
Abstract
Introduction
Nurses are continually faced with multiple demands to make decisions in their clinical practice. The Nursing Decision-Making Instrument (NDMI) assesses nurses’ decision-making styles during the several stages of this process.
Objectives
To adapt the NDMI into European Portuguese and evaluate the psychometric properties of the Portuguese version in a population of Portuguese nurses.
Methods
Descriptive study design was used to examine psychometric properties of NDMI. Nonprobability convenience sample of 339 Portuguese direct-care nurses. Data were collected using a questionnaire comprising sociodemographic and professional data and the NDMI–Portuguese version (NDMI-PT). An exploratory factor analysis (EFA; n = 125) and a confirmatory factor analysis (CFA; n = 214) were carried out using IBM SPSS (v. 24) and AMOS (v. 22).
Results
The EFA revealed a structure of four latent factors, which represent the reorganized stages of the decision-making process. The CFA found a good overall fit of the model (χ2/df = 2.13; comparative fit index [CFI] = 0.91; goodness of fit index [GFI] = 0.82; Tucker-Lewis Index [TLI] = 0.90; root mean square error of approximation [RMSEA] = 0.07; maximum-likelihood expected cross-validation index [MECVI] = 3.13). The psychometric analysis of the theoretical structure revealed that the four factors reflect the decision-making stages and have a better overall fit than the empirical structure (χ2/df = 1.82; CFI = 0.94; GFI = 0.86; TLI = 0.93; RMSEA = 0.06; MECVI = 2.55). The analysis of the construct reliability of the NDMI-PT revealed that the overall internal consistency was excellent (α=0.96).
Conclusions
This study revealed that the empirical and theoretical structures were appropriate and valid for the sample under analysis. The NDMI-PT is a reliable and valid tool for assessing nurses’ decision-making styles. Studies should be conducted to gain further insight into the robustness of this validated tool.
Introduction
Nursing care has become more complex due to advances in healthcare technology and demographic changes. As a result, nurses are continually challenged to provide more efficient and effective care (Martins et al., 2016; Martins et al., 2020; Nibbelink & Brewer, 2018; Oh et al., 2022).
Critical reasoning as the first attribute for decision making in nursing presupposes comprehensive thinking that can solve the most complex health problems of sick people, referring to the problem-solving ability necessary to recognize problems, predict the risks/benefits based on professional intuition or an analytical approach (Farčić et al., 2020; Oh et al., 2022).
Nursing decision making is a complex process that is typically based on either analytical (a step-by-step, conscious, logically defensible process) or intuitive (rapid information processing) thinking. This process is fundamental in solving patients’ priority nursing problems (Lauri & Salanterä, 2002; Stinson, 2017).
The quality of decision making depends on the nurses’ level of knowledge, their previous experiences and their professional skills, with previous clinical experience building nurses’ confidence and decision-making awareness (Maharmeh et al., 2016).
Although nurses have invested in the implementation of the nursing decision-making process in recent years, particularly through the use of health information systems, studies on the quality of nursing care continue to identify weaknesses in the implementation of the nursing process (Fernandes & Tareco, 2016; Ribeiro et al., 2018).
Review of Literature
Decision making is an essential deliberative process that nurses use in clinical practice. This process involves critical thinking, knowledge, and clinical experience. It consists of choosing alternatives to provide patient care in four stages: (1) data collection; (2) data processing and identification of nursing problems; (3) plans of action; and (4) implementation of plan, monitoring, and evaluation of the patient's condition (Farčić et al., 2020; Lauri & Salanterä, 2002).
Sist and Palese (2020) identified Hammond's Cognitive Continuum Theory as a model that helps to understand the complexity of decision-making processes. The theory states that nurses’ decision-making process runs on a continuum between analytical and intuitive approaches. According to Lauri and Salanterä (2002), the approach depends on the nature of the problem, the complexity of the nursing situation, and the context in which care is provided.
Lauri and Salanterä (2002) developed the Nursing Decision-Making Instrument (NDMI) to help nurses make decisions and solve problems. The NDMI has been extensively used in international research (Albanesi et al., 2021; Bjørk & Hamilton, 2011; Kim & Jung, 2014; Sist & Palese, 2020).
The NDMI is a 24-item self-report tool with 24 items (Albanesi et al., 2021). It was developed and validated in a multicenter study with convenience samples of nurses from seven different countries, using the Watson-Glaser Critical Thinking Appraisal instrument, a 56-item tool that assesses decision making in all its stages (Lauri & Salanterä, 2002; Sist & Palese, 2020).
Of the knowledge we have, only Albanesi et al. (2021) and Kim and Jung (2014) adapted the NDMI for the Italian and South Korean populations, respectively.
In the Italian context, the NDMI version demonstrated adequate content validity and reliability, having identified four factors that structure nurses’ decision-making process. However, the need to develop future investigations was identified to correlate decision making with the level of educational qualifications and level of competence of nurses (Albanesi et al., 2021).
In the study developed by Kim and Jung (2014), the instrument demonstrated satisfactory construct validity and reliability. However, contrary to the instructions of the author of the original instrument, the scores of the analytical items were not reversed and discrepancies emerged in the interpretation of the items in comparison with the results of the instrument development study.
In this way, and based on the studies carried out by Lauri and Salanterä (2002) and Sist and Palese (2020), the research team believes that this instrument can be used in training (i.e., to understand nurses’ decision making in a given context), research (i.e., to evaluate nurses’ decision making in a given nursing situation), or education (i.e. to enhance nursing students’ decision-making skills).
Therefore, it is important to evaluate nurses’ decision-making process to improve the quality of nursing care (Albanesi et al., 2021; Bjørk & Hamilton, 2011; Kim & Jung, 2014; Lauri et al., 2001; Sist & Palese, 2020).
The Clinical Decision-Making Nursing Scale is currently validated in Portugal, a work developed with nursing students by Duarte and Dixe (2021). However, it is a single instrument that allows evaluating the construct of nurses’ decision making. With a view to developing comparative studies in the future, and considering the lack of a valid alternative that allows this, this study aims to cultural adapt the NDMI into European Portuguese and evaluate the psychometric properties of the NDMI–Portuguese version (NDMI-PT).
Objectives
This study aimed to evaluate the psychometric properties of the NDMI-PT in a population of Portuguese nurses.
Methods
Design
A descriptive study design was used to examine psychometric properties of NDMI developed by Lauri and Salanterä (2002) adapted to the Portuguese nursing population.
Research Question
How is the version of the NDMI adapted to the Portuguese nursing population configured?
Setting, Sample, and Inclusion/Exclusion Criteria
The population consisted of all Portuguese nurses working in public or private health institutions in Portugal. The inclusion criteria were being a nurse working in direct patient care and agreeing to participate in the study.
To ensure a high response rate, the research team decided to involve the maximum number of participants from the target population, using a nonprobability convenience sampling technique.
The sample size was calculated to carry out an exploratory factor analysis (EFA) and a confirmatory factor analysis (CFA). For the EFA, a ratio of five subjects per item was used (Brymar & Cramer, 1992). For the CFA, Westland's (2010) formula (n ≥ 50r2–450r + 1100) was used, with an estimated 200 participants in which r = p/f (number of manifest variables/number of latent variables).
The sample consisted of 339 nurses, 278 women (82%), and 61 men (18%). Their mean age was 42 years (SD = 9; min. = 23; max. = 64). They had on average 19 years of professional experience (SD = 8.9; min. = 0.3; max. = 45), and 10.2 years of experience in their current workplace (SD = 8.1; min. = 0.1; max. = 40), as shown in Table 1.
Participants’ Sociodemographic Characteristics (n = 339).

Note. Portugal, PT, 2022.
% = Percentage; Max. = maximum; Min. = minimum; N = sample; SD = standard deviation.
With regard to academic qualifications, 0.6% of the participants held a bacharelato (3-year undergraduate degree), 63.7% held a bachelor's degree, 34.8% held a master's degree, and 0.9% held a Ph.D. in nursing.
Of the 339 participants, 76 (22.4%) had no postgraduate training, 67 (19.8%) had a postgraduate degree, 98 (28.9%) held the title of specialist in an area of nursing practice, and 28.9% had both.
Of the 57.8% of nurse specialists, 46% were categorized as specialist nurses by their employers.
The participants worked in various clinical settings, such as medical specialties (45.1%), surgical specialties (33.3%), community (14.2%), emergency (5.9%), long-term care (1.2%), and residential facilities for older people (0.3%).
The total sample was randomly divided into two subsamples. Of the 339 participants, 125 nurses were included in the EFA, while the remaining nurses (n = 214) were included in the CFA.
Data Collection
Data were collected in mainland Portugal and the Azores and Madeira archipelagos between May and July 2022.
The data collection instrument was made available by the Portuguese nursing regulator (Ordem dos Enfermeiros) on its website and social networks. It consisted of three parts: an introduction explaining the scope, nature, and objectives of the study; sociodemographic and professional questions; and the NDMI-PT.
The NDMI-PT, which consists of 24 items, was previously translated by the research team according to Beaton et al. (2000).
Of the 42 participants, six nurses (14.3%) reported difficulties in understanding items 6 (n = 2), 16 (n = 2) and 22 (n = 2). After consulting the original version of the instrument and its author, the necessary adjustments were made.
The NDMI-PT is rated on a five-point Likert scale (1: Never or almost rarely; 2: Rarely; 3: Sometimes; 4: Often, or 5: Almost or almost always).
To obtain the final score on the predominant decision-making style among nurses, the authors recommend maintaining the positioning of participants for even items and items 21 and 23 and reversing it for items 1, 3, 5, 7, 9, 11, 13, 15, 17, and 19.
The presence of odd items, with reverse scoring, prevents participants from expressing similar positions of agreement on the items that make up the scale. Even so, all items respect statements related to the poles of Hammond's Cognitive Continuum Theory: odd-numbered items respect statements related to the analytical pole of decision-making and even-numbered items with the intuitive pole of that process.
According to Lauri and Salanterä (2002) found that decision-making approaches can be categorized based on scores: analytical (24–67 points), flexible (68–77 points), and intuitive (78–120 points).
With regard to ethical principles in research, this study obtained a favorable opinion from the author of the original instrument and was submitted for consideration and approved by the Ethics Committee of the Health Sciences Research Unit: Nursing (process reference: P847_02_2022). Professor Sanna Salanterä monitored the development of the research, was the scientific consultant during the data analysis and processing process and gave us full permission to use the instrument.
The nurses gave their informed consent and were ensured the right to withdraw from the study. To ensure data confidentiality and anonymity, a code was assigned that did not reveal their identity.
Data Analysis
The NDMI was adapted into European Portuguese following Beaton et al.'s (2000) guidelines.
The psychometric properties were analyzed using IBM SPSS (version 24, SPSS An IBM Company, Chicago, IL, USA) and AMOS (version 22, An IBM Company, Chicago, IL, USA).
Descriptive statistics were calculated for each item and its sampling distribution (mean, standard deviation, skewness, and kurtosis). Skewness |Sk|<3 and kurtosis |Ku|<7 values indicated a normal distribution. To assess the structure of the NDMI-PT measurement model, an EFA was conducted on the correlation matrix. The factors were extracted using the principal components method with Varimax rotation. Factors with an eigenvalue greater than 1 were retained, as well as the Scree Plot and the percentage of variance retained, following the recommendation for triangulation of criteria to avoid retaining inadequate factors for describing the instrument's latent structure (Marôco, 2014). Cross-loadings greater than 0.4 were considered, and the magnitude of the loadings across the factors was subsequently assessed, taking to account the component where the item exhibits the strongest loading.
Then, a CFA was carried out to check if the data fitted the model under study. The presence of outliers was assessed using the squared Mahalanobis distance (D2). To adjust the model, sustained modifications were made to the modification indices (MI) (MI >11; p < .001) produced by the AMOS software. Different indices were used to assess the goodness-of-fit, with values of χ2/df < 5, comparative fit index (CFI) and goodness of fit index (GFI) > 0.90, Tucker-Lewis Index (TLI) > 0.90, root mean square error of approximation (RMSEA) < 0.08 being acceptable, with the lowest maximum-likelihood expected cross-validation index (MECVI) indicating the model with the best external validity (Byrne, 2010; Marôco, 2014).
Construct reliability and internal consistency were assessed using Cronbach's alpha (α) and composite reliability (CR), with values above 0.70 being considered adequate. Construct validity was assessed through factorial validity, convergent validity, and discriminant validity. Factorial validity is adequate when factor loadings are equal to or greater than 0.50, and individual reliability is equal to or greater than 0.25. Convergent validity is assessed by calculating the average variance extracted (AVE), with AVE ≥ 0.50 indicating convergent validity. Discriminant validity was established with two tests: (1) the χ2 difference test between the restricted model, assuming perfect correlation between factors, and the model with free correlation between factors, with a significant test indicating that the factors measure different constructs, as they are not perfectly correlated and (2) ensuring that the AVE of each of the two factors is equal to or greater than the square of the correlation between them (Marôco, 2014).
Results
Psychometric Analysis
The mean item response rate ranged from 3.76 (item 14) to 4.30 (item 8).
The item-total correlations were good, ranging from 0.61 (item 15) to 0.80 (items 11 and 18).
The descriptive analysis of the items revealed that skewness coefficients ranged from −1.45 to −0.68 and the kurtosis coefficients ranged from 0.48 to 3.58, indicating that the sample did follow a normal distribution (Table 2).
Descriptive Statistics of the Items of the NDMI-PT (n = 339).

Note. Portugal, PT, 2022.
EN = English version; I = item; Ku = kurtosis; NDMI-PT=Nursing Decision-Making Instrument–Portuguese version; PT = Portuguese version; SD = standard deviation; SEM = standard error of the mean; Sk = Skewness.
Exploratory Factor Analysis
The EFA sample adequacy test for the sample of 125 nurses showed that the distribution was suitable for data reduction based on the Kaise-Meyer-Olkin (KMO) criterion of 0.934 and Bartlett's test of sphericity with p < .001.
According to the eigenvalue greater than 1 criterion and the scree plot, the decision-making structure of the nurses who participated in the study is explained by four factors, which explain 69.52% of total variance (Table 3).
Factor Loadings of Each Item in the Four Retained Factors, Eigenvalues, and the Percentage of Variance Explained, After EFA With Factor Extraction Using the Principal Components Method With Varimax Rotation (n = 125).

Note. Portugal, PT, 2022. EFA= exploratory factor analysis; I = item.
All the communalities associated with the items were high (0.459–0.776), demonstrating that the four retained factors are adequate for describing the latent correlational structure of the four stages of nurses’ decision-making process.
Factor 1 had the highest eigenvalue, explaining 24.74% of the variance. It consisted of 10 items that mostly correspond to stages 1 and 4 of the decision-making process. Factor 2 explained 18.30% of the variance and included seven items that mostly correspond to stage 3 of the process. Factor 3 explained 14.69% of the variance and included four items that correspond to stage 2 of the process. Factor 4 explained 11.80% of the variance and included three items that correspond to stage 1 of the process.
The NDMI-PT shows excellent overall internal consistency (α=0.96) and the following values for each factor: factor 1 (10 items, α=0.94), factor 2 (7 items, α=0.91), factor 3 (4 items, α=0.86), and factor 4 (3 items, α=0.78).
Confirmatory Factor Analysis
To verify the adequacy of the data to the model, the CFA of the model resulting from the EFA and the original theoretical model was carried out on a sample of 214 nurses.
Confirmatory Factor Analysis of the Structure Resulting From the EFA
The model resulting from the EFA revealed an acceptable fit in the CFA, but most indices showed a poor fit (χ2/df = 2.86; CFI = 0.86; GFI = 0.76; TLI = 0.84; RMSEA = 0.09; MECVI = 3.88).
All items showed adequate normality values, but six observations with high D2 were considered multivariate outliers (p1 and p2 < .001). Following a conservative strategy, the data were reanalyzed excluding these observations, with evidence of a slight improvement in the fit indices.
The analysis of the MIs showed a strong correlation between the measurement errors of items 17 and 19 of factor 2 (MI = 24.69), as well as between items 7 and 8 (MI = 19.51) of factor 3, which is theoretically justified by the similarity of the content of the items, suggesting that the model should be refined.
After correlating the errors, the refined solution (Figure 1) showed a good fit for most of the indices (χ2/df = 2.13; CFI = 0.91; GFI = 0.82; TLI = 0.90; RMSEA = 0.07; MECVI = 3.13).

Factor structure of the refined model resulting from the EFA of the NDMI-PT. EFA= exploratory factor analysis; NDMI-PT=Nursing Decision-Making Instrument–Portuguese version.
The refined model, resulting from the EFA, fits better to the correlational structure between the items than the initial model (χ2(2) = 182.92; p < .05), with a lower MECVI (3.13 vs. 3.88).
Confirmatory Factor Analysis of the Theoretical Structure
The CFA of the theoretical structure revealed a poor fit for most indices (χ2/df = 2.90; CFI = 0.85; GFI = 0.76; TLI = 0.83; RMSEA = 0.09; MECVI = 3.93).
All the items had adequate normality values. However, seven observations with high D2 were considered multivariate outliers (p1 and p2 < .001). Therefore, following a conservative strategy, the analysis was redone excluding these observations, which resulted in an improvement in the fit indices.
The analysis of the MIs showed a strong correlation between the measurement errors of item 19 and the Planning and Evaluation factors (MI = 81.80 and 42.95, respectively). These items were removed from the model due to their correlation with other factors. A strong correlation was also found between the measurement errors of items 7 and 8 (MI = 50.74) of the Diagnosis factor, which is theoretically justified by the similarity of wording, suggesting that the model should be refined. After correlating the errors and removing item 19, a good fit was achieved (Figure 2; χ2/df = 1.82; CFI = 0.94; GFI = 0.83; TLI = 0.93; RMSEA = 0.06; MECVI = 2.55).
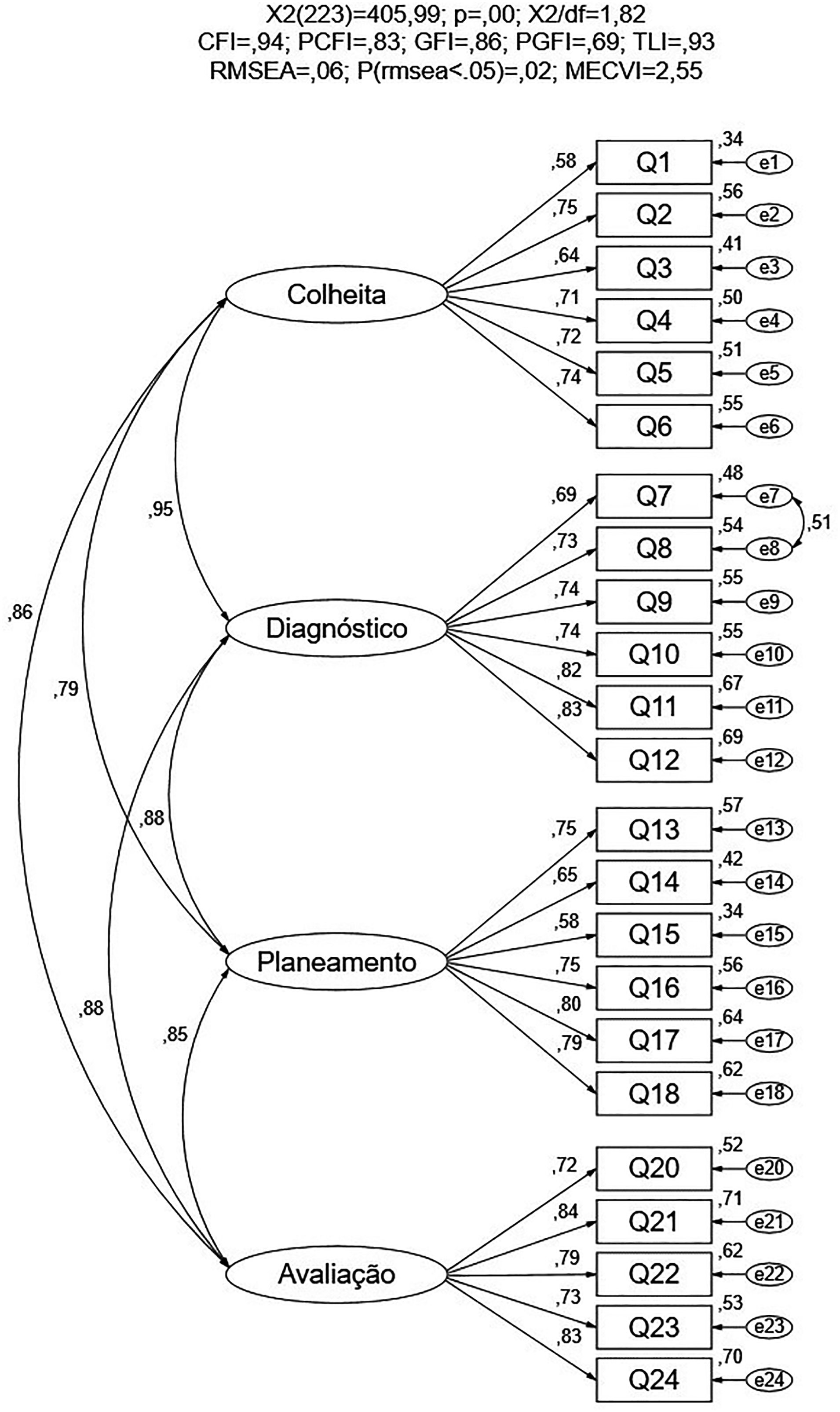
Factor structure of the refined model of the theoretical structure of the NDMI-PT. NDMI-PT=Nursing Decision-Making Instrument–Portuguese version.
The refined theoretical model fits the correlational structure observed between the items better than the original theoretical model (χ2(23) = 308.35; p < .05), showing a lower MECVI (2.55 vs. 3.93).
In this context, the factor solution obtained in the refined theoretical model seems to fit the correlational structure observed between the items better than the model resulting from the refined EFA (χ2(21) = 114.63; p < .05), also showing a lower MECVI (2.55 vs. 3.13) (Table 4).
Fit Indices of the Measurement Models.

Note. Portugal, PT, 2022.
χ2/df = Chi-square/degrees of freedom; CFI = comparative fit index; GFI = goodness of fit index; MECVI = maximum-likelihood expected cross-validation index; RMSEA = root mean square error of approximation; TLI = Tucker-Lewis Index.
The refined theoretical model demonstrated adequate construct in all dimensions (CF and α ≥ 0.85), as shown in Table 5.
Analysis of the Construct Reliability, Convergent Validity, and Discriminant Validity of NDMI-PT.

Note. Portugal, PT, 2022.
α = Cronbach's alpha; ρ2 = square of the correlation between factors; AVE = average variance extracted; CR = composite reliability; NDMI-PT=Nursing Decision-Making Instrument–Portuguese version.
The analysis of construct validity included the components of factorial validity, convergent validity, and discriminant validity. The standardized factor loadings ranged from 0.58 to 0.84 and the individual reliability of each item was also adequate, ranging from 0.34 to 0.71 (Figure 2). As for convergent validity, the AVE proved to be adequate in the Diagnosis, Planning, and Evaluation factors, and was close to acceptable in the Collection factor (AVE = 0.48), as shown in Table 5. With regard to discriminant validity, the χ2 difference tests showed that the correlation between each of the two factors was significantly different from 1 (p < .05), which indicates the discriminant validity of the factors. However, the AVE was lower than the square of the correlation between the factors (Table 5).
Discussion
The NDMI was cross-culturally adapted to the Portuguese reality following the guidelines recommended by Beaton et al. (2000).
To evaluate the psychometric properties of the NDMI-PT, EFA, and CFA were performed.
The cultural adaptation, and psychometric evaluation of the NDMI into European Portuguese is the starting point for assessing the decision-making skills of nurses who experience a cyclical paradox between the desire to care for patients and meeting the shortcomings of the organization and clinical practice standards, even if they do not master their field, but for which they are professionally responsible (Harvey et al., 2018).
The study used a global sample of 339 Portuguese nurses. The sample size for EFA was estimated at n = 120 and for CFA at n = 200.
Four factors emerged from the EFA, explaining 69.53% of the total variance, which seem appropriate for describing the latent correlational structure between the different stages of nurses’ decision-making process (Albanesi et al., 2021; Lauri et al., 2001). However, none of the factors is exclusively made up of items that correspond to each stage of the decision-making process. They have a mixed composition, with factor 1 including items from stages 1 and 4, factor 2 including items from stage 3, factor 3 including items from stage 2, and factor 4 including items from stage 1.
Overall, the instrument showed good internal consistency in the EFA subsample, with an α of 0.96, which is higher than in Finland (α: 0.85–0.90), Norway (α: 0.86), Korea (α: 0.89), or Italy (α: 0.92; Albanesi et al., 2021; Johansen & O’Brien, 2016; Kim & Jung, 2014).
In light of the knowledge available on the NDMI, the four-factor structure resulting from the EFA refers to a reorganization of the four stages of the decision-making process. This suggests that the sample studied may not make structured use of the decision-making process. This situation had already occurred in the studies carried out by Albanesi et al. (2021), who renamed the four factors Intuition, Prevision, Assessment, and Planning, and Kim and Jung (2014), who renamed the items Implementation of plan, monitoring and evaluation, plans of action, data collection, and data processing and identification.
The decision-making process has been reorganized into four factors due to the heterogeneity of the sample and the variation in decision-making depending on the cultural context, requiring the psychometric evaluation of this instrument to take place at each application (Albanesi et al., 2021).
The CFA of the model resulting from the EFA and the original theoretical model proposed by the authors of the NDMI were crucial in identifying the best factor solution for the sample under study.
From the CFA, the results of the MI analysis, based on theoretical, semantic, and conceptual grounds, led to the need to adapt and refine the original versions of both the theoretical model and the model resulting from the EFA. This refinement was achieved by correlating the errors of some items. In the theoretical model, item 19 was removed because it had a high correlation with factors other than the original factor—Evaluation. The refined models showed better fit indices than the original models in both cases. Moreover, the refined theoretical model fits the sample characteristics better than the refined model resulting from the EFA.
The studies carried out by Kim and Jung (2014) in South Korea and Albanesi et al. (2021) in Italy also found different factor structures from the original proposal by the authors of the NDMI, showing that the cultural context can influence nurses’ decision-making process.
This four-factor solution, resulting from the refined theoretical model, makes it possible to analyze the four stages of the decision-making process, namely collection, diagnosis, planning, and evaluation, as recommended by the authors of the instrument.
The analysis of the refined theoretical model revealed high construct reliability, as evidenced by the values of the HR and Cronbach's α. With regard to construct validity, the analysis showed factorial and convergent validity. However, the factor relating to the Collection stage shows convergent validity values close to acceptable, due to the high variability of the factor loadings of the items. The analysis of χ2 difference tests shows evidence of discriminant validity. However, the criterion of the AVE of the factors being greater than or equal to the square of the correlation between these factors does not provide clear evidence of discriminant validity. This result may indicate that the factors share a significant amount of common information, conditioning the discrimination of the measures obtained by each factor, which is intended to operationalize different latent variables.
Strengths and Limitations
This study made a fundamental contribution to increasing the knowledge of the psychometric properties of the NDMI-PT. It suggests that the proposed model is suitable for assessing nurses’ perceptions of nursing decision making in the Portuguese context. However, given the changes proposed in this refined version of the original version, an external validation should be conducted with a second independent sample to analyze the invariance and validation of the modified instrument.
On the other hand, the results should be analyzed while considering the limitations of the study, namely the heterogeneity of the contexts and the use of nonprobability sampling, which may affect the representativeness and generalizability of the results. Therefore, future studies should be conducted to implement the NDMI-PT in different contexts and explore different factor structures to identify the most appropriate factor solution for the Portuguese cultural context.
To make it easier for nurses to position themselves in the decision-making process when answering the instrument, the research team suggests subdividing the NDMI-PT into four sections that represent the stages of the decision-making process.
Implications for Practice
This instrument opens the door to research on nurses’ decision-making process and the training of nursing students in Portugal, which can lead to the development of strategies for providing more efficient and effective care.
Conclusions
Considering that the influence of nurses’ decision-making process on healthcare is one of today's challenges, this study is a notable advance in the psychometric analysis of the NDMI-PT as a means of exploring nurses’ decision making in Portugal.
This study was the first to validate the NDMI for the Portuguese health context and the NDMI-PT is only the second instrument capable of being used in the country to evaluate the decision-making process of nurses. The results of the factor analysis suggest refining the original model to obtain a factor solution with good goodness-of-fit. The NDMI-PT demonstrated high reliability and construct validity. However, further studies are needed to determine its cross-cultural validity.
Supplemental Material
sj-pdf-1-son-10.1177_23779608241278611 - Supplemental material for Cultural Adaptation and Psychometric Evaluation of the Nursing Decision-Making Instrument Into European Portuguese
Supplemental material, sj-pdf-1-son-10.1177_23779608241278611 for Cultural Adaptation and Psychometric Evaluation of the Nursing Decision-Making Instrument Into European Portuguese by Ivo Cristiano Soares Paiva, Teresa Margarida Almeida Neves, Filipa Isabel Quaresma Santos Ventura, António Carlos Lopes Vilela and Isabel Maria Pinheiro Borges Moreira in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608241278611 - Supplemental material for Cultural Adaptation and Psychometric Evaluation of the Nursing Decision-Making Instrument Into European Portuguese
Supplemental material, sj-pdf-2-son-10.1177_23779608241278611 for Cultural Adaptation and Psychometric Evaluation of the Nursing Decision-Making Instrument Into European Portuguese by Ivo Cristiano Soares Paiva, Teresa Margarida Almeida Neves, Filipa Isabel Quaresma Santos Ventura, António Carlos Lopes Vilela and Isabel Maria Pinheiro Borges Moreira in SAGE Open Nursing
Footnotes
Author Contributions
TMAN was involved in conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, resources, software, visualization, writing—original draft preparation, and writing—review & editing. FIQSV was involved in formal analysis, methodology, software, supervision, and writing—review & editing. ACLV was involved in conceptualization, formal analysis, methodology, project administration, software, supervision, validation, and writing—review & editing. IMPBM was involved in conceptualization, formal analysis, methodology, project administration, supervision, validation, and writing—review & editing.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study was submitted for consideration and approved by the Ethics Committee of the Health Sciences Research Unit: Nursing (process reference: P847_02_2022). Before completing the data collection instrument, an explanatory introductory text was presented to the participants, which consisted of obtaining written informed consent.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.