
Abstract
To discuss the knowledge gained and future implications for incarcerated parents and community members through the development and implementation of a standardized health education and promotion module for incarcerated mothers. A descriptive pilot study with a convenience sample of incarcerated mothers enrolled in a prison nursery program. A Midwestern women’s nursery program. The health education and promotion module was presented in a series of four group sessions. A posttest format was utilized to examine if knowledge acquisition perceived coping strategies and satisfaction with the health education and promotion module. The incarcerated mothers did acquire knowledge and were able to list coping strategies that would help them individually reduce stress while incarcerated. Also, the participants expressed interest in other health education topics.
Keywords
Introduction
The number of women incarcerated in the United States has significantly increased in the past several decades. Many of these women are of child-bearing age, and although many factors have been identified as contributing to the rate of incarceration, there is less information known about the experience of the pregnant, incarcerated woman. There are only a few U.S. prisons that allow women to keep their infants in their care while incarcerated, and little is known about the transition of these mothers from incarceration to return to expected societal norms. Although there are a few exemplar programs in the United States to help women transition, the stress of raising an infant in prison, then transitioning to the outside world can be challenging. This article reports on a pilot project designed to help incarcerated mothers learn to successfully manage the stresses of daily life and acquire coping mechanisms and feelings of self-respect and accomplishment through health education. The setting is a mother–infant prison nursery system in Ohio. Villanueva, From, and Lerner (2009) report that such programs, with adequate resources, allow for the formation of maternal or child bonds during a critical period of infant development and prevent foster care placement. Further, women who participate show lower rates of recidivism.
Background
The number of women incarcerated in the United States has increased by 832% over the past 35 years (Villanueva et al., 2009). The reasons for the increase in women inmates can be related to low socioeconomic status and drug or substance abuse (Alleyne, 2006; Hayes, 2009; van den Bergh, Gatherer, Fraser, & Moller, 2011; Zust, 2009). Incarcerated women may have a family history of substance or drug abuse that is often perpetuated by the psychological trauma of sexual or physical abuse (Borelli, Goshin, Joestl, Clark, & Byrne, 2010). Because of the lack of consistent employment, the use of fiscal resources to purchase drugs or illegal substances, the inconsistent family support, women may turn to crime such as robbery or fraud. These nonviolent crimes are committed to dull the pain of poverty, addiction, and abuse (Alleyne, 2006; Byrne, 2005; Few-Demo & Arditti, 2014).
The majority of incarcerated women are single, between the age 25 and 34 years, with minor children (Glaze & Maruschak, 2010). Five percent of these women enter prison pregnant (Maruschak, 2006), yet only a few prisons provide a mother–infant or nursery unit for the newborns. In most instances, after the delivery of the newborn, the child is sent to live with an extended family member until the mother is released from the prison system. Then the mother-inmate may face significant challenges in the transition to the community while seeking employment, establishing a safe lifestyle and parenting a child. Inmates require solid social support to maintain their families when they reenter the community but the resources to provide the services necessary to aid them and prevent recidivism are limited (Gilham, 2012).
The prison nursery concept began in the early 1900s. Many states operated prison nursery units within the correctional system for women until the 1950s when a steady decline began (Villanueva et al., 2009). The number of prison nurseries decreased due to lack of need, a decrease in financial resources, and the belief that the incarcerated woman’s family would raise the child (Cecil, McHale, Stozier, & Pietsch, 2008; Villanueva et al., 2009). With the steady increase in incarcerated women in the past 35 years, many researchers and policy makers are calling for financial and governmental support to include prison nursery units in U.S. prisons (Villanueva et al., 2009). Byrne, Goshin, and Joestl (2010) found only three countries, including the United States, that separate incarcerated women from their children rather than allow continued maternal–child interaction after birth. Currently in the United States, only nine states have prison nursery units fully operational in their prisons: California, Illinois, Indiana, Nebraska, New York, Ohio, South Dakota, Washington, and West Virginia (Villanueva et al., 2009).
The prison nursery in Ohio, established in 2001, can accommodate up to 20 mother–infant dyads and is the only one in the state as the eligible inmates are located in one centrally located state prison (“Ohio Department of Rehabilitation and Corrections,” 2013). The unit is arranged as a large barrack with partitions approximately 9 feet tall; the open ceiling space allows correctional personnel to hear problems happening within the unit. The unit has two office areas for administrative personnel and the unit case manager; the lavatory and kitchen are across from the office space with a large entrance area. On the right are the incarcerated mother–child rooms which can accommodate two mother–infant dyads. The rooms contain two beds, two cribs, and two foot lockers and are usually decorated in bright colors with nursery-style decals on the walls. On the left side is a large communal area with an abundance of toys, swings, layettes, books, a television, and videos for adults and children and a quiet room with a rocker chair and more books for a mother to spend time alone with her child. This room has a large glass window so the mother and infant can be observed. The unit also has a nanny room for the inmate who has been approved as the alternative caregiver for the children when the incarcerated mothers are out of the unit, for dinner, work or education training, or visiting the medical clinic. An outdoor play area with picnic tables and a walking path surrounded by a large fence allows the mothers and children to enjoy fresh air and exercise together when possible.
Historically, the unit census has been between 12 and 18 mother–infant dyads. Recent legislative changes have resulted in reassigning prisoners to community programs based on the level of severity of their offense. The numbers in the unit began to fall over an 18-month period to an average of two to six dyads in the unit.
Review of Literature
Becoming a parent can have a positive effect on the incarcerated mother, giving her a sense of purpose or a valid reason to remain out of prison. Cecil et al. (2008) found that incarcerated mothers are highly motivated to be good parents to their children. Yet, the need to maintain one’s physical energy when caring for a child can add to the emotional stress of parenting (Cooklin, Giallo, & Rose, 2012). Parenting for the general nonincarcerated population is stressful especially as children experience different stages of development (Cappa, Begle, Conger, Dumas, & Conger, 2011). The incarcerated mother faces many other stressors as well. Many of the mother-inmates have older children being cared for by family members, intimate partners, or the foster care system, and this separation can cause increased stress even if they are in a prison nursery unit with their youngest child (Byrne, Goshin, & Blanchard-Lewis, 2012; Freitas, Inacio, & Saavedra, 2016; Rose & LeBel, 2016). The stress can affect the maternal-child bond, child developmental outcomes, and the mother’s physical and emotional health (Arditti, 2014; Byrne et al., 2012; Goshin, Byrne, & Blanchard-Lewis, 2014). The incarcerated mothers may experience an increase in depressive symptoms as a result of confinement. These symptoms could be increased as a result of several preincarcerated factors from lower economic status, drug abuse, single parenting, to serial broken or traumatic family relationships (Few-Demo & Arditti, 2014; Friestad, 2016; Rose & LeBel, 2016). Depression may be a result of social isolation and a rigid routine with unstructured free time that does not provide intellectual stimulating thoughts or actions (Borelli et al., 2010; Goshin, Byrne, & Henninger, 2013).
Knowledge about stress and coping and developing appropriate skills is important for all new parents who face multiple stressors including financial, time management, personal or child health concerns, child-rearing concerns, and adapting to a new role (Cappa et al., 2011; Raphael, Zhang, Lui, & Giaridon, 2009; Solem, Christopherson, & Marinussen, 2011). Furthermore, Shelton and Wakai (2015) discuss that the inmate’s ability to cope with prison often determines the inmate’s functioning and health needs in the future. This point illustrates that coping and stress reduction skills may be beneficial to both the family’s health as well as decreasing the mother’s risk for recidivism. The incarcerated mother armed with coping skills may be able to successfully navigate this transition and improve her competency as a parent (Byrne et al., 2010; van den Bergh et al., 2011). Most importantly, Goshin et al. (2014) report that “women released from a prison nursery have a low likelihood of recidivism within 3 years of release” (p. 113). This is significant when considering that 47% of women released from the general prison population during one 8-year study were reincarcerated within the first few years (Huebner, DeJong, & Cobbina, 2010).
Stress for the incarcerated mother often persists during the transition period after her release to the home community. Hayes (2009) describes the incarcerated mother’s reentry to home as extremely happy and almost a honeymoon, before reality sets in with the stresses of parenting and maintaining a home. The transition to the outside community can be even more challenging when adding the emotional stress of parenting a child whose routine the mother may not have had the opportunity to become familiar with (Cooklin et al., 2012). The stress of parenting during the transition process to the outside world can actually increase substance abuse, leading women back to prison (Hayes, 2009). The incarcerated mother armed with coping skills may be able to successfully navigate this transition and improve her competency as a parent (Byrne et al., 2010).
Several programs have been described in the literature to help decrease the mother’s stress and increase her coping skills. Whitehead (2006) discussed the health promoting prison to encourage continuity of care for prisoners during and after incarceration and to include health promotion and prevention interventions. Whitehead calls for a formal standardized plan of action for health promoting clinics within prisons in New Zealand and for parenting training that begins in prison and continues into the community for former prisoners and their children. In the United States, Stephan (2008) notes that both federal and state correctional facilities offer a variety of programs that assist inmates with social, physical, emotional, and economic problems. Topics include counseling, life skills or community adjustment, drug or alcohol dependency, employment, psychological or psychiatric, HIV or AIDS, parenting, and sex offender. In the publication Educational Programs Available to Incarcerated Populations in Federal and State Facilities, Stephan notes that Ohio has been offering more educational programs for inmates compared with the national average. However, details about course content and the impact of the courses on participant satisfaction, knowledge, or behavior are not available. Specific programs related to parenting skills and the transition to the outside community are not described in the literature.
In one Ohio designated mother–infant prison nursery unit, health promotion and education teaching are offered to the incarcerated mothers. However as a result of budget constraints, health and parenting programs were presented inconsistently due to reliance on community volunteers. Little education was focused on stress and coping strategies for the incarcerated mother.
Methods
The health education and promotion module (HEP-Mod) program was developed to impact the incarcerated mother’s knowledge acquisition and coping skills using Pender’s theory of health promotion (Pender, Murdaugh, & Parsons, 2011). Factors such as perceived barriers to the benefits of health promotion education activities were considered through open discussion with the administrative staff of the mother–infant unit and with an agency offering infant development education to the mothers. Despite consideration of several topics to be included such as healthy family meals on a budget, sexually transmitted infection awareness and prevention, and exercise for health and family fun, the consensus from community experts was that stress reduction and coping would be most helpful. It was thought that stress reduction and coping could serve as an umbrella, incorporating aspects of other relevant topics.
Design and Sample
Design
The descriptive pilot study included a convenience sample of incarcerated mothers in a mother–infant unit in a selected Ohio prison who participated in an educational module that included a pretest and posttest as well as other questionnaires to gather demographic and content knowledge on the educational module’s topic(s). The education module was presented in a total of four 1-hr sessions over a 4-week period of time.
Sample and Protection of Human Subjects
The pilot project was approved by the University’s institutional review board and the State’s department of rehabilitation and corrections institutional review board for protection of human subjects prior to the implementation of the pilot project. Each participant voluntarily signed a written consent before the first education session. Participants were assured that their participation was strictly voluntary, and no penalties would be associated with nonparticipation.
The convenience sample was recruited through individual discussion of the research project with six incarcerated mothers. Inclusion criteria included the following:
Must be 18 years old or older; Must be pregnant at the time of incarceration; Must be due to deliver during incarceration; Must have a nonviolent criminal background; Must not have committed a crime against children; Must have security status of minimum or medium; Must have no more than 18 months left on her sentence after she delivers; Must be the legal custodian of the child; and Along with the infant, must meet predetermined medical and mental health criteria governed by the Midwestern State’s department of rehabilitation and corrections (“Ohio Department of Rehabilitation and Corrections,” 2013).
Additional project criteria included the following:
Willingness to participate in the health education program and evaluation.
Each participant was assigned a number in the order of recruitment. An envelope with this number was given to each participant for their completed instruments. The data were not reviewed until after the four sessions were completed in an effort to eliminate researcher bias.
Educational Modules
Teaching Plan.

The modules were developed to occur over a period of time, as the literature supports teaching content over several sessions to reinforce knowledge acquisition (Baier, 2013; D’Amico & Barbarito, 2012; Davis et al., 2008; Lawson, 2011; Segal et al., 2012). The repeated practice of stress reduction techniques and the use of “yoga for stress relief” videos provided the participants an opportunity to practice individually or as a group and at various times throughout the day. Pender et al. (2011) state that changes over time and in small increments with feedback from participants can increase resistance to stress. Thus, it was thought that providing health education and encouraging participants to practice coping skill strategies such as yoga would enable the incarcerated mothers to demonstrate a greater ability to cope when faced with stressful situations.
Each group was offered the educational modules for 1-hr sessions twice weekly for 2 weeks which maximized the cohort’s subject count. Each session had two to four participants. Only subjects who completed all four sessions were included in the results.
Instruments
Three survey questionnaires were developed by the research team. Content validity of the survey instruments was confirmed by review by the expert panel and reviewed for readability. Four content experts (1 PhD prepared; 2 duel PhD and DNP prepared; 1 BA prepared Certified Pediatric Nurse Practitioner with 30 years clinical expertise) reviewed each instrument resulting in content validity index of 1.0 for each individual instrument. According to Polit and Beck (2006), a Content Validity Index (CVI) of 1.0 is sufficient for assuring content validity when three to five experts review each item of an instrument. The instruments included a (a) demographic information survey, (b) current health education satisfaction survey, and (c) personal knowledge survey. The demographic information survey was the instrument used to collect descriptive data about study participants. The current health education satisfaction survey was an instrument that collects data about recent health education experiences that the mother-inmate attended during incarceration prior to the intervention. The personal knowledge survey was used as a posttest to evaluate the knowledge of the mother-inmate after completion of the HEP-Mod program.
Results
Two of the mother–infant dyads were released from the prison prior to the beginning of the pilot project. A total of three mothers and one nanny participated in the project. The nanny was an inmate who served as a support person for the mothers. The unit manager requested that the nanny be included in the educational sessions since she could reinforce the session content on a daily basis. The nanny was not included in the results since she was not a mother with an infant on the unit.
Demographical Information of Study Participants (N = 3).
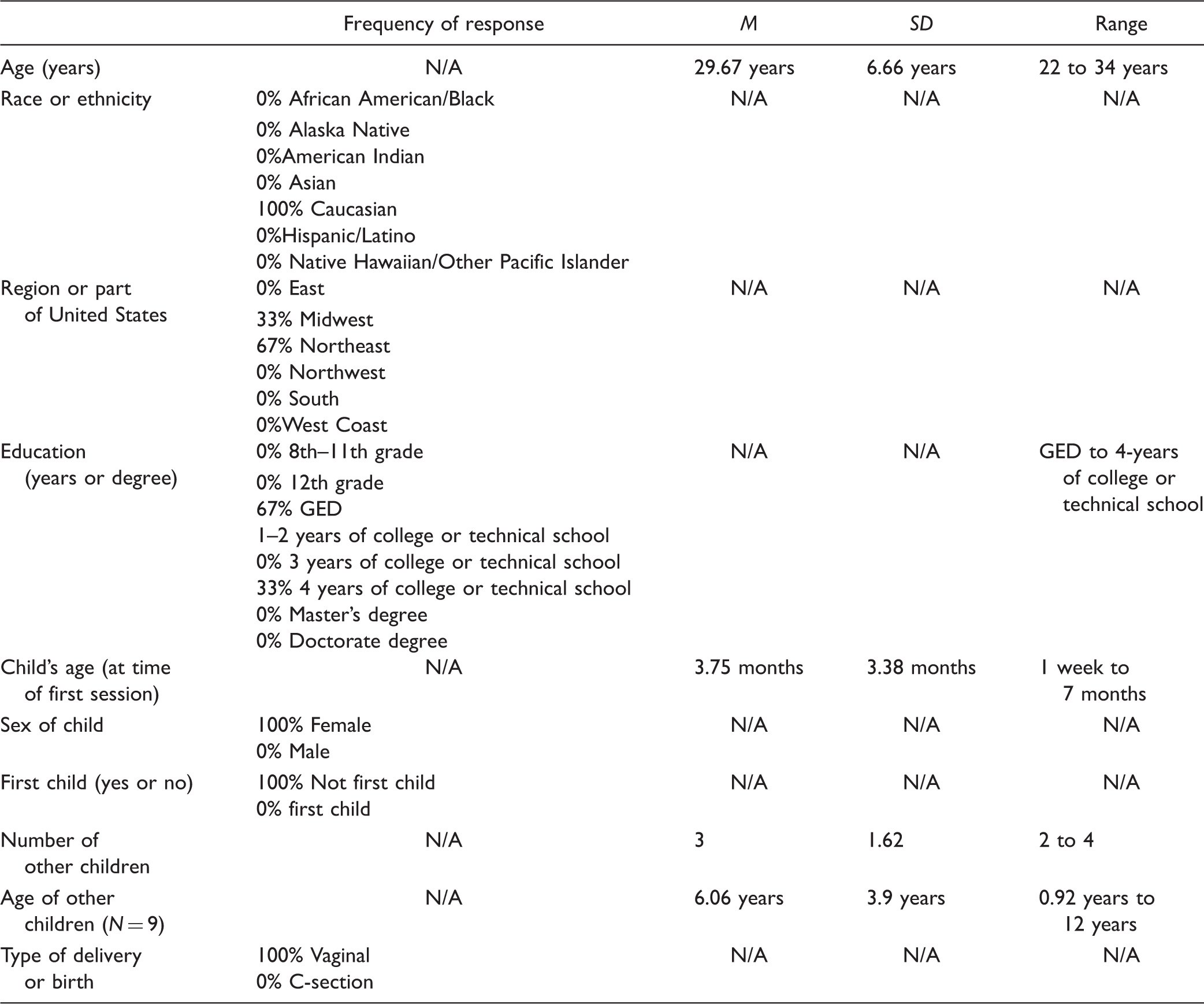
GED = general education development.
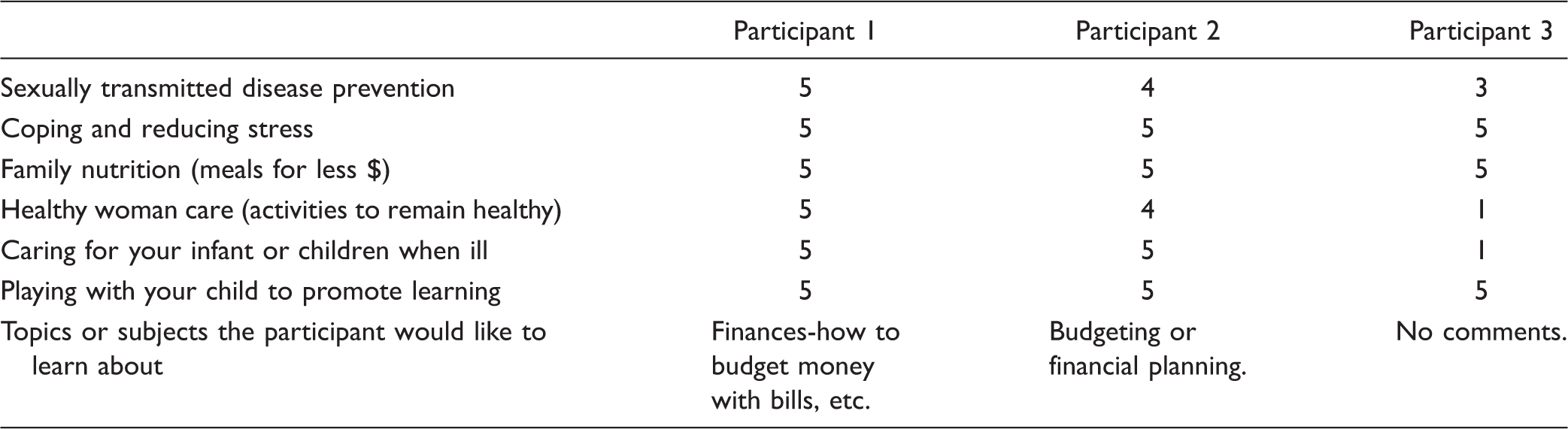
Health and Wellness Education Survey: Likelihood of Attending Health Education Classes on Selected Topics (Ranking 0–5 Likert Scale With 0 = Not Likely and 5 = Very Likely).
Personal Knowledge Survey—Posttest: Topic: Coping and Stress Reduction.

Common Topics of Discussion During Teaching Sessions.

The HEP-Mod educational program with its focus on stress reduction and coping strategies could be a valuable resource for the mother–child dyad transitioning to the community outside of prison. Through offering standardized health education classes, mothers may be able to acquire knowledge that could support successful transition into the community and decrease recidivism as supported by the literature (Byrne et al., 2010; Shelton & Wakai, 2015; van den Bergh et al., 2011). As women who may have been part of the prison nursery programs, feasibility of the HEP-Mod classes in a community setting should be explored as well.
Although the HEP-Mod program focused on stress reduction and coping strategies, additional comprehensive standardized health education strategies may be useful for the incarcerated mother transitioning to the outside community. This model may also be helpful in community-based parent education programs. With standardization of the health education modules, more interdisciplinary health-care professionals may be willing to volunteer their time in the prison setting to promote a positive transition. Data related to reduced rates of recidivism related to participation in the standardized education modules may encourage policy makers and community leaders to continue to support the prison nursery program.
Cronbach’s alpha coefficient was not calculated due to small sample size and designation of pilot study. Future research will attempt to ensure a large enough sample size in order to complete reliability statistical testing.
Limitations
The small number of participants in this pilot project limits the generalizability of the findings; however, the participants’ comments related to future educational programs provide a direction for future projects. Replication of the HEP-Mod health promotion project should be undertaken at other prison nursery units with larger numbers of participants, and over an extended period of time to determine the validity of these preliminary findings. Finally, a longitudinal analysis on the impact of these standardized education programs related to transitions of the mother–infant dyads into the community and the rate of recidivism should be undertaken.
Conclusion
Through the process of conducting the HEP-Mod on stress reduction and coping in a prison nursery, a new understanding of some of the issues facing incarcerated mothers has emerged. This new knowledge may lead to new solutions and encourage other health-care professionals to become involved either as community servants or through research. Research findings, as well as increased volunteering by professionals, may lead policy makers in Ohio to continue the valuable prison nursery program and expand health education and promotion programs into community corrections.
The knowledge that the prison nursery mothers acquired is a beginning. Newman, Fowler, and Cashin (2011) state that incarceration “provides an opportunity to enhance parenting competence and through parenting education and support reduce parent and child distress” (p. 9). Health education may give incarcerated mothers the tools to remain healthy and to promote a healthy family, but further research is needed. The commitment to continue researching the experience of the prison nursery mother and the effects on her behavior as a parent and a healthy woman is ongoing. Although, many challenges are expected, the potential benefits for promoting strong healthy mother–infant families are worth the work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author was a participant in the NLN Scholarly Writing Retreat 2014, sponsored by the NLN Foundation for Education and PocketNurse.