
Abstract
Background
Comorbid anxiety in hypertensive patients yields poor remedy adherence which may additionally restrict treatment choices.
Objective
To assess the magnitude and severity of anxiety and risk factors among hypertensive patients attending public hospitals in Arba Minch town, Ethiopia, 2022.
Methods
A hospital-based cross-sectional study design was performed from June 1 to July 30/2022. The overall sample size was 336 and a systematic random sampling technique was used to pick out sufferers. Used Epi data version 3.1 for data entry and SPSS version 25 for analysis. Logistic regression analysis was done and variables with p-values less than .25 were taken into multivariable. Statistical significance was declared at a p-value of less than .05 with a 95% confidence interval in the adjusted odds ratio.
Result
The magnitude of anxiety among hypertensive patients was 32.1% with 95% CI (26.2%–37.1%). Sex [AOR: 2.25, 95%CI: 1.22–4.13], status of blood pressure [AOR: 0.30, 95%CI: 0.15–0.63], family history of hypertension [AOR: 2.48, 95%CI: 1.20–5.12], family history of mental illness [AOR: 0.19, 95%CI: 0.09–0.39], history of admission [AOR: 5.14, 95%CI: 2.73–9.68], social support status [AOR: 2.96, 95%CI: 1.09–7.97], and current alcohol use [AOR: 0.39, 95%CI: 0.18–0.86] had been notably related.
Conclusion
About three in 10 hypertensive patients attending public hospitals in Arba Minch town public hospitals were anxious. Approximately two in 10 hypertensive sufferers had moderate to severe anxiety. Sex, status of blood pressure, family history of hypertension, family history of mental illness, history of admission, social support status, and current alcohol use have been substantially associated with anxiety among hypertensive patients. Therefore, enhancing gender identity, controlling blood pressure, screening and treating a family history of high blood pressure and family history of mental illness, coping with previous admission, improving social help, and cessation of alcohol use might lessen the burden of anxiety among hypertensive sufferers.
Introduction
Raised blood pressure is a chief cardiovascular chance element and out of control, hypertension reasons stroke, myocardial infarction, cardiac failure, dementia, renal failure, and blindness and ends in humans struggling and implementing extreme economic and service burdens on health systems (Abdisa et al., 2022; Marina et al., 2012; Nigusu et al., 2023). Raised blood pressure is one of the leading risk factors for worldwide mortality and is predicted to have induced 9.4 million deaths and 7% of sickness burden, as measured in disability-adjusted life years (Shah et al., 2022; Shanthi et al., 2014).
Mental illnesses are common in all international locations and have a sizeable effect on socioeconomic development and growth (Ambikile & Iseselo, 2017). At some unspecified time in their lives, more than a quarter of the global population is afflicted by a mental illness (Bacon et al., 2014). Patients with chronic illnesses like hypertension have a great tendency to acquire anxiety (Kessler et al., 2009).
Internationally, anxiety problems are ranked as the sixth biggest contributor to nondead fitness loss (WHO, 2017). Anxiety is always better in people stricken by persistent illnesses. Like patients with different persistent medical conditions, hypertensive patients enjoy many profound emotions that increase the chance of the development of mental health disorders, particularly anxiety (DeJean et al., 2013; Gebre et al., 2020; Shah et al., 2022).
Literature Review
Various studies show that biological and psychosocial factors are associated with anxiety among people with hypertension. These included gender, physical activity, socioeconomic status, concern about medication and poor blood pressure control (Ademola et al., 2019), comorbid chronic illness (Hamrah et al., 2018), older age, family history, being a woman (Abdisa et al., 2022; Hamrah et al., 2018), stressful life event, diabetic, poor social support (Aberha et al., 2016; Nigusu et al., 2023), weight change, and low income (AlKhathami et al., 2017).
In hypertensive patients, anxiety is associated with poor health status, which includes low-quality lifestyles (Rueda & Perez-Garcia, 2013), lower rate of remedy compliance (Moise et al., 2014), or even increased mortality (Oganov et al., 2011). People with anxiety are afflicted by a lack of occupational and social role features (Kretchy et al., 2014).
Anxiety in hypertensive patients outcomes in poor remedy adherence which may additionally restrict treatment choices, get worse patient analysis, and boost morbidity and mortality (Kretchy et al., 2014). Unhealthy lifestyles, including intake of alcohol, smoking, dangerous eating regimens, and physical inaction are related to anxiety in sufferers at risk of cardiovascular ailment (Bitew, 2014; FDRE Ministry of Health, 2014; Gebre et al., 2020; Shah et al., 2022).
Determining the magnitude and severity of anxiety in hypertensive patients offers a clear picture of its burden. Addressing and identifying factors related to anxiety and its severity among hypertensive patients enables to enhancement of patients’ compliance with the endorsed way of life and adherence to the antihypertensive treatment (DeJean et al., 2013). As a result, this study assessed the magnitude and severity of anxiety and risk factors among hypertensive patients attending public hospitals in Arba Minch town.
Methods and Materials
Study Area and Period
The look-at was performed in Arba Minch town. The town is the capital of the Gamo zone. It is found 505 km south of Addis Ababa. Primarily based on the 2007 Ethiopian census document, the projected population of Arba Minch town has a total population of 118,040. Arba Minch town has one General hospital, one primary hospital, and two public health centers. The study was carried out from June 1 to July 30/2022.
Study Design
A hospital-based cross-sectional study design was employed.
Source Population
All hypertensive patients attending public hospitals in Arba Minch town.
Study Population
All selected hypertensive patients attending public hospitals in Arba Minch town.
Eligibility Criteria
All hypertensive patients attending public hospitals in Arba Minch town for the duration of the study period have been included; however, hypertensive patients aged less than 18 years old, critically ill patients, and patients with excessive psychiatric disorders that could not give accurate responses were excluded from the study.
Sample Size Determination
The sample size was determined by using a single population formula. The assumptions used to calculate the sample size were proportion anxiety 0.295% taken from a previous study (Asmare et al., 2022) with a 95% confidence level and a margin of error of 5% as follows.

Sampling Technique and Approaches
The two public hospitals that hypertensive patients attend in the city (Arba Minch General Hospital and Dilfana Primary Hospital) have been blanketed in the observation. Then, the 2 months (April and May/2022) attending a report of each hospital become determined. The two-month record of Arba Minch General Hospital was 1,030 and Dilfana Primary Hospital was 158 patients. Subsequently, the determined number became proportionally allotted according to the entire sample size. Later, the patients for an interview in every hospital were decided on with the aid of the usage of a systematic random sampling approach primarily based on the calculated constant value, which became 1188/336 = 3, the constant value was 3 and the data collectors interviewed every regular three intervals day by day in every hospital and the first interview patient was determined by a lottery approach (Figure 1).

Schematic Diagram Displaying Sampling Method of Magnitude and Severity of Anxiety among Hypertensive Patients Attending Public Hospitals of Arba Minch Town, Ethiopia, 2022.
Operational Definitions
Hypertension
An upward thrust in blood pressure when systolic blood stress is ≥140 mm Hg and/or diastolic blood pressure is ≥90 mm Hg (Asmare et al., 2022; WHO, 2013).
Anxiety
It was assessed using seven hospital anxiety subscale questions, each question has 3 response options. The score changed into computed and in every one of the subscales, the scores ranged from 0 to 21. Subsequently, categorized as anxious (if scored ≥ eight) or not anxious (if scored < 8). Similarly, the severity of anxiety was categorized as no or minimal (if scored 0–4), mild (if scored from 5 to 9), moderate (if scored 10–14), or severe (if scored > 14) (Abdisa et al., 2022; Shah et al., 2022).
Current Smoker
When the patient has been smoking cigarettes for the past month (Asmare et al., 2022).
Current Drinker
When the patient has been drinking alcohol-containing drinks in the past month (Asmare et al., 2022).
Current Chat Chewer
When the patient has been chewing chat within the past month (Asmare et al., 2022).
Data Tool and Data Collection Procedure
The tool was organized in English and was a structured questionnaire collected through face-to-face interviews with patients inside the hospital. The statistics were gathered through two clinical nurses and supervised by an experienced epidemiologist.
Data Quality Assurance
The tool was adapted from formerly demonstrated hospital anxiety Scale formats prepared in English. The hospital anxiety Scale has seven questions that verify anxiety. In each of the subscales, the ratings vary from 0 to 21. The better the rating is, the more the signs and symptoms (James et al., 2014; Reda, 2011; WHO, 2013; Zigmond & Snaith, 1983). The tool has been validated in the Ethiopian context (Reda, 2011). It was translated to Amharic earlier than data collection and back to English after data collection to make certain consistency. One day training was given for data collectors and supervisors about, how to pick out the study participants, a way to preserve the confidentiality of statistics, the contents of the questionnaire, and the way to interview and fill on the questionnaire. A pretest was carried out on 5% of the total sample size at Geresse Primary Hospital and modified and executed primarily based on the pretest. The supervisor conducted every day comply with us throughout the complete period of data collection. Each questionnaire was reviewed and checked for completeness by way of the investigators.
Data Processing and Analysis
Data was entered into Epi data 3.1 and then exported to the SPSS version 25 for analysis. Data cleansing was performed to check for missed values after which descriptive analysis along with proportions, frequencies, and percentages was carried out and tables and graphs were used for presentation. Multicollinearity is checked by considering the variance inflation factor greater than 10 and tolerance less than 0.05. Goodness of fit test was performed using the Hosmer–Lemeshow goodness of fit test. To test the association between the independent and the outcome variable, a logistic regression analysis was executed. Variables significant in bivariate analysis with a p-value less than .25 were entered in multivariable analysis to pick out the independent association of impartial variables with anxiety. In the end, a significant independent association was interpreted at a p-value of less than .05 with 95%CI.
Result
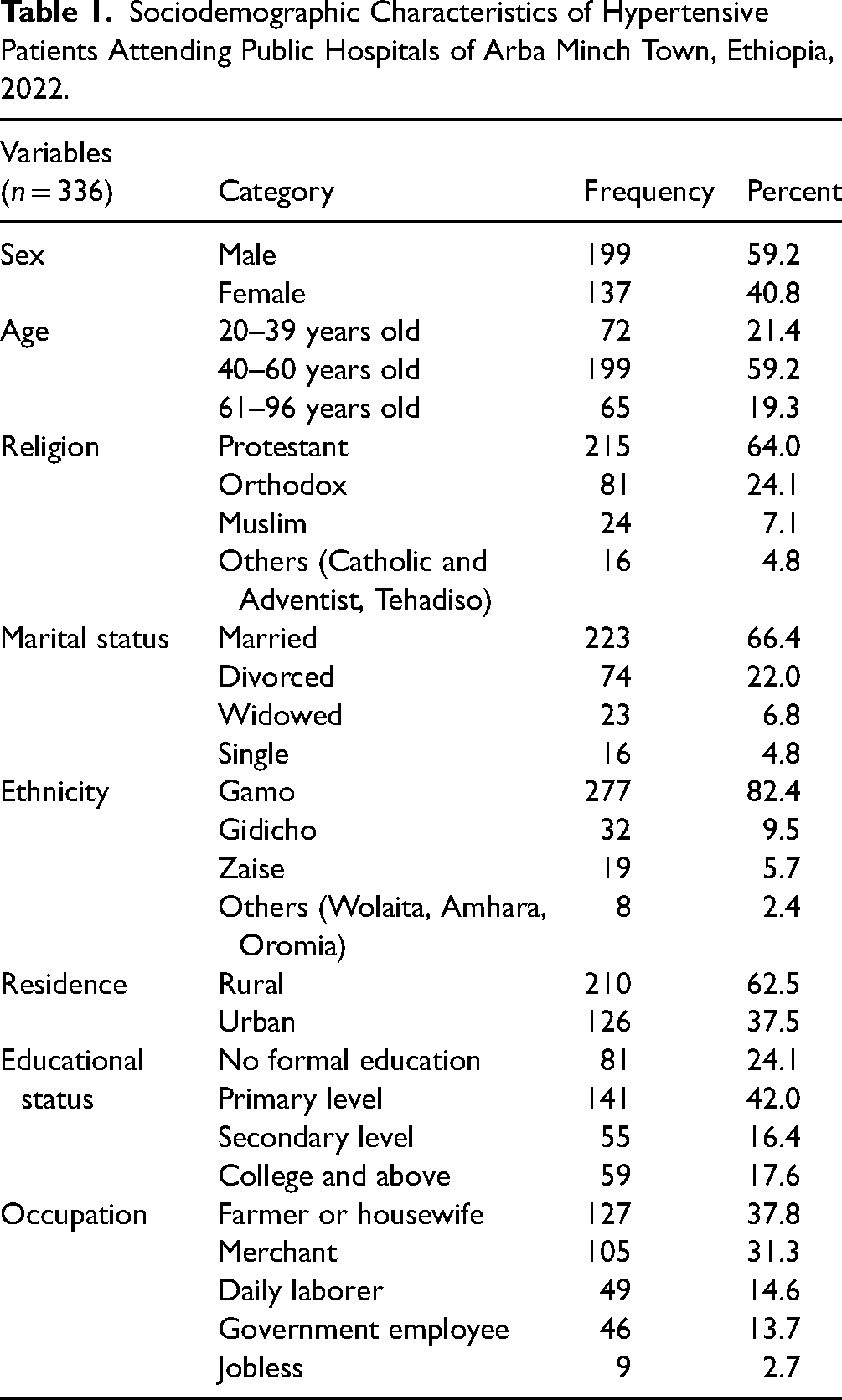
Sociodemographic Characteristics of Hypertensive Patients
A total of three hundred thirty-six hypertensive patients spoke back to the interview making an overall response of 100%. Of the sex more than half, 199(59.2%) were male and the age group of 199(59.2%) were in the age group of 40–60 years old. More than half of, 215(64.0%) of the contributors, were followers of the protestant religion and in addition, 223(66.4%) were married. The ethnicity of 277(82.4%) became Gamo and the residents of greater than half, 210(62.5%) were from rural. Regarding educational status, 81(24.1%) had no formal schooling and the occupation of 127(37.8%) were farmers or housewives (Table 1).
Sociodemographic Characteristics of Hypertensive Patients Attending Public Hospitals of Arba Minch Town, Ethiopia, 2022.
Clinical-Related Characteristics of Hypertensive Patients
The blood pressure of more than half, 220 (65.5%) participants was controlled and the body mass index of 220(65.5%) was 19.12–24.9 kg/m2. Most of the participants 227(67.6%) had no family history of high blood pressure and more than half, 251(74.7%) had no family history of mental illness. Greater than half, 195(58.0%) had a record of admission, and the majority, 288(85.7%) did not have diagnosed comorbid chronic medical illness (Table 2).
Clinical-Related Factors of Hypertensive Patients Attending Public Hospitals of Arba Minch Town, Ethiopia, 2022.

* Diabetes mellitus, myocardial infarction, thyrotoxicosis, ischemic heart disorder, persistent heart sickness, and persistent kidney disease.
Medical-Related Characteristics of Hypertensive Patients
Less than half, 120(35.7%) acquire a single antihypertensive medicinal drug, however, the rest 216(64.3%) get hold of a combination of two or more antihypertensive medicines. The period of remedy for the majority of the respondents, 284(84.5%) was found to be less than 10 years, but, for 52(15.5%) it was greater than or equal to 10 years. The medicine of 148(44.0%), 58(17.3%), and 130(38.7%) hypertensive patients had low, moderate, and high medication adherence respectively.
Psychological and Behavioral Characteristics of Hypertensive Patients
Out of the 336 hypertensive patients, the most effective 79(23.5%) have been current alcohol users, but the rest 257(76.5%) have been not. Further, 53(15.8%) had been current smokers, on the other hand, 283(84.2%) had been not. Concerning chat, 70(20.8%) had been current chat chewers, but, 266(79.2%) had been not current chat chewers. The social help of 189(56.3%), 42(12.5%), and 105(31.2%) hypertensive patients had low, moderate, and high social assistance respectively.
Magnitude of Anxiety Among Hypertensive Patients
Out of 336 hypertensive patients, 228(67.9%) have been not anxious, but, 108(32.1%) were anxious (Figure 2).
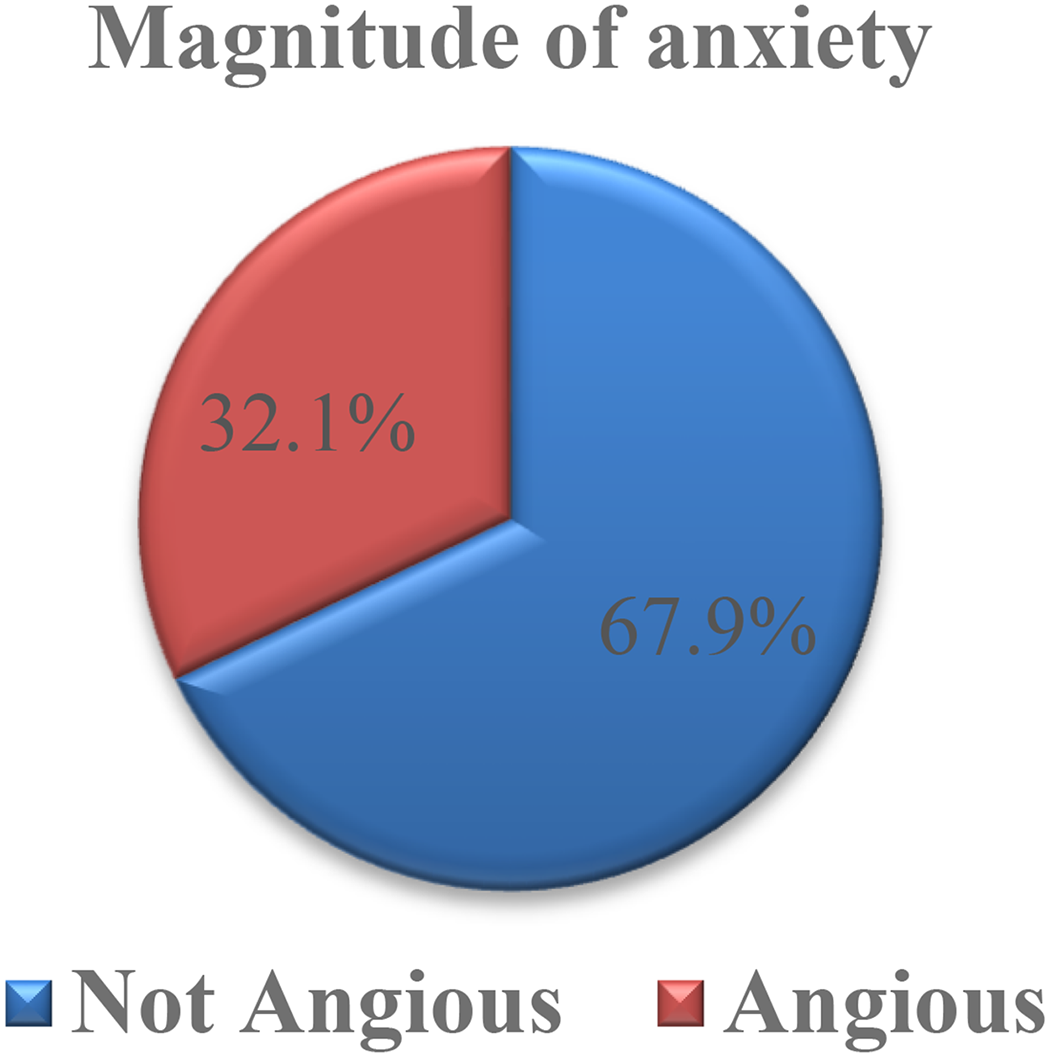
Magnitude of anxiety among hypertensive patients attending public hospitals of Arba Minch town, Ethiopia, 2022 (n = 336).
Severity of Anxiety Among Hypertensive Patients
Out of the 336 hypertensive patients, 148(44.1%) had no anxiety, 35(10.4%) had mild anxiety, 70(20.8%) had moderate anxiety, and 83(24.7%) had severe anxiety (Figure 3).

Severity of Anxiety among Hypertensive Patients Attending Public Hospitals of Arba Minch Town, Ethiopia, 2022 (n = 336).
Factors Associated With Anxiety Among Hypertensive Patients
In bivariable logistic regression analysis; sex, age, status of blood pressure, body mass index, family history of hypertension, family history of mental illness, records of admission, comorbid chronic illness, social support status, current alcohol use, and current smoking had been substantially related to anxiety among hypertensive patients. Whereas in multivariable logistic regression analysis; sex [AOR: 2.25, 95%CI: 1.22–4.13], the status of blood pressure [AOR: 0.30, 95%CI: 0.15–0.63], family history of hypertension [AOR: 2.48, 95%CI: 1.20–5.12], family history of mental illness [AOR: 0.19, 95%CI: 0.09–0.39], history of admission [AOR: 5.14, 95%CI: 2.73–9.68], social support status [AOR: 2.96, 95%CI: 1.09–7.97], and current alcohol use [AOR: 0.39, 95%CI: 0.18–0.86] were substantially associated with anxiety among hypertensive patients (Table 3).
Factors Associated with Anxiety among Hypertensive Patients Attending Public Hospitals of Arba Minch Town, Ethiopia, 2022.
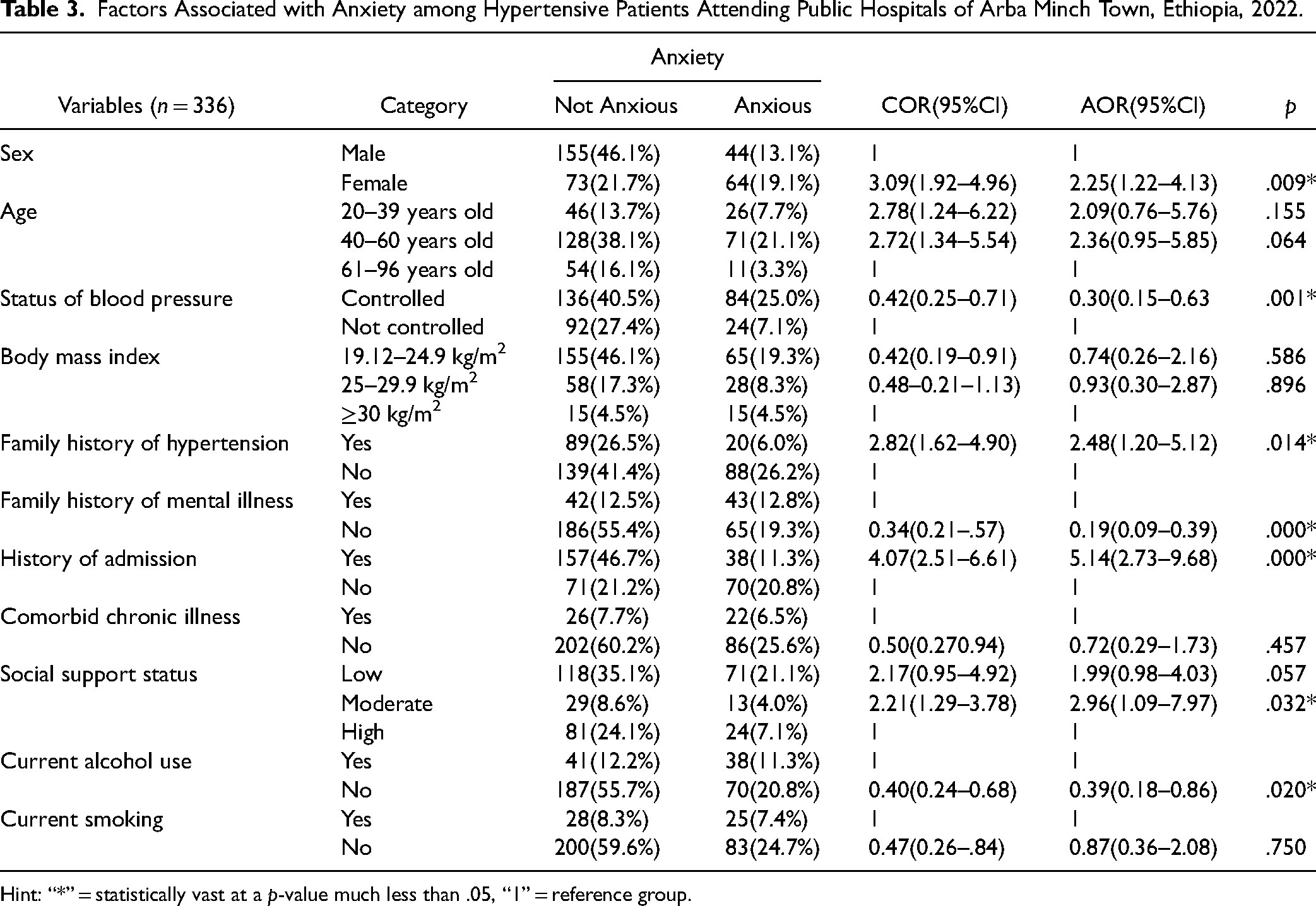
Hint: “*” = statistically vast at a p-value much less than .05, “1” = reference group.
Discussion
The importance of tension among hypertensive patients becomes 32.1% with 95% CI (26.2%–37.1%). It was consistent with studies performed in unique hospitals of Addis Ababa, 28.5% (Aberha et al., 2016; Asmare et al., 2022) and 32.7% in eastern Ethiopia (Abdisa et al., 2022). This might be due to similarities in study design and comparable behavioral characteristics of respondents. However, it was lower than research in Afghanistan 42.3% (Hamrah et al., 2018), Ghana 57% (Kretchy et al., 2014), and Saudi Arabia 38.4% (AlKhathami et al., 2017). This discrepancy might be because of differences that would arise from cultural and environmental differences. Similarly, statistics collection contraptions and the financial status of the study participants may contribute to this change.
The study discovered that 44.1% of hypertensive sufferers had no anxiety, 10.4% had mild anxiety, 20.8% had moderate anxiety, and 24.7% had severe anxiety. This is just like other studies that indicated patients with hypertension had slight to extreme anxiety disorders (AlKhathami et al., 2017; Shah et al., 2022).
In this study, sex was statistically associated with anxiety among hypertensive patients. Female hypertensive patients were 2.25 instances more likely to have anxiety as compared to male hypertensive patients. It is similar to a study carried out in Al-Khobar, Saudi Arabia (AlKhathami et al., 2017) and Nepal (Shah et al., 2022). This link is probably explained in part using the fact that tension has been connected to hormonal changes associated with pregnancy, postpartum, and postmenopausal durations in ladies’ lives (Russell et al., 2013). Furthermore, Ethiopian girls are greater liable to intellectual illnesses due to socio-cultural and environmental issues. Additionally, divorced/widowed respondents had a better chance of hysteria because after they experience lonely, lack desire, are worthless, and grow to be aggravated.
Blood pressure status was statistically related to anxiety among hypertensive sufferers. Hypertensive patients whose blood stress was managed were 70% less likely to have anxiety compared to hypertensive patients whose blood pressure was not controlled. This might have originated from the sufferers’ belief regarding the multiplied blood pressure.
A family history of high blood pressure changed into statistically related to anxiety among hypertensive patients. Hypertensive sufferers who had a circle of family records of high blood pressure were 2.48 times more likely to have anxiety as compared to hypertensive patients who did not have family records of hypertension. This might be because of the conditions shared by way of households, which include eating and consuming fashion, monetary fame of the own family, and environmental situations that could predispose them to tension.
A family history of a mental illness turned into statistically related to anxiety among hypertensive sufferers. Hypertensive patients who did not have a family history of mental illness were 81% less likely to have anxiety in comparison to hypertensive sufferers who had family records of mental illness. This was much like some other study accomplished in eastern Ethiopia. This might be because if one parent has a mental problem, the child has a hazard of growing it. After all, they proportion comparable lifestyles and psychosocial strain (Abdisa et al., 2022; Gebre et al., 2020).
Records of admission became statistically related to anxiety among hypertensive patients. Hypertensive sufferers who had a history of admission were 5.14 instances more likely to have anxiety in comparison to hypertensive sufferers who no longer have a record of admission. This is probably because of the mental instabilities that can arise from situations preceding admission, like medical institution surroundings, length of time in hospital, type of sickness diagnosed, and the way they controlled would possibly make them develop tension.
Social support status became statistically associated with anxiety among hypertensive sufferers. Hypertensive patients whose social help reputation became mild have been 2.96 times more likely to have anxiety compared to hypertensive patients whose social assistance reputation turned high. This is supported by other research carried out in various countries (Aberha et al., 2016; Abdisa et al., 2022; Gebre et al., 2020). This is probably because of the perceived feeling of being on my own and remoted which ends in multiplied psychosocial strain, and on the contrary, desirable social support reduces the danger of anxiety.
Current alcohol use is statistically associated with anxiety among hypertensive patients. Hypertensive patients who no longer use alcohol currently are 61% less in all likelihood to have anxiety in comparison to hypertensive patients who use alcohol currently. A possible explanation could be the influence of health effects, social problems, and economic and productivity loss due to continuous alcohol consumption.
Limitations of the Study
The study might be susceptible to recall bias as it asks back, and it might be prone to social-cultural desirability bias as the community gives their own concern for illness.
Implications for Nursing Practice
Assessing the magnitude and severity of anxiety among hypertensive patients is a vital action to manage in a clinical setting. Additionally, determining the factors that hinder or enhance anxiety among hypertensive patients is a clue in policy-making. Health stakeholders can have better results if develop strategic interventions regarding enhancing gender identification, controlling blood pressure, screening and treating family records of high blood pressure and mental illness, coping with preceding admission, enhancing social guidance, and cessation of alcohol use might lessen the load of anxiety among hypertensive patients.
Conclusion
About 3 in 10 hypertensive patients attending public hospitals in Arba Minch town were irritating from anxiety. About 2 in 10 hypertensive patients had moderate and severe anxiety. Sex, status of blood pressure, family history of hypertension, family history of mental illness, records of admission, social assistance reputation, and current alcohol use have been considerably associated with anxiety among hypertensive sufferers. Therefore, enhancing gender identification, controlling blood pressure, screening and treating family records of high blood pressure and mental illness, coping with preceding admission, enhancing social guidance, and cessation of alcohol use might lessen the load of anxiety among hypertensive patients.
Supplemental Material
sj-docx-1-son-10.1177_23779608241276764 - Supplemental material for Magnitude and Severity of Anxiety and Risk Factors among Hypertensive Patients Attending Public Hospitals in Arba Minch Town, Ethiopia
Supplemental material, sj-docx-1-son-10.1177_23779608241276764 for Magnitude and Severity of Anxiety and Risk Factors among Hypertensive Patients Attending Public Hospitals in Arba Minch Town, Ethiopia by Andinet Akililu, Elias Ezo, Wubishet Gezimu, Elias Nigusu, Taye Mezgebu, Asnakech Zekiwos, Bethelhem Birhanu, Getachew Ossabo and Sentayehu Admasu in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241276764 - Supplemental material for Magnitude and Severity of Anxiety and Risk Factors among Hypertensive Patients Attending Public Hospitals in Arba Minch Town, Ethiopia
Supplemental material, sj-docx-2-son-10.1177_23779608241276764 for Magnitude and Severity of Anxiety and Risk Factors among Hypertensive Patients Attending Public Hospitals in Arba Minch Town, Ethiopia by Andinet Akililu, Elias Ezo, Wubishet Gezimu, Elias Nigusu, Taye Mezgebu, Asnakech Zekiwos, Bethelhem Birhanu, Getachew Ossabo and Sentayehu Admasu in SAGE Open Nursing
Footnotes
Acknowledgments
We would like to thank the study participants for the scarification of their precious time.
Authors’ Contribution
Elias Ezo, Andinet Akililu, and Wubishet Gezimu: conceptualization, data curation, formal analysis, investigation, methodology, supervision, validation, visualization, writing-original draft, writing-review and editing. Elias Ezo, Elias Nigusu, Taye Mezgebu, and Asnakech Zekiwos: conceptualization, data curation, formal analysis, investigation, methodology, supervision, validation, visualization, writing-original draft, and writing-review and editing. Elias Ezo, Andinet Akililu, Bethelhem Birhanu, Getachew Ossabo, and Sentayehu Admasu: conceptualization, formal analysis, methodology, software, writing-review and editing. Elias Ezo, Taye Mezgebu, and Asnakech Zekiwos: conceptualization, formal analysis, methodology, software, writing-review and editing. Elias Ezo, Taye Mezgebu, Wubishet Gezimu, and Sentayehu Admasu: conceptualization, formal analysis, methodology, software, writing-review and editing. Elias Ezo, Elias Nigusu, Bethelhem Birhanu, and Getachew Ossabo: conceptualization, formal analysis, methodology, supervision, visualization, writing-original draft, writing-review & editing. Elias Ezo, Wubishet Gezimu, and Asnakech Zekiwos: conceptualization, formal analysis, methodology, software, writing-review and editing.
Availability of Data
The data used for this study are available from the corresponding author on secured and reasonable request
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
The research ethical review committee of Paramed College approved the proposal for this research (PMC/AM/32/14). Then, another support letter was sent to each hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Data collectors gave written informed consent, asked for openness, and explained the necessity including the aim and purpose of data collection, confidentiality, and privacy were introduced and kept. The right of respondents to stop after starting the interview or reject the interview was clearly explained by the data collectors before starting the interview.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.