
Abstract
Background
Sociodemographic factors have been implicated in cardiovascular health with differential morbidity and mortality. It is essential to comprehend how sociodemographic factors contribute to the improvement of Metabolic Syndrome (MetS), the primary cardiovascular diseases indicator.
Objective
Determine the role of sociodemographic factors in improving MetS among adults residing in the Slums of Nairobi, Kenya.
Methods
Adults with MetS participated in this randomized controlled trial study for a period of 12-months. A random assignment was used to place eligible participants in the intervention or control groups. The intervention group received lifestyle intervention that entails not using tobacco products or alcohol, exercising, and adhering to recommended dietary guidelines, while the control group had standard medical care. Clinical, biochemistry, and lifestyle habits were measured before and a year after the intervention. The association between the sociodemographic factors and the improvement in MetS was examined using a multiple logistic regression model with backward conditional.
Results
In the intervention group, lack of improvement in metabolic syndrome was significantly higher among aged (≥50 years) respondents [AOR = 9.097; P < .001]; Protestants [AOR = 7.292; P = .017] and Catholics [AOR = 5.270; P = .050]. Compared to unemployed, formally employed respondents had an 84.6% lower chance of having MetS [AOR = 0.154; P = .005]. Within the control group, lack of improvement in metabolic syndrome was significantly higher among aged (≥50 years) respondents [AOR = 5.013; P = .047]. Compared to respondents who had less than $100, individuals with monthly incomes between $100 and $500 had a roughly 10-fold [AOR = 10.499; P = .024] higher chance of having MetS.
Conclusion
In the current study, the findings show that sociodemographic factors namely: advanced age, unemployment, being Protestants and Catholics as well as higher income were negatively associated with improvement in MetS. The findings indicate that social factors have impact in the management and intervention outcomes of CVDs. Programmers and policy makers should plan interventions for CVD prevention and response with these factors in mind.
Keywords
Introduction
Background
Globally, cardiovascular diseases (CVDs) are the primary cause of premature death among the most productive age group (50–70 years) (Roth et al., 2017). Less developed countries have a substantially greater CVD burden than developed ones. For instance, in 2017, 17.9 million premature deaths were ascribed to CVDs; 86% of these occurred in low- and middle-income countries (LMICs) (WHO, 2020). More than half of all deaths in the Sub-Saharan African (SSA) region are attributable to CVDs (Townsend et al., 2016). In Kenya, 28 percent of deaths are related to CVDs (Kenya Ministry of Health, 2018). In addition to the associated mortality and morbidity rates, it is anticipated that the rapid rise in the incidence of CVDs can increase household expenses linked to medical expenses, which can lead to poverty in LMICs (WHO, 2020). The group of linked cardiovascular risk factors known as metabolic syndrome (MetS) is defined by the presence of central obesity, raised FBG, dyslipidemia, and elevated blood pressure (Alberti et al., 2009). Globally, the prevalence of MetS is progressively rising and is regarded as a serious public health issue (Virani et al., 2021). People with MetS are at twice the risk for CVDs and about five-fold the risk for Type-2 diabetes compared with those without the syndrome (Tan & Wand, 2019).
Although everyone is exposed to certain levels of risk factors, some are more burdened than others by social and economic disadvantages, contributing to health inequalities (Atkinson, 2017). Certainly, CVDs are significantly impacted by sociodemographic characteristics such as sex, education, income, employment and job instability, and access to health care (Virani et al., 2021; Wang et al., 2020). In fact, the burden of CVDs falls disproportionately on those from socially disadvantaged backgrounds (Benjamin et al., 2019; Minhas et al., 2023). Because they are more likely to be exposed to dangerous products and have less access to screening and early treatment than persons with favorable socioeconomic standing, vulnerable and socially disadvantaged individuals suffer from CVDs more often and die sooner from CVDs (Havranek et al., 2015). Indeed, cardiovascular events, including heart attack, stroke, and overall mortality, is significantly influenced by sociodemographic variables (Jilani et al., 2021). In the high-income nations, an inverse relationship between socioeconomic status and CVD has been observed (Girolamo et al., 2020; Havranek et al., 2015; Stringhini et al., 2017). Studies performed in Kenyan revealed that the impoverished population is disadvantaged by socioeconomic disparities in hypertension (Gatimu and John, 2020), a major risk factor for CVD (WHO, 2013). Furthermore, in Kenya awareness and detection rates involving CVD remain very low. According to estimates, 75% of Kenyans with hypertension are unaware that they have the condition, and only 4% of those who do aware are able to control their BP (Kenya Ministry of Health, 2018). Nonetheless, there is a dearth of information in Kenya about the direct connection between socioeconomic levels and CVD status.
In Kenya, evidence obtained from the informal settlement dwellers of Nairobi, revealed a high prevalence of the main risk factors for CVDs including, cigarette smoking, consumption of excessive alcohol and an unhealthy diet (Haregu et al., 2015). Because of this, the majority of residents of these informal settlements receives late-stage medical diagnoses and pass away from CVDs and other NCDs at a younger age (Riley et al., 2016). The informal or slums residents are referred to as the “urban poor” and often adopt unhealthy lifestyles (Doulougou et al., 2014). With an average household income of USD 39 per month, Kibera is undoubtedly the biggest and most populated informal settlement in Africa (Mukeku, 2018). Hence, these informal settlements disproportionately suffer from unfavorable social status such as limited access to healthcare services, unemployment and job insecurity, housing and clean water due to their limited purchasing ability, which may contribute for late diagnosis and poor disease outcome.
Sociodemographic factors are frequently viewed as the primary factors impacting cardiovascular health due to their effects on human physiology, health behaviors, and clinical outcomes (WHO, 2019a, 2019b). In addition to lifestyle changes like diet and exercise, sociodemographic characteristics are crucial to take into account during interventions in order to create the best preventative and treatment plans. Certainly, identification of the social factors of cardiovascular health and evaluation their moderation effect on the outcome of interventions could help in designing appropriate health service delivery models to narrow health disparities and thus reduce the burden of CVD in the most disadvantaged population. However, evidence is scarce on the association between sociodemographic factors and improvement in MetS among slum dwelling adults in Kenya. This study, the researchers assessed the association between sociodemographic factors and improvement in MetS among slum dwelling adults in Kenya using a randomized controlled trial design. The findings of this study may be used to inform the designing and development of contextually appropriate strategies and approaches to mitigate health disparities for the prevention and management of CVD.
Literature Review
Globally, CVD is the leading cause of death and long-term illness (Harikrishnan et al., 2018). Regrettably, the LMICs are disproportionately affected by CVD, where more than 80% of CVD deaths occur (Cesare et al., 2023). In the LMICs, a majority of people with CVD remain undiagnosed (WHO, 2019a, 2019b) due to lack of awareness and limited access to screening services (Yuyun et al., 2020). Indeed, the LMICs are far from achieving the equitable distribution of prevention, diagnosis, treatment, and management of CVDs (Cesare et al., 2023).
The rapid urbanization undergoing in the SSA region has been connected to an increase in the prevalence of CVD in this region (Assah et al., 2011). The bulk of people in the SSA who live in cities do so in informal settlements, which are notorious for their high rates of crime, destitution, and lack of access to essential social services (UN-Habitat, 2016). In Kenya, more than half (56%) of the urban population live in slums and 60–70% of Nairobi's population resided in slums and/or slum-like conditions [UN-Habitat, 2016]. Because slum dwellers are poorer than the general population, they are disproportionately exposed to behavioral and metabolic risk factors for CVD (Havranek et al., 2015). For example, the main risk factors for CVD, such as excessive alcohol use, cigarette smoking, and poor dietary habits, are very common among the informal settlement dwellers of Nairobi, Kenya (Haregu et al., 2015).
Sociodemographic variables such as education level, employment, income level can have an impact on behavioral risk factors, which can then have an impact on physiological risk factors that raise the chance of having CVD. Many studies have determined the role of sociodemographic as risk factors for CVDs (Adhikary et al., 2022; Cai et al., 2022; Rahman et al., 2015). Sociodemographic variables may reveal differences in adoption of healthy lifestyles and improvements in CVD risk factors. However, there is insufficient information to determine if sociodemographic variables significantly impact improvements in metabolic syndrome status, a key CVD risk factor. Certainly determining the nature of relationship between changes in CVD risk factors and sociodemographic characteristics is essential for formulating effective plans to reduce inequities in cardiovascular health. In this study, the researchers used a randomized controlled trial design to evaluate the relationship between sociodemographic characteristics and improvements in MetS among persons living in Kenyan slums.
Methods
Study Setting
The study participants were recruited at the outpatient clinic of St. Mary's Mission Hospital in the Langata constituency of Nairobi County, with a 12-month follow-up conducted in the community. The hospital is a faith-based medical institution and serves a sizable number of low-income residents from Kibera and other Nairobi sub-counties at affordable health services. Specifically, with an average monthly household income of just 39 USD, Kibera is the biggest and poorest slum in Africa. The inhabitants reside in modest mud shacks that can accommodate eight or more people (Mukeku, 2018).
Study Design, Sampling Methods, and Respondents
The study materials and techniques have been thoroughly explained elsewhere (Okube et al., 2022). Briefly, the study was a randomized controlled trial involving 352 MetS persons between the ages of 19 and 65 years. A random assignment was used to place the eligible participants in the intervention or control groups on an equal ratio. The International Diabetes Federation's guideline was used to determine MetS (Alberti et al., 2009). In addition to central obesity (waist circumference of ≥94 cm for males and ≥80 cm for women), a person was classified as having MetS if the person had at least two of the main CVD risk factors namely: decreased HDL-C (<1.03 mmol/L in males and <1.29 mmol/L in females), high blood pressure (systolic BP ≥ 130 mm Hg and/or diastolic BP ≥ 85 mm Hg) or previously diagnosed hypertension, elevated TGs (≥1.7 mmol/L), and elevated FBG (≥5.6 mmol) or known type-2 diabetes. The participants were followed for 12-months.
The participants had to meet the following inclusion criteria at baseline: be between the ages of 18 and 64; have a waist circumference of at least 80 cm for women and 94 cm for men; and have at least two risk factors for CVDs (low HDL-C, high TGs, elevated BP, and raised FBG). The exclusion criteria were: pregnant and nursing women, those with significant illnesses including cancer, cardiovascular events, mental illness, or physical impairment.
Sample Size Calculation
The formula by Casagrande et al. (1978) was used to established the required sample size

α = 0.05 (Type I error), β = 0.10 (Type II error), at 95% confidence interval, Ζ1−α/2 = 1.96, and at 90% power, Ζ1−β = 1.28.
P1= Prevalence of MetS at 25.6% in Kenya (Omuse et al., 2017) in the control arm.
P2= Rate of MetS in the intervention arm to be 11.6% (assuming that the lifestyle intervention will reduce the prevalence of MetS by 14%). Thus, the effect size was 14%.


In addition, 10% (n = 16) of each group’s initial estimated sample size was added to account for attrition. Thus, there were 176 responders in each group, totaling 352 participants.
Randomization and Allocation of Study Subjects
Block stratified randomization was used to select and randomly assign eligible individuals to the groups. The method was splitting up the subjects into groups of 16 on average every block. According to a written piece of paper, individuals from each block were assigned at random to either the intervention group (IG) or the control group (CG). Recruitment of the participants was done by the research assistants, while allocation into the groups was determined by the principal investigator. The research assistants and the participants were blinded during the randomization. Furthermore, the laboratory, clinical and physical measurements were determined by individuals who were blinded to the groups.
Study Intervention
The intervention group received a thorough and customized lifestyle intervention that comprised individual health education delivered verbally and in writing form. The health education intervention was targeted the common behavioral risk factors for MetS and CVDs (WHO, 2019a, 2019b). This includes abstaining from alcohol drinking and smoking, engaging in physical activity, and following suggested food patterns (Supplementary Materials-I). While, the control group received standard care from medical professionals in accordance with the hospital's protocol. Drug therapy, patient counseling, screenings, and examinations were all part of the standard care. The study outcome included changes in prevalence of Metabolic Syndrome and its components.
Data Gathering Instruments and Techniques
A researcher-assisted structured questionnaire that was adapted from the WHO's STEP-wise method to NCD risk factor surveillance was used to gather the data (WHO, 2017). The tool was divided into four sections: demographic characteristics, dietary and physical activity intake patterns and physical and biochemical measurements (Supplementary Materials-II). The data were gathered by two research assistants who had a bachelor's degree in nursing. Two seasoned lab technicians who were blind to the groups collected and analyzed samples of fasting blood glucose and cholesterol levels.
Validity and Reliability of the Study Tool
The data were gathered using the WHO-steps approach to NCDs behavioral risk assessment questionnaire (WHO, 2017). Nutrition and CVD specialists revised the instruments’ validity in terms of content, and their comments were incorporated into the questionnaire. To ensure its validity, the BP device utilized in this study was regularly cross-checked with another the hospital's device. After three weeks, the questionnaire was retested using the test-retest method to gauge its reliability. The level of agreement between the two outcomes was ascertained using Cohen's kappa coefficient. A 0.91 kappa value was obtained from the repeated questions, which was considered reliable.
Data Analysis
IBM SPSS (Ver. 22) Statistics Software was used for data analysis. A binary logistic regression analysis and the chi-square test of independence were used to see if there were any significant differences between the sociodemographic characteristics and improvements in MetS. The association between the sociodemographic characteristics acting as independent variables and the improvement in MetS acting as a dependent variable was examined using a multivariate logistic regression model with backward conditional. Statistical significance was considered when the p-value was less than 0.05.
Participants’ Recruitment and Follow-up
Using IDF diagnostic criteria, 404 persons who had central obesity were examined for the presence of MetS; 352 were determined to be affected. Participants with MetS were randomly assigned to either standard CVD care group or lifestyle intervention group over a 12-month period. Of the participants, 294 (138 from the control and 156 from the intervention group) completed the study period. Fifty-eight individuals (control = 38; intervention = 20) left the study mostly due to poor compliance and lost follow-up. A few of the participants left the programme due to residence relocation, travel to other counties, and pregnancies of two women. There was no noticeable difference in terms of sociodemographic characteristics between those who left the study and those who completed it (Figure 1).

Consort flow diagram of the study participation (F = female; M = male).
Results
The Link Between Demographic Charactristics and Improvement in MetS status in the Intervention Group
Participants who completed the study program were included in the final analysis (Figure 1). Age, marital position, religion, educational attainment, and work position in the intervention group were among the sociodemographic factors that were strongly associated with improvements in MetS after the intervention. Aged (≥50 years) individuals had a 10-times (COR = 10.095; P < .001) increased likelihood of not seeing improvement in their MetS status as compared to respondents under 50. Compared to Muslim respondents, respondents who identified as protestants (COR = 8.595; P = .007) and Catholics (COR = 8.182; P = .010) had about eight times higher rates of MetS after the intervention. Improvement in MetS status was 2.5 times higher among participants who attained postsecondary education levels compared to those with primary (COR = 2.500; P = .052) and secondary (COR = 2.559; P = .013) levels of education. When compared to respondents who were divorced/separated/widowed and jobless, the improvement in MetS status was significantly bigger among married (COR = 0.175; P = .026) and employed (COR = 0.204; P = .004) respondents, respectively (Table 1).
The Link Between Demographic Charactristics and Improvement in MetS Status in the Intervention Group.

Note. D/S/W = divorced/separated/widowed; COR = crude odds ratio.
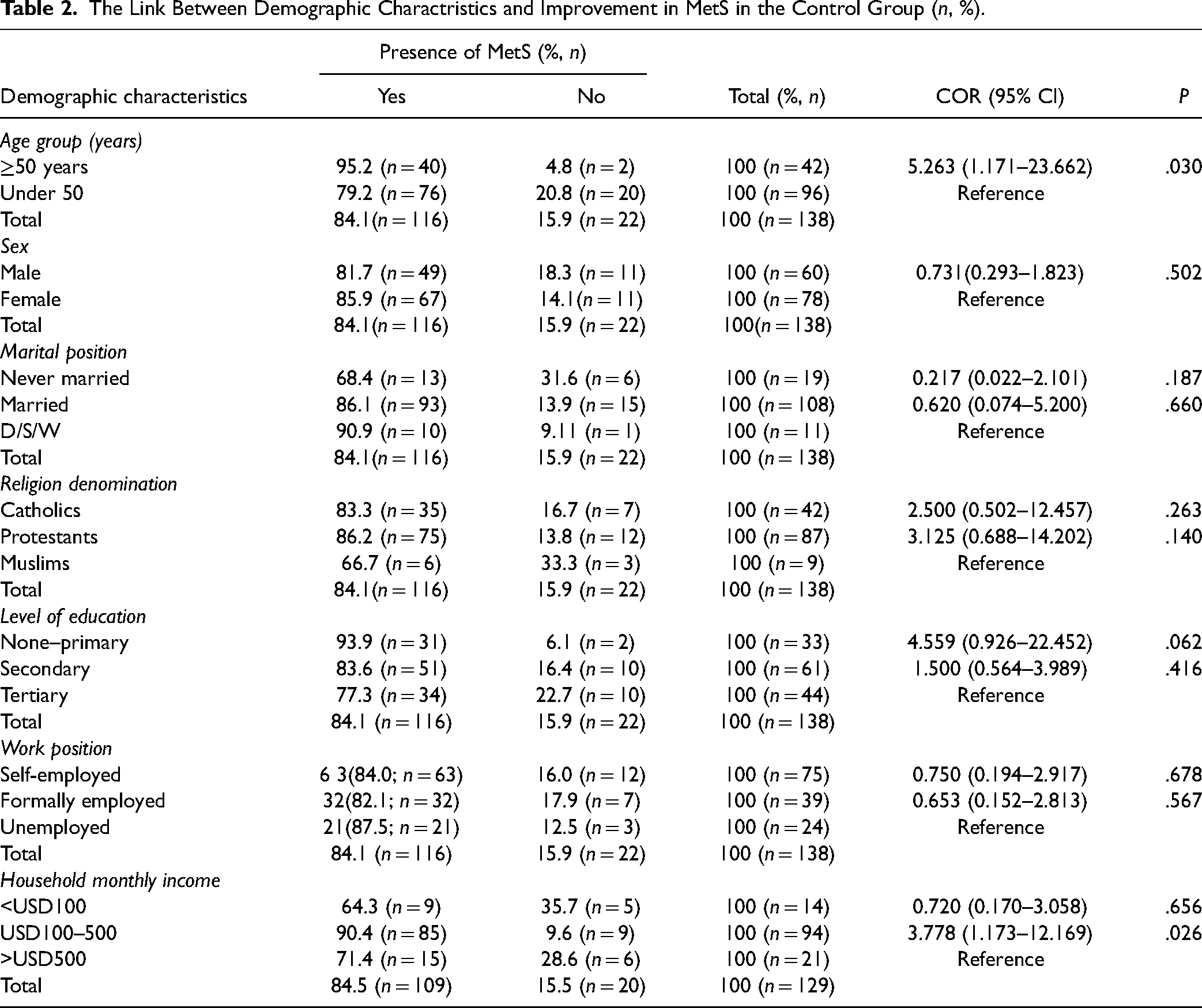
The Link Between Demographic Charactristics and Improvement in MetS in the Control Group
The study revealed a significant correlation between the age and income level of the respondents and the improvement in MetS in the control arm after the intervention. Aged (≥50 years) individuals had a 5.3-fold (COR = 5.263; P = .030) increased likelihood of not seeing improvement in their MetS status as compared to respondents under 50. Compared to respondents with monthly incomes over USD 500, individuals with incomes between USD 100 and USD 500 (OR = 3.778; P = .026) were approximately four times as likely to have a lack of improvement in their MetS status (Table 2).
The Link Between Demographic Charactristics and Improvement in MetS in the Control Group (n, %).
Demographic Charactristics Independently Linked to Improvement in MetS in the Intervention Group
Using a multivariate logistic regression analysis, the independent sociodemographic variables associated with MetS improvement were identified. Age, marital position, religion denomination, education attainment, and work status were all substantially (P < .05) linked to improvement in MetS in the intervention group at bivariate analysis. After running these variables through a multivariate analysis and using the “backward conditional” system and removal at P < .05, it was discovered that age, religion denomination, and work position independently predicted MetS improvement. The fitness model was found to be 0.573 using the Hosmer and Lemeshow Test, indicating that the model fits. Respondents 50 years of age and older had a 9-fold [AOR = 9.097; P < .001] greater likelihood of not seeing improvement in their MetS status than respondents under 50 years of age. In comparison to Muslims, respondents who identified as Protestants [AOR = 7.292; P = .017] and Catholics [AOR = 5.270; P = .050] were seven and five times, respectively, more likely to have a lack of improvement in MetS. Compared to respondents who were unemployed, formally employed respondents were significantly more likely to have improved their MetS status [AOR = 0.154; P = .005] (Table 3).
Demographic Charactristics Independently Linked to Improvement in MetS in the Intervention Group.

Note. D/S/W = divorced/separated/widowed; AOR = adjusted odds ratio. The fitted model's goodness of fit was evaluated using the Hosmer–Lemeshow test; a p-value of .573 suggests that the fitted model is sufficient.
Demographic Charactristics Independently Linked to Improvement in MetS in the Control Group
Age and household income were the demographic characteristics that were substantially (P < .05) correlated with MetS improvement in the control group during a bivariate analysis. Following a multivariate examination of these variables, age and income continued to be independent predictors of improvement in MetS. The aged (≥ 50 years) respondents showed a five-times [AOR = 5.013; P = .047] greater lack of improvement in their MetS status than the younger (<50 years) respondents. When compared to respondents with monthly incomes of less than USD100, individuals with incomes between USD100 and 5000 were 10-times [AOR = 10.499; P = .024] more likely to not seeing improvement in their MetS status (Table 4).
Demographic Charactristics Independently Linked to Improvement in MetS in the Control Group.

Note. According to Hosmer–Lemeshow test, the fitted model produced a p-value of .573, indicates that the fitted model is satisfactory.
Discussion
In this study, the findings revealed that age, religion denomination, and employment status in the intervention group, and age and household income level in the control group were markedly and independently linked to improvement in MetS status following the 12-months lifestyle intervention. Improvement in MetS was significantly higher among respondents who were formally employed and those belonged to Muslims in the intervention group. On the other hand, older people (≥50 years old) were more likely to have not improved their MetS status in both the groups. Moreover, individuals with higher monthly incomes in the control group were more likely to display no change in MetS status. The current study sheds light on the dynamics of socio-demographic factors in the prevention and management of CVD risk factors.
The lack of improvement in MetS status among aged (≥50 years) respondents was consistent with recently conducted studies (Chung et al., 2021; Iqbal et al., 2020; Jahangiry et al., 2019; Okube et al., 2020), which have indicated a clear correlation between MetS and age. Numerous CVD risk factors, including insulin resistance, inflammation, decreased baroreceptor activity, the kidneys’ buffering function, and blood vessel stiffening, are strongly correlated with aging (Adeva-Andany et al., 2019; Penuela & Penuela, 2015). Furthermore, older people are more likely to experience a lack of improvement in their MetS status because they rarely engage in an adequate level of physical exercise (Kim & Hwang, 2018). In particular, for older women, this can be supported by gradual hormonal changes brought on by a drop in estrogen level of concentration (Rodgers et al., 2019). This emphasizes the necessity to take age into account when developing and implementing interventions aimed at controlling and preventing CVD.
The finding of the current study indicates that Muslim respondents in the intervention group significantly improved their MetS status compared to Protestant and Catholic respondents. The likely reason for such difference is that Muslims and believers of other religions lead somewhat different lifestyles. Muslims, for instance, abstain from alcohol, which is a significant risk factor for MetS (Shimoshikiryo et al., 2020). The impact of the Ramadan fasting may be an additional factor. A study by Sadiya et al. (2011) shown how fasting throughout Ramadan protects against MetS. During the Ramadan fasting, a person fasts for 13–18 h a day, which can lower MetS indicators like levels of blood glucose, triglycerides, and cholesterol (Silva et al., 2023). A recently performed systematic review and meta-analysis indicated that Ramadan fasting positively impact the MetS components and the overall MetS status (Jahrami et al., 2022).
In the current study, improved MetS status was significantly observed among formally employed people than unemployed individuals, which is consistent with a study conducted by Chung et al. (2021). People without work are probably older and retired, which puts them at a higher risk of getting age-related MetS. In fact, aging is strongly linked to a number of factors that can exacerbate metabolic syndrome, including decreased baroreceptor function, blood vessel hardening, insulin resistance, and renal buffering activity (Huang et al., 2022). Moreover, bad lifestyle choices such as smoking, eating poorly, drinking alcohol, and not exercising—have a positive correlation with unemployment (Zagożdżon et al., 2014) major risk factors for MetS. Furthermore, low socioeconomic level is a typical cause of chronic stress that promotes a proinflammatory state and atherogenesis (Miller et al., 2019; Schultz et al., 2018), key risk factors for MetS and CVDs. Individuals without a job are therefore more likely to have these conditions. Indeed, socially disadvantaged people are disproportionally burdened with cardiovascular risk factors and CVD due to socioeconomic disparities (Atkinson, 2017). Therefore, developing and implementing a CVD preventive program with an emphasis on the unemployed is essential.
Those with higher monthly incomes in the control group were noticeably more likely to display no improvement in MetS. This finding is consistent with researches conducted by Rosengren et al. (2019) and Hulzebosch et al. (2015), which demonstrated a direct correlation between MetS and income level in low- and middle-income nations. Conversely, studies performed in industrialized nations revealed a negative correlation between MetS and income (Abdalla et al., 2020; Minhas et al., 2023). The disparity in lifestyle between developed and underdeveloped nations can account for this variance. High earnings in underdeveloped nations tend to lead sedentary lives and regularly consume junk and processed food. On the contrary, people in the developed world have an active lifestyle and consume quality foods (Micklesfield et al., 2013). Sociodemographic characteristics should be taken into account when designing and implementing interventions in order to minimize health disparities and lower the burden of CVDs in the less developed nations.
The Strength and Limitations of This Study
This study is strengthened by its randomized controlled trial design in which the findings are attributed to the lifestyle intervention and not by chance. This is the first study in Kenya that determined the sociodemographic factors associated with improved Metabolic Syndrome in slum dwelling adults in Kenya. This is a novel finding that, by taking social factors of cardiovascular health into account, can have a significant impact on the prevention and early management of cardio-metabolic disorders. However, the findings should be interpreted with some limitations. All the participants were recruited from Nairobi, the capital city of Kenya. Thus, it may be difficult to extrapolate the findings to other areas given the variations in socioeconomic and demographic factors.
Implications for Practice
Cardiovascular disease risks are influenced by social determinants of health, including sociodemographic status. The findings of the current study revealed that advanced age, unemployment as well as higher income were negatively associated with improvement in MetS, a major risk factor for CVD. The data on the sociodemographic implications of CVD are needed to inform preventive interventions and can drive the agenda for future health financing models. Thus, understanding sociodemographic inequalities in CVD risk factors is key to inform policy, practice and science on the prevention and management of CVD.
Conclusion
Sociodemographic factors have a significant impact on CVD risk and intervention outcomes among low income communities. In this study, the indings show that sociodemographic variables such as advanced age, unemployment, being Protestants and Catholics as well as higher income were negatively associated with improvement in MetS. The findings indicate that sociodemographic factors not only influence the incidence of CVDs, but they also impact the management and the outcomes of CVDs. Such findings may have the potential to inform science, policy, and practice for better planning and designing of appropriate strategies for the prevention of CVDs. Consideration of sociodemographic factors during lifestyle intervention are essential to guide public health efforts and narrow disparities in the burden of CVDs. To tackle the disparities in CVD burden and treatment outcome, innovative equity-focused interventions supported by health, economic, and demographic rationales are needed.
Supplemental Material
sj-docx-1-son-10.1177_23779608241299647 - Supplemental material for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial
Supplemental material, sj-docx-1-son-10.1177_23779608241299647 for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial by Okubatsion Tekeste Okube, PhD and Samuel T. Kimani, PhD in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241299647 - Supplemental material for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial
Supplemental material, sj-docx-2-son-10.1177_23779608241299647 for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial by Okubatsion Tekeste Okube, PhD and Samuel T. Kimani, PhD in SAGE Open Nursing
Supplemental Material
sj-doc-3-son-10.1177_23779608241299647 - Supplemental material for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial
Supplemental material, sj-doc-3-son-10.1177_23779608241299647 for Sociodemographic Factors Associated with Improved Metabolic Syndrome in Slum Dwelling Adults in Kenya: A Randomized Controlled Trial by Okubatsion Tekeste Okube, PhD and Samuel T. Kimani, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
The authors thank the personnel at St. Mary’s Mission Hospital (SMMH) for their support during the data collection period. They also thank SMMH's administration for allowing us to conduct this research there.
Availability of Data and Materials
The data set used to generate this results is available on a seasonal request
Contributions of the Authors
The study’s conception was shared by OT and SK. OT and SK involved in the design of the study including the study protocol. OT drafted the manuscript, which SK carefully edited. The final manuscript was reviewed and approved by both authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
An Ethical Review Committee (ERC) board constituted by the University of Nairobi and Kenyatta National Hospital approved the study (Reference number: P430.07/2017). Prior to being enrolled in to study, each participant gave their written informed permission. In order to safeguard the participants’ privacy, all of the data obtained remained anonymous and was handled with absolute confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.