
Abstract
Background
Nonpharmacological pain control strategies combine numerous strategies that contain nondrug measures for pain remedies for sufferers.
Objective
To assess the practice of nonpharmacological pain control strategies among nurses working in public hospitals of West Arsi zone, Ethiopia, 2022.
Methods
An institutional-based cross-sectional study design was employed from April 15 to May 30, 2022. The total sample size was 422 and a simple random sampling technique was used. Data were entered using Epi-information 4.6 version and analyzed using SPSS version 25. Multicollinearity was checked by considering the variance inflation factor and tolerance. The goodness of fit test was done using the Hosmer-Lemeshow goodness of fit check. Binary logistic regression analysis was done and variables with a p-value of < 0.25 within the bivariable analysis were taken into the multivariable analysis. Statistical significance was declared at a p-value of < 0.05 with an adjusted odds ratio (AOR) and 95% confidence interval (CI).
Result
The practice of nonpharmacological pain control strategies was 53.8% (95% CI: 48.9–58.7). Age of 30–39 years old (AOR: 2.28, 95% CI: 1.34–3.86), educational status bachelor's degree (AOR: 2.25, 95% CI: 1.47–4.45), marital status married (AOR: 0.46, 95% CI: 0.28–0.73), and having training (AOR: 1.98, 95% CI: 1.23–3.17) were found to be significantly associated with practice of nonpharmacological pain control strategies.
Conclusion
About five in 10 nurses working in West Arsi zone public hospitals had good practice of nonpharmacological pain control strategies. Age, educational status, marital status, and training were found to be significantly associated with practice. Therefore, improving the educational status of nurses through various opportunities such as continued professional development and regular updating, and training nurses about methods may increase the nurses’ practice toward nonpharmacological pain control strategies.
Introduction
Pain is an unpleasant sensory emotional experience and it causes potential damage (Kahsay, 2019; Raja et al., 2020). The clinical manifestation of pain is a highly subjective and deeply personal experience (Osama, 2018; Kahsay, 2019). Pain management is an important aspect of patient care and nurses play a crucial role in providing pain assessment and treatment (Huang et al., 2013; Kahsay, 2019; Raja et al., 2020). Effect pain management improves outcomes and increases patient satisfaction (Zeb et al., 2018). On the other hand, ineffective pain management leads to a marked decrease in desirable clinical and psychological outcomes and patients’ overall quality of life (Cornett et al., 2018; Kahsay, 2019).
Nonpharmacological pain control strategies (NPPCS) are a combination of different approaches that involve nondrug measures to relieve pain such as exercise, deep breathing, positioning, ambulating, and music therapy (Ali, 2015; Ung et al., 2016). It reduces potential risks like drug dependency, respiratory depression, vital organ damage, and high costs of drugs (Christian & Centre 2014; Karabulut, 2016). The good practice of nurses is to take corrective action in pain control and improve outcomes (Ou et al., 2020).
Globally, millions of people suffer from pain in hospitals, in their homes, or in assisted living facilities. About 20% of adults are estimated to suffer from pain worldwide and 10% are diagnosed with chronic pain each year (Goldberg & McGee, 2011). In Africa, the prevalence of pain is 87.5% in palliative care and it has a devastating effect on the socioeconomic system (Huang et al., 2013).
Literature Review
Literature indicates that 90% of hospitals have no documented evidence of NPPCS use. The nonpharmacological control of pain and its documentation evidence in Ethiopian university hospitals are inadequate (Woldehaimanot et al., 2014) even though both academic and clinical nurses caring in these hospitals. Thus, the problem is related to the nurses’ practice of NPPCS in the health facility setting. Therefore, this study assessed the practice of NPPCS among nurses working in public hospitals of the West Arsi zone.
Methods and Materials
Study Area and Period
The study was done in public hospitals of the West Arsi zone, Oromia region, Ethiopia. There are seven public hospitals in the zone. These are Shashamene Specialized Hospital, Melka Oda General Hospital, Dodola General Hospital, Loke General Hospital, Gambo General Hospital, Arsi Negele primary Hospital, and Kokosa primary Hospital. The zone was located in the Eastern part of the Oromia region at 235 km from Addis Ababa, the capital of Ethiopia. The study was conducted from April 15 to May 30, 2022.
Eligibility Criteria
Nurses working at public hospitals in the West Arsi zone during the study period were included. However, nurses on maternity and annual leave, nurses working for <6 months, and those critically ill during the data collection period were excluded.
Sample Size Determination
The sample size was determined using a single population formula. The assumptions of a 95% confidence interval, 5% margin of error, and a proportion of 51.2% are as follows:

Sampling Procedure
All seven hospitals in the West Arsi zone were included in the study. Then, the total number of nurses in each hospital were determined, 103 nurses in Shashamane Specialized Hospital, 104 nurses in Melka Oda General Hospital, 68 nurses in Dodola General Hospital, 55 nurses in Gambo General Rural Hospital, 60 nurses in Loke general hospital, 43 nurses in Arsi Nagele primary hospital, and 38 nurses working in Kokosa Primary Hospital. The total number of nurses working in all hospitals was 471. Secondly, the proportional allocation was used to determine the required number of nurses from each hospital. Finally, a simple random sampling technique was used to select nurses by taking the registration from the human resource management of the respective hospitals as a sampling frame (Figure 1).

Ischemic presentation of sampling procedure of selecting nurses working in public hospitals of West Arsi zone, Ethiopia, 2022.
Study Variables
Independent Variables
Operational Definition
Data Collection Tool and Procedure
The data was collected using structured, pretested, and self-administered questions. The tool was adapted by reviewing related kinds of literature (Ali et al., 2013; Kheshti et al., 2016; Kidanemariam et al., 2020). Seven bachelor's degree pharmacy technicians and four master's degree holder public health officers were recruited for data collection and supervision, respectively. The data collection was carried out by self-administering the questionnaire for the selected nurses in their work settings.
Data Quality Assurance
The tool was prepared in English version. A 2-day training was given for data collectors and supervisors. A pretest was conducted on 5% (21 nurses) of sample size at Bokoji General Hospital a week before the start of the study. Based on the pretest result, the necessary modification was made. The Cronbach’s Alpha reliability test was done and it was 0.782. Continued follow up and supervision were done by supervisors and researchers throughout the data collection period. All filled questionnaires were reviewed for completeness and cleared before data entry.
Statistical Analysis
Data were entered using the Epi-data version 4.6 and analyzed using SPSS version 25. Multicollinearity was checked by considering the variance inflation factor (VIF > 10) and tolerance <0.05. The goodness of health take a look at was done using of the Hosmer-Lemeshow goodness of fit test. Binary logistic regression analysis was done, and variables with a p-value < 0.25 in the bivariable analysis were taken into the multivariable analysis. Statistical significance was declared at a p-value < 0.05 with an adjusted odds ratio (AOR) and 95% confidence interval (CI).
Result
Sociodemographic Characteristics of Nurses
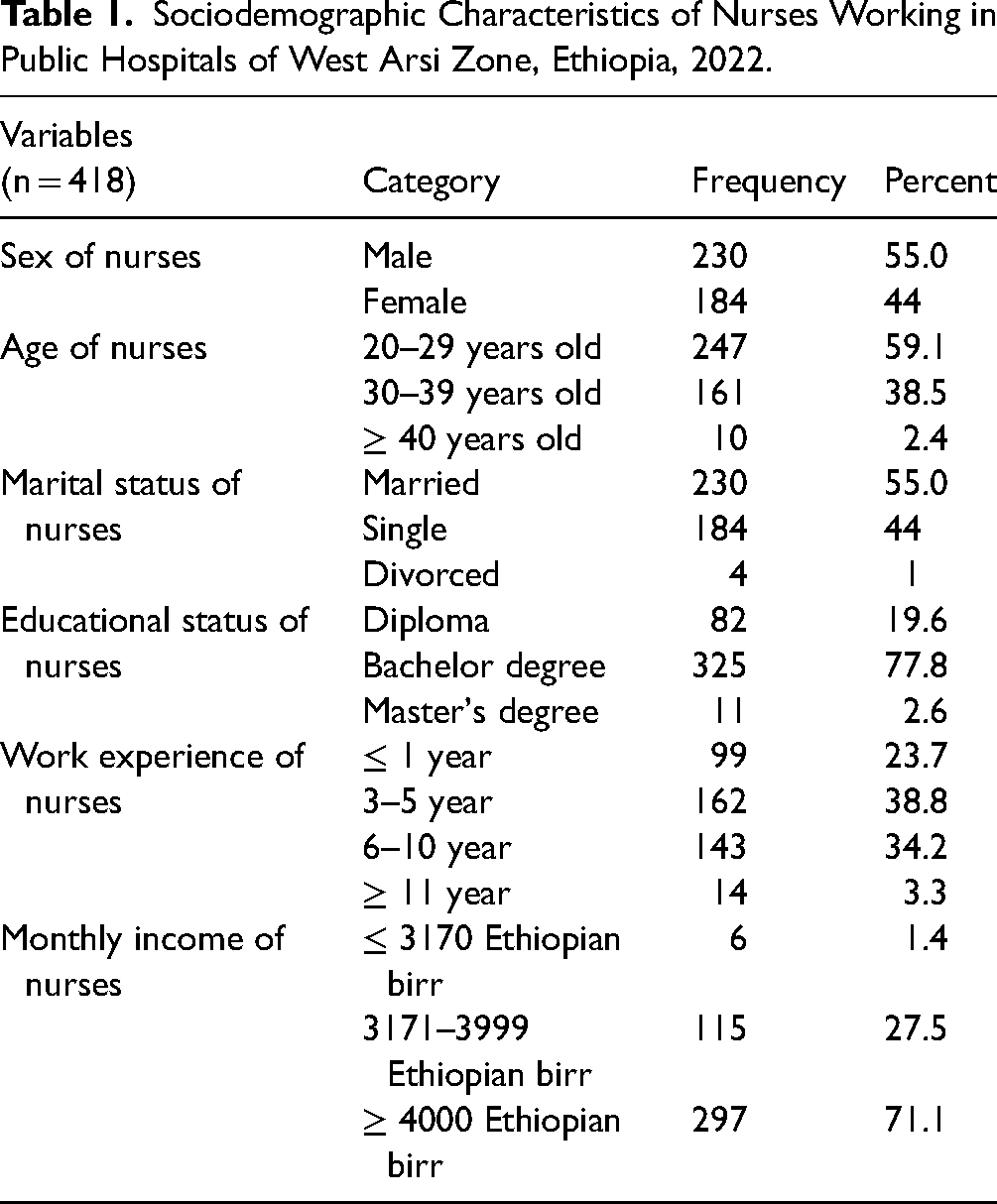
Four hundred eighteen nurses gave responses that made the overall response price 99%. More than half, 245 (58.6%) have been male and 247 (59.1%) have been inside the age group of 20–29 years. Of the nurses, 230 (55.0%) had been married and 325 (77.8%) were bachelor diploma holders. The work revealed that 162 (38.8%) nurses were 35 years and the month-to-month income of 297 (71.1%) nurses was ≥4000 Ethiopian birr (Table 1).
Sociodemographic Characteristics of Nurses Working in Public Hospitals of West Arsi Zone, Ethiopia, 2022.
Healthcare System-Related Factors
Out of 418 respondents, 244 (58.4%) mentioned that a heavy workload is a barrier to NPPCS. However, 40 (9.6%) stated loss of administrative support was a barrier to NPPCS. Less than half, 98 (23.4%) suggested a lack of resources, and 135 (32.3%) suggested a loss of pain control coverage as a barrier to NPPCS (Table 2).
Healthcare System-Related Factors of NPPCS of Nurses Working in Public Hospitals of West Arsi Zone, Ethiopia, 2022.

NPPCS=nonpharmacological pain control strategies.
Nurses-Related Factors
Of 418 nurses, 136 (32.5%) suggested a loss of experience in using NPPCS, and 81(17.4%) pronounced that the belief of nurses’ number one venture is to administer pain medicinal drugs. Less than half, 29 (30.9%) nurses said a history of training is a barrier for NPPCS (Table 3).
Nurses-Related Factors for the Practice of NPPCS Among Nurses Running in Public Hospitals of West Arsi Zone, Ethiopia, 2022.
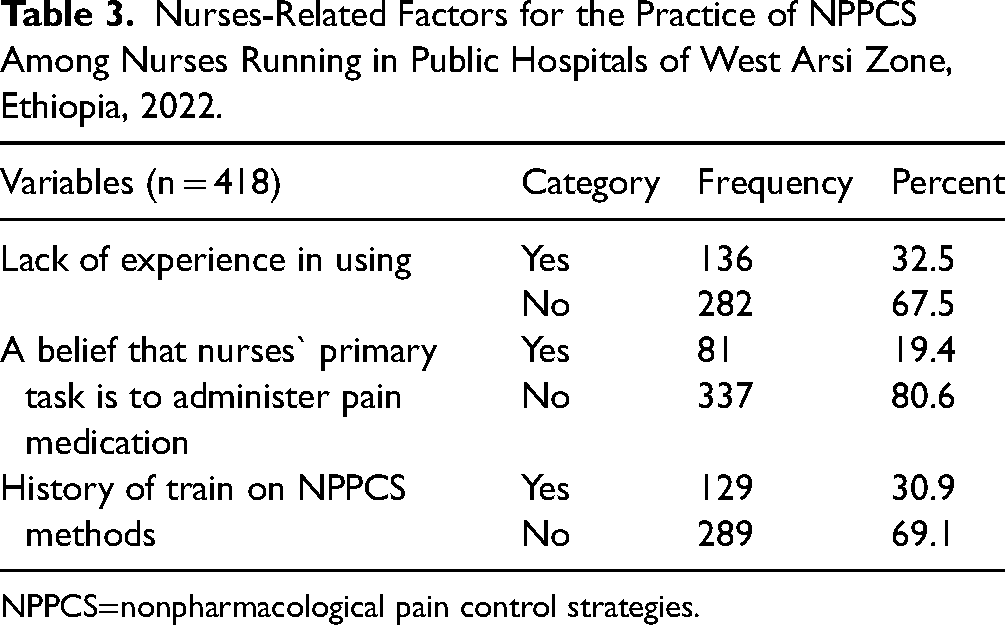
NPPCS=nonpharmacological pain control strategies.
Patient-Related Factors
Much less than half, 156(37.3%) suggested that loss of affected person cognizance. But, 262 (62.7%) reported affected person focus. Similarly, 185 (44.3%) stated patient unwillingness. On the other hand, 233 (55.7%) mentioned willingness. Regarding patients’ robust ideals in capsules, 204 (48.8%) suggested patients’ sturdy beliefs in drugs as limitations to NPPCS. However, 214 (51.2%) patients do not believe as a barrier.
Knowledge of Nurses Toward NPPCS
Of the 418 nurses, 66.7% had good knowledge and 33.3% had poor knowledge of NPPCS (Figure 2).

Nurses’ knowledge of NPPCS among nurses working in public hospitals of West Arsi zone, Ethiopia, 2022. NPPCS=nonpharmacological pain control strategies.
Practice of NPPCS Among Nurses
Of the full 418 nurses, 53.8% had good practice, but 46.2% had poor practices of NPPCS (Figure 3).
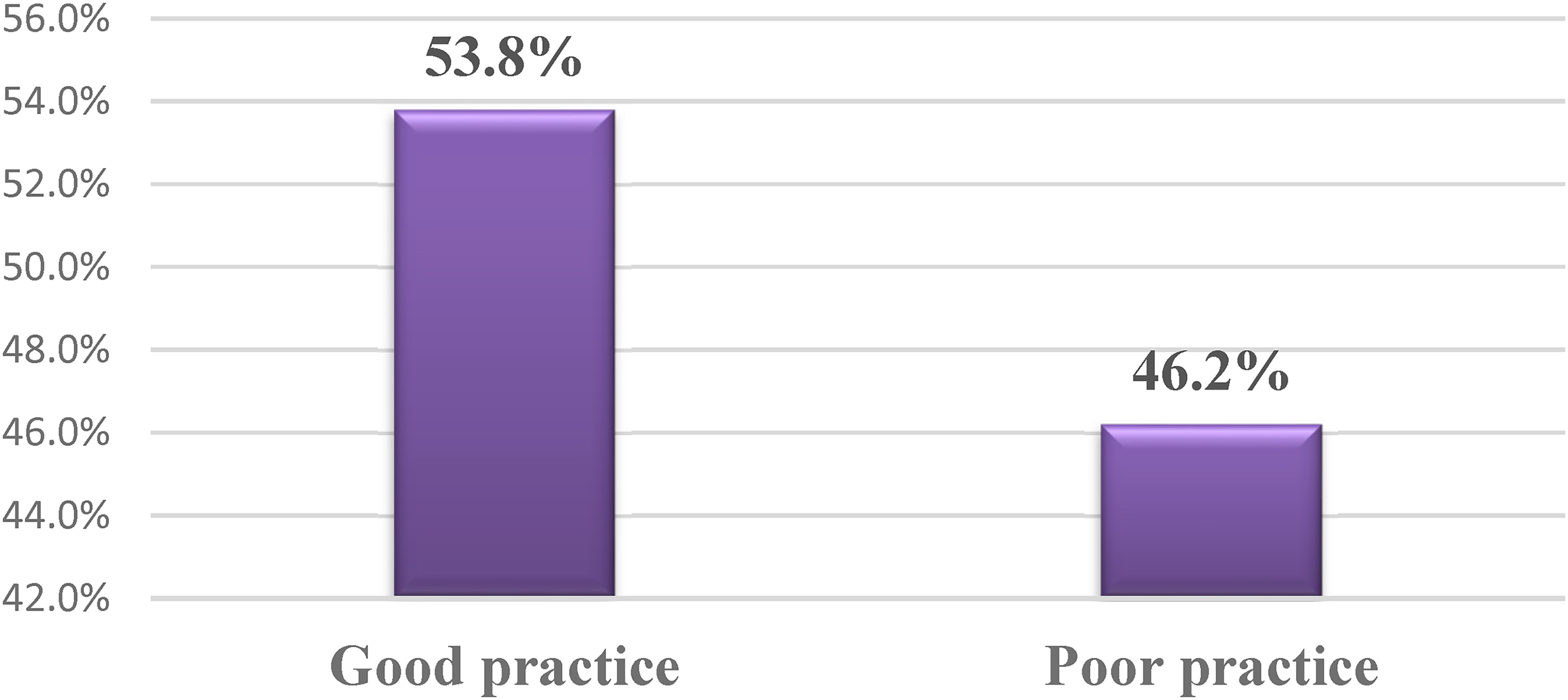
Practice of NPPCS among nurses working in public hospitals of West Arsi zone, Ethiopia, 2022. NPPCS=nonpharmacological pain control strategies.
Factors Associated With the Practice of NPPCS
In bivariable logistic regression, age, educational popularity, work revel, lack of pain control coverage, and training were related to the exercise of NPPCS strategies. While, in multivariable analysis, age of 30–39 years (AOR: 2.28, 95% CI: 1.34–3.86), educational status bachelor’s degree (AOR: 2.25, 95% CI: 1.47–4.45), marital status married (AOR: 0.46, 95% CI: 0.28–0.73), and having training (AOR: 1.98, 95% CI: 1.23–3.17) have been discovered to be drastically related to practice of NPPCS (Table 4).
Factors associated with nurses practice of nonpharmacological pain control strategies among nurses working in public hospitals of West Arsi zone, Ethiopia, 2022.

*Significant at a p-value <0.05, “1”: reference group.
AOR=adjusted odds ratio; CI=confidence interval; COR=crude odds ratio; NPPCS=nonpharmacological pain control strategies.
Discussion
The level of exercise toward NPPCS becomes 53.8% (95% CI: 48.9–58.7). It was higher than a study executed in Egypt at 32.7% (Mohamed et al., 2021), and Debre Tabor Comprehensives specialized health facility at 26% (Zeleke et al., 2021). This difference is probably due to differences in sample size, the sociocultural history of nurses, the international locations’ coverage and motivation to enforce NPPCS, and the nurses’ openness to practice NPPCS.
This study revealed that age was significantly related to the exercise of NPPCS. Nurses aged 30–39 years have been 2.28 times more likely to have suitable practice as compared to nurses aged 20–29 years old. It was just like another research achieved in Singapore and the United States (Becker et al., 2017), and Eritrea (Kidanemariam et al., 2020) that said the nurses’ age had results on the practice of NPPCS. This is probably because as age increases they may be greater eager to exercise those strategies, professionally boost their capacity, interpret threat-gain evaluation, and exercise holistically in their lifetime.
In this look, educational status changed substantially related to the exercise of NPPCS. Bachelor’s degree nurses are 2.55 instances more likely to have exact practice as compared to diploma nurses. This was supported using research completed within the United States (Becker et al., 2017), Singapore, Cairo (Badr et al., 2015), and Eretria (Kidanemariam et al., 2020). The possible rationalization might be nurses with higher academic stages had an opportunity to refer to distinct books and get up-to-date data and they modified these to exercise their paintings.
Marital status became considerably related to the exercise of NPPCS. Married nurses were 54% less likely to have practice compared to divorced nurses. This might be related with that married nurse have diverse familial and social obligations that would make them busy and decrease their time for working toward NPPCS.
In this study, the training change into determined to be tremendous in the practice of NPPCS. The nurses who have a history of education in NPPCS have been 1.98 times more likely to have desirable practice in comparison to nurses who did not train. This turned into just like studies carried out in Saudi Arabia (Ali et al., 2013), Turkey (Tercan, 2017), and Debre Tabor complete clinic (Zeleke et al., 2021). This may be due to trained nurses with updated records approximately NPPCS that ought to help them exercise the NPPCS of their work.
Limitations of the Study
The observer is probably liable to subjectivity and recall bias.
Implications for Practice
As it's far recognized, pain is an unpleasant sensory enjoyment and its medical manifestation is subjective, the use of a mixture of individualized NPPCS technique procedures relieves it. Almost, the NPPCS minimize capacity dangers like drug dependency, respiratory depression, essential organ harm, and high charges for tablets. On this, the practice of nurses are crucial and a clue to expand techniques and enforce them in exercise.
Conclusion
About five in 10 nurses working in West Arsi zone public hospitals had good practice of NPPCS. Age, academic reputation, marital reputation, and training were considerably associated with practice. Therefore, enhancing the educational reputation of nurses through various opportunities which include persistent professional improvement and regular updating, and schooling nurses about techniques may boost the nurses’ practice of NPPCS.
Footnotes
Acknowledegment
We would want to thank the study participants for the scarification of their valuable time spent filling out questionnaires.
Authors’ Contribution
All authors have made substantial contributions to the work. Participated in the conception, design, and acquisition, conducted the data analysis and interpretation; took part in drafting, revising, and critically reviewing the article. All authors gave final approval of the version to be published and all authors have agreed on the journal to which the article has been submitted; agreed to be personally accountable for all aspects of the work.
Availability of Data
The data used for this study are available from corresponding authors on secured and reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hawassa University (grant number IRB/115/13).
Ethical Consideration
Ethical clearance was obtained from Hawassa University College of medicine and health science, institutional review board and a formal letter of cooperation to conduct this research was written to West Arsi zone public hospitals.
Informed consent
Written informed consent was obtained from each participant nurses, and the information obtained from them would not have been disclosed. Coding was used to eliminate names and other personal identification of respondents to ensure anonymity, privacy, and confidentiality. Thoroughly, our research passed required the principles of the declaration of the Helsinki General Assembly, Seoul, Korea, and October 2008.