
Abstract
Background
Evidence revealed that, 60% of deaths in the underdeveloped nations are linked to adoption of unhealthy lifestyles. The Trans-theoretical Model (TTM) has been considered a useful interventional approach in smoking cessation, drug addiction and weight control. However, its effectiveness in improving changes in dietary pattern, physical activity and alcohol consumption has not been reported.
Purpose
The study aimed at evaluating the effectiveness of the TTM-based health education intervention in the promotion of lifestyle changes among adults with metabolic syndrome.
Methods
This was an experimental design where 352 participants with metabolic syndrome were allocated to intervention and control groups. The participants were randomly assigned to receive either standard CVD care or a TTM stage-based lifestyle modification intervention for 12-months. Lifestyle patterns were assessed at baseline and endpoint. The mean difference of the subtotal TTM concept scores between pre and post intervention was evaluated using paired t-test. The chi-square test of independence was used to detect between group differences in the categorical data.
Results
Most of the participants were in the pre-action stage of change for their dietary intake patterns and physical activity habits at the baseline assessment with no difference between the groups. The intervention group's total level of change toward adopting a healthy lifestyle was markedly (p < 0.001) improved than the control group at the endpoint. The mean scores for the intervention group's stage of change, self-efficacy, and pros and cons of decisional balance all improved significantly (p < 0.001) from the baseline. The mean scores for the control group's pros and cons of decisional balance and stage of change also considerably (p < 0.05) improved from baseline to the endpoint.
Conclusion
The TTM- based health education intervention was effective in improving the participants’ lifestyles that includes diet and physical activity. Health care providers, particularly nurses should implement TTM staged-matched educational intervention for individuals who are at risk for cardiovascular diseases.
Introduction
Metabolic syndrome (MetS) is a group of health maladies namely: central obesity, elevated fasting blood sugar (FBG), increased level of blood pressure (BP), elevated serum triglycerides (TGs), and low levels of high density lipoprotein cholesterol (HDL-C) (Alberti et al., 2009). It is a main precursor for type-2 diabetes and cardiovascular disease (CVD) (Cantiello et al., 2015; Mendonça et al., 2015). Evidence show that, those with MetS are around five times more likely than people without the syndrome to develop type-2 diabetes, two times as likely to pass away from it, and three times as likely to have a heart attack or stroke (Van Namen et al., 2019). The four main behavior-based risk factors for CVD include excessive alcohol intake, poor diet, tobacco use, and physical inactivity (Bull et al., 2020).
If individuals with MetS are timely identified and properly informed to change their lifestyles, the risk of developing CVD can be greatly reduced (IDF, 2015; Peikani et al., 2018). Given that one of the World Health Organization key strategies for the prevention of CVD is to adopt a healthy lifestyle (Al-Qahtani, 2015), design and implementation of lifestyle interventions is critically important. One of the most relevant approaches of interventions for promotion of healthy lifestyles is the use of the Trans-theoretical Model (TTM) (Sousa et al., 2015). According to the model, people are at different stage of readiness to change their current behaviors towards diseases prevention, and interventions to promote positive behavior are more effective when matched with the individual's readiness (Prochaska & DiClemente, 2003). Hence, the TTM stage-based intervention considers the readiness of each individual to adopt a new behavior. Stages of change, self-efficacy, and pros & cons decisional balance are the three main components of the model.
The two primary behavioral determinants are self-efficacy and decisional balance.
Literature Review
CVD is a severe public health burden in the less developed nations, where awareness level and diagnostic rates are still poor (Bigna & Noubiap, 2019). The risk of type-2 diabetes and CVD is significantly increased by MetS. As a result, diabetes, coronary heart disease, hypertension, and stroke are all becoming more commonplace globally (Van Namen et al., 2019). In the less developed nations, CVDs are expensive to identify and treat, leading to premature death among the most productive individuals in the society. CVD is becoming more common in the Sub-Saharan African (SSA) nations (Hamid et al., 2019) and the prevalence is anticipated to double by 2030 due to population growth and lifestyle choices (Ndejjo et al., 2020). In Kenya, the major CVD risk factors such as alcohol misuse, unhealthy diets and overweight are high and rising (Kimani et al., 2019; Okube et al., 2020). In Kenya, CVD account for 26% of all NCD-related fatalities (Wekesah et al., 2020).
New approaches for maintaining a healthy lifestyle are required to address the rising CVD risk factors and help communities to attain improved cardiovascular health outcomes in the less developed nations. A recent meta-analysis discovered that lifestyle change interventions significantly improved the majority of MetS indicators (Van Namen et al., 2019). However, adherence to the recommended lifestyle changes is a major challenge for the prevention and treatment of lifestyle-related diseases. The TTM, which has been used to several health disorders such as smoking, drug addiction, and obesity, was proposed to encourage behavioral changes (Stanton & Grimshaw, 2013). Despite the evidence, little is known about the effectiveness of TTM-stage-based health education intervention in promotion of lifestyle changes among adults with MetS. This study looked at how well a TTM-based health education intervention affected adults with metabolic syndrome's ability to change their lifestyles.
Difference Between the Trans-Theoretical Model and Motivational Interviewing
In the literature, there is a correlation between interventions based on the Motivational Interviewing (MI) and the Trans-theoretical Model (TTM) of Behavior Change (Miller & Rollnick, 2013). Understanding what triggers behavior change and how it could happen is possible using the TMM of Behavior Change (Prochaska & DiClemente, 1984). Conversely, MI is a unique counseling strategy that maximizes the person's motivation for change (Hoy et al., 2016; Martinasek et al., 2021). The goal of MI as an intervention is to facilitate the TTM of change's stages of progression. According to Miller and Rollnick (2009), MI is a cooperative, person-centered method of leading that elicits and strengthens motivation for change.
Four basic processes—engaging, focusing, evoking, and planning—are involved in MI, according to Miller and Rollnick (2009). Engaging refers to a method that understands the client's challenge toward behavioral adjustments by using a person-centered counseling strategy demonstrated by active listening. By establishing an agenda and finding out what matters to the client, focusing involves assisting the client in reaching a desired behavior. Focusing involves assisting the client in reaching a desired behavior by establishing a specific agenda and finding out what matters to the client. Evoking is the transition to MI where the therapist or counselor engages in selective eliciting, responding and summaries. Building a bridge to client change is the process of planning. Together, the client and the therapist develop a strategy for change and strengthen the client's resolve to make the necessary changes. In particular, clients who are pre-contemplative or contemplative stage of the TMM about their conduct benefit the most from MI. However, MI style is less appropriate for clients in the action stage, who have already surmounted the main obstacles to change. To sum up, the TTM provides an understanding of the broader process involved in altering a challenging habit, while MI is a particular intervention that falls into a particular phase of the TTM process.
Success of Motivational Interviewing on MetS Components
Following exercise intervention employing motivational interviewing, a recently completed randomized controlled trial study found that majority of the components of MetS were less prevalent among the intervention group compared to the control group (Suire et al., 2022). Another study also discovered that the telephone-based motivational interviewing group significantly improved their weekly physical activity and metabolic syndrome status when compared to a usual care control group (Lin et al., 2016).
Methods
Study Setting
The participants were recruited from the outpatient department of St. Mary's Mission Hospital in Nairobi, and they were followed in the community for 12-month period. The hospital is situated in the adjacent Kibera shantytown. It is a facility founded on the Christian faith that is committed to giving low-income slum dwellers access to quality healthcare service at a reasonable cost. The Kibera slum is the largest and poorest in all of Africa, with an average household monthly income of USD 39 (Desgroppes & Taupin, 2011). Indeed, the population of Kibera is disproportionately affected by poor socioeconomic determinants of health, including limited access to healthcare services, unemployment and job insecurity, housing, and clean water. People with low socioeconomic status have a higher risk of developing CVDs due to exposure to unhealthy behaviours, stress related to their psychosocial environment, and lack of access to high-quality healthcare resources (Van de Vijver et al., 2015). According to a study conducted in the Kibera slum, Nairobi, there are high rates of the main risk factors for CVDs, such as smoking, poor dietary patterns, and excessive alcohol consumption (Hulzebosch et al., 2015).
Design, Sampling Procedures, and Study Respondents
The study was a two-arm randomized controlled trial design comparing a TTM stage-based health education intervention with standard CVD care to promote lifestyle changes among adults with MetS for a period of 12 months. Individuals who visited the outpatient clinic of the study hospital were screened and evaluated for MetS using the revised International Diabetes Federation criteria, which considers gender and race-specific waistline measurement cutoffs (Alberti et al., 2009). Accordingly, central obesity (a waist measurement greater or equal to 80 cm for women and greater or equal to 94 cm for men) plus at least two of the major four CVD risk factors are considered for the presence of MetS in Sub-Saharan African nations. These are; (
Age 18–64 and presence of MetS were the inclusion criteria at the baseline. Women who were pregnant or nursing, and those who had major illnesses like cancer, cardiovascular events, mental illnesses, or physical disabilities, were excluded from the study. Using a block stratified randomization technique, participants who met the inclusion criteria were recruited and randomly assigned to receive either standard CVD care (n = 176) or a TTM stage-based lifestyle modification intervention (n = 176). The procedure entailed grouping the participants into blocks of, on average, 16 subjects each. A written piece of paper was used to randomly place people from each block into the intervention or control group. Two research assistants handled participant recruitment, while the primary investigator determined the randomization of the groups. During the randomization, the research assistants and the subjects were blinded. Measurements were made in laboratories, clinical settings, and physically by experts who had no knowledge of the groups. Those who live together and are members of the same family were allocated to the same group in order to reduce treatment contamination between intervention and control participants.
Intervention
Standard Care
The participants in the control arm received their screening results and standard CVD care at the baseline and second visit (month 6). Clinical/laboratory investigations, medication-assisted therapy, and post-discharge general health education are all included in standard CVD care, which is delivered by medical staff in accordance with hospital policy. For instance, if someone is identified as having hypertension, the person gets prescription for anti-hypertension medication and general guidance. No TTM stage-based suggested food intake patterns (vegetables, fruits, salt, sugar, etc.), use of alcohol, and physical activity was provided at baseline and halfway, which was reserved for participants in the intervention arm. However, after the evaluation phase (endpoint), the participants in the control group received a thorough TTM stage-based targeted lifestyle change intervention, together with a health education package and brochures. Unaware participants but found with diabetes (FBG greater or equal to 7.0 mmol/L) and/or high BP (greater or equal to 140/90 mmHg) were advised to visit the hospital's clinic for additional testing and follow-up.
TTM Stage-Based Lifestyle Modification Intervention
The TTM was utilized to offer stage-based individualized intervention for dietary, alcohol intake, physical activity, and smoking cessation modifications. The intervention group received TTM stage-tailored intervention in addition to standard CVD care at baseline, six and twelve months to increase intake of physical activity, intake of vegetables, fruits, legumes, nuts, cereals, and control intake of alcohol, saturated and processed foods, sugar and salt. Hence, the total period for the intervention was 12 months. The intervention was administered by determining the individuals’ present stage of change with reference to their readiness to modify their lifestyle and the extent of their lifestyle modifications. The ideas of the stages of change, self-efficacy, and the pros and cons of decisional balance were rearranged based on the assessment results in order to provide stage-matched interventions. Three face-to-face contact sessions and at least two online coaching sessions through email, Whatsapp, or direct phone call took place during the 12-month intervention period.
Measurements
Two nurse research assistants who had been trained in research protocols collected the primary data. A healthy lifestyle practice (dietary and alcohol intake patterns, cigarette smoking, and physical activity) was examined at baseline and endpoint using three major TTM components (self-efficacy, the benefits (pros) and drawbacks (cons) of decisional balancing and stages of change).
Assessment of Stages of Change Towards Lifestyle Modification
Questionnaire on the stages of change for fruits and vegetables intake designed by Ma et al. (2002) and level of physical activity by Marcus et al. (1992) were used to evaluate the respondents’ stages of change. Nine behavioural patterns including intake of vegetables, fruits, processed foods, sugar, salt, follow the Dietary Approaches to Stop Hypertension (DASH) diet, use of alcohol, smoking, and level of physical activity, were used to measure respondents’ stages of change toward lifestyle characteristics. Participants indicated their present intentions to change for each of the nine behavioral patterns by selecting one of five statements. Pre-contemplation received a score of 1, contemplation a score of 2, preparation a score of 3, action a score of 4, and maintenance a score of 5. After the data had been gathered, the first three components of the model (preparation, contemplation and pre-contemplation) were combined together as a pre-action stage.
Then, pre-action respondents were given “
Determination of Self-Efficacy in Relation to Lifestyle Modification
Nine factors were used to measure self-efficacy in relation to patterns of dietary intake (salt, sugar, follow the DASH diet, vegetables, fruits and processed food), alcohol use, cigarette smoking, and degree of physical activity. A 3-point Likert scale that has undergone validity and reliability testing was used to rate the respondents for each variable (Louangrath & Sutanapong, 2018). The respondents were asked to rate their confidence in following the suggested healthy lifestyle on a scale of 1 to 3, with 3 denoting “extremely confident,” 2 denoting “somewhat confident,” and 1 denoting” not at all confident”. Consequently, 27 was the highest possible self-efficacy score.
Determination of Pros and Cons of Decisional Balance in Relation to Lifestyle Modification
A valid questionnaire established by Nigg et al. (1998) was used to evaluate decisional balance with reference to lifestyle adjustment. This was evaluated by asking the respondents what weight they assigned to each of the benefits and drawbacks in making the decision to lead a healthy lifestyle. This was measured using 11 cons to evaluate obstacles to adopting a healthy lifestyle and 15 pros to evaluate perceived benefits. A 3-point Likert scale was used to rate each item. Scores for pros ranged from 1 for disagree, 2 for somewhat agree and 3 for agree. The cons scores were 3 for agree, 2 for somewhat agree, and 1 for disagree. The pros and cons were given a maximum score of 45 and 33, respectively.
The Questionnaire's Validity and Reliability
The questionnaires were adopted from literature on the stage of change for fruits and vegetables intake designed by Ma et al. (2002) and level of physical activity by Marcus et al. (1992) which were tested for their Validity and reliability. Additionally, experts in the fields of nutrition and cardiovascular disease examined the tools’ content validity to ensure their completeness and relevance. The final questionnaire included the suggestions and recommendations. A test-retest method was utilized to assess the questionnaire's reliability. After three weeks, a duplicate pre-test was administered to determine the degree of agreement between the two results. The duplicate pre-test produced a kappa score of 0.91, indicates its reliability.
Ethical Consideration
An Ethical Review Committee (ERC) board constituted by the University of Nairobi and Kenyatta National Hospital approved the study (Reference number: P430.07/2017). Prior to being enrolled in to study, all the participants gave their written informed permission. In order to safeguard the participants’ privacy, all of the data obtained remained anonymous and was handled with absolute confidentiality.
Statistical Analyses
The SPSS software (Ver.22) was utilized to analyse the data. Significant difference for categorical variables between the two groups was established using the Pearson chi-square test of independence. The participants’ mean differences in subtotal TTM concept scores between before and after intervention was tested using a paired t-test. At p-value <0.05, the results were deemed statistically significant.
Participants’ Recruitment and Follow-up
Four hundred and four persons who had central obesity were examined for the presence of MetS; 352 were determined to be affected. Participants with MetS were randomly assigned to either standard CVD care group or a TTM stage-based health education intervention group over a 12-month period. Of the 352 participants, 294 (control =138; intervention = 156) completed the study period. Fifty eight individuals (control = 38; intervention = 20) left the study mostly due to poor compliance and lost follow-up. A few left the program due to residence relocation, travel to other counties, and pregnancies of two women. There was no noticeable difference in terms of sociodemographic and lifestyle patterns between those who left the study and those who completed it (Figure 1).

Consort Flow Diagram of the Study Participation (F = Female; M = Male).
Participants’ Stages of Changes in Relation to Adoption of a Healthy Lifestyle Before the Intervention
The demographic profiles of the two groups were well elaborated in our recently published work (Okube et al., 2023). At baseline, most of the participants were at pre-action stage of change for intake of the required amounts of salt, sugar, fruits and vegetables, use of the DASH diet, and alcohol with no significant difference between the groups. At baseline, there was no discernible (p = 0.456) variance between the two groups regarding overall commitment to adopt a healthy lifestyle (Table 1).
Stages of Changes in Relation to Adoption of a Healthy Lifestyle Before the Intervention (n, %).
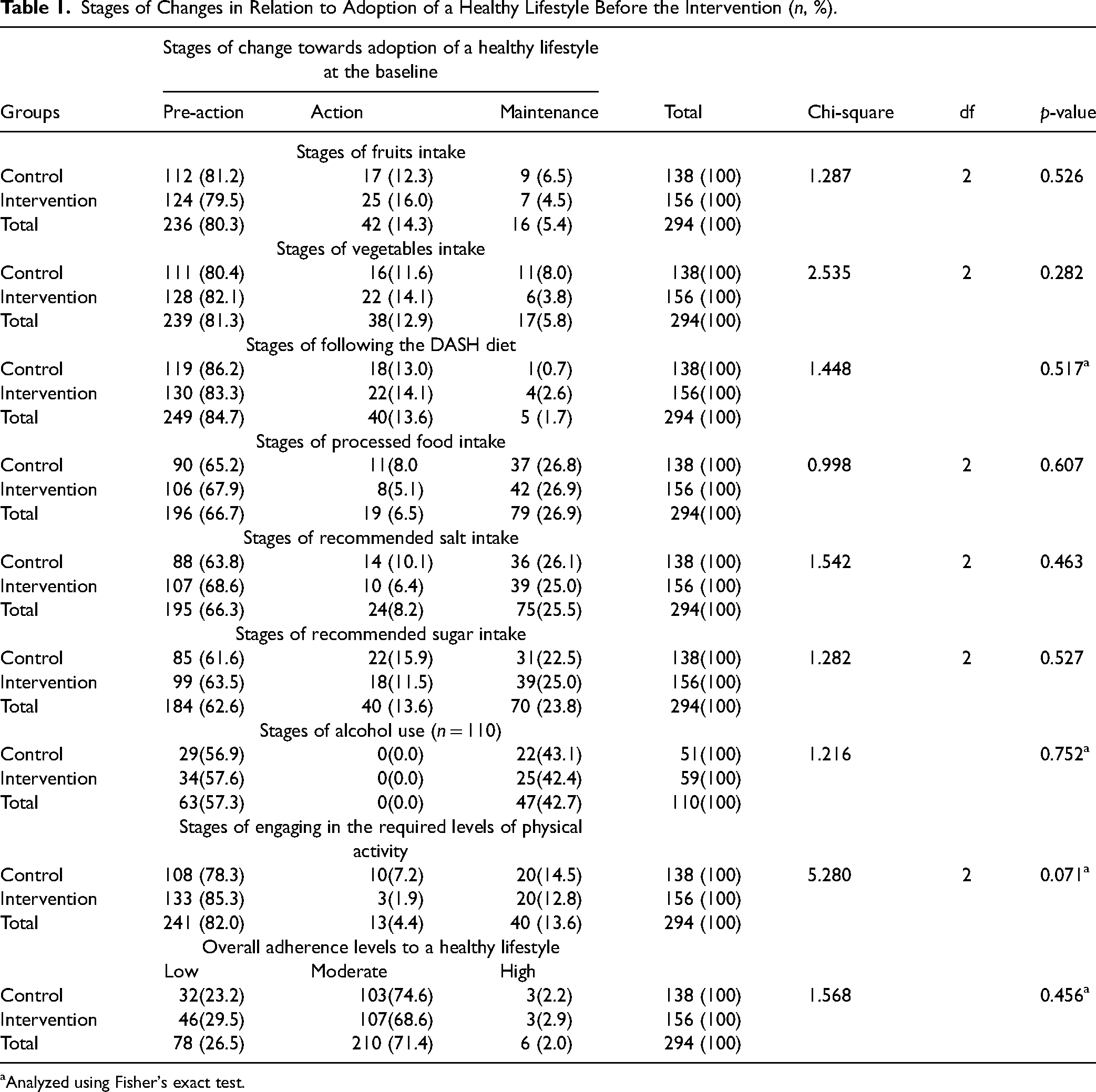
Stages of Changes in Relation to Adoption of a Healthy Lifestyle Before the Intervention (n, %).
Analyzed using Fisher's exact test.
In general, both groups’ lifestyle patterns improved at the endpoint in comparison to the baseline. At the study's endpoint, however, significantly (p < 0.001) more members of the intervention group than the control group had reached the maintenance stage of change with regard to eating fruits and vegetables, adhering to the DASH diet, reducing processed food intake, limiting salt and sugar, and engaging in the recommended amount of physical activity. Overall, the intervention group (68.6%) had a significantly (p < 0.001) higher level of change leading to adoption of a healthy lifestyle than the control group (25.4%) at the endpoint (Table 2).
Participants’ Stages of Change Leading to Adopting a Healthy Lifestyle at the Endpoint (n, %).
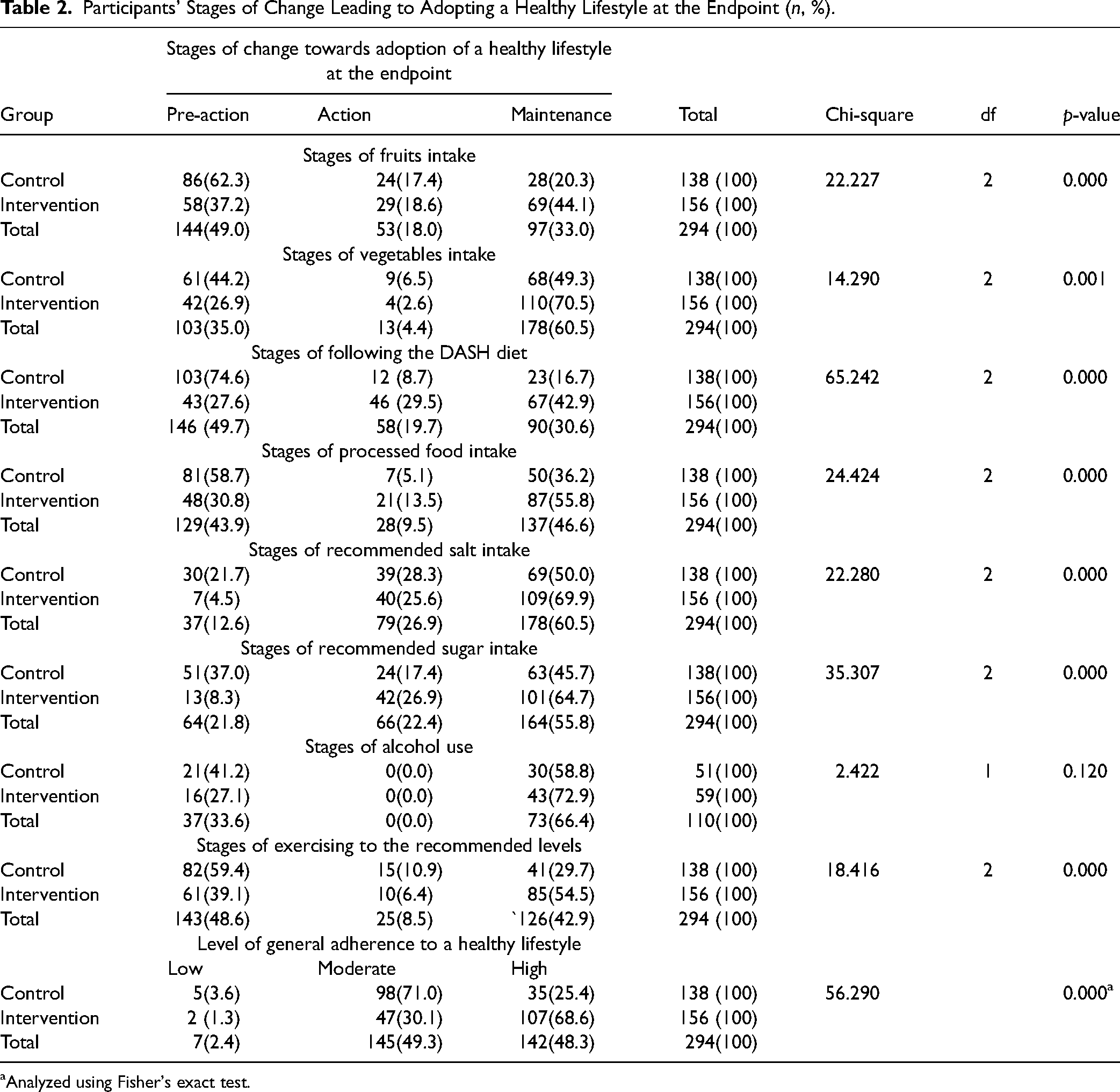
Participants’ Stages of Change Leading to Adopting a Healthy Lifestyle at the Endpoint (n, %).
Analyzed using Fisher's exact test.
Approximately, one-third of the participants (36.5% from the intervention and 31.9% from the control groups) felt that fruits and vegetables provide a good alternative to junk food. The majority of participants concurred that eating at least five servings of vegetables & fruits each day could aid in preventing diabetes and high blood pressure. Nearly half (44.9%) of the intervention group and a third (37.7%) of the control group thought that consuming vegetables and fruits regularly could help them lose extra weight. The majority of respondents, however, concurred that they were unable to find fairly priced vegetables and fruits in their neighborhood markets. The majority of the participants in both groups agreed that consuming the suggested amounts of sugar and salt, cutting back on processed foods and fast food, exercising for at least 30 min, five to seven days a week, and avoiding or limiting alcohol use could all help people prevent hypertension and diabetes. There was no discernible difference between the two groups in their perceptions of the pros of acquiring a new behavior at baseline (Table 3).
Participants’ Perceptions of the Pros of Acquiring a New Behavior Before the Intervention (n, %).

Participants’ Perceptions of the Pros of Acquiring a New Behavior Before the Intervention (n, %).
The number of people in the intervention arm who felt that regular consumption of fruits and vegetables could help them achieve a healthy weight (p < 0.001), that they are a good replacement for junk food (p < 0.001), and that eating at least five servings of vegetables and fruits per day could help them avoid high BP and diabetes (p = 0.001) was significantly higher than that of participants in the control group at the endpoint. However, only a fifth (20.3%) of the control group and a third (31.4%) of the intervention group agreed that their local markets offer reasonably priced fruits and vegetables. At the end of the intervention, considerably (p < 0.05) more participants from the intervention arm than the control arm concurred that limiting their intake of salt to less than one tea spoon per day, sugar to less than five tea spoons per day, reducing or totally avoiding processed foods, and alcohol could help them avoid developing hypertension and diabetes. Additionally, considerably (p = 0.001) more participants from the intervention group than to those in the control side agreed that exercising for at least 30 min, five to seven days a week, could help them avoid developing hypertension and diabetes (Table 4).
Participants’ Perceptions of the Pros of Acquiring a New Behavior After the Intervention (n, %).

Participants’ Perceptions of the Pros of Acquiring a New Behavior After the Intervention (n, %).
Most of the participants stated that eating at least five servings of vegetables and fruits in a day is too challenging due to their high price. Each group had around a third of the participants who said they were concerned about the safety of the chemicals used in vegetables and fruits. About a third of the participants (35.5% from control and 37.2% from intervention groups) expressed that it is challenging to limit one's daily sugar and salt intake. Approximately half of the participants (51.3% from the intervention and 44.9% from the control groups) felt that food with less salt or sugar or none at all has no flavor. Most of the participants (control = 58.7%; intervention = 50.0%) agreed that because processed foods are so widely available, it is challenging to limit or avoid consuming them. Of those alcohol drinkers, most concurred that it is challenging for them to restrict or avoid it at all. A small fraction (10.5%) of the control group and one-third (33.3%) of the intervention group concurred that quitting smoking is difficult for them. Of the participants, roughly one-third (control = 40.6%; intervention = 31.4%) felt they didn't have enough time to exercise five to seven days a week. Generally, there was no discernible difference in the two groups’ perceptions of the drawbacks to changing to a healthier lifestyle at the baseline (Table 5).
Participants Perceptions of the Cons of Acquiring a New Behavior Before the Intervention (n, %).

Participants Perceptions of the Cons of Acquiring a New Behavior Before the Intervention (n, %).
Analyzed using Fisher's exact test.
At the endpoint, most of the participants in both the groups felt that eating at least five servings of fruits and vegetables each day is too expensive and challenging. Approximately a third of the intervention (34.6%) and control (38.4%) groups concurred that they are concerned about the risk of chemicals used in vegetables and fruits. A significantly (p = 0.038) higher percentage of participants in the control (44.9%) than in the intervention (31.4%) group agreed that they have limitation for including vegetables and fruits in their meals.
Most participants in the control group (52.9%) and almost a third in the intervention group (35.9%) expressed that processed/fast meals are widely available and thus difficult to limit or avoid them, with the control group's percentage being considerably (p = 0.001) higher than that of the intervention group. Most of those who take alcohol concurred that limiting or avoiding alcohol use is not difficult. A quarter (28.6%) of the intervention group and a negligible percentage (10.5%) of the control group of the active smokers agreed that it is difficult for them to quit. A small percentage (9.6%) of the intervention group and about a fifth (19.6%) of the control group agreed that they lack enough time for physical activity for five to seven days per week, with the control group's percentage being considerably (p = 0.018) higher than the intervention group's (Table 6).
Participants Perceptions of the Cons of Acquiring a New Behavior After the Intervention (n, %).

Participants Perceptions of the Cons of Acquiring a New Behavior After the Intervention (n, %).
Analyzed using Fisher's exact test.
The baseline and endpoint differences in the TTM core components are shown in Table 7. Stage of change, levels of self-efficacy, and decisional balance (pros, cons) are the three TTM domains that all significantly improved after the intervention compared to baseline in both groups. Specifically, participants in the intervention side substantially increased mean scores in the decisional balance of pros (p < 0.001), level of self-efficacy (p < 0.001), stage of change (p < 0.001), and decreased decisional balance of cons (p < 0.001) at the endpoint relative to the baseline values. Similarly, participants in the control side considerably improved mean scores in the decisional balance of pros (p < 0.001), and stage of change (p < 0.001) and decreased in the decisional balance of cons (p = 0.008) at the endpoint relative to the baseline measurements. The level of self-efficacy construct in the control arm did not demonstrate considerable change at the endpoint when compared to baseline values.
Mean Variations of Subtotal TTM Construct Scores Between Baseline and Endpoint (Mean ± SD).

Mean Variations of Subtotal TTM Construct Scores Between Baseline and Endpoint (Mean ± SD).
This study's primary objective was to assess the effectiveness of a TTM-based health education intervention in promoting behavioral changes in people with MetS. The study showed that, most of the participants in both the groups were in pre-action stage of change for dietary intake patterns, alcohol use (for alcohol consumers), and physical activity at the baseline. With regards to level of self-efficacy, most of the participants were either somewhat confident or not at all confident in their ability to follow a healthy lifestyle, with no discernible difference between the two groups. The baseline findings are consistent with a study performed by Holmen et al. (2016) that looked at “stages of change for physical activity and dietary habits among patients with type 2 diabetes” and revealed that the majority of the participants were in the pre-action stage of change for dietary practice at baseline. Similarly, the majority of the participants, according to Mohammadi (2013), who used the TTM to examine the exercise status of Iranian officers, were in the pre-action stage of change for physical activity.
Overall, the three TTM domains namely: stages of change, levels of self-efficacy, and pros & cons decisional balance toward adopting a healthy lifestyle were significantly improved at the endpoint compared to baseline values in both groups. At the endpoint, however, considerably a higher percentage of participants from the intervention arm had advanced to the maintenance stage of change for physical activity and most of the dietary intake patterns compared to those in control group. Individuals in the intervention group showed a considerably higher overall level of behavioral change than those in the control group at the endpoint. Moreover, the intervention group had a higher percentage of participants than the control group who were extremely confident in adopting a healthy lifestyle at the endpoint. Additionally, participants the intervention group significantly improved the overall mean scores in decisional balance pros, level of self-efficacy, and stages of change and decreased cons decisional-balance at the endpoint compared to the baseline values. Participants in the control group also showed a substantial improvement in mean scores of stage of change and decisional balancing pros and a decrease in cons decisional balance at the endpoint when compared to the baseline values. In the control group, the self-efficacy construct, however, showed no significant change. According to the findings, the TTM stage-based intervention was successful in raising participants’ levels of self-efficacy, decisional balance, and readiness to adopt a healthy lifestyle. The plausible explanation for these notable changes in lifestyle modification is the comprehensive health education intervention based on the TTM framework, which supported cultivating greater efficacy of perceived benefits (pros) and decreasing the unfavorable perceptions (cons). The results lend credence to the idea that TTM can be used to prevent CVD.
The endpoint findings are consistent with a systematic review report of TTM's efficiency in managing behavioral change (Hashemzadeh et al., 2019). The findings also support a study performed by Nitzke et al. (2007) that evaluated “the efficacy of behavioral intervention to enhance fruits and vegetable intake among low-income adults. According to the report, more participants from the intervention arm consumed the recommended servings of fruit and vegetables and advanced to maintenance stage of change than those in the control arm after the intervention (Nitzke et al., 2007). Another report by Huang et al. (2013) showed that the majority of the study participants were in the maintenance stage of change for dietary intake patterns after taking part in a TTM-based educational intervention. Similarly, a study performed in Turkey by Koyun and Eroglu (2014), revealed that progression to maintenance stage of change was considerably higher among members in the intervention arm relative to those in the control side after receiving TTM-Tailored health education intervention. According to a study by Ibrahim et al. (2017) about diet modification of antenatal mothers using the TTM framework, the participants in intervention group significantly outperformed the control group in terms of decisional-balance, level of self-efficacy, and stages of change at the endpoint compared to the baseline status.
According to our findings, perceived benefits (the pros) of acquiring a new behavior have greatly improved in the maintenance stage of change compared to the pre-action phase, while perceived drawbacks (the cons) have significantly decreased at the maintenance stage of change compared to the pre-action phase, which are in accordance to the findings of other researchers (Hashemzadeh et al., 2019; Kang et al., 2012). According to Mohsen et al.'s study (2014), which used a TTM-based intervention to promote lifestyle change, the intervention group's mean scores for the pros of decisional-balance and level self-efficacy regarding dietary management behavior were significantly higher than those of the control group, which is consistent with our findings. The two primary behavioral determinants are self-efficacy and decisional balance. Perceived benefits and drawbacks have been shown to be able to predict the stage of change, according to a study by Abbaspour et al. (2017). The model states that change happens when advantages (pros) outweigh disadvantages (cons) (Yasin et al., 2011). As a person progresses through the stages, the benefits of the new behavior are anticipated to grow, while the drawbacks are anticipated to diminish. As a result, behavioral change happens when supporters of the new conduct outweigh opponents.
The study also identified some perceived berries to adopt a healthy lifestyle among the studied population. The majority of respondents in both groups concurred that because they are so expensive to purchase, it is too challenging to consume the recommended servings of vegetables and fruits every day. They consequently have limited options for including fruits and vegetables in their regular diets. It is also interesting to note that, in each group, nearly one-third of the participants said they were concerned about the safety of the chemicals used in vegetables and fruits. According to Hromi-Fiedler et al.'s study (2016), which supports our findings, appropriate intake of fruits and vegetables is significantly hampered by the safety of the chemicals employed in producing them. Additionally, economic factors like income and cost, availability, and preferences are among the factors that have been identified as influencing the consumption of fruits and vegetables (Di Noia & Byrd-Bredbenner, 2014; Miller et al., 2016). According to a report by the Kenya Ministry of Health (2018), some of the obstacles to eating healthy diets in Kenya include poverty, social and cultural factors, urbanization, and globalization.
Strengths and Limitations
The study's randomized controlled design and the control of the effects of potential variables on the modification of lifestyle characteristics. The large sample size and long duration (12-month) of follow-up period enabled us to evaluate changes in lifestyle characteristics towards the common modifiable risk factors of CVDs. Participants who live together were allocated to the same group in order to reduce treatment contamination between intervention and control participants. There are a number of limitations to the current study that should also be mentioned, such as the absence of objective assessments of food intake or physical activity. Because participants might have inflated exercise levels and understated nutritional intake after the intervention, the likelihood of a reporting bias cannot be completely ruled out.
Implications for Nursing Practice
A nurse-led, TTM-tailored health education intervention for behavior modification was crucial in influencing respondents’ actions in the direction of a healthy lifestyle for MetS control. Nurses play a key role to facilitate cardio-metabolic risk factor reduction in higher-risk individuals and communities. Targeting adults with elevated levels of multiple CVD risk factors is necessary for preventing the onset of cardio-metabolic diseases. To reduce the burden of CVD in the community, the team advises nurses and community health workers to employ TTM stage-based health education interventions for individuals who are at risk for CVDs such as those diagnosed with MetS.
Conclusion
In conclusion, our findings show that following the TTM-based health education intervention, the majority of the intervention group moved on to the maintenance stage of lifestyle modification. Participants’ decisional balance, level of self-efficacy, and stages of change toward lifestyle modification were all considerably better than baseline. There was a notably greater overall levels of change toward adopting a healthy lifestyle in the intervention group when compared to the control group. The findings show how crucial the TTM-tailored educational intervention is for encouraging adjustments and tracking respondents’ progress toward adopting a healthy lifestyle. TTM-tailored lifestyle intervention is a realistic and successful approach to change the major modifiable risk factors of CVD. This calls for nurses and community health workers to implement TTM stage-based health education intervention to reduce the burden of CVD in the community. The approach could include a health education plan centered on a health facility or a community-based awareness creation strategy like outreach initiatives, church or school-based programs. In order to promote healthy lifestyles, national health promotion programs should take into account subsidizing healthy foods like fruits and vegetables and raising prices for harmful meals like processed/fast/junk foods.
Supplemental Material
sj-docx-1-son-10.1177_23779608241251658 - Supplemental material for Effectiveness of Trans-Theoretical Model-Based Health Education Intervention in the Promotion of Lifestyle Changes among Adults with Metabolic Syndrome: A Randomized Controlled Trial
Supplemental material, sj-docx-1-son-10.1177_23779608241251658 for Effectiveness of Trans-Theoretical Model-Based Health Education Intervention in the Promotion of Lifestyle Changes among Adults with Metabolic Syndrome: A Randomized Controlled Trial by Okubatsion Tekeste Okube and Samuel T. Kimani in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241251658 - Supplemental material for Effectiveness of Trans-Theoretical Model-Based Health Education Intervention in the Promotion of Lifestyle Changes among Adults with Metabolic Syndrome: A Randomized Controlled Trial
Supplemental material, sj-docx-2-son-10.1177_23779608241251658 for Effectiveness of Trans-Theoretical Model-Based Health Education Intervention in the Promotion of Lifestyle Changes among Adults with Metabolic Syndrome: A Randomized Controlled Trial by Okubatsion Tekeste Okube and Samuel T. Kimani in SAGE Open Nursing
Footnotes
Acknowledgments
The personnel at St. Mary's Mission Hospital (SMMH) is thanked by the authors for their support during the data collection period. We also thank SMMH's administration for allowing us to conduct this research there.
Authors’ Contributions
The study's conception was shared by OT and SK. OT and SK involved in the design of the study including the study protocol. OT drafted the manuscript, which SK carefully edited. The final manuscript was reviewed and approved by both authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
An Ethical Review Committee (ERC) board constituted by the University of Nairobi and Kenyatta National Hospital approved the study (Reference number: P430.07/2017). Prior to being enrolled into study, each participant gave their written informed permission. In order to safeguard the participants’ privacy, all of the data obtained remained anonymous and was handled with absolute confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.