
Abstract
Introduction
Cognitive impairment is having trouble remembering, learning new things, concentrating, or making decisions that affect the daily life of diabetic patients. The worldwide prevalence of diabetes mellitus (DM) was 2.8% in 2000 and is estimated to be 4.4% by 2030.
Objective
To assess the prevalence of cognitive impairment and associated factors among DM patients attending follow-up treatment at Fiche General Hospital, North Ethiopia, 2022.
Methods
A hospital-based cross-sectional study was conducted from July 15 to September 15, 2022. The total sample size was 421 and a systematic random sampling technique was used. Data were collected through a face-to-face interview. Data were entered using EpiData Version 3.1 and exported to SPSS Version 24 for analysis. Statistically significant was declared at a P-value of less than .05 with an adjusted odds ratio (AOR) and 95% confidence interval (CI).
Result
The prevalence of cognitive impairment in the current study was 56.3% with (95% CI: 51.5–60.8). Primary educational status (AOR 6.73, 95% CI: 2.92–15.51), having Type II DM (AOR 4.93, 95% CI: 2.84–8.56), uncontrolled blood sugar (AOR 6.24, 95% CI: 3.84–10.17), and current alcohol use (AOR 1.94, 95% CI: 1.11–3.36) were significantly associated.
Conclusion
About three in 5 DM patients attending follow-up treatment at Fiche General Hospital were suffering from cognitive impairment. Educational status, type of DM, status of fasting blood sugar, and current alcohol use were associated with cognitive impairment among DM patients. Therefore, improving educational status, controlling blood sugar, and avoiding alcohol use may reduce the risk of cognitive impairment in DM patients.
Keywords
Introduction
Cognitive impairment is having trouble remembering, learning new things, concentrating, or making decisions that affect their daily life in diabetic patients. It is one of the chronic complications of diabetes mellitus (DM) patients (Mavrodaris et al., 2013; Moheet et al., 2015). The worldwide prevalence of DM was 2.8% in 2000 and is estimated to be 4.4% by 2030 (Krishna et al., 2015; Mavrodaris et al., 2013; Sandhir & Gupta, 2015; Umegaki et al., 2013).
Impaired glycemic control and lack of insulin within the nerve cell results in cognitive impairment in DM patients and the increase in blood sugar past the physiological limit leads to acute or chronic complications to different body parts including the central nervous system particularly cognition (Anderson et al., 2001). Cognitive impairment contributes to impairment in the quality of life and additionally, the resulting cognitive dysfunction may result from a lack of adherence to treatment, resulting in high morbidity and mortality (Logroscino et al., 2004).
The definite mechanisms of cognitive impairment in DM are hypothesized due to brain vasculature changes, disturbances of cerebral insulin signaling, glucose toxicity, accumulation of advanced glycation end products, hypoglycemic episodes, and alteration in amyloid metabolism (Bornstein et al., 2014; Das et al., 2019; Lavielle et al., 2015; Ojo & Brooke, 2015; Saedi et al., 2016).
Literature Review
Studies indicate that psychomotor efficiency, memory, attention, visual construction, and mental flexibility are greatly impaired. This results in reduced walking speed, impaired balance, increased risk of failing, and fractures that reduce the quality of life (Bornstein et al., 2014; Das et al., 2019; Lavielle et al., 2015; Saedi et al., 2016). Studies report that age, sex, educational level, duration of DM (Kawamura et al., 2012), metformin use (Moore et al., 2014), poor health, sensory impairments, incontinence, and falls (Rait et al., 2005), and residence were some of the important risk factors for cognitive impairment in DM patients (Hamed & Bartosz, 2018; Sengupta et al., 2014). Damage of cognitive function domains has been reported in diabetic patients, but there are some differences in the aspects of function that are damaged between Type I and II DM (Birhanu et al., 2019).
Studies conducted in developing countries on cognitive impairment among DM patients were limited to Type II DM only (Dagnew & Wolide, 2017; Muluneh, 2013). Similarly, to the best of our knowledge, the literature lacks studies that were conducted on cognitive impairment in both Type I and Type II in Ethiopia. As a result, the authors were interested in identifying the prevalence in both types and this study assessed the prevalence and associated factors of cognitive impairment among DM (both types) attending follow-up treatment in Fiche General Hospital, North Ethiopia.
Materials and Methods
Study Area and Period
The study was conducted in the Fiche General Hospital outpatient department in the Selale zone, Oromia region. The zone is located 112 km away from Addis Ababa, the capital of Ethiopia. The hospital serves about 1.5 million population. Currently, there are more than 1,500 DM patients attending follow-up treatment in outpatient departments and on average, 25–30 patients visit daily. The study was conducted from July 15 to September 15, 2022.
Study design: A hospital-based cross-sectional study design was employed.
Source Population
All DM patients attending follow-up treatment at Fiche General Hospital.
Study Population
All selected DM patients attended follow-up treatment at Fiche General Hospital during the study period.
Eligibility Criteria
DM patients aged greater than 18 years old were included, however, severely ill and duration of illness of less than 1-year patients during the data collection period were excluded.
Sample Size Determination
The sample size was determined by using a single population proportion formula, assuming a prevalence of 53.3% (Dagnew & Wolide, 2017) from the previous study, a margin of error of 5%, and a confidence level of 95% as follows.

Sampling Procedure
The number of 4-month (March, April, May, and June) reports of the DM patients attending follow-up treatment at Fiche General Hospital was determined. Then, the determined number of patients in 4 months was averaged for 2 months, as the data collection was for 2 months. The 2-month average number of patients was 900. Then, by using a systematic random sampling technique, the DM patients attending follow-up treatment were included in the study based on the calculated constant value 2 that was gained by (900/421 = 2). The first DM patient was selected by lottery method and then, every second DM patient attending follow-up treatment was interviewed.
Study Variables
Dependent variable: Cognitive impairment.
Independent Variables
Sociodemographic factors: Age, sex, religion, ethnicity, educational status, marital status, occupation, monthly income, and residence.
Clinical factors: Type of DM, episode of hypoglycemia, type of DM medication, duration of treatment, Body Mass Index, blood sugar status, medication adherence, and presence of comorbidity.
Behavioral factors: Lifetime alcohol drink, current alcohol drink, lifetime tobacco used, current tobacco used, lifetime chewing chat, and current chewing chat.
Operational Definition
Cognitive impairment: Assessed using Mini-Mental State Examination (MMSE) (Kurlowicz & Wallace, 1999). It evaluates several cognitive domains; temporal and spinal orientation, working and immediate memory, attention and calculation, the naming of objects, repetition of a sentence, execution, planning, and praxis. In all items, each answer scores 1 point, and each incorrect scores 0. The maximum score that can be obtained was 30 and the minimum was 0. Then, by using the Receiver-Operating characteristic Curves analysis cutoff value, the score was categorized as no (if scored 24–30) or yes (if scored 0–23) (Dagnew & Wolide, 2017; Kurlowicz & Wallace, 1999).
The severity of cognitive impairment: Measured using MMSE similarly to cognitive impairment. Then, categorized as mild (if scored 20–23), moderate (if scored 10–19), and severe (if scored 0–9) out of 30 questions (Gugssa et al., 2011).
Medication adherence: Measured by using the Morisky Medical Adherence Scale-8. It consists of eight items with a scoring scheme of yes for 1 and no for 0 for the first seven items and a 5-point scale (i.e., 1: never, 2: once in a while, 3: sometimes, 4: usually, and 5: all the time) for the eighth item. Then, the score was categorized as low (if scored ≤2), moderate (if scored 3–7), and high (if scored 8–12) (Moon et al., 2018).
Fasting blood sugar: Blood sugar is measured from venous blood after at least 8 h of fasting (American Diabetes Association, 2020).
Lifetime substance user: Use at least one of the substances (alcohol, chat, cigarette) in an individual’s lifetime.
Current user: A person who consumed any substance within the last 3 months before the study period.
Data Collection Tool
A structured and pre-tested questionnaire was adapted from the literature (Shaw & Sicree, 2010; Tan et al., 2014). The questionnaire was validated for the Brazilian population (Kochhann et al., 2010) and used in Ethiopia (Dagnew & Wolide, 2017; Muluneh, 2013). It had a sensitivity of 86% and a specificity of 83% (Kochhann et al., 2010).
Data Collection Procedure
The data were collected through face-to-face interviews with DM patients. Four bachelors of psychiatry nurses collected the data and one experienced epidemiologist supervised the collection process. The interview was conducted in a patient waiting room after receiving the day's follow-up treatment. The weight and height of the patients were measured by the data collectors at data collection time. During the weight measurement, the participant stood with arms hanging at the sides after taking off heavy wear. Height was measured in a meter that was set from the bottom up; the patient standing in an anatomical position toward the examiner. Diabetes-related questions and fasting blood sugar were filled from the patient medical chart. Two data collectors were assigned together on morning and afternoon shit and an average of seven patients were interviewed per day.
Data Quality Assurance
The questionnaire was prepared first in English and translated to Afan Oromo (the local language of the Oromia region) for data collection and back to English by language expertise. The 2-day training was given to data collectors and supervisors about a smooth and polite approach to patients, how to interview the patients, filling questionnaires, measuring weight and height, and respecting the patient’s autonomy. A pre-test was conducted on 5% of the total sample size (21 DM patients) at Chancho General Hospital a week before the actual data collection. Based on the pre-test result, the necessary corrections were made. The reliability Cronbach’s test was done and it was 0.785. Continued close follow-up and supervision were performed by the supervisor and authors during the data collection. All filled questionnaires were reviewed for completeness before data entry.
Statistical Analysis
Data were entered using EpiData Version 3.1 and exported to SPSS Version 24 software for analysis. Descriptive findings were presented by frequency tables, graphs, and percentages. Multi-collinearity was checked and the goodness of fit test was done using the Hosmer–Lemeshow model goodness fit test. Bivariable analysis was done and variables with a P-value <.25 were taken to multivariable logistic regression analysis. Adjusted odds ratio (AOR) with a 95% confidence interval (CI) was considered and statistical significance was declared at P-value less than .05.
Results
Sociodemographic Characteristics of DM Patients
A total of 421 DM patients responded to the interview which yields an overall response rate of 100%. Out of the total patients, 252 (59.9%) were males and the religion most of the 397 (90.0%) were orthodox religious followers. More than half, 272 (64.6%) were Oromo by ethnicity and 161 (38.2%) were in the age range of 40–60 years. The educational status of 236 (56.1%) was primary and the marital status of 293 (69.6%) was married. The average monthly income of 190 (45.1%) was greater than 2,000 Ethiopian birrs, about 246 (58.4%) lived in rural areas and 113 (26.8%) were farmers (Table 1).
Sociodemographic Characteristics of DM Patients Attending Follow-up Treatment in Fiche General Hospital, Central Ethiopia, 2022.

Note. DM = diabetes mellitus.
Clinical Characteristics of DM Patients
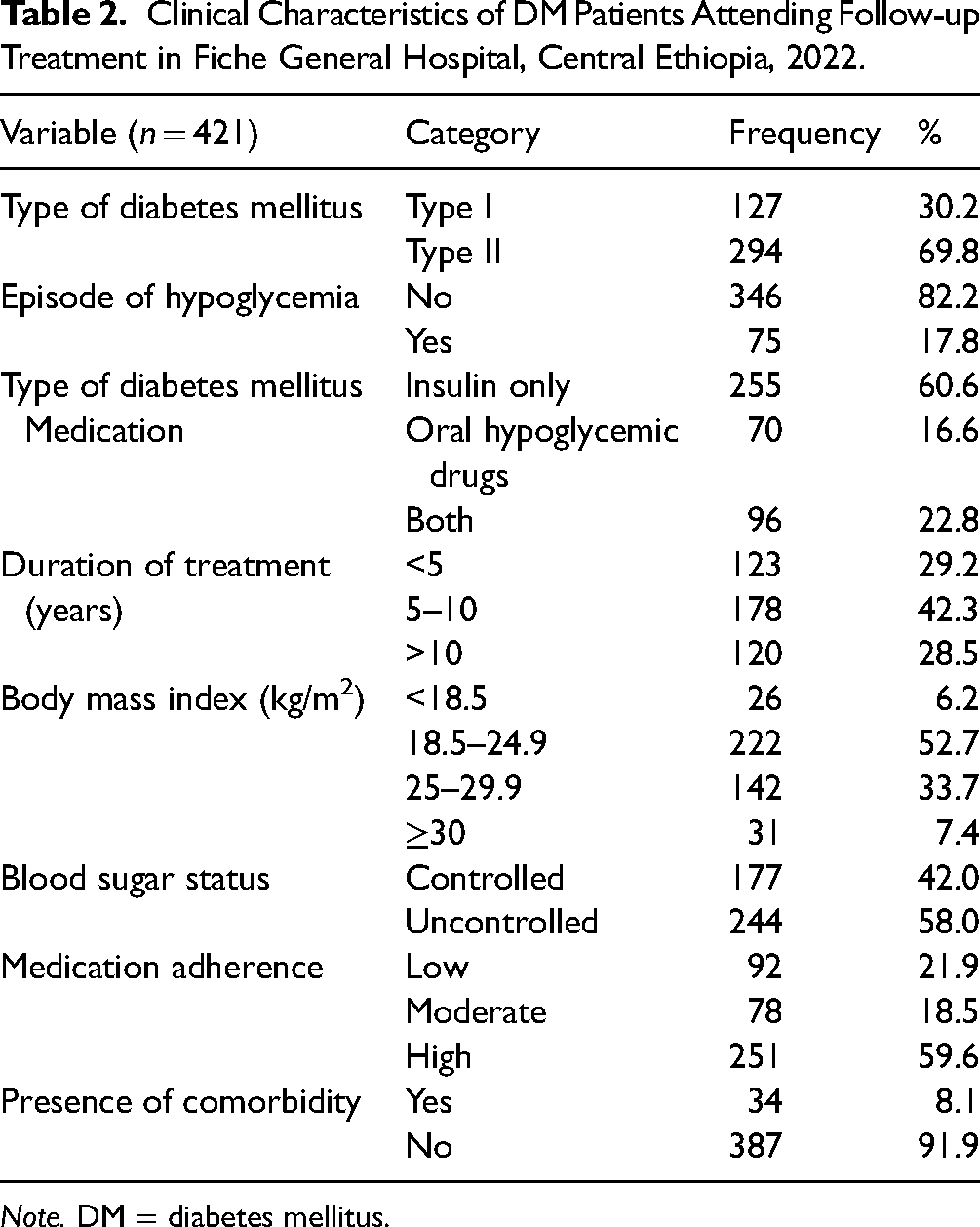
A majority, 294 (68.9%) had Type II DM, and 346 (82.2%) had no episode of hypoglycemia. More than half, 255 (60%) patients were receiving insulin only and 251 (59.6%) had high adherence to medication. The duration of treatment for 178 (42.3%) was 5–10 years, and 244 (58%) had uncontrolled blood sugar (Table 2).
Clinical Characteristics of DM Patients Attending Follow-up Treatment in Fiche General Hospital, Central Ethiopia, 2022.
Note. DM = diabetes mellitus.
Behavioral Characteristics of DM Patients
More than half, 251 (59.6%) had no history of drinking alcohol. However, 170 (40.4%) had a lifetime history of drinking alcohol. Only eight (1.9%) had currently used tobacco (Table 3).
Behavioral Characteristics of DM Patients Attending Follow-up Treatment in Fiche General Hospital, Central Ethiopia, 2022.

Note. DM = diabetes mellitus.
Prevalence of Cognitive Impairment Among DM Patients
Out of 421 DM patients, 237 (56.3%) had cognitive impairment, but, 184 (43.7%) did not have cognitive impairment (Figure 1).

Prevalence of cognitive impairment among diabetes mellitus patients attending follow-up treatment at Fiche General Hospital, North Ethiopia, 2022.
Specific Prevalence of Cognitive Impairment
Out of 237 DM patients who had cognitive impairment, 199 (84.0%) had Type II DM, however, 38 (16.0%) had Type I DM (Figure 2).

Specific prevalence of cognitive impairment among diabetes mellitus patients attending follow-up treatment at Fiche General Hospital, North Ethiopia, 2022.
The Severity of Cognitive Impairment of DM Patients
The severity of cognitive impairment among DM patients was 150 (63.3%), 78 (32.9%), and 9 (3.8%) mild, moderate, and severe, respectively (Figure 3).

Severity of cognitive impairment among diabetes mellitus patients attending follow-up treatment at Fiche General Hospital, North Ethiopia, 2022.
Factor Associated With Cognitive Impairment
In bivariable analysis; educational status, income level, type of DM, status of fast blood sugar, current alcohol use, and medication adherence were associated with cognitive impairment among DM patients. In multivariable analysis, primary educational status (AOR 6.73, 95% CI: 2.92–15.51), having Type II DM (AOR 4.93, 95% CI: 2.84–8.56), uncontrolled blood sugar (AOR 6.24, 95% CI: 3.84–10.17), and current alcohol use (AOR 1.94, 95% CI: 1.11–3.36) were significantly associated with cognitive impairment among DM patients (Table 4).
Bivariable and Multivariable Logistic Regression Analysis of Cognitive Impairment Among Diabetes Mellitus Patients Attending Follow-up Treatment at Fiche General Hospital, North Ethiopia, 2022.

Note. COR = crude odds ratio; AOR = adjusted odds ratio; CI = confidence interval. “1”: Reference group.
P-value <.05 in multivariable analysis.
Discussion
This study's prevalence of cognitive impairment was 56.3% (95% CI: 51.5–60.8). It was in line with a research result from Jimma University Medical Center, Ethiopia at 53.3% (Dagnew & Wolide, 2017) and Iran at 52.0% (Ali et al., 2012). However, it was higher than study reports from Black Lion Referral Hospital, Ethiopia at 45.0% (Muluneh, 2013), Nigeria at 40.0% (Eze et al., 2014), India at 33.7% (Sengupta et al., 2014), Jamaica at 32.2% (Hamed & Bartosz, 2018), the Central Africa Republic and Congo 18.8% (Mavrodaris et al., 2013), South Korea 9.7% (Sosa-ortiz et al., 2012), and Cameron 14.8% (Abba et al., 2017). The possible reason for the various prevalence of cognitive impairment among DM patients might be using different cognitive impairment screening tools, differences in sample size, educational status, socioeconomic status, and living standards of the participants. Additionally, including Type I and Type II DM patients in the current study might bring the difference.
In this study, educational status was statistically associated with cognitive impairment among DM patients. DM patients who had primary educational status were 6.73 times more likely to have cognitive impairment compared to DM patients whose educational status was college and above. This might be due to that memory and language functions were found to be more resistant to declining in highly educated patients, while attention, implicit memory, and visuospatial skills are found to decline irrespective of educational level. This finding was similar to a study report from Cameron (Abba et al., 2017).
This study revealed that the type of DM was statistically significant for the occurrence of cognitive impairment. Patients who had Type II DM were 4.93 times more likely to have cognitive impairment compared to patients who had Type I DM. This might be due to the neurotransmitter derangement resulting from insulin insufficiency either in quantity or quality which might result in defects of cognitive components like memory in Type II DM patients.
This study identified that the status of blood sugar was significantly associated with cognitive impairment. DM patients whose blood sugar was uncontrolled were 6.24 times more likely to have cognitive impairment compared to DM patients whose blood sugar was controlled. This could be due to the effect of hyperglycemia in neuronal toxicity and accumulation of free radical formation leading to oxidative stress (Vijayakumar & Dhanaraju, 2014). This finding was similar to a study report from Jimma University Medical Center (Dagnew & Wolide, 2017).
Current alcohol use was significantly associated with cognitive impairment. DM patients who were current alcohol users were 1.94 times more likely to have cognitive impairment compared to DM patients who were not current alcohol users. This might be due to the action of alcohol on the central nervous system depression, which leads to distraction and intention. This significantly inhibits neuronal activity in the hippo campus, and the formation of new declarative memory (Owan & Emily, 2019; Tsinuel et al., 2015).
Limitation of the Study
This study may be susceptible to recall bias as it asks back, and it might be prone to social–cultural desirability bias as the community gives their own concern for illness.
Implications for Practice
Identifying the independent risk factors of cognitive impairment in both Type I and Type II DM is important in aiding policymakers with important strategies. Planning and implementing a strategy for DM patients in consideration of educational status, type of DM, the status of fasting blood sugar, and current alcohol use can imply effective prevention.
Conclusion
About three in five DM patients attending follow-up treatment at Fiche General Hospital were suffering from cognitive impairment. Educational status, type of DM, status of fasting blood sugar, and current alcohol use were associated with cognitive impairment among DM patients. Therefore, improving educational status, controlling blood sugar, and avoiding alcohol use may reduce the risk of cognitive impairment in DM patients.
Footnotes
Acknowledgements
The authors would like to thank the study participants for giving accurate information and Jimma University for funding.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all areas; took part in drafting, revising, and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Data Availability
The data used for this study are available from the corresponding author on secured and reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical clearance was obtained from Jimma University Institute of Health, the institutional review board, and a formal letter of cooperation was written to Fiche General Hospital.
Funding
The funding for this study was covered by Jimma University.
Informed Consent
Written informed consent was obtained from each participant, and the information obtained from them would not have been disclosed. Coding was used to eliminate names and other personal identification of respondents to ensure anonymity, privacy, and confidentiality. Thoroughly, our research required the principles of the declaration of the Helsinki General Assembly, Seoul, Korea, October 2008.