
Abstract
Introduction
Many people, often older adults, living in long-term care homes (OA-LTCH) became socially isolated during the COVID-19 pandemic due to variable restrictions on in-person visits and challenges associated with using technology for social connectivity. Health providers were key to supporting these OA by providing additional care and facilitating their connections with family using technology such as smartphones and iPads. It is important to learn from these experiences to move forwards from the COVID-19 pandemic with evidence-informed strategies that will better position health providers to foster social engagement for OA-LTCH across a range of contextual situations.
Objective
This exploratory qualitative description study sought to explore health provider experiences in supporting social connectedness between family members and OA-LTCH within the COVID-19 context.
Methods
Qualitative, in-depth semistructured interviews were conducted with 11 health providers.
Results
Using inductive qualitative content analysis study findings were represented by the following themes: (a) changes in provider roles and responsibilities while challenging for health providers did not impact their commitment to supporting OA-LTCH social and emotional health, (b) a predominant focus on OA-LTCH physical well-being with resultant neglect for emotional well-being resulted in collective trauma, and (c) health providers faced multiple challenges in using technology to support social connectivity.
Conclusion
Study findings suggest the need for increased funding for LTC to support activities and initiatives that promote the well-being of health providers and OA living in LTC, the need to prioritize social well-being during outbreak contexts, and more formalized approaches to guide the appropriate use of technology within LTC.
Introduction/Background
Throughout the COVID-19 pandemic, older adults (OA) experienced high morbidity, extensive mortality and lasting impacts on their health and well-being (López et al., 2020; Wong et al., 2022; Yanez et al., 2020). While all OA were impacted by COVID-19, those living in long-term care home (LTCH) in Canada experienced some of the highest rates of COVID-19 mortality and morbidity of any population within Canada and globally (Badone, 2021; Canadian Institute for Health Information, 2021b; DeClerq, 2021; Thompson et al., 2020). In the earliest waves of the pandemic, widespread stringent visitor restrictions were used across Canada to help curb the spread of the virus within long-term care settings (Canadian Institute for Health Information, 2021a; Ministry of Health of Ontario, 2020; Public Health Agency of Canada, 2020). Although extreme restrictions (e.g., requirement to wear personal protective equipment, no gathering in common areas, no in-person visits) on visitors and staff were necessary as an infection control measure, these drastic measures increased social isolation and decreased the well-being of OA living in long-term care (OA-LTCH) (Canadian Institute for Health Information, 2021a; Paananen, 2021; Stall et al., 2020). Research has shown that social isolation and loneliness experienced by OA have significant impacts on their physical and mental health (Bethell et al., 2021; Courtin & Knapp, 2017; Hado & Feinberg, 2020; Kehyayan et al., 2016). Prior to the pandemic, many family members provided key emotional support and social engagement to OA-LTCH (Bethell et al., 2021; Hado & Feinberg, 2020; Provincial Geriatrics Leadership Office et al., 2020). But throughout the pandemic, in-person access to LTCH was variably restricted. As a result, health providers assumed greater responsibility for the care and well-being of OA-LTCH raising concerns about health providers’ ability to provide quality care in the context of increased workloads. In addition, amplified workloads were raised as potentially increasing their risk for experiencing burnout (Bethell et al., 2021; Kemp, 2021; White et al., 2021).
Long-term care home implemented a variety of visiting options for family members, including window, virtual, outdoor, and indoor visits with associated precautions in place. These options for social engagement were hampered by OA’ physical and cognitive limitations, the use of personal protective equipment and their limited familiarity with technology often made it difficult to establish meaningful connections (Ickert et al., 2020; Moyle et al., 2020; Seifert et al., 2020). Health providers had a crucial role in supporting social connectedness between family members and OA-LTCH by being physically and emotionally present to facilitate communication, support the use of technology, and manage the OA-LTCH responses. Their engagement in these roles compounded their workload, contributing to the strain they were already experiencing (Bethell et al., 2021).
Social connectedness is the subjective evaluation of having close and meaningful bonding with others and has been described as both the opposite of loneliness (O’Rourke & Sidani, 2017) and a potential antidote to loneliness (Hare-Duke et al., 2019). Hare-Duke et al. (2019) developed a conceptual framework suggesting there are multiple dimensions, such as the closeness and level of involvement between individuals that can impact the feeling of being socially connected. Formal interventions have been shown to have value in preventing loneliness and social isolation in OA (Chipps et al., 2017; Fakoya et al., 2020), including those that specifically target building or maintaining social connectedness (Bethell et al., 2021; Lem et al., 2021; O’Rourke et al., 2018). Within the COVID-19 context, interventions to reduce social isolation and loneliness, such as video chats, telephoning, and visiting family behind glass, have demonstrated promise (Beogo et al., 2022; Bethell et al., 2021; Ickert et al., 2020; Lem et al., 2021). However, the available literature suggests a gap in understanding health providers’ roles in supporting social connections between OA-LTCH and their family members, particularly during periods where in-person visits were limited.
COVID-19 and associated government mandated restrictions on in-person engagement in LTCH had profound physical and emotional impacts on OA-LTCH, their family members and health providers. These effects are expected to endure over time. Moving forward, it will be paramount to use lessons learned from the COVID-19 pandemic to inform policies, resources, and staffing within LTCH so that the physical and emotional needs of OA-LTCH and their family members are met. In addition, priority must be given to ensure that LTCH staff are adequately supported and trained so that they can successfully provide person-centered care across a range of situations including outbreaks. To inform next steps to better support LTCH staff and OA-LTCH, it will be important to establish a clear understanding of health providers’ roles in facilitating social connectedness between OA-LTCH and their family members. Therefore, this study aimed to examine LTCH health providers’ experiences in providing care and supporting the social connectedness between family members and OA-LTCH in the context of a pandemic.
Methods
Design
An exploratory qualitative description approach was used to inform our understanding of the experiences of LTCH health providers in providing care and supporting OA-LTCH social connectedness (Bradshaw et al., 2017; Sandelowski, 2000). These interviews were a component of a larger study that sought to explore the impact that restrictions on physical access to LTCH had on the experience of social connectedness between family members and OA living in long-term care from both the perspectives of family members and health providers. The findings from the interviews with family members are presented elsewhere (Garnett et al., 2023).
Research Question
This research was guided by the following question: What were LTCH health providers’ experiences in providing care and supporting the social connectedness between family members and OA-LTCH during the COVID-19 pandemic?
Sample
The study setting was comprised of two LTCH within southwestern Ontario. Purposeful sampling was used to recruit a variety of health providers who had provided care to OA-LTCH during the COVID-19 pandemic (Palinkas et al., 2015). Recruitment strategies employed included online newsletters, social media channels, and posters placed within the LTCH.
Inclusion Criteria
Inclusion criteria stipulated that health providers who were employed within LTCH during the COVID-19 pandemic, able to consent, provided frontline care to OA, spoke English, and were able to discuss how they provided support with social connectedness between family members and OA-LTCH were eligible to participate. Those health providers who did not provide frontline care to older adults and their families during the COVID-19 pandemic were ineligible to participate. A review of the literature on studies using a qualitative descriptive design determined that most studies using this approach recruit between 11 and 20 participants, therefore, we sought to include at least 10 health providers and 10 family members for the full study (Garnett et al, 2023; Kim et al., 2017).
Institutional Review Board Approval
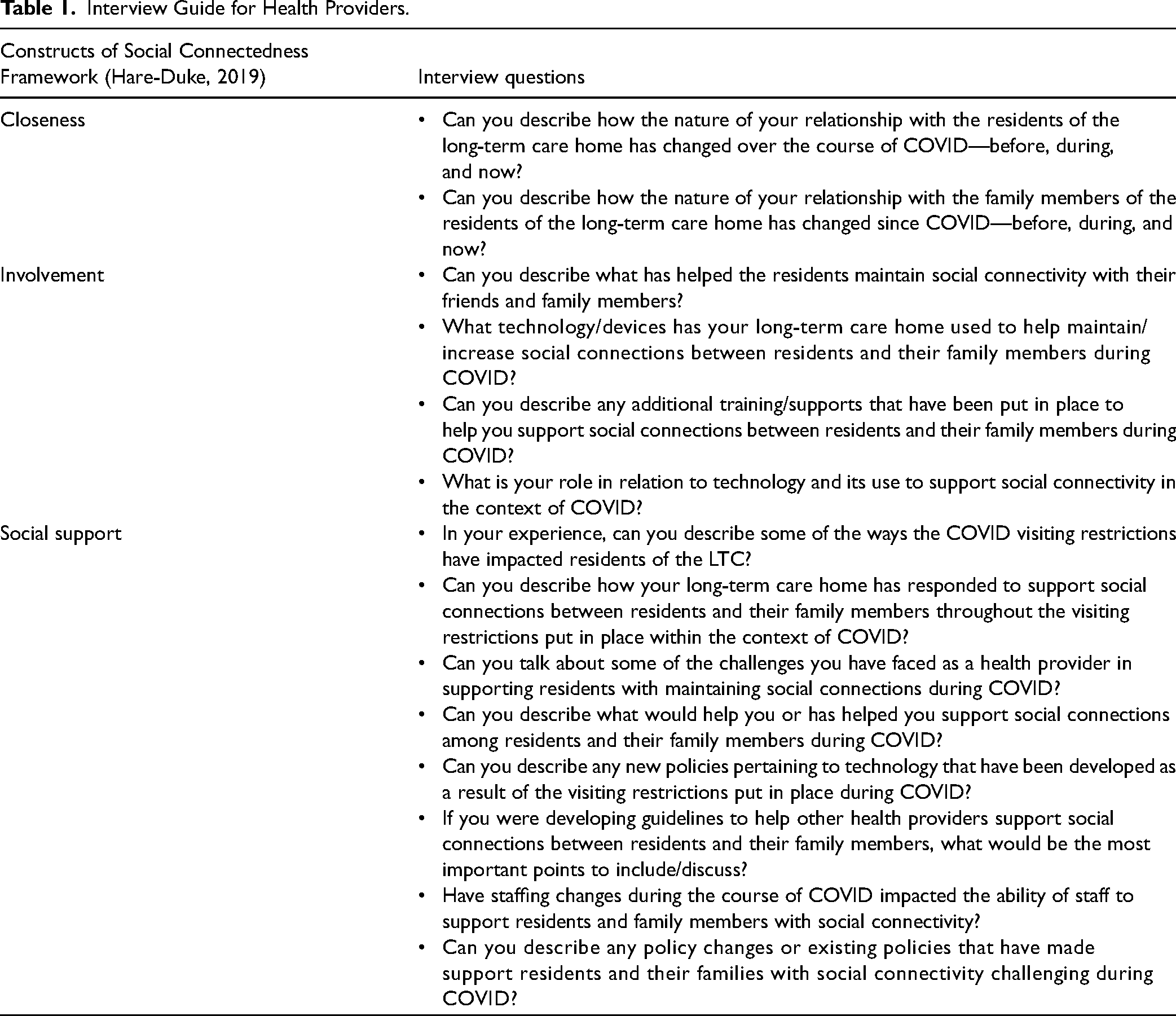
The University of Western Ontaro Health Sciences Non-Medical Research Ethics Board [REB # 116510] gave ethical approval for this study. Interviews with health providers (HP and NF) were conducted using a semistructured interview guide developed using the Hare-Duke et al. (2019) social connectedness conceptual framework. Informed by the mental health literature, the framework's main premise is that an intervention designed to foster an individual's social connectedness may be more successful if it contains a range of components rather than a singular focus (Hare-Duke et al., 2019). While the framework consists of five constructs (closeness, identity and common bond, valued relationships, involvement, and cared for and accepted), we chose to use the constructs of closeness, involvement, and social support, a subcomponent of “care for an accepted” to explore their application to the health provider role in facilitating social connectedness among OA-LTCH (Hare-Duke et al., 2019) (Table 1). These specific constructs were chosen as best suited to investigate the health providers’ perspective as individuals who were external to the OA-LTCH and therefore separate from their identity. The interview guide was trialed on one study participant, the responses discussed with the study team, and minor modifications made to the guide to ensure that the interview questions were eliciting data necessary to inform the study research question.
Interview Guide for Health Providers.
In-depth semi-structured interviews were conducted with participants between November 2020 and January 2021. Three interviews were conducted using the university's secure Zoom platform and eight were conducted by telephone to ensure public health guidelines for physical distancing were followed. Interviews were typically about 50 min long, were audio recorded, deidentified, and transcribed verbatim. Each participant received a $25 gift certificate in remuneration. HP and NF kept field notes throughout the interviews where they documented additional information about the study interviews such as time of day, interruptions, or expressions of emotion that were noteworthy. Immediately following interviews reflexive notes were also documented.
Analysis
Data collection and analysis proceeded iteratively, and the decision was made to conclude data collection once a point of data saturation was reached (Saunders et al., 2018). Inductive qualitative content analysis was used to analyze the data (Neergaard et al., 2009). Three researchers (AG, HP, and NF) conducted initial coding of data using NVivo 12 (QSR International, 2020) and individually recorded thoughts and reflections on the patterns or themes emerging from the data. In addition, they explicitly discussed how their own position as researcher and clinician influenced their understanding of the study data. Regular meetings allowed for ongoing discussion of study findings whereby the researchers for similarities and differences in the data, deciding on themes which described the data well, and compared themes to current knowledge within the literature (Neergaard et al., 2009; QSR International, 2020). Any discrepancies among the researchers were resolved through discussion among the full research team and final themes were unanimously agreed upon. Throughout this analytic process, the authors engaged in a process of reflecting on how their professional and personal experience influenced their understanding of the study data, and a book of field notes was kept documenting discussions pertaining to reflexivity. Moreover, all authors provided critical feedback throughout analysis to ensure various perspectives were considered and represented in the research (Neergaard et al., 2009).
Strategies employed to help ensure study rigor included obtaining a rich description of the phenomenon of interest, maintaining detailed field notes to allow for replication of the study, through the explicit acknowledgement of the researchers’ positionality and its potential influence on the study data and through the efforts of the researchers to practice reflexivity throughout the study (Guba & Lincoln, 1989; Maher et al., 2018). Researchers (HP, NF, and AG) regularly debriefed following interviews to discuss how their respective positionality influenced the data collection and understanding of the data. In addition, all researchers practiced reflexivity throughout the research process, and HP and NF engaged in reflexive journaling following individual interviews, while acknowledging how their respeective perspectives influenced their understanding of the study findings and the emergent thematic constructs.
Results
Sample
A total of 11 health providers participated in the study representing various health fields (e.g., personal support worker, registered practical nurse, therapeutic recreation therapist). No participants withdrew from the study at any point, and each participant was interviewed at a single timepoint. Most health providers were employed in their field for over 10 years and in their current position for 4–10 years (Table 2).
Health Provider Demographics.

Note. N = 11.
Themes
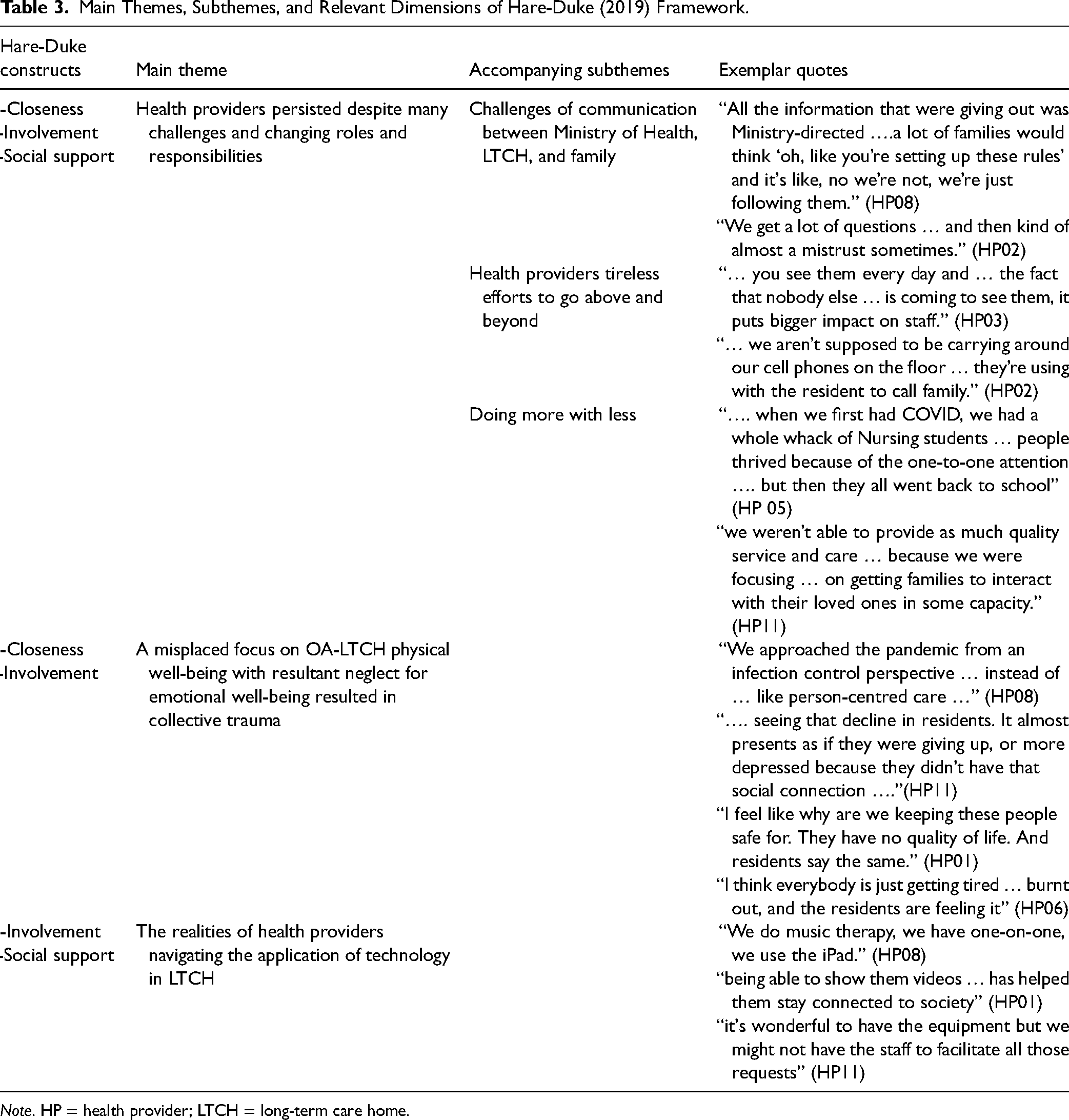
Three main themes with applicable subthemes were identified during the analysis: (a) changes in health provider roles and responsibilities caused them to experience emotional turmoil, with three subthemes including, (i) the challenges of communication between Ministry of Health, LTCH, and family; (ii) health providers “tireless efforts to go above and beyond”; and (iii) doing more with less; (b) a predominant focus on OA-LTCH physical well-being with resultant neglect for emotional well-being resulted in collective trauma, and (c) the challenges experienced by health providers using technology to support social connectivity (Table 3).
Main Themes, Subthemes, and Relevant Dimensions of Hare-Duke (2019) Framework.
Note. HP = health provider; LTCH = long-term care home.
Health Providers Persisted in Supporting the Well-Being of OA-LTCH Despite Many Challenges and Changing Roles and Responsibilities
Throughout the pandemic, health providers working in LTCH experienced frequently changing rules and regulations in addition to assuming a dramatically increased workload. Results of this study suggest that these challenging conditions in combination with family members’ responses to the conditions left health providers feeling frustrated but still determined to continue supporting OA-LTCH and their families in any way they could. Three subthemes demonstrate the varying ways LTCH health providers experienced changes in their roles and responsibilities: (a) the challenges of communication between Ministry of Health, LTCH, and family, (b) health providers tireless effort to go above and beyond, and (c) doing more with less.
The challenges of communication between ministry of health, LTCH, and family
Health providers struggled to adhere to the rapidly changing rules and communicate the changes to OA-LTCH and their families. The uncertainty of Ministry guidelines set a precedent for mistrust by both family members and health providers. For instance, some guidelines were contradictory and led to concern about risk for OA-LTCH. Family members were required to have a COVID-19 test to visit; however, they could take the OA-LTCH out bring them back to the LTCH without a test. Health providers were concerned about the ramifications of these actions: … and then a lot of the directives don’t make sense … you’re not allowed to come in and visit your family member, unless you get a COVID swab and you’re wearing a mask and staying six feet apart. But you’re allowed to come and pick your family member up and take them to your house and you don’t need a COVID swab to do that. (HP01)
Additionally, participants experienced mistrust from family members regarding Ministry directives, “All the information that we were giving out was all Ministry-directed … a lot of the families would think ‘oh, like you’re setting up these rules’ and it's like ‘no we’re not we’re just following them” (HP08). Families asked many questions, but health provider participants felt their responses were unsatisfactory, “We get a lot of questions about how we’re doing and then kind of almost a mistrust sometimes. If I tell them, yeah everybody is healthy here, they’re like, “Are they though? Are you not telling us?” (HP02). Health providers felt futile in gaining the trust of family members.
Health providers’ tireless efforts to go above and beyond
Health provider participants worked tirelessly to support the social connectedness needs of OA-LTCH and their families, “… you see them every day and … the fact that nobody else … is coming in to see them, it puts that bigger impact on the staff, right” (HP03). In another example, health providers were careful to acknowledge others who passed away during the pandemic: We brought butterflies for each resident who had passed because we had lost 14 people during COVID, and so we named the person and we put the butterfly up in the garden area and so it's there for the residents, you know, like so it was like a closure to the whole thing because you know these were their friends … (HP08)
Participants would occasionally bend the rules to try and support the OA-LTCHs’ emotional needs. For example, one participant described using their personal phone to provide virtual visits or phone calls to families: … we aren’t supposed to be carrying around our cell phones on the floor, but I know some of the staff have been, because that's how the residents can connect with family … we’ve been a bit more lenient if we see a staff member with a cell phone, because we see that they’re using it with the resident to call family (HP01)
They described turning a blind eye to physical interactions between family members and OA-LTCH because they recognized how critical touch was for their emotional well-being, “Once they’re in their room and the door's shut, I know that their hugging, they’re holding hands, and I’m not going to go in there and tell them not to. I just won’t” (HP02). Some participants also discussed being approached by family members in the parking lot and would take the time to connect with family members, “Families in the parking lot [would stop] us as we went into [work] just [to] … give their well wishes and get any updates they could out of us … Just devastating really …” (HP04). Health providers shared the struggles OA-LTCH have endured in addition to their own emotional burdens.
Doing more with less
This subtheme describes how health provider participants supported OA-LTCH in maintaining social connections but were ill-equipped to do so. Initially during the pandemic, participants described supports they received such as extra staff through redeployment and having nursing students present within the LTCH. This allowed the health providers to spend more time with OA-LTCH to meet some of their social needs. Eventually, this increased level of support diminished, leaving a large void that core staff were not adequately able to fill: … when we first went into COVID, we had a whole whack of Nursing students … that gave us so much more support on the halls when people got isolated to their rooms. And people thrived because they had a lot of one-to-one attention … and meaningful engagement. Then the students all went back to school, and we we're … back down to our base staffing numbers, which of course through all the reports is not enough. (HP05)
The pandemic restrictions also impacted recreational staff's ability to implement programs as they prioritized their efforts in facilitating family visits. This significantly affected some OA-LTCH who had limited family and relied on the programs: … in terms of our programming … we weren’t able to provide as much quality service and care … because we were focusing so much attention on getting the families to be able to interact with their loved ones in some capacity. (HP11)
The participants discussed how they tried to prioritize the OA-LTCH needs and wants, however, the standards and guidelines often conflicted with the OA-LTCH and families’ preferences. Health providers emphasized the necessity of maintaining the rules, but stressed that this created internal conflict for them, “… having to stand up for something that you don’t necessarily agree with and then be reprimanded by a reasonably upset family member. It's hard. It's really hard” (HP04). Participants felt as though they had tried their best given the circumstances but recognized the damage that had been done and acknowledged the need for improvement for future situations, “I feel like we’ve done the best job we can do, but it's not enough. If you were used to seeing your wife every single day for hours a day, and then for the past nine and a half months, she's come in and did a visit with you for an hour once or twice a week, it's not the same” (HP03).
Participants also highlighted the need for growth and policy development from government to ensure that there is proper guidance for future lockdown circumstances: I think the government really has to take a look at how they expect anyone to be able to provide adequate care to their own Ministry standard … I know it comes down to funding and it's very complicated but … we have to do better. (HP04)
The participants were frustrated with the limited direction and agency they had to respond to extremely challenging conditions during the pandemic, “… we’re trying to be leaders but also kind of figuring out as we go along without a lot of guidance” (HP11).
A Misplaced Focus on OA-LTCH Physical Well-Being with Resultant Neglect for Emotional Well-Being Resulted in Collective Trauma
Study participants noted there was a strong focus on physical health but at a cost to emotional well-being, “We approached the pandemic from an infection-control practice … instead of … like personal-centered care; so … removing the family had a huge impact on their connectivity and their psychosocial well-being for sure” (HP08). The failure to consider the emotional health of OA-LTCH, family members, and health providers compounded what was already a very traumatic experience for all involved. The participants described how they witnessed firsthand the physical and emotional consequences of enforced separation: … mentally you can definitely tell that it has taken a toll on a lot of them and then when you’re having those mental concerns, it leads to, physically you just don’t feel happy enough, so you don’t want something to eat or maybe you’re not drinking well … it can systemically really affect you. (HP03)
Health providers indicated that while they were keeping the OA-LTCH physically safe many experienced declines in their quality of life. Going forward, study participants emphasized the need for more resources to understand how best to support OA-LTCH in a holistic manner: Really, 70% of a person's overall quality of life and wellness is based on their emotional wellbeing and their connectedness and their engagement and their purpose and meaning in their life and there's so little money and resources put into that at this time when it's really needed. (HP05)
Health provider participants also expressed concern around the connection between loneliness and its influence on mortality during the pandemic, noticing that many OA-LTCH appeared despondent. It was as if loneliness triggered a loss of interest in life, … I feel like the overall arching theme is … seeing that decline in residents. We have several residents that have passed away—it almost presents as if they were giving up, or more depressed because they didn’t have that social connection from their family and from that core group of resident volunteers, and … co-residents participating in programs. (HP11)
One health provider shared an emotional story about how the rapid and severe deterioration of an OA-LTCH subsequently impacted their family: … One gentleman would come every day to see his wife … once they allowed an outdoor visit, I think he came once or twice … it's too hard for him to see her now because she's declined so much and she doesn’t know who he is anymore … I don’t think he's been here in months … I don’t think he can handle it anymore. (HP06)
The participants began to question the value of the infection control protocols: I feel like what are we keeping these people safe for? They have no quality of life. Why am I -? And a lot of the residents, they feel the same. They’re like, “Why? Why are you keeping me safe, just to sit in this box and I can’t see my husband or I can’t see my grandchildren? What is the point?” … we need to remember that they do have rights … we’re trying to keep them safe, but at what cost? (HP01)
The toll of caring for and supporting OA-LTCH and their families as they experienced social and emotional isolation left health providers overwhelmed. One participant expressed the emotional toll health providers were collectively experiencing, … I think everybody's just getting tired and … burnt out, and the residents are feeling it and the staff are going through it, and I think they … get short-tempered and impatient … I think they take it out on the residents, and I know they don’t mean to … (HP06)
Interviews with participants have highlighted the enormous discord between physical health and OA-LTCH and family members’ emotional well-being. The stringent policies and directives greatly impacted providers, OA-LTCH, and family members alike.
The Realities of Health Providers Navigating the Application of Technology in LTCH
Interviews with health providers revealed the barriers and facilitators of technology use during the pandemic. The availability of staff, time, resources, knowledge, and individual capacity to utilize technology appropriately to support social connectedness was variable across LTCH. Health providers noted benefits associated with technology use and expressed gratitude for having so many options available to promote social connections and engagement among OA-LTCH: … we’re so lucky, the day and age that this pandemic has happened because we have so much technology … Skype or Zoom or whatever has been very helpful for them to stay connected with their family members. (HP01)
Not only was technology beneficial for visits, it facilitated other types of social engagement for OA-LTCH but staff were able to continue music therapy, virtual concerts, virtual church services, and more, “We do music therapy … we have one-on-one, we use the iPad. We have a therapist on the other end singing to the residents, talking to them because they knew them from before.” (HP08) Many participants showed videos to OA-LTCH to stimulate their interests and keep them engaged, “Being able to show them YouTube videos of babies or puppies or just funny things on the internet, has really helped them stay connected to society …” (HP01) For some OA-LTCH, technology provided a way to stimulate their interests and provided them with social connection and engagement.
Technology donations were made during the pandemic to enable programming to continue virtually throughout the pandemic. One health provider shared that Google donated multiple Google Home consoles and provided support and education to staff, which was appreciated by the home: … last week we had a donation from Google [to have a] Google Home on each neighbourhood … and a year's subscription … that's brand new to us … there are phones associated so we can use it to set up virtual visits … we are in touch with a technician from Google who's going … to give us some training, our recreation department … then we can … be the experts that teach the floor staff how to use it … (HP11)
In addition to external support, participants noted that the provision of technology provided the impetus for them to become more proficient in using technology. Due to the scarcity of onsite support or formal technology focused education, providers often sought training from other sources such as younger coworkers, Google, Amazon, and the Ontario Centres for Learning, Research and Innovation in Long-Term Care (CLRI). They were motivated to support OA-LTCH and found ways to adapt quickly: And the CLRI helped me come up with an easy fact sheet on how to operate the Fire Sticks so that we could train staff on the floor to use it. So, I guess that ties in with the training but it was kind of me doing some exploration to figure out how to use it on my own and then getting that information, typing it up, and now we have several policies and procedures on how to operate the device. (HP11)
Though participants spoke about the many benefits of technology, there were also challenges associated with its use. For many providers, the pandemic marked the first time they had used technology to support OA-LTCH and guidance was limited, “Yes, we started with virtual visits and it was quite the process to get it started because we didn’t have a lot of direction from management and our recreation department kind of took it on …” (HP11) Even as the pandemic persisted, initiating and facilitating virtual visits was a constant challenge for staff. Redeployed staff eventually left, leaving fewer staff available to engage in virtual visits: … starting off with not a lot, we did get a lot now, and our current challenge is we’re never going to be able to facilitate as many virtual visits as we did at the beginning when we had redeployed staff, while still providing quality programming … it's wonderful to have the equipment but we might not have the staff to facilitate all those requests. (HP11)
In addition, health providers noted that technology was not helpful for all OA-LTCH. Any visual, auditory, physical, or cognitive issues experienced by OA-LTCH made it challenging for them to fully engage with or benefit from technology use: It certainly takes a lot more time and supervision to have a dementia patient utilize the technology. They require constant supervision with that type of interaction. You can’t really just set them up and walk away … we do the best we can trying to work around those obstacles but they still are obstacles at some point. (HP04)
When OA-LTCH were challenged to initiate or maintain virtual connections, health provider presence was of particular importance. Having to engage in these additional tasks typically outside of providers’ usual roles and witness OA-LTCH reactions to virtual visits, whether positive or negative, was mentally and emotionally draining for health providers: … lots of different reactions from both residents and staff. And occasionally the calls would become emotional too, and they could become upsetting. And that's why it was so important, we did have to make sure we were present for almost every single call. Every resident did need the support to be able to facilitate the conversation with us there. (HP11)
Throughout this study, participants shared the various benefits and challenges associated with technology use within LTCH for the purposes of social connection. Technology was instrumental in enabling families to see each other and interact, however, having the proper resources, staff, and time to ensure visits were meaningful was difficult to achieve. Furthermore, health providers were often necessary and invaluable in facilitating connectivity, but this came with a toll to their own well-being as they sought to compensate for the absence of family members.
Discussion
Findings from this qualitative research study enhance our understanding of LTCH health providers’ experience in supporting social connectedness between family members and OA-LTCH during COVID-19. Results suggest that health providers were committed to supporting OA-LTCH social and emotional well-being despite experiencing sudden changes in their own roles and responsibilities while also navigating frequently changing infection control directives. The primary focus by the Ministry of Health on infection control measures at the expense of social and emotional well-being of OA-LTCH had a collective toll on health providers, OA-LTCH and family members alike in the early waves of the COVID-19 pandemic. Additionally, health providers embraced technology to try and support social connections in the absence of in-person visits but experienced many challenges.
Key among the findings were the challenges faced by health providers in continuing to support OA-LTCH while abiding by frequently changing ministry directives. Findings suggest that early efforts to focus solely on physical health and infection control left the health providers frustrated but determined to continue to provide person-centered care with a support on psychosocial well-being. Their experiences highlight the juxtaposition of the directives, informed by a medical model, which ran counter to the values of person-centered care. Health provider participants highlighted both the cost to their own well-being of trying to implement the directives and questioned their ultimate value given their focus on longevity as opposed to quality of life. This finding corroborates other perspectives presented in the literature which note that attention on mortality failed to acknowledge the morbidity, including loss of quality of life which resulted from the extreme measures (Chu et al., 2020). Historically, LTCH has struggled to successfully actualize person-centered care with constraints on staffing and resources frequently being noted as key contributors (Kong et al., 2021; McArthur et al., 2021). As such, the findings highlight the need for more resources and innovative approaches to allow for collaborative care particularly in times of crisis or constrained resources (Hsu & Chao, 2022).
Technology was a key component used to help maintain social connectedness between OA-LTCH and family members, but its use compounded the burden placed on health providers. Health providers readily acknowledged its benefits, while noting it was not a panacea for in-person engagement. This finding is corroborated in the literature and adds emphasis to the need for policy and guidelines to enable incorporate technology as another pillar to help facilitate social engagement beyond the pandemic (Chu et al., 2021). A recent scoping review highlighted that factors such as equipment, additional workload, and organizational structure must be considered if technology is to be successfully implemented for social connection within LTCH (Lemaire et al., 2023).
Examination of study findings in relation to the Hare-Duke et al. (2019) framework of social connectedness highlights how the health providers often supplemented and facilitated the social connections of OA-LTCH. Their actions can be mapped onto the main constructs of the framework: closeness, involvement, and social support (Hare-Duke et al., 2019). Their actions functioned both as both facilitators of social connection and in some cases as providers of closeness and support for the OA-LTCH. This was particularly relevant with those OA who had advanced dementia. In these instances, it was the health providers who helped the OA manage their emotions brought on by the remote engagement with their families (e.g., virtual visits, phone, or window visits). Findings call attention to complexity of social connection among OA-LTCH and the need to include the health providers as integral and necessary for healthy social connections among OA particularly in the absence of family.
Study participants expressed concern over the impacts of social isolation on OA-LTCH and the concomitant burden it placed on health providers. Our analysis supports White et al. (2021)'s findings that LTCH health providers have experienced emotional burdens caring for OA-LTCH by witnessing increased distress, illness, and death. While health provider participants were cognizant of the need to prevent the spread of COVID-19, many were conflicted as they witnessed the decline of OA-LTCH. Like White et al. (2021) our study findings determined that health providers working in LTCH had increased concerns about OA-LTCH's emotional well-being. Health provider participants from a range of disciplines advocated for the OA-LTCH and stepped in to provide social connection when it was absent or difficult to obtain. Their actions speak to the construct of social support which is a subconstruct of “feeling cared for” in Hare-Duke et als' (2019, p. 193) model of social connectedness. In line with Hare-Duke et als' (2019) conceptualization, the health providers took action to provide the assistance that was necessary in the absence of family members or other opportunities for social connection. The health providers also acted as facilitators fostering involvement and recognizing the importance of maintaining human connections even if through remote means such as technology. However, the study findings suggest there may be additional complexity to consider regarding a framework of social connectedness particularly in LTCH or other institutional settings where multiple health or allied health providers may have a key role in supporting the social and emotional well-being of residents in addition to family members and other OA-LTCH. Study findings suggest that there may be opportunity to include a parameter that speaks to the external parameters that influence an individual's ability to achieve social connectedness. In the current study, many health providers struggled to keep the OA-LTCH safe and socially connected, efforts that were hampered by the need to follow the political and institutional mandates. The prevalence of negative emotional impacts on health providers working within LTCH during COVID-19 such as sadness, stress, and vicarious trauma is increasingly being documented in the literature and warrants additional research (Boamah et al., 2023; Tupper et al., 2020).
Throughout the pandemic, LTCH health providers faced significant changes in their roles, responsibilities, and expectations that resulted in experiencing emotional turmoil. Health providers in this study and within the literature have discussed their role in supporting visits throughout the pandemic, such as scheduling visits, setting up technology, being present during visits, and cleaning equipment (Ickert et al., 2020; Kemp, 2021; Verbeek et al., 2020). The current study findings extend the literature by increasing our understanding of the emotional burden health providers experienced because of their tremendous efforts to socially support OA-LTCH.
In addition, the lack of family presence within the LTCH left a void that many health providers tried to fill. Pre-pandemic, families were instrumental in providing additional support to OA-LTCH with significant physical and emotional needs (Bethell et al., 2021; Provincial Geriatrics Leadership Office et al., 2020). When the pandemic began, policies failed to take into consideration the substantial involvement of family and the potential consequences of their exclusion (Bethell et al., 2021; Kemp, 2021). Study participants shared their challenges of adhering to Ministry mandates while trying to provide OA-LTCH with the care and social connections they needed for their well-being, such as using their personal devices to communicate with the families of OA-LTCH. A growing body of evidence emerging from the COVID-19 pandemic suggests that health providers working in LTCH experienced profound negative impacts on their health and well-being as a result of the working conditions they faced (Martin et al., 2021; Reynolds et al., 2022; Statistics Canada, 2021). Moving forward from the the pandemic, LTCH health provider retention and recruitment has emerged as a widespread and troubling concern (Connelly et al., 2023; Organization for Economic Co-operation and Development, 2021; White et al., 2021). In order to provide the care and support OA-LTCH require across a range of situations, including seasonal outbreaks, attention must be given to providing the resources, tools, and funding that LTCH require to function safely and compassionately for both OA and health providers.
Finally, technology became essential for OA-LTCH and families to try and maintain social connections throughout the pandemic. Research completed before the start of the pandemic suggested that smartphone videoconferencing between OA-LTCH and families was an effective way to reduce feelings of loneliness at one, three, and six months (Tsai et al., 2020). However, this study's findings highlight that OA-LTCH living with dementia may find it difficult to establish meaningful connections with family members and the assistance of health providers was often necessary, similar to other research (Bethell et al., 2021; Ickert et al., 2020; Seifert et al., 2020). Current study findings showed that health providers continued to address limitations in OA-LTCH's ways of socially connecting by having family members write letters or share pictures or YouTube videos to encourage mental stimulation. The health providers further demonstrated their willingness to expand their roles throughout the pandemic by learning to work with technology to meet the OA-LTCHs’ needs.
Strengths and Limitations
By sampling health provider participants during the second wave of the pandemic, the study data reflect some of the most challenging and unprecedented circumstances faced by health providers within LTCH. However, there are study limitations. The research was conducted in Ontario within a public/private LTCH system; therefore, findings may not be transferable to other areas of Canada, or globally. We also acknowledge that some health provider perspectives that were not represented in this study sample such as Registered Nurses and Physicians, although they routinely comprise less than 25% of the workforce within the LTCH setting in Ontario. Nevertheless, perspectives of Registered Practical Nurses, a key health provider in LTC were presented in the data. Also missing from the data was demographic information on the race and ethnicity of participating health providers. Future studies can address this gap which will help inform strategies such as fostering an inclusive organizational culture (Debesay et al., 2022). While efforts were made to ensure the rigor of the study processes and validity of the findings, engaging in a process of member checking could be done as a next step to both confirm the study findings and ensure that additional perspectives were not missed (Creswell & Plano Clark, 2007). The Hare-Duke et al., (2019) framework used to inform participant interviews was developed within a mental health context and not validated for OA. Therefore, in future research, it may be helpful to explore social connectedness in this population using a framework that considers conditions such as dementia and their potential impact on social relationships. Moreover, the experiences of participants in this study do not necessarily represent all health provider experiences or perspectives. Next steps include research to inform formalizing the use of technology for social connectedness among OA-LTCH. As such it will be important to understand how health providers' time, education, and roles may evolve with formal integration of technology within LTCH.
Implications
Study findings suggest that a holistic approach to infection control approaches would be beneficial to help minimize the collateral impacts on OA-LTCH, their families, and health providers. Although COVID-19's impact on LTCH was unprecedented, the system was ill-prepared and health providers were consistently placed in situations where they were challenged to adequately respond and which subsequently caused negative impacts on their health and well-being. Policy makers are encouraged to balance safety with the physical and emotional well-being of OA-LTCH, family members, and health providers in their mandates. Potential strategies could entail developing crisis support task forces to assist in training and preparation of health providers for crisis situations (Ripp et al., 2020). There is also a need to systematically examine policies and procedures that were in place during COVID-19 taking into consideration emerging research on the impacts of stringent infection control procedures on patient outcomes and health provider and family member well-being (Gupta et al., 2021; Kuhlman et al., 2021).
In addition, greater attention and funding must be implemented to support health providers working in LTCH. This includes providing the financing and resources to enhance their capacity to respond to crisis situations. Although health human resources challenges existed within LTCH prior to the pandemic, COVID-19 drew attention to the resultant negative impact this has had on the health and well-being of OA-LTCH and the health providers themselves (Clarke, 2021; Estabrooks et al., 2020). Job security, full-time positions, and sufficient staffing must be a priority to ensure the health and well-being of OA-LTCH and health providers.
Finally, technology has a meaningful place in LTCH settings with its many benefits for fostering social connectivity, particularly during lockdown situations. However, technology may not be able to meet all OA-LTCH’ needs, such as those living with advanced dementia. In such contexts, maintaining physical interaction should be prioritized to ensure that social connectedness is equitable for all OA-LTCH and their families. Additional funding will allow for more technology within the homes to enhance options for social connectivity to OA-LTCHs and family members and avoid health providers having to use their personal devices to maintain these connections.
Conclusion
This study sought to examine health providers’ experiences in supporting social connectedness between family members and OA-LTCH during the COVID-19 pandemic. Sudden changes in the health providers’ roles and responsibilities coupled with frequently changing ministry directives compounded the challenges faced by health providers as they sought to support OA-LTCH and their families in new and different ways. Collective trauma resulted from the neglect of the emotional well-being of providers, OA, and their family members arising from the overall crisis experienced by LTCH. Lastly, while technology could provide some elements of social connectedness for OA-LTCH and their family members, there were also challenges at individual and systemic levels associated with using technology. Analysis emphasizes the need for more holistic approaches to infection control that considers potential impacts on OA-LTCH, their families, and staffing requirements within LTCH. Further research is required to optimize possible benefits of technology for engagement and social connectedness among OA-LTCH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the University of Western Ontario Research COVID-19 Catalyst Grant.