
Abstract
Introduction
Diabetes mellitus (DM) is one of the world's major public health problems. There are few published data on 25-hydroxyvitamin D (25[OH]D) concentrations and DM, and these studies showed different results.
Objectives
The current study aimed to compare 25[OH]D concentrations between patients with type 2 DM (T2DM) and healthy controls in eastern Sudan.
Methods
A case–control study of two groups matched for age and gender (88 in each group) was conducted in eastern Sudan from March to May 2022. The cases were patients with T2DM, and the controls were healthy participants. Sociodemographic data were collected, and serum 25(OH)D levels were assessed. A univariate analysis was performed.
Results
Of the total 176, 82 (47%) were males, and 94 (53%) were females; the median (interquartile range [IQR]) of age, body mass index (BMI), and 25(OH)D concentration were 55 (50–61) years, 27 (23–31) kg/m2, and 13 (10–19) ng/mL, respectively. Of the 176, 137 (78%) were vitamin D deficiency cases. Compared with the controls, age, gender, educational level, marital status, or BMI were not different in the circumstances. Moreover, the median (IQR) for serum 25(OH)D concentrations showed no difference between patients with T2DM and the healthy controls (12 [10–18] ng/mL vs. 13 [10–20] ng/mL). The prevalence of vitamin D deficiency (25(OH)D level < 20 ng/mL) was not different between patients with T2DM and the healthy controls (66/88 [75%] vs. 71/88 [81%]). There was no association in the serum 25(OH)D levels between diabetic and nondiabetic participants (OR = 1.01, 95% CI 0.97–1.06) or in vitamin D deficiency between diabetic and nondiabetic participants (OR = 0.72, 95% CI 0.35–1.47).
Conclusion
There was no significant difference in 25(OH)D levels between diabetic and nondiabetic participants in this study. Further studies investigating the mechanisms of association between 25(OH)D levels and DM are needed.
Introduction
Diabetes mellitus (DM), especially type 2 (T2DM), is one of the leading global public health problems (Magliano & Boyko, 2021). The economic and social burden of DM is significantly more significant in settings with limited resources, such as Africa, including Sudan, where DM with its complications is prevalent (Abdelbagi et al., 2021; Mapa-Tassou et al., 2019; Omer et al., 2018). Several factors, such as older age, family history of DM, and high body mass index (BMI)/obesity, have been observed as risk factors for T2DM (Ali et al., 2017; Eltom et al., 2018; Omer et al., 2018).
Review of Literature
Vitamin D is one of the fat-soluble vitamins, and it has an essential/vital role in health (Melmed et al., 2019). Several diseases, such as DM, chronic hypertension, obesity and higher BMI, cardiovascular and metabolic syndrome, Alzheimer's disease, and mental illness, are reported to be associated with 25-hydroxyvitamin D (25[OH]D) concentrations or vitamin D status (Barrea et al., 2021; Liu et al., 2022; Sinema et al., 2021; Soh et al., 2021; Zainel et al., 2019). Likewise, DM and low 25[OH]D levels or vitamin D deficiency are major public health problems worldwide, especially in African countries (Mogire et al., 2020).
While some studies have reported a positive association between low levels of 25[OH]D or vitamin D deficiency and DM (Khudayar et al., 2022; Nasr et al., 2022; Park et al., 2018; Zhang et al., 2016), others have reported no association between vitamin D and DM (Fondjo et al., 2017; Sheth et al., 2015). Nevertheless, the high prevalence of vitamin D deficiency and its effects on the population's health require urgent public health intervention (Darling, 2020). Therefore, the optimum steps are needed to address vitamin D deficiency and its consequences for the health of the community. To achieve this, the prevalence of vitamin D in the community and its association with noncommunicable diseases such as DM must be investigated first. Based on that, appropriate, optimum healthcare and preventive measures can be applied as needed. The previous data show a high prevalence of T2DM and its complications among Sudanese adults (Abdelbagi et al., 2021; Omer et al., 2018). For example, a cross-sectional community-based study that was conducted in eastern Sudan and included 600 adults showed a high prevalence of DM (30%), and 80.0% of adults with DM had uncontrolled disease (Omer et al., 2018). On the other hand, high prevalence rates of vitamin D deficiency and its complications across the country regions in different groups, including children and adults, were reported in Sudan (Hassan et al., 2023). While the association between vitamin D and DM has been studied in other countries (Fondjo et al., 2017; Khudayar et al., 2022; Nasr et al., 2022; Sheth et al., 2015; Zhang et al., 2016). However, such an association has not yet been investigated in Sudan, where vitamin D and DM are prevalent (Abdelbagi et al., 2021; Husain et al., 2017; Omer et al., 2018). Thus, the current study aimed to compare 25[OH]D levels between patients with T2DM and healthy controls in eastern Sudan.
Methods
Study Design
A case–control study was conducted in Gadarif, eastern Sudan.
Research Question
Is there any difference in the serum 25[OH]D concentrations between patients with T2DM and healthy controls in eastern Sudan?
Sample
Details of the study area and procedures were mentioned in our previous work (Of Nat & Environ, n.d.; Omar et al., 2019). In summary, a case–control study was conducted during the period of March to May 2022. It was conducted in Gadarif State, eastern Sudan, which is one of the 18 states of Sudan. According to the 2008 census, the total population of Gadarif State was 1,400,000 people (5th Sudan Population and Housing Census - 2008, 2009). Gadarif State is located in the east of Sudan and neighboring Ethiopia. The capital of the state is Gadarif City. There are 11 localities (the lowest administrative units in Sudan) in Gadarif State. It has vast land suitable for agriculture and is home to Sudan's largest projects for rain-fed agriculture. It consists of ethnic groups representing different tribes, that is, a multiethnic society (UNICEF, 2022). Initially, four localities were chosen randomly from the 11 localities. From each of the four localities, an appropriate sample size was recruited according to their size. The population of Gadarif State includes all Sudanese tribes from all different regions of Sudan.
Inclusion/Exclusion Criteria
In the current study, a participant was defined as newly diagnosed with T2DM when she knew his/her status for the first time (i.e., during our study). Those with hypertension, aged less than 18 years, thyroid problems, T1DM, renal disease, and pregnant women were excluded from both the cases and the control group.
Ethical Considerations
The current work was conducted according to the Declaration of Helsinki. The study was approved by the by the Faculty of Medicine, Gadarif University, Sudan. The reference number is 2019# 07. All participants signed written informed consent forms. The authors followed all measures to ensure the privacy and confidentiality of all participants, that is, excluding personal identifiers during data collection.
Study Procedure
Sudanese adults whose ages were >18 years were randomly selected from households who signed informed consent were enrolled. Then, using questioners, two trained medical officers (male and female) interviewed the participants by face-to-face interview.
Sample Size Calculation
A sample size of 88 participants in each study group was calculated as equal cases and controls. In accordance with the previous study on the level of 25(OH)D among adults in Sudan (Taha et al., 2017), we assumed there would be a difference of 4 in the level of 25(OH)D between the participants who had T2DM and the healthy controls. This sample size (88 participants in each group) was calculated to detect a difference of 5% at α = 0.05 with a power of 80%.
Data Collection
An informed consent form was signed by each of the participants. Then, a questionnaire was used to collect sociodemographic data (age, gender, education) and determine whether DM had been diagnosed previously. Relevant clinical and physical measurements, especially the participants’ blood pressure. Weight and height were measured following the standard procedures and recorded (Supplementary file 1). The cases were adults with T2DM (known diabetics or newly discovered), according to the International Diabetes Federation guidelines (Magliano & Boyko, 2021).
For each participant, weight (in kg) and height (in cm) were measured as per the standard procedures, and their values were used to compute BMI using the equation weight (kg)/height (m2). Then, a total of 5 mL of venous blood was taken and divided into two tubes (plain and containing EDTA). While nonfasting blood glucose levels were measured within an hour of the blood extraction using a glucometer (Accu-Check Active; Roche Diagnostics, Germany), HbA1c levels were measured using an Ichroma machine guided by the manufacturer's instructions (Republic of Korea).
The enzyme-linked immunosorbent assay (Euroimmun, Lubeck, Germany) was used to measure serum 25(OH)D levels according to the manufacturer's instructions. Manufacturer quality control measures and six standard solutions (calibrators) levels set between 0 and 120 ng/mL were applied for each assay. The sample was considered vitamin D deficient if the serum 25(OH)D level was < 20 ng/mL (International Osteoporosis Foundation, 2023). The serum levels of 25(OH)D cut points are interpreted differently among agencies and countries (Bouillon, 2017). The variability of 25(OH)D assays is widely recognized (Rahme et al., 2018; Wise et al., 2017). This method (the enzyme-linked immunosorbent assay) and cut point (<20 ng/mL) were used in a similar context in Sudan (Hassan et al., 2023).
Statistical Analysis
Data were entered in the computer using the IBM Statistical Package for the Social Sciences (SPSS®) for Windows, version 22.0 (SPSS Inc., Armonk, New York, United States). Shapiro–Wilk test was used to evaluate the normality for all the included continuous data/variables, and none of them was found to be normally distributed; hence, their values were expressed as a median (interquartile range [IQR]) and were compared between the two groups by the nonparametric test (Mann–Whitney U test). The chi-square test was used to compare categorized variables. Spearman correlation was performed between 25(OH)D concentration and HbA1c levels. Univariate analysis was performed with T2DM as the dependent variable, while the independents (covariates) were the sociodemographic characteristics (age, gender, marital status, educational level), BMI, and 25(OH)D concentration. We planned to build up multivariable models using variables from univariate analysis with a p-value of <0.2 with backward elimination to adjust for covariates; however, only BMI was found to have a p < 0.20. Therefore, logistic regression was not performed.
Results
One hundred seventy-six participants (88 with T2DM and 88 healthy controls) were enrolled in this study. Out of the 88 diabetic participants, 53 were newly diagnosed with T2DM, and 35 were known to have DM.
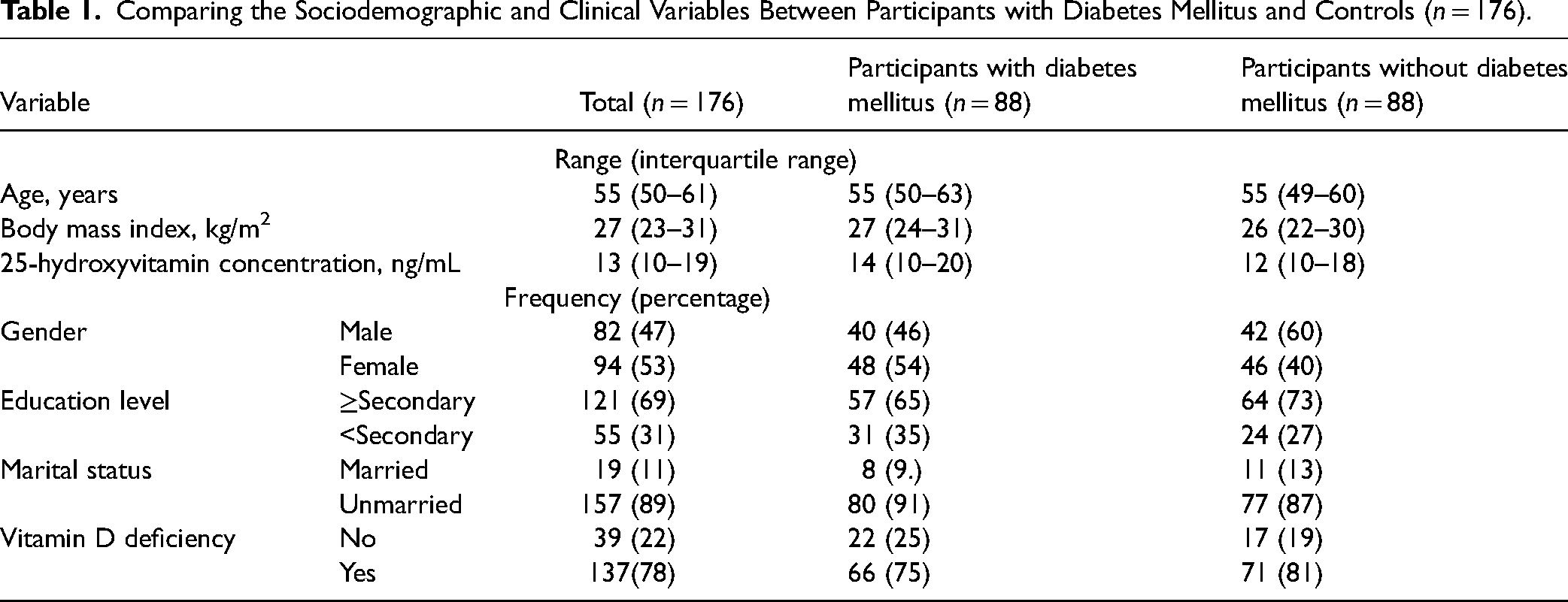
Of the total 176, 82 (47%) were males, and 94 (53%) were females; the median (IQR) of age, BMI, and 25(OH)D concentration were 55 (50–61) years, 27(23–31) kg/m2, and 13 (10–19) ng/mL, respectively. Of the 176, 137 (78%) were vitamin D deficiency cases.
The two groups (88 with T2DM and 88 healthy controls) were no different in their age and sex, educational level, and marital status. Moreover, BMI was not associated with T2DM. Likewise, the median (IQR) for serum 25(OH)D concentration was not different between the patients with T2DM and the healthy controls (13 [10–20] ng/mL vs. 12 [10–18] ng/mL, p = 0.16). There was no significant difference in the prevalence of vitamin D deficiency (25(OH)D level ≤ 20 ng/mL) in patients with T2DM and the healthy controls (66/88 [75.0%] vs. 71/88 [80.7%], p = 0.360) (Table 1). There was no correlation between 25(OH)D concentration and HbA1c levels (r = 0.102, p = 0.176).
Comparing the Sociodemographic and Clinical Variables Between Participants with Diabetes Mellitus and Controls (n = 176).
There was no association in the serum 25(OH)D levels between diabetic and nondiabetic participants (OR = 1.01, 95% CI 0.97–1.06, p = 0.50) or in vitamin D deficiency between diabetic and nondiabetic participants (OR = 0.72, 95% CI 0.35–1.47, p = 0.36) (Table 2).
Univariate Analysis of Variables Associated with Diabetes Mellitus among the Studied Participants (n = 176).

Discussion
The current study's main finding was that the serum 25(OH)D level was not associated with T2DM. Several previous studies reported similar results (Fondjo et al., 2017; Kibirige et al., 2022; Said et al., 2021; Sheth et al., 2015). For example, in Ghana, a case–control study (118 diabetics vs. 100 nondiabetics) revealed that vitamin D deficiency was prevalent in both diabetics (92.4%) and nondiabetics (60.2%); however, they reported no association between both insulin resistance and beta cell function and vitamin D deficiency (Fondjo et al., 2017). In Uganda, a study among 327 adult participants with recently diagnosed DM found no association between insulin resistance and low vitamin D status (Kibirige et al., 2022). In Kenya, no correlation was observed between vitamin D deficiency and insulin resistance (Said et al., 2021). A cross-sectional study that was conducted in Western India enrolled 429 diabetics and 483 nondiabetics and showed vitamin D deficiencies in 91.4% and 93.0%, respectively; there was no association between serum 25(OH)D level and DM (Sheth et al., 2015).
On the other hand, several previous studies reported a significant difference/association between vitamin D status and DM (Khudayar et al., 2022; Nasr et al., 2022; Park et al., 2018; Zhang et al., 2016). We have previously shown that a low 25(OH)D level was associated with an increased risk of gestational DM in Sudan (Mahmoud et al., 2019). In Saudi Arabia, a study that was conducted on 64 participants (T2DM = 32, nondiabetic = 32) showed a significant association between vitamin D deficiency and T2DM (p = 0.001) (Nasr et al., 2022). In Kuwait, vitamin D deficiency was reported to be associated with increased odds of prediabetes (Zhang et al., 2016). In Jordan, in a case–control study (125 in each group), reduced 25(OH)D was associated with the risk of T2DM (Alfaqih et al., 2022). In Pakistan, a cross-sectional study conducted among 525 T2DM and 525 healthy controls revealed vitamin D deficiencies of 54.1% and 25.9%, respectively; vitamin D deficiency was significantly associated with the occurrence of T2DM (p < 0.001) (Khudayar et al., 2022). Park et al. in their cohort study of 903 adults who were known to be free of diabetes or prediabetes during a 1997–1999 visit, concluded that there was an inverse dose–response gradient between 25(OH)D concentration and risk of diabetes (Park et al., 2018). Moreover, Dawson-Hughes et al. suggested daily vitamin D supplementation to maintain a serum 25(OH)D level ≥100 nmol/L as a promising approach to reducing the risk of DM in adults with prediabetes (Dawson-Hughes et al., 2020).
Interestingly, in the current study, vitamin D deficiency was more prevalent among nondiabetic participants (80.7%) compared to diabetic participants (75.0%); however, it was not statistically significant. It is worth mentioning that previous studies, in agreement with our study, found low levels of 25(OH)D in both diabetics and nondiabetics (Fondjo et al., 2017; Sheth et al., 2015). Such an observation could explain the lack of association, that is, the role of vitamin D in HbA1c and insulin resistance could not be established when vitamin D deficiency is highly prevalent in both diabetic and nondiabetic participants.
Notably, our results should be cautiously compared with findings to the contrary in other studies. First, the current study was a community-based study, while some later studies enrolled symptomatic participants, and the study was a facility-based study. Second, more participants were newly diagnosed with DM (53 newly diagnosed vs. 35 known diabetics). Long-term follow-up of our newly diagnosed diabetic participants might result in a higher prevalence of vitamin D deficiency (Karau et al., 2019). Third, differences in cutoff points for serum 25(OH)D deficiency must be taken into account. Recently, there has been ongoing discussion/debate among researchers on the optimum cutoff point to define vitamin D deficiency (Bouillon, 2017). It merits mentioning that a recent study conducted in Qatar highlighted the issue of justifying the use of the existing cutoff value and called for defining a new cutoff value for Qatar (Zainel et al., 2019). Our study can serve as a base for further study to set a suitable cutoff value for the Sudanese population.
It is not clear how vitamin D could influence DM or vice versa. However, researchers have suggested differing explanations for the association between vitamin D and DM. These explanations include the anti-inflammatory properties and extraskeletal activity of vitamin D (Bt Md Razipand & Bt Khaza’ai, 2018; Contreras-bol et al., 2021). For example, vitamin D works synergistically with several factors on calcium homeostasis, and these could interact with insulin (Bt Md Razipand & Bt Khaza’ai, 2018). Recently, aiming to explore such an association between vitamin D and DM, researchers have called for research in molecular, biochemical, and clinical trials to explore further the molecular pathways involved in this association (Contreras-bol et al., 2021).
The current study was conducted to assess the association between vitamin D and DM. We discussed the factors associated with DM in our previous work in eastern Sudan (Omer et al., 2018). Thus, a discussion of these factors might extend this manuscript.
Strength and Limitations
The present study assessed vitamin D status in a remote area in one of the poorest countries in the world. According to the authors’ knowledge, this is the first study to address vitamin D and DM in Sudan. However, the current study has some limitations that need to be mentioned and covered in future research. The present study assessed the association at one point in time. A longitudinal study will provide more clarity regarding the association between vitamin D and DM. This study covered one geographical area; thus, it may not represent the entire country (Sudan). Due to the nature of living in villages, we assumed a similar exposure to sunlight in villages; therefore, we did not collect such information. It is worth mentioning that, in Sudan, it has been documented that sunshine alone cannot guarantee vitamin D sufficiency in the tropics (Husain et al., 2017). In addition, information about the dietary patterns of the participants was not collected in this study. For example, Wang et al. suggested that dietary patterns that are associated with markers of hyperinsulinemia, inflammation, and DM development may inform future dietary guidelines for chronic disease prevention, including T2DM, cardiovascular disease, and cancer (Wang et al., 2023).
Implications for Practice
The results have implications for improving adults’ health since vitamin D deficiency is preventable and treatable. We recommend screening and correcting vitamin D status for all people, regardless of DM status. The high rate of newly diagnosed participants with DM in our study (53 newly diagnosed vs. 35 known diabetics) necessitates a regular community screening for DM. These results and the proposed recommendations will be communicated to the decision-makers and integrated into the existing policies.
Conclusion
There was no significant difference in 25(OH)D levels between diabetic and nondiabetic participants in this study. The current study showed a high prevalence of vitamin D deficiency among both diabetic and nondiabetic participants. Screening and correction of vitamin D status are recommended for all people, regardless of DM status. Further studies investigating the mechanisms of association between 25(OH)D levels and DM are needed.
Supplemental Material
sj-docx-1-son-10.1177_23779608241265203 - Supplemental material for Serum 25-Hydroxyvitamin D Concentrations in Patients with Type 2 Diabetes Mellitus in Eastern Sudan: A Case–Control Study
Supplemental material, sj-docx-1-son-10.1177_23779608241265203 for Serum 25-Hydroxyvitamin D Concentrations in Patients with Type 2 Diabetes Mellitus in Eastern Sudan: A Case–Control Study by Ahmed A. Hassan, Saeed M. Omar, Omer Abdelbagi and Ishag Adam in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to thank all the participants who participated in this study.
Authors’ Contributions
AAH and IA conceived the study; SMO and OA supervised the work, guided the analysis, and critically reviewed the manuscript; AAH, OA, and IA prepared the analysis plan, performed the data analysis, and wrote the first draft of the paper; SMO and OA supervised data collection. All authors reviewed and approved the final manuscript.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available (because the manuscript is still under peer review), but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The current work was conducted according to the Declaration of Helsinki. The study was approved by the Faculty of Medicine, Gadarif University, Sudan. The reference number is 2019# 07. All participants signed written informed consent forms. The authors followed all measures to ensure the privacy and confidentiality of all participants, that is, excluding personal identifiers during data collection.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.