
Abstract
Introduction
Health literacy refers to acquiring and utilizing health information to make health-related actions and decisions. Filipino domestic workers with low health literacy are often vulnerable to health problems due to poor living and working conditions.
Objective
This study examined the effect of an online health literacy promotion program on health literacy and health knowledge of Filipino domestic workers in Macao.
Methods
The mixed method combined quantitative findings of a quasi-experimental study with qualitative results applied. The quasi-experiment included three parallel groups: a synchronous online education group (videoconference group), an asynchronous online education group (video group), and a control group. A total of 88 Filipino domestic workers were assigned to one of these groups, and eight respondents participated in two focus-group interviews respectively after the intervention.
Results
For quantitative data, both synchronous and asynchronous online education interventions had positive effects. While comparing with the control group, participants in the videoconference group were more likely to have better health promotion health literacy after the intervention (β = 5.36, p = .02), and participants in the video group were more likely to have better general health literacy (β = 5.17, p = .01), disease prevention health literacy (β = 5.31, p = .04), health promotion health literacy (β = 5.97, p = .01). For qualitative data, three themes and eight subthemes were extracted after the online health literacy promotion program. After integrating the findings of this study, the study found that this program was essential and beneficial for Filipino domestic workers’ health knowledge and health literacy.
Conclusion
Overall, online health literacy promotion programe had positive impacts on participants revealed in this study. Asynchronous online education has made significant progress in overall health literacy, which may be more suitable as a widely promoted education method because of the characteristics and working conditions of this population.
Keywords
Introduction
Health literacy refers to the skills and abilities to access and utilize health information to make appropriate decisions about health-related issues (World Health Organization [WHO], 1998). Health literacy is a significant predictor of health knowledge (Baker, 2006; Quinlan et al., 2013; Speros, 2005). Based on a more comprehensive understanding of health literacy, health knowledge can also be conceptualized as a dimension of health literacy (Gellert & Tille, 2015). Adequate health literacy, which implies a better ability to identify and follow healthy habits and a greater willingness to self-manage health conditions, is seen as a key factor influencing people's use of health services and the control of diseases, thereby affecting the health outcomes of society (Bernadas, 2015; Marmot, 2005; Sørensen et al., 2012; Tejero & Fowler, 2012). According to the integrated model of health literacy developed by Sørensen et al. (2012), health literacy can be influenced by (a) societal and environmental determinants (e.g., language), (b) personal determinants (e.g., socio-economic status), and (c) situational determinants (e.g., social support). Poor socio-economic status and living conditions, language barriers, limited access to education, and chronic stresses caused by social alienation can all contribute to inequalities in healthcare (Bernadas, 2015; Maarmot, 2005).
As a minority group in host countries, foreign domestic workers are likely to be marginalized and face challenges when accessing health information or services. Poor work conditions, long working hours, and lack of social contact exacerbate the limited health knowledge of foreign domestic workers (Bernadas, 2015; Tejero & Fowler, 2012). Coupled with the experience of culture shock, language barriers, and limited knowledge of the health system make it difficult for foreign domestic workers to access health information and lead to low levels of health literacy, poor self-health management, and vulnerability to diseases (Bernadas & Jiang, 2015; Chen et al., 2022; Cheong et al., 2021; Gibson, 2012; Kirmayer et al., 2011; Lindert et al., 2009; Maneze et al., 2016; Rechel et al., 2013; Straiton & Myhre, 2017; Tai & Yang, 2022).
Currently, the number of Filipino domestic workers in Macao is approximately 12,900. Accounting for approximately half (58.8%) of the non-Chinese domestic workers, the remaining non-Chinese domestic workers are mostly from Vietnam (19.5%), Indonesia (15.1%), and Myanmar (5.8%) (Labour Affairs Bureau of Macao SAR Government, n.d.). Cheong et al. (2021) studied the status of health literacy among Filipino domestic workers in Macao and found that only 37.4% of the respondents had sufficient general health literacy. According to Hall et al. (2019), Filipino domestic workers in Macao suffered from various health issues exacerbated by inadequate support in accessing healthcare resources, unfavorable working conditions, long hours, exploitation, and a host of health problems (Bernardo et al., 2016; Cheong et al., 2021; Hall et al., 2019). A scoping review found that exploitation, persistent economic hardship, poor working conditions, and social isolation posed significant barriers for foreign domestic workers accessing health services in Hong Kong (Ho et al., 2023). In Macao, the available health information is often provided in Chinese and Portuguese, the languages that most Filipino domestic workers know little about, making it challenging for them to communicate with locals when accessing services (Cheong et al., 2021; Hall et al., 2019). Limited knowledge and insufficient access to appropriate healthcare and social support have also contributed to a lack of trust in local healthcare, leading to reluctance to seek treatment (Hall et al., 2019). Therefore, more attention should be paid to the health needs among vulnerable populations like Filipino domestic workers by providing more accessible and readable health information, implementing an online health literacy promotion program to support them in making health decisions. This is a point that cannot be overstated.
Review of Literature
The popularity of the Internet has transformed the way people access health information. Online education is seen to enable more people to be informed and empowered to better manage their health and risk factors at lower cost and with fewer human resources, and it has been established in different health fields as a flexible and cost-effective means of delivering health education or training (Chou et al., 2013; Korda & Itani, 2011; Samoocha et al., 2010).
Extensive research has demonstrated the effectiveness of online interventions in enhancing health literacy levels and improving health outcomes among diverse populations. Online platforms offer a convenient and accessible medium for delivering health information, overcoming language barriers, and addressing the specific needs of diverse communities (Chen & Wang, 2021). Moreover, online health interventions have been found to strengthen health knowledge, self-efficacy, and self-management skills, empowering individuals to make informed decisions about their health (Niu, Willoughby, & Zhou, 2021). Additionally, online platforms like video conferencing software can facilitate peer support and virtual community engagement. This enables individuals to connect with others facing similar health challenges, share experiences, and access social support networks (Newman et al., 2019).
Regarding online education, asynchronous and synchronous are often compared. Asynchronous online education setting means that learning is not limited by time and place and can be arranged based on an individual's schedule, while synchronous online education is real-time interpersonal interaction and immediate feedback (Blau et al., 2017; Fabriz et al., 2021).
Asynchronous video has been used in many ways for online courses, which also have been regarded as health knowledge transfer tools to supplement or replace traditional training. Individuals with lower health literacy were more inclined to video-based education (Myint-U et al., 2010). On the other hand, a meta-analysis of randomized controlled trials showed that webinar sessions were more effective than asynchronous learning (d = .044) and face-to-face instruction (d = .156) (Gegenfurtner & Ebner, 2019). Further, studies show that internet-based education can effectively teach foreign workers regardless of age, education level, and working conditions (Cai & Abbott, 2013; Gegenfurtner & Ebner, 2019; Gegenfurtner et al., 2020; Lee & Lee, 2015; Tseng et al., 2019). Research by Hall et al. (2018) found that most Filipino domestic workers in Macao owned a smartphone and had access to the Internet, given the flexibility and effectiveness of online platforms for disseminating health knowledge. Nonetheless, existing research on health literacy for Filipino domestic workers currently focuses on mental health literacy in the United Kingdom, in which a lack of effectiveness among asynchronous, synchronous, internet-based education of health literacy promotion program was examined (Martinez et al., 2022).
To address this gap, the purpose of this study is to examine the effectiveness of an online health literacy promotion program among Filipino domestic workers in Macao. By leveraging the power of the programs, tailored to the specific needs and preferences of Filipino domestic workers in Macao, it is possible to bridge the gap in health knowledge, empower individuals to take control of their health, and ultimately improve their overall wellbeing. We hypothesized that this program would promote a positive change in health literacy and health knowledge of Filipino domestic workers in Macao.
Methods
Study Design
Health literacy is measured using a mixed method approach, as recommended by the WHO (World Health Organization, 2014). The study followed this recommendation, applying a mixed method approach to measure health literacy. This present study used a mixed method combining quantitative findings of a quasi-experimental study and qualitative results from interviews (Polit & Beck, 2017). With a mixed method design, embedding usually occurs in interventional studies (Fetters et al., 2013). This study applies embedding as the mixed method integration at the methods level according to Creswell and Plano Clark's (2011) concept of integration. In embedding, qualitative data is collected after a trial to interpret outliers and report to researchers on experiences or events. Results from quantitative measures and qualitative interviews were integrated to inform and enrich each other's overall findings and to recognize areas of consistency and inconsistency in the results, which were discussed to produce a more comprehensive understanding of the outcomes of the health literacy program (World Health Organization, 2014).
The quasi-experimental included three parallel groups, including a synchronous education group (videoconference group), an asynchronous online education group (video group) and a control group (website group). In addition to posting e-poster recruitment on social media platforms, participants were recruited by sharing posts that include e-posters on social media through nongovernmental organizations (NGOs) providing support to Filipino domestic workers in Macao. To avoid duplicate participation, participants in the three groups were tested on the same day, and the electronic questionnaire used was restricted by IP address to avoid repetition. Pretest and post-test were performed respectively before and after the intervention.
Research Questions
How is the effectiveness of an online health literacy promotion program for Filipino domestic workers?
What are participants’ perceptions of the online health literacy promotion program?
Participants and Data Collection
Data collection took place from January to February 2023 in Macao. All Filipino domestic workers working in Macao were eligible to participate. Exclusion criteria were holding Macao resident identity cards or being informally employed in domestic work (e.g., trial work, part-time work, etc.). The sample size calculation was performed using G*Power 3.1. We assumed an effect size of 0.35 (medium) for the within–between interaction of group and time in repeated-measurements analysis of variance with three groups and two points of measurement (α = .05; Power = 0.8), and a total sample size of 67 was indicated. Considering a 10% reduction due to withdrawal, we aimed to recruit at least 25 subjects per group. In similar studies, the sample size varies between 21 and 26 per experimental group (Blau et al., 2017; Martinez et al., 2022). A nonrandom assignment was made after participants enrolled. For example, when the videoconference group was about to start, participants were preferentially assigned to this group, and those who entered later were assigned to the other two groups. All participants were invited from the videoconferencing and video conferencing groups, respectively, to additionally participate in focus group interviews.
Ethics Considerations
The study was approved by the Research Management & Development Department, Kiang Wu Nursing College of Macau (REC-2021.1203). The study was conducted following the Code of Ethics of the World Medical Association (Declaration of Helsinki) for research studies involving humans (World Medical Association, 2013). Written consent was obtained from participants online. Confidentiality and anonymity were guaranteed. Participants’ information was kept anonymous throughout the study, and only the research team had access to used, or disclosed it. All participants received a supermarket voucher (MOP$100) to compensate them for their time and mobile data usage.
Intervention
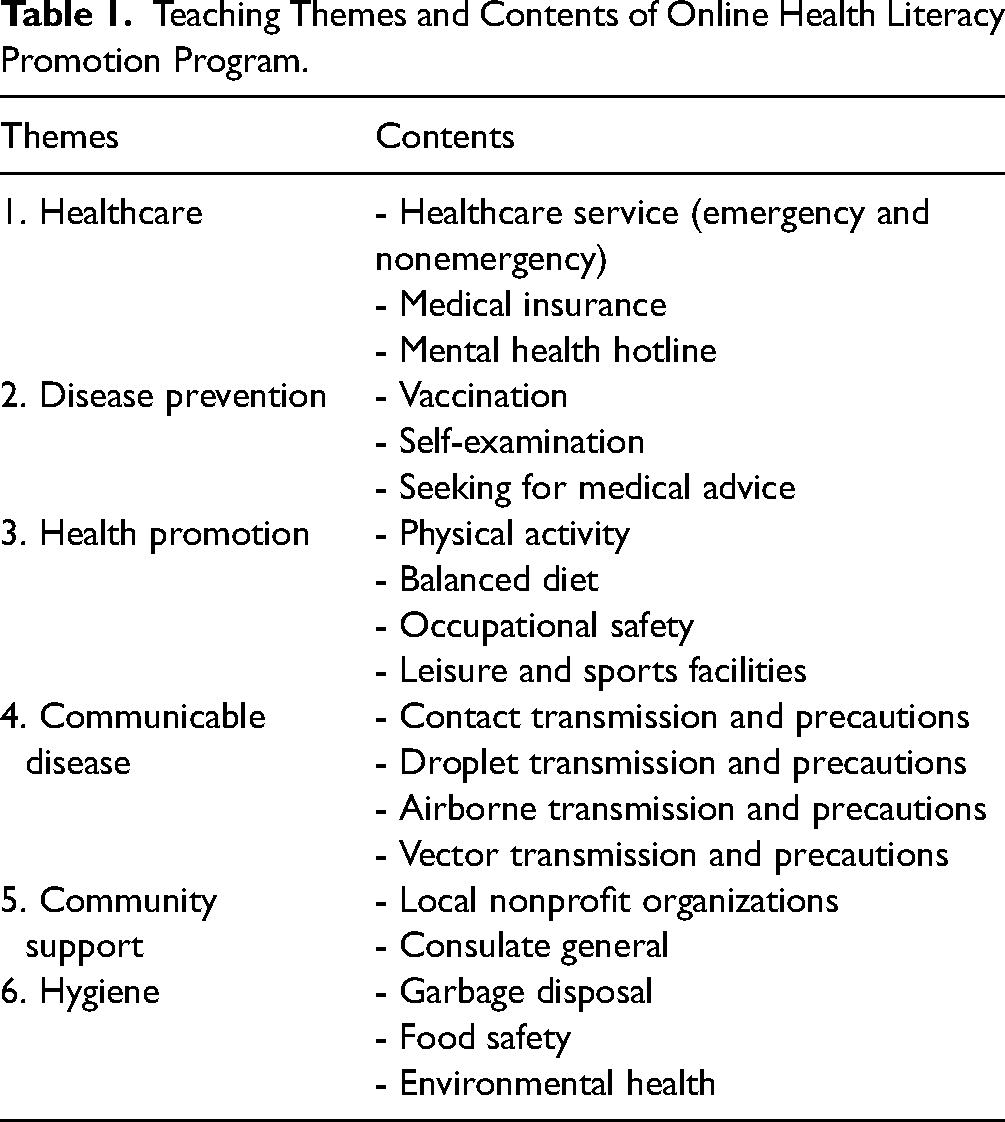
To enhance health literacy, support for empowerment is needed. Studies showed that empowerment is most important for health literacy and that social determinants of health, individual and group perceptions of health, and health needs must be included and highlighted (Crondahl & Eklund Karlsson, 2016). Empowerment is a process of promoting knowledge and skills and increasing awareness of social conditions. In this study, we value cultural adaptation and empowerment in the research and following the recommendations of effective participatory processes from culturally and linguistically diverse backgrounds when developing health education videos (O’Mara, 2013). Based on the health literacy model proposed by Sørensen et al. (2012), a conceptual framework for health literacy promotion programs was formulated. By partnering with NGOs that advocate for Filipino domestic workers in Macao, Filipino domestic workers were invited to design health literacy teaching themes and make health literacy education videos. Furthermore, social workers who work with Filipino domestic workers were invited to share their views on the teaching themes and content. The teaching themes were then confirmed and divided into six themes: healthcare, disease prevention, health promotion, communicable disease, community support, and hygiene refer to Table 1 for more detail. Tagalog, Filipino domestic workers’ preference language, was adopted to introduce relevant health information in Macao. The study included two experimental groups (videoconference and video) and one control group. The teaching contents of health literacy in the two experimental groups were the same, but the teaching methods were differed. Participants in the video group watched a health literacy education video as an intervention, while those in the videoconference group attended an online health literacy lecture with interactive sessions via Zoom. A trained nursing background Filipino as a tutor in the videoconference group. The control group did not receive any health literacy teaching and was only provided with relevant websites for health information, but they were supplemented with health literacy education videos after the test.
Teaching Themes and Contents of Online Health Literacy Promotion Program.
Measures
Quantitative Measures
An electronic questionnaire was used in this study. Each consisted of (1) demographic data, (2) health literacy (Short-form Health Literacy Instrument, HLS-SF12), and (3) health knowledge.
Referring to the results of Cheong et al. (2021) health literacy survey of Filipino domestic workers, demographic data in this study included gender, age, level of education, living status, English and Chinese proficiency, diagnosed diseases, self-evaluation of health, and main channel for health information.
The health literacy scale was self-reported, and the HLS-SF12 developed by Duong et al. (2019) was used, covering 12 items and three dimensions, including healthcare, disease prevention and health promotion. Participants ranked the items on a Likert-style 4-point scale (Very difficult =1, Quite difficult = 2, Fairly easy = 3, Very easy = 4). Index scores were standardized between 0 and 50, using the formula: index = (mean – 1) × (50/3). The total score ranges from 1 to 50. As suggested by the European Health Literacy Project, a health literacy index of 33 or less health literacy index is regarded as limited health literacy (HLS-EU Consortium, 2012). In our previous project, the HLS-SF12 has been translated back into Tagalog with good reliability and validity (α = .94) (Cheong et al., 2021).
Since health knowledge is a key feature of critical health literacy, health knowledge questions were also developed to understand participants’ health knowledge levels (Sykes et al., 2013). Ten true-false knowledge questions on health literacy were formulated based on the health literacy model by Sørensen et al. (2012), combined with the specific circumstances of Macao and the characteristics of Filipino domestic workers. For example, healthcare service, knowledge of disease prevention, health promotion, and safety measures. A panel of experts was consulted, and their comments were further discussed to fine-tune the final health literacy test, see Table 2. The scoring method is one point for correct answers and none for incorrect or uncertain answers; a score of 5 or less for health knowledge is regarded as limited health knowledge.
Health Knowledge Questions

Qualitative Interviews
Focus group discussions were conducted to understand the experience of the online health literacy promotion program and to triangulate the potential effectiveness. After completing the online health literacy promotion program, all participants in both experimental groups were invited to participate in focus group interviews conducted in Tagalog via videoconference. A Filipino with a nursing education background facilitated the focus group interviews. The participants had been given qualitative research training in advance, including the role of an interviewer, ethical issues, data collection procedures, and moderating skills. A mock interview within the research team was also conducted (Greenbaum, 2000; Goodell et al., 2016). A semistructured interview guide questions was adapted to ask participants to provide feedback on the online health literacy promotion program and recommendations for improvement (see Table 3). The interviewer used open-ended questions with the group participants. The interview was transcribed word for word and translated into English, then checked for accuracy by the interviewer and another expert fluent in Filipino and English. In addition, participants volunteered for focus group interviews and were fully informed that they could withdraw from the study at any time. Information may be disclosed by focus group members or researchers, and both internal and external research confidentiality was protected in this study, including anonymity throughout the research process, and participants were notified and required to adhere to confidentiality principles prior to focus group interviews. The interviewer observed the interactions within the group during the process to alert potential distress, violation of confidentiality, or over-disclosure. The fact that a significant number of participants declined to take part in the interview may indicate that they freely made the decision to participate.
Semistructured Interview Guide Questions

Data Analysis
Data sorting and statistical analysis were performed using SPSS 26.0. Descriptive statistics, including mean, standard deviation (SD), and pretest/post-test differences, were utilized to provide information on the three groups. To assess the program's effect, the generalized estimating equation (GEE) was applied for inferential statistics to account for repeated binary measurements in logistic regression analysis. This allowed for the evaluation of the procedure's impact. A significance level of α < 0.05 was considered statistically significant.
Focus group data were analyzed using inductive thematic analysis. The trustworthiness of the study was established by a series of measures. (1) Having a team of experienced researchers: All research team members had postgraduate degrees, two of them independently analyzed the transcripts in NVivo10 software. Interview transcripts were analyzed and coded according to Braun and Clarke (2012) the six-phase process: familiarizing data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing a report. (2) Conducting member checks: The two sets of codes were then merged and agreed upon by the authors. After that, a primary researcher reviewed the results of the coding, and other members of the research team approved the analytic results, to ensure intercoder reliability and credibility. The research team then sent transcribed interviews and analytic results to the participants to validate the transcription accuracy and to enhance confirmability. (3) Possessing triangulation of data sources: The quantitative and qualitative results were analyzed simultaneously to allow triangulation and convergence of the data, in order to enhance the integration of conclusions. Apart from having the same occupation and nationality, the different backgrounds of the participants also contributed to the triangulation.
Quantitative and qualitative results were analyzed simultaneously, and the findings of both were merged and compared at the interpretation stage in order to enhance the conclusions.
Results
Participant Characteristics
Figure 1 shows participant allocation and the flow of subjects. A total of 152 participants were collected, of which 88 (57.9%) were effective. Invalid questionnaires mainly refer to incomplete participation in the study. Participants were assigned to receive either videoconference education (n = 30), video group (n = 31), or website information group (n = 27). The demographic characteristics of the participants are shown in Table 4. All participants were female, with a mean age of 47.82 years old (SD = 8.47). Most of them had college degrees, had average English proficiency and poor Chinese proficiency, and were living with the employer. In terms of channels for health information, Macao and the Philippines government websites and social media were the most popular channels chosen by participants. After intervention, a total of eight participants consented to participate to focus group interviews. Participants in videoconference group (n = 4) and video group (n = 4) were interviewed in separate group. While the remaining participants declined due to scheduling or lack of interest in participating. Two focus groups were conducted online in Tagalog via videoconference, each lasting approximately 30–40 min.
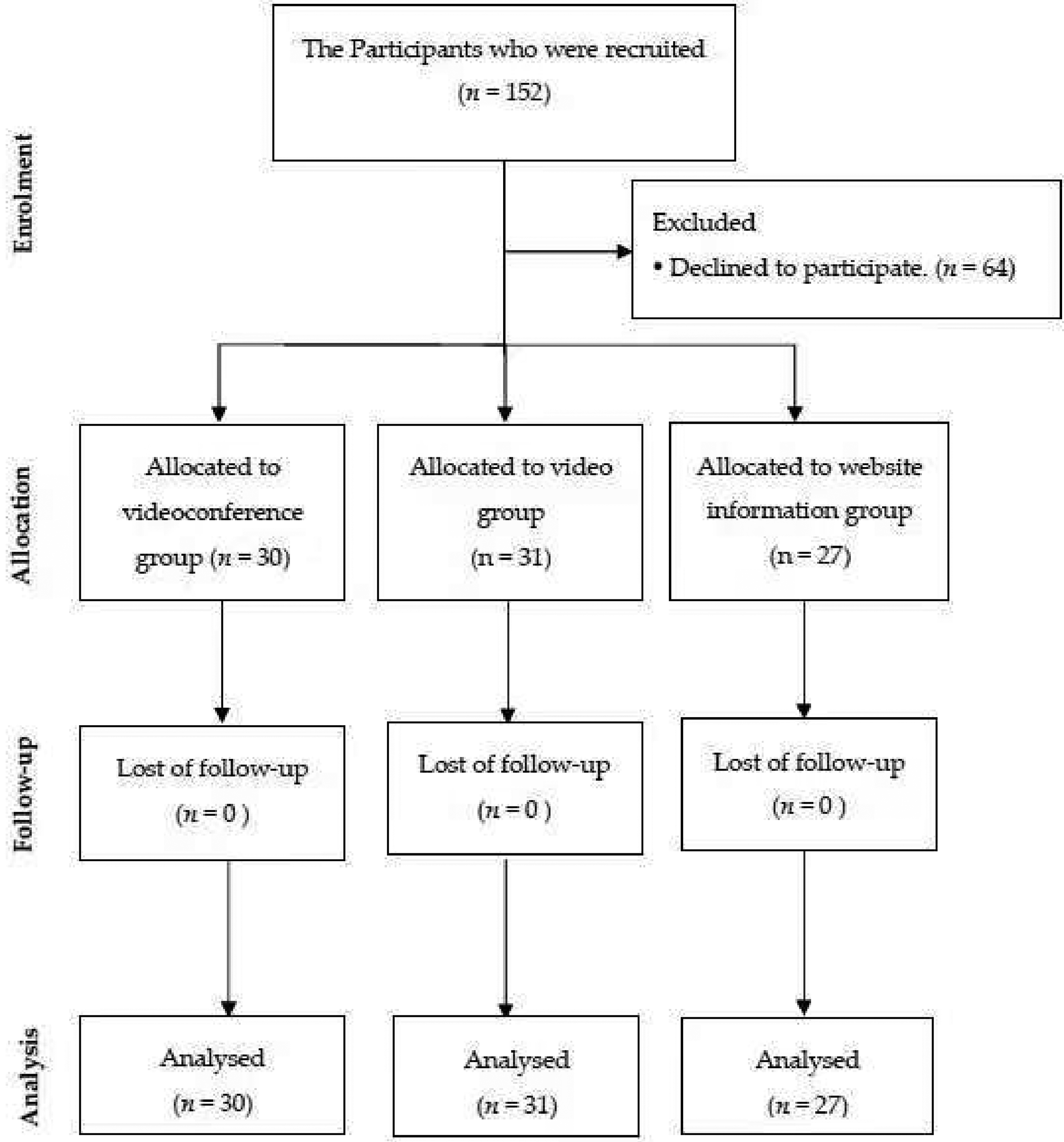
Participant allocation and flow of subjects.
Demographic Characteristics of Respondents (n = 88).

Notes. * p < .05, ** p < .01
Quantitative Results
Table 5 shows the results of the health literacy and health knowledge of the participants. After the intervention, the health knowledge of three groups of participants increased, and the mean score in different health literacy domains also improved except for Healthcare and Health promotion health literacy in the control group.
Mean and Standard Deviation of Health Literacy and Health Knowledge (n = 88).

The GEE analysis was performed to examine the effect of intervention types on the health literacy and health knowledge of the participants, which is provided in Table 6. Independent variables in GEE analyses included: group (experimental or control); time (pretest or post-test); and interaction of group and time; the dependent variable was health knowledge and health literacy. After controlling the variables of English proficiency, self-evaluation health status, and the main channel for health information, the results showed no significant change in participants’ health knowledge. Nevertheless, participants in the videoconference group were more likely to have better health promotion health literacy after the intervention compared to participants in the control group (β = 5.36, p = .02), and participants in the video group were more likely to have better general health literacy (β = 5.17, p = .01), disease prevention health literacy(β = 5.31, p = .04), health promotion health literacy(β = 5.97, p = .01) after intervention compared to participants in the control group.
Generalized Estimating Equation Analysis of Knowledge of Health Education (n = 88).

Notes. * p < .05, ** p < .01
Qualitative Results
Questions in the guide are included in Table 3. Three themes and eight subthemes were extracted after the online health literacy promotion program, including (1) difficulty in accessing healthcare: language barrier, limited knowledge, and finance issue; (2) strive for health: learn from experience and role of employers; (3) need for health education: helpful program, difficulty accessing online seminar, and prefer interaction. Table 7 provides a summary of all themes.
Summary of Themes From Focus Group Interviews.

Integration of Quantitative and Qualitative Findings
The Essential for an Online Health Literacy Promotion Program
The special background of the participants makes it difficult for them to obtain medical information and services in Macao, mainly because of language barrier, finance issue, limited knowledge, and health literacy.
The native language of Filipino domestic workers is Filipino, and English or Chinese are the main languages of communication in Macau. However, in our study, most of participants’ English and Chinese proficiency are average (60.2%) and poor (59.1%), respectively, while the available health information is often provided in Chinese and Portuguese, and most of healthcare providers are Chinese in Macao. “Especially the website, which is not very understandable… You need to ask what had be written… We also get information on T.V. My boss updates me with information from the government.” (z52–60) “At the height of COVID. My partner … died of COVID. Actually, he's not positive yet, but our heads hurt and we can't get up. I took him to the hospital. The problem is that it is difficult to communicate in the hospital because there is a language barrier.”(z1–4)
Filipino domestic helpers not only encounter language barriers in daily life, but also become more difficult when there is a need for medical services. From interviews with respondents, they also revealed that factors that may influence their health decisions include financial issues, past experience, and employer support. “They (Filipino domestic helpers) don't have money. If they get treatment here, they really need money…Their main problem is that they lack finances which is really sad.” (v30–31) “I was operated on ovarian cancer. But for my health, by the mercy of the Lord, I don't get sick here…Our food is colorful…we don't drink soft drinks and hot water only…” (z96–99) “Maybe it's too difficult for them … they are not supported by the boss…Especially those who don't get out of the boss’ house very much. They don't have enough food and enough time to exercise.” (v210–211)
Some respondents believed that the knowledge of Filipino domestic workers was limited. Of the participants in the study, 45.5% had secondary school education or less; in terms of quantitative results, the pretest score for health knowledge, and the average score of the participants was 5.06 ± 0.98, which also reflected the unsatisfactory level of health knowledge among the participants. Also, when it comes to receiving public information, especially when there is a large amount of complex information, respondents mentioned that there can be unclear situations. “To migrant workers, they are really limited in their knowledge. Not everything is conveyed what the Government wants to convey here in Macao…”(z4–6) “If you need to see a doctor because you feel something wrong, (you should) go to the doctor for help. Those who self-medicate because they don't know what their problem is and the problem they don't know how to ask for help.” (v195–197) “ I see people I know who have health problems. But they don't know how to handle it.”(v28–29)
One of the factors that influence health behaviors and decisions is health literacy, which is the skill and ability to make appropriate decisions on health-related issues from access to and use of health information. According to quantitative data from this study, general health literacy levels among Filipino domestic workers were low (27.5 ± 8.2) in pretest, with only 32% of participants having sufficient general health literacy.
The Benefits of the Online Health Literacy Promotion Program
Most respondents affirmed that this online health literacy promotion program is useful. In terms of the video group, the participants considered that the video provided a lot of health-related information and supplemented information that they did not know, such as the use of medical services and health promotion facilities, and hoped that the video could be further promoted to benefit more Filipino domestic workers. “What are the problems of Overseas Filipino workers like us, who encounter health problems, at least this video taught a lot, so they know where they can go.” (v19–21) “For me it's helpful because it's something new. About community we can easily find a way to go somewhere like hospital, healthcare, sport activities or something like that, it really helps.” (v51–53) “The description is informative and brief. So easy to understand.” (z87) “…999 to the ambulance, 911 to the police station. It will be a big help if I listen to you.”(z39–40)
While participants rated the program positively, the study also sought to understand the participants’ further opinions. Some participants said that because the program was held online, it was a difficulty for some participants who were not familiar with using online platforms. “I’m old, I'm not good at computers… We still need to learn website…” (z65–66) “She cannot set-up the videoconference. My friend cannot. When we are using and downloading it, it takes almost an hour and the internet needs to be fast.” (v295–296) “But in face to face is much better, we can ask questions directly and tutor can answer back. And we could easily ask more rather than the video, you just watching… Surely, not all people understand everything what's in the video.” (v297–301) “Not easy to organize, because not all are available. If ever they off on Sunday, they need to do something else, like go to mass and not all are interested.” (v334–335)
Discussion
The study revealed that respondents’ health literacy and health knowledge were insufficient. The results were similar to the survey conducted by Cheong et al. (2021) on this group. At the same time, unsurprisingly, respondents were facing different working and living challenges, such as limited language skills and a lack of social support. They were always in a more vulnerable state with poor determinants of health. These unsatisfactory social determinants of health are also faced by domestic workers around the world, and their health and quality of life are further affected (Choeng et al., 2020; International Labour Organization, 2013). Obviously, a health literacy promotion program was clearly beneficial to them.
Overall, videoconference group (synchronous) and video group (asynchronous) online education had slightly different learning effects on participants revealed in this study. The videoconference group has made significant progress in health promotion health literacy, while the video group has made significant progress in overall health literacy, including general health literacy, disease prevention health literacy, and health promotion health literacy. Although the content of health education in the two groups is the same, this may be related to the different learning needs of the participants. Asynchronous online interventions appeared to be beneficial for general use and cost-effective, suitable for promotion on the Internet or social media, which similar practices were also implemented in other studies; synchronous online intervention is beneficial to deepening learning and consolidating effect, it is beneficial for subjects with different learning needs (Gegenfurtner & Ebner, 2019; Vandormael et al., 2021). As a result, while both synchronous and asynchronous online education interventions had positive effects, asynchronous online education may be a more ideal way to widely promote health education because of the characteristics and working conditions of this population.
Moreover, some participants reported that they preferred the opportunity for direct interaction so that they could get an immediate understanding of what was unclear. Indeed, research on online education showed that participants tend to have more opportunities for communication and interaction, and the relevant learning effect is better (Gegenfurtner et al., 2020). So, an interactive element is desirable for the online health literacy promotion program.
Although a previous study showed that most Filipino domestic workers in Macao had smartphones and Internet access, and participants in this study also mainly received health information from relevant websites and social media, some participants in this study expressed that it was difficult in accessing the relevant applications to participate in the online seminar (Hall et al., 2018). The digital literacy of objects must be addressed when developing online education. In the planning process of this study, supported by the NGOs, a technical support station was set up at a designated location to support participants who were not able to access the program, which was an essential element of web-based intervention, a similar approach was used in other studies (Eysenbach & CONSORT-EHEALTH Group, 2011; Tao et al., 2023; van Gelder et al., 2020). Thus, it is important to note that online interventions may not be able to reach groups with low digital literacy, and the special condition of this population needs to be careful when it comes to the actual implementation of online education.
Besides, the results showed that the health knowledge of the two experimental groups did not improve significantly after the intervention, which may be related to the inadequate health literacy of the participants. It can be seen from Table 5 that the average health literacy level in the three groups was limited, whether before or after the intervention. Studies indicated that health literacy is associated with health knowledge; people with adequate health literacy are more likely to have better health knowledge and learning attitudes than those with limited health literacy (Quinlan et al., 2013; Tao et al., 2023). Therefore, there is a need for research to consider the sustainability of health literacy promotion programs for this population.
Furthermore, this study found that Filipino domestic workers in Macao had many difficulties in receiving medical services, not only limited health knowledge but also language and financial difficulties in qualitative results. Through the goal of “Health for all” by the Alma-Ata Declaration in 1978, universal health coverage is an essential right in which everyone should have access to accessible and affordable health services (World Health Organization, 2010, 2022). Some countries and organizations are concerned about the exploitation of migrant workers’ rights and have put forward guidelines on protecting living and working conditions, improving the health and safety of migrant workers (International Labour Organization, 2016; United Nations, 1990). Additionally, the result revealed that employers played an important role in this process, so it is not only medical workers and NGOs that promote the health of Filipino domestic workers in Macao, but employers should also be included in relevant action plans. Also, participants access health information mainly through the Internet, followed by healthcare personnel, as shown in this study. Thus, in addition to the Internet, health workers play a key role in providing health information to improve the health literacy of Filipino domestic workers in Macao. Although the results of this study show that the online education intervention is effective, the multicultural care competency of healthcare personnel is also an important part of promoting foreign domestic workers’ health, which deserves further discussion to create a friendly environment for foreign domestic workers in Macao.
Strengths and Limitations
This study sheds light on the health literacy needs of Filipino domestic workers in Macao and provides evidence for an online health literacy promotion program for this population. Our findings add to the existing literature on online health literacy interventions for migrant worker populations, and we highlight the importance of considering the unique learning needs and cultures of migrant worker populations when developing health education interventions. In addition, this study provides insights into the role of employers in the health decision-making process for migrant workers, which has important implications for public health practice and policy. To our best knowledge, our study is the first to provide evidence for an online health literacy promotion program for Filipino domestic workers in Macao due to research on digital health intervention for Filipino or other foreign domestic workers being scarce in the literature. The content, form, and delivery method of the intervention may be feasible for different subcultural groups. Additional research should be carried out in the future. However, its major limitations should be acknowledged. First, this was a quasi-experimental study, without randomization; hence, causal relationships between promotion program, health literacy, and knowledge could not be determined. It is necessary to conduct future experimental research to analyze the possible causal relationships between promotion program, health literacy, and knowledge in Filipino domestic workers over time. Second, the participants were limited to all female respondents associated with most domestic workers today being women; selection bias in gender could not be controlled (International Labour Organization, 2021). Third, although the number of participants in qualitative interviews was small, the main purpose of the interviews was to provide a platform for respondents to share information in their own words and to help gather detailed information and interpret quantitative results. To gain a deeper understanding of participants’ experiences, this study was done in smaller groups. Guest et al. (2016) indicated that two or three focus groups were sufficient to reach 80% saturation, including the most prevalent themes in a population by using a semistructured discussion guide. Fourth, due to the intervention being carried out synchronously and asynchronously online, the interference between groups who were not observed on-site may have resulted in bias even though the implementation of all groups independently at a specific time was as much as possible. Lastly, this study was conducted in Macao, and the health literacy promotion material was developed for Filipino domestic workers in Macao, so the health literacy promotion material may not be representative of other regions due to different healthcare policies.
Implications for Practice
The findings of this study, encompassing the developed health educational themes and contents for promoting health literacy, as well as the generated instructional materials such as videos and related resources, those can be disseminated and implemented to further enhance the awareness of health literacy among Filipino domestic workers and benefit a larger population. Furthermore, in a multicultural society, healthcare providers bear the responsibility of safeguarding public health amidst various challenges, such as language barriers and cultural differences. The outcomes of this research will serve as an exemplary model for promoting health literacy among migrant workers, while extending outreach efforts will enable individuals from diverse ethnicities and backgrounds to access opportunities for improving their understanding of health information. Consequently, this will contribute towards enhancing overall health outcomes within this specific group.
Conclusion
In conclusion, this study found that both synchronous and asynchronous online education interventions had positive effects on this population. Asynchronous online education may be more appropriate as a way of widely promoting health education due to their characteristics and working conditions. Future research should be paid to the digital literacy of the population, and interactive elements should be included in the implementation of online health literacy promotion programs.
Footnotes
Acknowledgments
Authors appreciate all cooperative organizations for supporting in this research, thank all participating Filipino domestic workers in this study. Special thanks to Caritas Macau WelAnser Centre, Progressive Labor Union Domestic Workers -Macau.
Authors’ Contributions
P-LC, HW, WC, and MIL contributed to conceptualization, methodology, project administration, and funding acquisition; P-LC and HW to data collection, P-LC and LSML to quantitative data analysis and writing—original draft preparation; P-LC, WC, and MIL to qualitative data analysis; and P-LC, HW, WC, MIL, and LSML to writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Ethical Approval and Consent to Participate
The study was approved by the Research Management & Development Department of Kiang Wu Nursing College of Macau, which is the department responsible for ethical approval (Reference no: REC-2021.1203), and all experiments in this study were conducted in accordance with the relevant guidelines.
Consent for Publication
Informed written consent for publication was obtained from all participants.
Availability of Data and Materials
All data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research: Funding of this study was provided from Macao Foundation (Reference number: 2674/DGAF/2022–01).