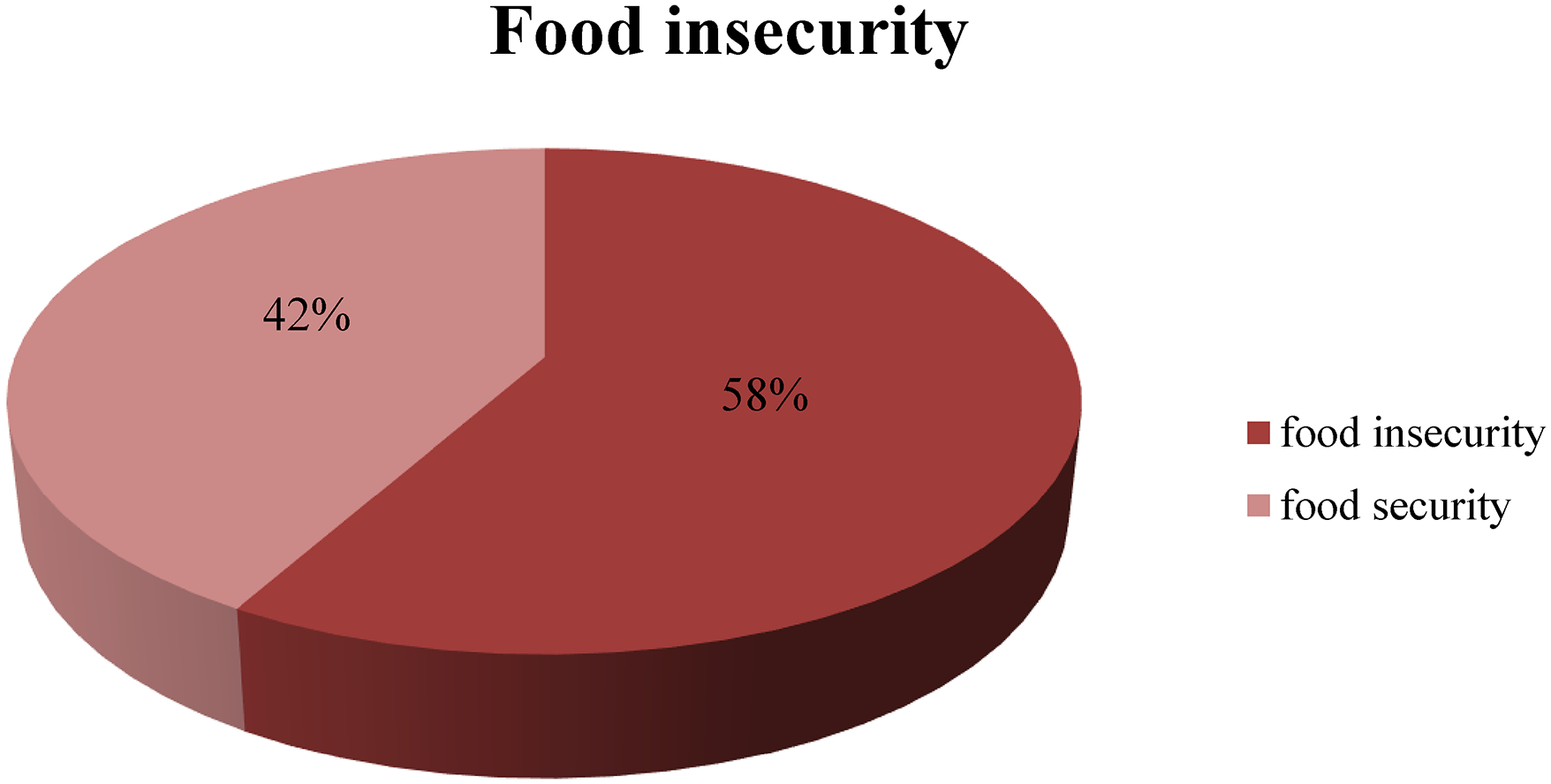
Magnitude of food insecurity among lactating mothers in Yirgalem Town, South Ethiopia 2022.
Four percent of mothers were mildly food insecure, 39.5% were moderately food insecure, and 14.4% were severely food insecure (Figure 3).
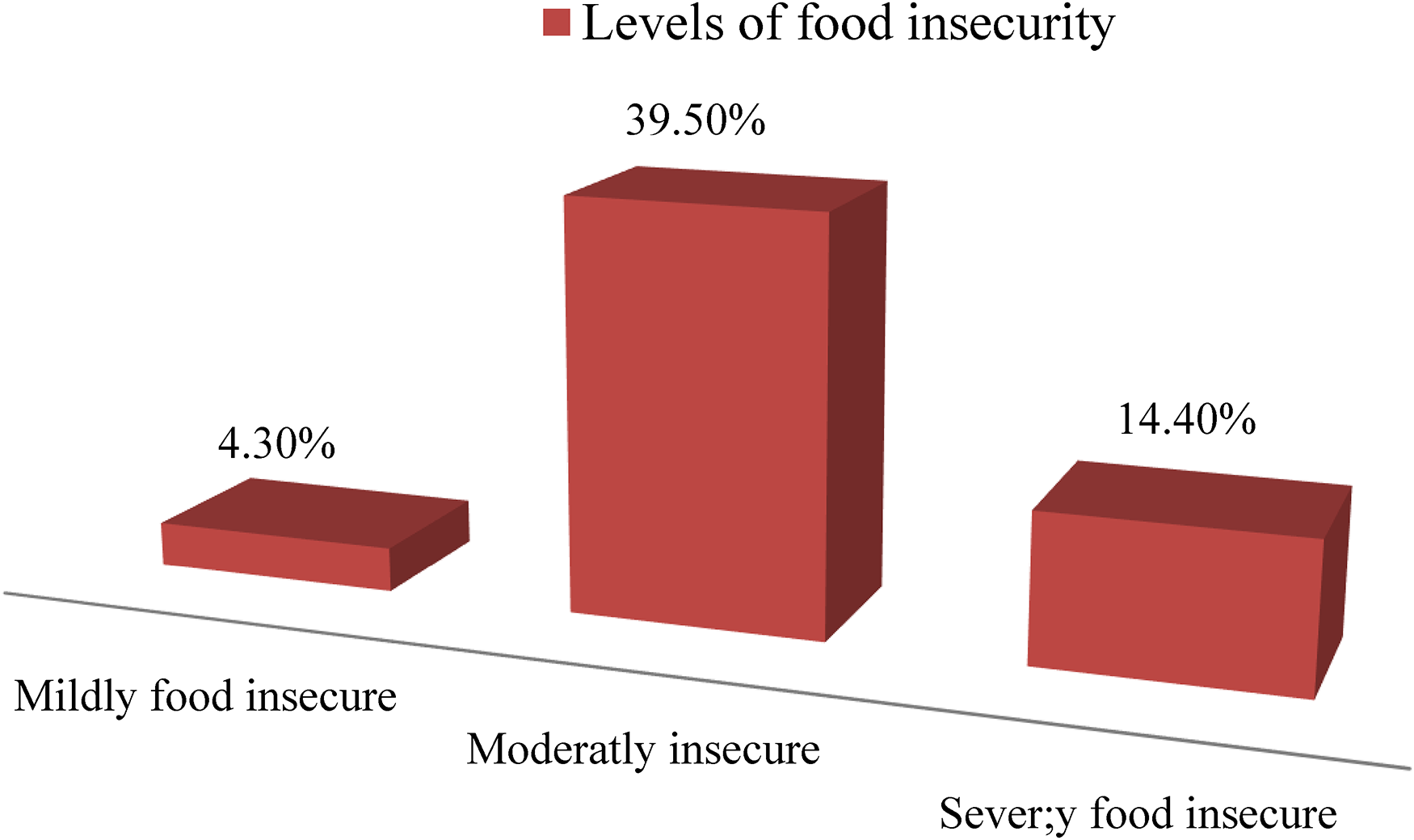
Classification of food insecurity among lactating mothers in Yirgalem Town, South Ethiopia 2022.
Description of the nine items of HFIAS food access questions of mothers in Yirgalem Town, South Ethiopia, 2022 (Table 4).
Descriptions of the Nine Items of HFIAS Food Access Questions of Mothers in Yirgalem Town, South Ethiopia, 2022.
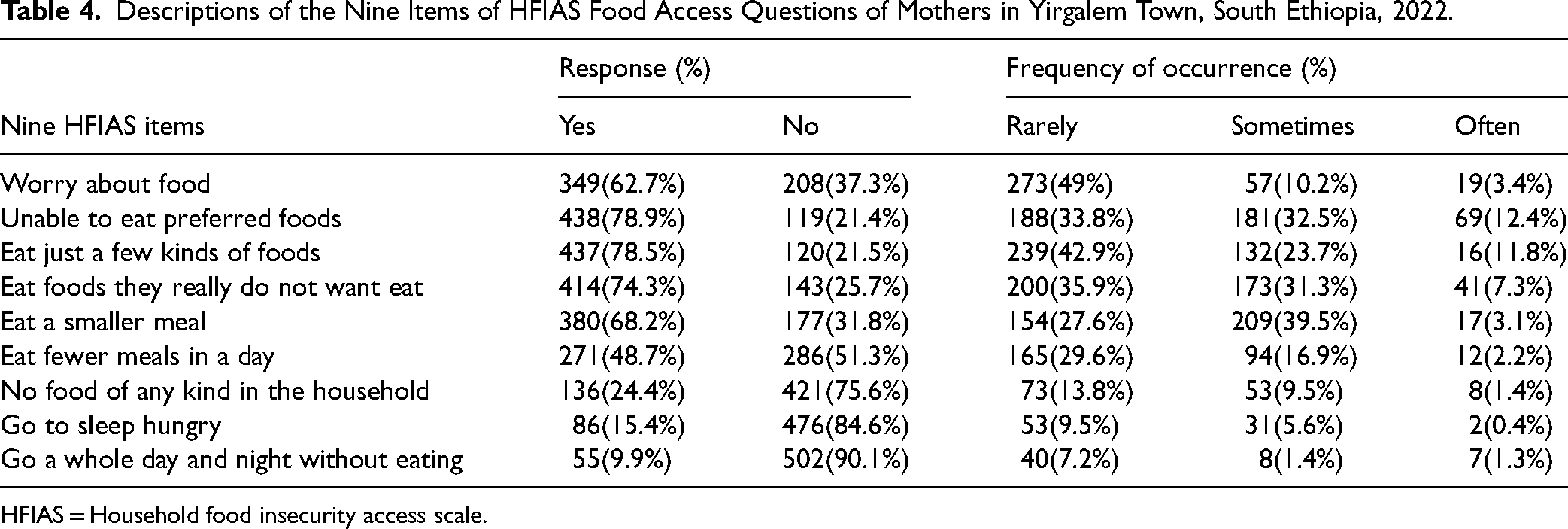
HFIAS = Household food insecurity access scale.
Associated Factors of Food Insecurity Among Lactating Mothers
In the bi-variable logistic regression analysis, the educational level of the mother, occupation of the mother, marital status, family size, number of children under 5 years, mothers having antenatal care, place of delivery, frequency of meal per day, nutritional knowledge of the mothers, minimum dietary diversity score, home gardening practice, having illness in the last 2 weeks, and mothers having postnatal follow-up were associated with food insecurity
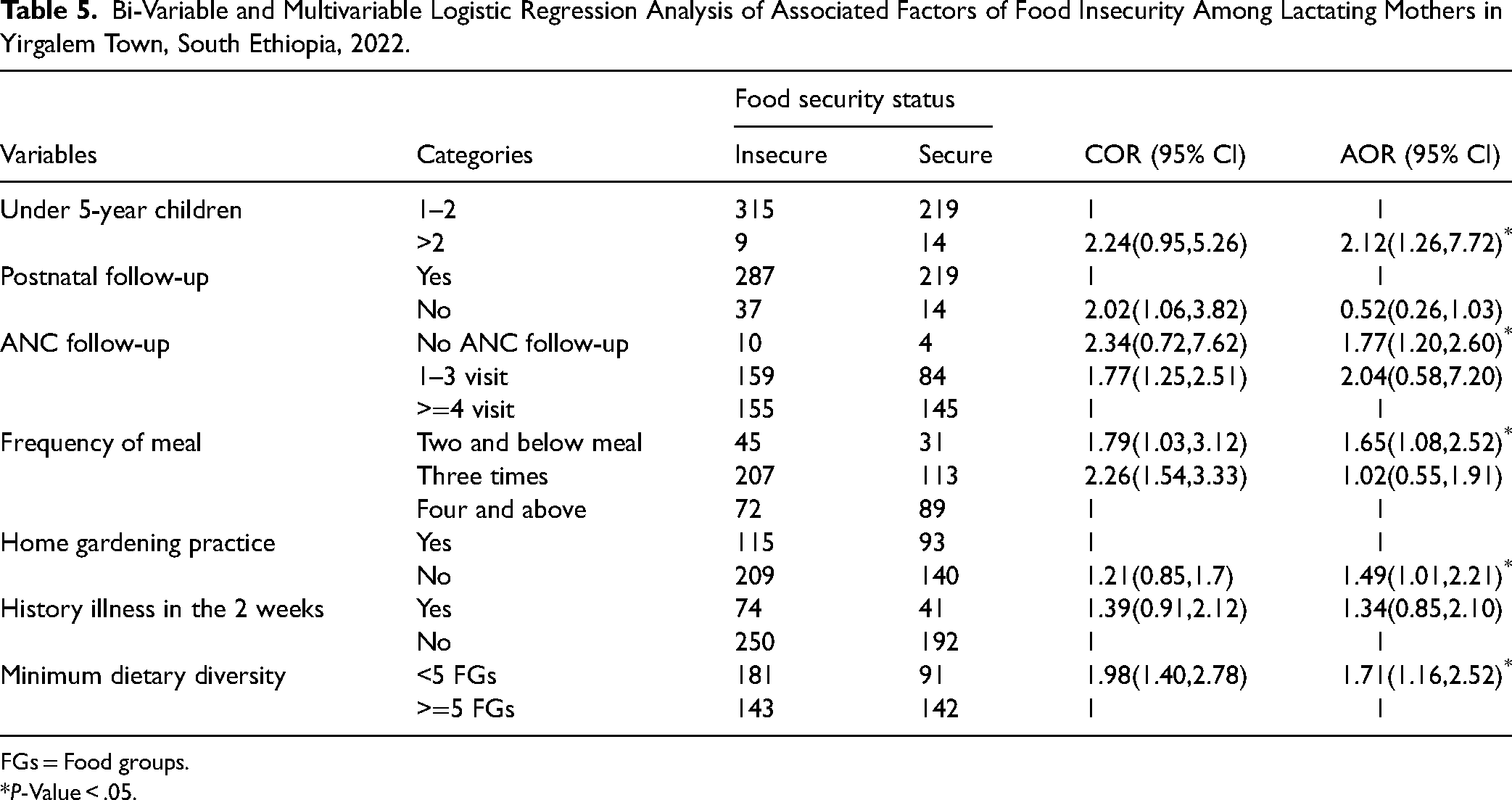
Those variables with a value of P ≤ .25 in the bi-variable logistic regression analysis were entered into a multivariable logistic regression analysis to identify the independent factors of food insecurity. Accordingly, mothers having two and below antenatal care, mothers who had no home gardening practice, mothers who have more than two children under 5 years, a low minimum dietary diversity score, and lactating mothers having meals two and below per day were significantly associated with food insecurity.
Mothers with low minimum dietary diversity scores were nearly two times (AOR = 1.71, 95% CI 1.16–2.51) more likely to have food insecurity than mothers who had high minimum dietary diversity scores. Mothers who had two and below antenatal care had approximately two times (AOR = 1.77, 95% CI 1.20–2.60) more probability of being food insecure than their counterparts.
The odds of food insecurity were two times higher among the mothers who had more than two children under 5 years (AOR = 2.12, 95% CI 1.26–7.72) than lactating mothers who had less than two children under 5 years. Lactating mothers who had no home gardening practice were approximately 1.5 (AOR = 1.49, 95% CI 1.01–2.21) times more likely to be prone to food insecurity than lactating mothers who had home gardening practice.
The odds of food insecurity were two times higher among mothers with a low minimum dietary diversity score (AOR = 1.71, 95% CI 1.16–2.52) than among mothers who had a high minimum diversity score. Lactating mothers who had meals two and below were around two times more likely to have a chance to meet food insecurity than their counterparts (AOR = 1.65, 95% CI 1.08–2.52) (Table 5).
Bi-Variable and Multivariable Logistic Regression Analysis of Associated Factors of Food Insecurity Among Lactating Mothers in Yirgalem Town, South Ethiopia, 2022.
FGs = Food groups.
P-Value < .05.
Discussion
The magnitude of food insecurity was 58.2% in the study area. Lactating mothers who had no home gardening practice, a low minimum dietary diversity score, frequency of meals two and below per day, mothers with two and above children under 5 years, and mothers who have two and below antenatal care were significant predictors of food insecurity.
The findings of this study indicate a prevalence rate of 58.2%. It is consistent with the study conducted in the Babilo district, which was 57% (Tilksew & Fekadu, 2014), in Shashemene, it was 55.7% (Asgharian Dastnaei et al., 2013). While it is higher than the study conducted in South Africa, which was 53% (De Cock et al., 2013), in Ataye district (36.8%) (Getacher et al., 2020), in Iran (40.9%) (Gholami et al., 2013), in Jimma zone (6.8%) (Arba, 2016). These inconsistencies could be due to the differences in some sociodemographic characteristics of the study participants.
However, it was lower compared to the study conducted in Malaysia, which was 83.9% (Ihab et al., 2012), in Tanzania (80%) (Ntwenya et al., 2015), in Farta district (70.7%) (Endale et al., 2014), and in Benishangul Gumuz (72%) (Guyu & Muluneh, 2018). This variation may be due to differences in some socio-demographic characteristics of the study participants such as the educational status of lactating mothers and the total number of families in the household.
Another possible reason may be related to seasonal variation. This research was conducted in the post-harvest season. The availability of cereals, fruits, and vegetables increased during the post-harvest season. It may have the possibility of decreasing the magnitude of food insecurity. While some of the research was conducted during the pre-harvest season, such as a study conducted in Tanzania and Malaysia, there is a possibility of increasing food insecurity because there was poor access to fruits, vegetables, and cereals during the pre-harvest season.
Associated Factors of Food Insecurity Among Lactating Mothers in Yirgalem Town, South Ethiopia
Lactating mothers who had no home gardening practice were 1.5 times more likely to have food insecurity than the mothers who had home gardening practice within their compound. This finding is comparable with the study conducted in Ataye, North Ethiopia (Getacher et al., 2020). Mothers who have no home gardening practice within their compound will have a probability of developing food insecurity, because they cannot easily access fresh and organic food like vegetables, fruits, and other important crops. While mothers who have home gardening practice can easily access fresh foods (Rammohan et al., 2019).
Concerning mothers frequency of meal per day, mothers who had meals two and below per day were two times more likely to have food insecurity than mothers who had more than two meals per day. This is consistent with the study done in northwestern Ethiopia and Ataye, north Ethiopia (Getacher et al., 2020; Sani & Kemaw, 2019). Lactating mothers who had meals two and below per day were at risk of developing undernutrition. Therefore, food insecurity is the direct cause of malnutrition for mothers and children. It was related to a low income level and large family size, specifically having more than two children under the age of 5 within the family.
Regarding children under 5 years, the odds of food insecurity were two times higher among mothers who had more than two children under 5 years than their counterparts. This finding is consistent with the study conducted in the east and west Gojam (Motbainor et al., 2015). Mothers who have more than two children under age of 5 need more food. This results in mothers and children being exposed to malnutrition as compared to lactating mothers who have two and fewer children under 5 years (Motbainor et al., 2015).
The odds of food insecurity were two times more common among mothers with low minimum dietary diversity scores than among mothers who had high minimum dietary diversity scores. This is supported by the study conducted in Ataye, North Ethiopia, and Tanzania. Mothers who had not gotten a diversified diet were highly correlated with food insecurity. It is related to poor availability of food (different food groups), low income level, and increasing family members (Getacher et al., 2020; Ntwenya et al., 2015).
Concerning mothers who had two and below antenatal care, mothers who had two and below antenatal care were two times more likely to be food insecure than their counterparts. This finding is consistent with the research conducted in Bangladesh (Chowdhury et al., 2018), since mothers who have poor antenatal care follow-up did not get proper service, including nutritional advice.
The findings support the Ethiopian National Nutrition Program II (NNP II) and the productive safety net program (PSNP) to improve the habit of consuming a diversified diet among lactating mothers and reduce the burden of food insecurity. The Ethiopia government should design intervention programs aimed at improving maternal food security status through appropriate food-based approaches for mothers to have good coping strategies.
The district should strengthen nutrition education programs and create strong multi-sectored collaboration with the agricultural sector targeted at improving home gardening practice, and dietary diversity practice. The district should work on improving health service utilization, such as antenatal care and family planning. Further study with a stronger study design, like a prospective cohort study, is needed to identify other independent predictors of food insecurity and to address seasonal variation.
Limitations of Study
Recall bias is one of the limitations of the study. The questions were asked in the past 4 weeks, but it could be minimize by probing the respondent about the event.
Seasonal variation is the other limitation of this study. Since food insecurity may increase or decrease during the post-harvest and pre-harvest periods. Since the data collection was started in the dry season, which is the postharvest period. It may decrease the magnitude of food insecurity.
This study was also affected by over- or under-reporting.
It also affected social desirability bias. Sometimes, the respondent may also conceal their true opinion due to different reasons, thus affect the prevalence of food insecurity.
Implications for Practice
It is important to consider the effect of food insecurity on maternal and child health during lactation. Furthermore, it is important to show the factors that have contributed to food insecurity. The health sectors, particularly the districts, provide health education on nutrition and deliver appropriate antenatal and family planning services to reduce frequent childbirth.
Home gardening practice has a direct contribution to household food security by increasing the availability of food because it is a source of fresh and organic food. Therefore, the agricultural sector prepares and provides training for mothers on how to prepare home gardening and supports the mothers to have home gardening.
Conclusion
The magnitude of food insecurity was 58.2% in the study area. Therefore, the agricultural and health sectors should work collaboratively to improve home gardening practice and dietary diversity practice. The districts should work on providing health education on nutrition and improving antenatal and family planning services, which are highly recommended to reduce food insecurity.
Supplemental Material
sj-docx-1-son-10.1177_23779608241278628 - Supplemental material for Food Insecurity and Its Associated Factors Among Lactating Mothers in Yirgalem Town, South Ethiopia: A Community-Based Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608241278628 for Food Insecurity and Its Associated Factors Among Lactating Mothers in Yirgalem Town, South Ethiopia: A Community-Based Cross-Sectional Study by Fikremariam Endeshaw, Haregwa Asnake W/kidan, Fentahun Tamene Zeleke, Daniel Tsega Tefera, Shimelis Tadesse Abebe, Ahmed Nuru Muhamed and Esuyawkal Mislu Kasahun in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241278628 - Supplemental material for Food Insecurity and Its Associated Factors Among Lactating Mothers in Yirgalem Town, South Ethiopia: A Community-Based Cross-Sectional Study
Supplemental material, sj-docx-2-son-10.1177_23779608241278628 for Food Insecurity and Its Associated Factors Among Lactating Mothers in Yirgalem Town, South Ethiopia: A Community-Based Cross-Sectional Study by Fikremariam Endeshaw, Haregwa Asnake W/kidan, Fentahun Tamene Zeleke, Daniel Tsega Tefera, Shimelis Tadesse Abebe, Ahmed Nuru Muhamed and Esuyawkal Mislu Kasahun in SAGE Open Nursing
Footnotes
Acknowledgments
Authors would like to express their deepest gratitude to Hawassa University, College of Medicine and Health Science, for ethical clearance. They also thank their study participants, data collectors, supervisors, and language translators for their invaluable contribution to this study and thank you to Yirgalem town health office and health extension workers for their collaboration during data collection.
Authors' Contributions
Fikremariam Endeshaw and Haregwa Asnake revised subsequent drafts of the paper, and contributed to the finalization of the manuscript Ahmed Nuru and Fantahun Tamene performed the data collection, performed the statistical analysis, and Shimelis Tadesse and Fikremariam Endeshaw served as the lead author of the manuscript, Daniel Tsega and Esuyawkal Mislu participated in the design of the study. Finally, all authors read and approved the final manuscript.
Data Availability
The data used in this study is available upon reasonable request from the principal investigator.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval letter was obtained from Hawassa University, College of Medicine and Health Science Institutional Health Research board (IRB-ref. No-269/13). Both Written and verbal informed consent were obtained from each participant before initiation of study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Hawassa University, and the funders had no involvement in the study design, data collection, analysis, publication decision, or article writing.
Informed Consent
Written and verbal informed consent was obtained from all subjects and legally authorized representatives of minor subjects before the study.
ORCID iDs
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.