
Abstract
Introduction
The proportion of stunted children in Indonesia is slowly decreasing. In most families, a mother is responsible for child care. The quality of maternal caregiving capability influences the mother’s ability to adopt appropriate childcare practices, which is essential to prevent childhood stunting.
Objectives
This study aimed to develop a model to enhance maternal caregiving capabilities in preventing childhood stunting based on the UNICEF model of care.
Methods
The study used an analytical observational design involving a pair of mothers and their youngest 6–23-month-old children registered at Posyandu (Community-based Integrated Health Care Center). Six hundred respondents were taken using a cluster sampling technique across seven healthcare centers in Surabaya City, East Java, Indonesia. The independent variables were child, mother, father, and household factors, then maternal caregiving capabilities. The dependent variable was the nutritional behavior to prevent childhood stunting. Data were collected using questionnaires and then analyzed using the Structural Equation Model-Partial Least Squares (SEM-PLS) test.
Results
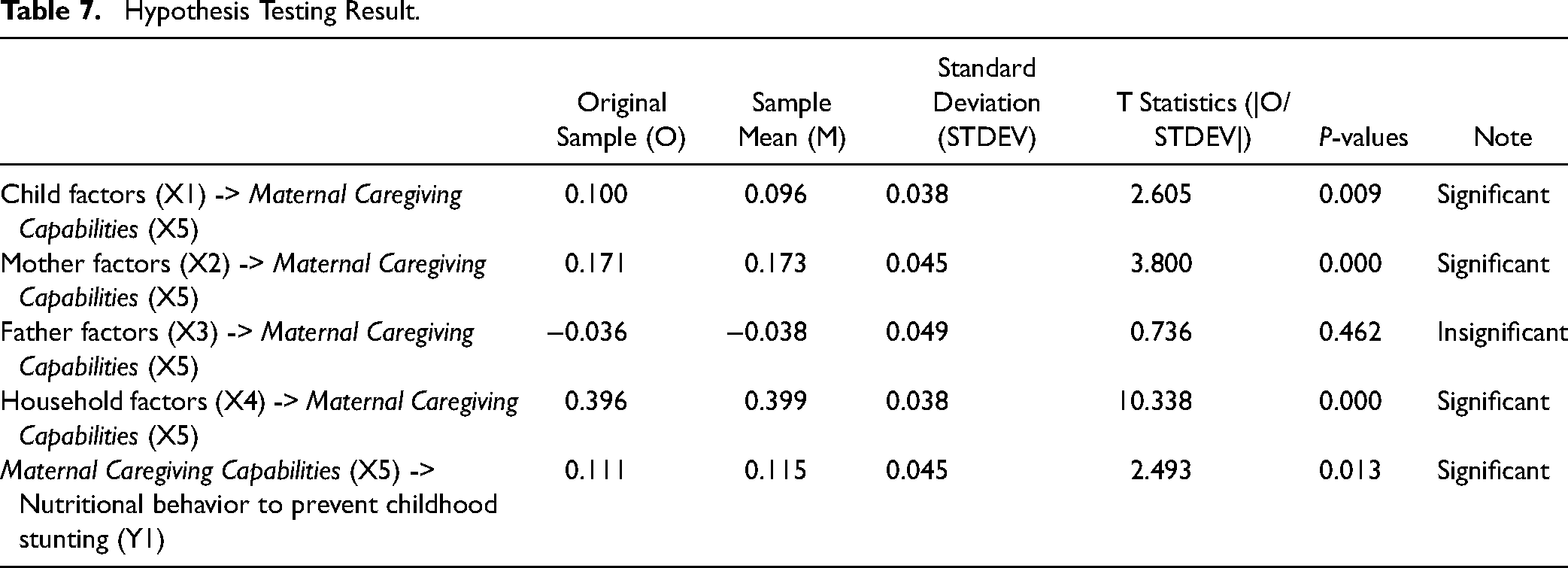
The study found that maternal caregiving capabilities are influenced by child (T-stat 2.605), mother (T-stat 3,800), and household factors (T-stat 10,338). Maternal caregiving capabilities affect stunting preventive behavior in children aged 6–23 months (T-stat 2.493). Household factors were the strongest factor affecting maternal caregiving capabilities.
Conclusion
Enhancing maternal caregiving capabilities model can be developed using its constituents, especially perceived physical health, psychological well-being, and decision-making. Household factors, including economic level and food security, were also important. High maternal caregiving capabilities were expected to enable mothers to improve their behavior to prevent childhood stunting (6–23 months).
Keywords
Introduction
Stunting has been declining steadily over the last decade but still is the most predominant type of malnutrition that affects children globally. In 2022, 148.1 million, or 22.3% of children under age five worldwide, experienced stunting. Indonesia has the highest prevalence of childhood stunting in South-East Asia (UNICEF et al., 2023). Zero Hunger is a Sustainable Development Goal (SDG) target that Indonesia has yet to achieve due to a decrease in the prevalence of stunting slower compared to the roadmap (United Nations, 2022). Although progress has been made, 30.8% of children under 5 were still affected as of 2018, which is classified as very high according to WHO (>30%). The Indonesian Nutritional Status Study (SSGI) by 2019, 2021, and 2022 also noticed a decreased trend of childhood stunting from 27.7% to 24.4%, then 21.6% (Ministry of Health Indonesia, 2021, 2022; Sudikno et al., 2019). This average yearly decrease needs to be accelerated to achieve a 14% stunting prevalence by 2024, as targeted by the Indonesian government (The National Medium-Term Development Plan for 2020-2024, 2020). According to Indonesian Basic Health Research 2018, East Java is one of the 18 provinces with stunting prevalence higher than the national average (Balitbangkes Kemenkes RI, 2018). Surabaya City is included in the 260 districts/cities designated priority locus for stunting prevention in East Java for 2020 (Perpres Nomor 61 Tahun 2019 Tentang Rencana Kerja Pemerintah Tahun 2020, 2019).
Children are defined as stunted if their height for age is above two standard deviations below the WHO Child Growth Standards median for the same age and sex (WHO, 2014b). Inappropriate child-caregiving practice during their critical period (6–23 months old) increases the risk of stunting by up to 42% when they reach 24–35 months old (Satriawan, 2018). Stunting has short-term and long-term consequences in the child’s life. Stunted children will struggle to reach their ideal height and weight (WHO, 2015). Stunting makes future generations become the lost generation as it increases morbidity and mortality, reduces the potential for physical growth (short as an adult), reduces the development of cognitive and neurological functions (stunted brain), and increases the risk of chronic disease as adults (Onis & Branca, 2016). Therefore, providing appropriate care for children needs to be improved.
Children depend on others in their families, especially mothers, for nutrition, safe housing, stimulation, and healthcare (Tome et al., 2021). Maternal caregiving capabilities are the mother’s characteristic which determines her ability to care for their children, to support their healthy and optimum growth and development. Maternal caregiving capabilities include perceived physical health, psychological well-being, social support, decision-making, and empowerment (Matare et al., 2015). Maternal caregiving capabilities allow mothers to utilize skills and resources for their child’s health (Mchome et al., 2020).
Previous studies have explained that the quality of maternal caregiving capabilities affects a mother’s ability to adopt appropriate child-caregiving practices (Ickes et al., 2018). Maternal caregiving capabilities relate to appropriate child-feeding practice as recommended by the WHO (Matare et al., 2021) and the child’s linear growth (Tome et al., 2021). However, maternal caregiving capabilities have yet to become a strategic issue that has been explored in childcare practices as an effort to prevent childhood stunting.
Appropriate child-caregiving behavior to prevent childhood stunting is influenced by maternal caregiving capabilities. Meanwhile, maternal caregiving capabilities are influenced by child, mother, husband, and household factors (Martin et al., 2021; Matare et al., 2021). The maternal caregiving capabilities model based on the UNICEF model of care is expected to improve mothers’ ability to care for their children to prevent childhood stunting, including providing proper diet and stimulation and a healthy living environment such as water, sanitation, and hygiene (Engle et al., 1997; Peter & Kumar, 2014).
Review of the Literature
The complementary feeding period, generally 6–23 months, represents an important period of sensitivity to stunting with lifelong, possibly irreversible consequences (Prendergast & Humphrey, 2014). During this period, children learn to consume food besides breast milk. The food consistency and variety are gradually increased as the infant gets older, adapting to their requirements and abilities. If they are given inappropriately, a child’s growth may falter (D’Auria et al., 2020). Growth faltering begins to be detected when children reach 12–23 months of age. If this condition persists over time, a child’s height will be lower than that of children of the same sex in their age group (Alderman & Headey, 2018). When their height for age is above two standard deviations below the WHO Child Growth Standards median for the same age and sex, they are called stunted children.
The primary strategy to prevent childhood stunting is through the family approach, as the main microsystem of children is their family. Children cannot fulfill their nutritional needs alone, so they depend on their parents (Dijk et al., 2018). In Indonesia, the mother is the family member responsible for all household activities, including providing care for their children (Hardisman, 2011). Resources available to them may play a pivotal role in determining care behaviors (Basnet et al., 2020). Therefore, mothers play an important role in their child’s health and nutritional conditions (Beal et al., 2018; Kunto & Bras, 2018). Mothers can contribute significantly to childhood stunting prevention by adopting appropriate child-caregiving practices as well as possible. Interventions to optimize child growth (such as child-feeding and caregiving practices) rely heavily on the mother’s implementation. The differences in the quality of care children receive allow for heterogeneity in nutritional status even though the children live in a community with the same resources (Tome et al., 2021).
According to the Extended UNICEF Model of Care, care is important for children’s growth and development. Lack or inadequacy of resources for care can constrain appropriate caregiving (Basnet et al., 2020). The caregiver needs sufficient resources and capabilities to manage resources, to perform adequate care practices (Engle et al., 1999; Ruel & Menon, 2003). Maternal caregiving capabilities are the psychosocial characteristics of the mother that underlie her abilities to look after their children so they will be healthy and grow optimally. Maternal caregiving capabilities allow mothers to utilize the skills and resources for child health (Mchome et al., 2020). Maternal caregiving capabilities are important to support child growth and development (Peter & Kumar, 2014).
Maternal caregiving capabilities have five dimensions: perceived physical health, psychological well-being, social support, decision-making, and empowerment (Matare et al., 2015). Perceived physical health is defined as the mother’s perception that she is healthy and disease-free (Engle et al., 1997; Tome et al., 2021). Psychological well-being is defined as the level of a mother’s satisfaction with a variety of attributes: life overall, food, housing, income, health, work, perceived safety (personal and community), freedom from physical violence, education, dignity, ability to help others, and freedom to express their spiritual beliefs (Ickes et al., 2018). Social support is defined as access to relationships that provide positive physical, psychological, and informational resources, which help the mother feel she belongs, is competent, and can overcome the problems encountered (Tome et al., 2021). Decision-making is defined as choice or control in decisions, and access to resources affects mothers and their children (Dixon-Mueller, 2013). Empowerment is defined as a mother’s ability to claim available resources, have a voice for their aspiration, control, participate in decision-making, and act on her wishes to improve her life (Has et al., 2022; Kabeer, 1999). Mothers with high-quality maternal caregiving capabilities are physically and mentally healthy, have positive social support, have high decision-making ability in the household, and have a high empowerment level (Taylor et al., 2015; Tome et al., 2021).
High maternal caregiving capabilities are strategic to improve childhood stunting preventive behavior, including healthy eating patterns, proper parenting, and healthy environmental sanitation (Saleh et al., 2021). Health promotion to improve the quality of maternal caregiving capabilities to prevent childhood stunting is urgently needed in the family setting (Hardisman, 2011). This study aimed to develop a model to enhance maternal caregiving capabilities in preventing childhood stunting based on the UNICEF model of care.
Method
Design
The study used an analytical observational design with a cross-sectional approach. The researchers evaluate the influences between variables without any intervention. The data was collected at a single point without further follow-up.
Research Questions
There were two main research questions: what factors influence the enhancement of maternal caregiving capabilities based on the UNICEF model of care in preventing childhood stunting? And how is the model to enhance maternal caregiving capabilities based on the UNICEF model of care in preventing childhood stunting among 6–23-month-old children?
Sample and Settings
The population was a pair of mothers and their youngest 6–23-month-old children, who are registered at Posyandu (Community-based Integrated Health Care Center) in Surabaya City, East Java, Indonesia. The sample size was calculated based on the rule of thumb for SEM-PLS (Structural Equation Modeling-Partial Least Square). The minimum sample size is 5–10 times the estimated parameters. The researcher used it 25 times (Jhantasana, 2023). A total of 600 respondents is required to reach the level significance of 95%, taken using cluster sampling technique across seven healthcare centers in Surabaya City, East Java, Indonesia.
Variables/Instruments
The variables in this study were child factors, mother factors, father factors, household factors, maternal caregiving capabilities, and nutritional behavior to prevent childhood stunting. A packet of questionnaires was used as an instrument to gather the data.
All instruments have gone through the back-translation process. The back-translation process involved two bilingual translators (Bahasa–English) and the researcher. Firstly, the researcher translates the original instrument from English to Bahasa. The first translator then translates the researcher’s translation back from Bahasa to English. The second translator then translated the English version of the first translator into Bahasa. Comparison and correction were checked between the original instrument and the second translator’s translation results. The researcher wrote the final translation from the original language (English) to Bahasa based on corrections and discussions with the two translators.
All instruments were statistically tested for their validity and reliability. It involved 25 mothers with similar characteristics to the sample, which will not become the research’s samples. The R-table used is the R-table product moment for 25 respondents, with a significance level of 5% (>0.396). Results show that all question items in the questionnaire are valid and reliable.
Child factors include the child’s age, sex, gestational age at birth, birth weight, birth length, birth order, history of exclusive breastfeeding, age of first complementary feeding, and history of infection in the past three months. The child’s age was divided into three groups: 6–11 months old, 12–17 months old, and 18–23 months old. The child’s sex was male and female (Has et al., 2022). Gestational age at birth was divided into preterm (<37 weeks) and a term ( ≥ 37 weeks) (WHO, 2018). Birth weight was divided into low birth weight (<2,500 g) and normal ( ≥ 2,500 g) (WHO, 2014a). Birth length was divided into small for gestational age (<48 cm) and normal ( ≥ 48 cm) (Judiono et al., 2023; Kemenkes RI, 2011). Birth order was divided into six groups: the first, second, third, fourth, fifth, and sixth children. The history of exclusive breastfeeding was divided into no (<6 months) and yes (≥6 months). The age of first complementary feeding was divided into too early (<6 months) and appropriate (6 months) (Permenkes RI No 41 Tahun 2014 Tentang Pedoman Gizi Seimbang, 2014). The history of infection in the past three months was divided into four groups: often (≥6 times), sometimes (3–5 times), rarely (1–2 times), and never (0) (Suiraoka et al., 2011).
Mother and father factors include the mother’s age, level of education, working status, height, and body mass index. Age was divided into eight groups: 15–19 years old, 20–24 years old, 25–29 years old, 30–34 years old, 35–39 years old, 40–44 years old, 45–49 years old, and ≥50 years old (Has et al., 2020). The level of education was divided into five groups: never attended any formal education, attended primary school, junior high school, senior high school, and university or higher. Working status was divided into five groups: civil servant, private employee, entrepreneur, farmer, and unemployed. Height was divided into short (<159 cm for mother and <168 cm for father) (WorldData.Info, 2019). Body mass index was divided into five groups: severe underweight (<17), underweight (17.0–18.4), normal (18.5–25.0), overweight (25.1–27.0), and obese (>27) (Permenkes RI No 41 Tahun 2014 Tentang Pedoman Gizi Seimbang, 2014).
Household factors include the number of under 5-year children in a household, economic level, living areas, hygiene and sanitation, and food security status. The number of children under five in a household was divided into 1 or >1. The economic level was divided into low (less than the minimum regional wage of Surabaya, IDR 3,500,000) and high (greater than or equal to the minimum regional wage of Surabaya). Living areas were divided into rural, peri-urban, and urban (Siswanto et al., 2014). Hygiene and sanitation were divided into good (score = 16) or not good (score <16) (Rizal, 2018). Food security status was divided into four groups: food insecure severe hunger (score 8–18), food insecure moderate hunger (score 3–7), food insecure no hunger (score 1–2), and food secure (0) (Septiani et al., 2021; USDA, 2012).
Maternal caregiving capabilities include perceived physical health, psychological well-being, social support, decision-making, and empowerment. Perceived physical health was assessed by using a questionnaire adapted from the RAND 36-item health survey classified as unhealthy (T < median) and healthy (T ≥ median) (Hays et al., 1993). The psychological well-being questionnaire was adopted from The OECD Guidelines on Measuring Subjective Well-being and classified as negative (T < median) and positive (T ≥ median) (Ickes et al., 2018). The social support questionnaire adopted from The Duke-UNC Functional Social Support Questionnaire was classified as weak (T < median) and strong (T ≥ median) (Broadhead et al., 1988). The decision-making power was assessed by using a questionnaire adapted from the Demographic Survey and Indonesian Health, classified as weak (T < median) and strong (T ≥ median) (Kementrian Kesehatan RI, 2018). The empowerment questionnaire was adopted from Cantril’s Self-Anchoring Striving Scale and classified into low (T < median) and high (T ≥ median) (Ickes et al., 2018).
The nutritional behavior to prevent childhood stunting was measured from (1) minimum dietary diversity (MDD); (2) minimum meal frequency (MMF); and (3) minimum acceptable diet (MAD). The MDD is defined as the proportion of children aged 6–11 months who receive food at least from four of seven groups of food, as follows: (1) grains, roots, and tubers; (2) legumes and nuts; (3) dairy products (milk, yogurt, and cheese); (4) flesh foods (meat, fish, poultry, and liver/organ meats); (5) eggs; (6) vitamin-A rich fruits and vegetables; and (7) other fruits and vegetables. The MMF was defined as a 6–11-months-old child who received solid, semisolid, or soft foods (including milk feeds for non-breastfed children) in minimum frequency in the last 24 hr before the interview, which differed by child’s age and their breastfeeding status. The guide for MMF was as follows: (1) a breastfed 6–9-months-old child should get solid/semisolid food at least twice a day; (2) a breastfed 9–23-months-old child should get solid/semisolid food at least three times a day, and (3) a non-breastfed 6–23-months-old child should get solid/semisolid food at least four times a day. The MAD combines MDD and MMF with different criteria between a breastfed and non-breastfed 6–11-month-old child. Data are then classified as good (if the nutritional behavior complies with the WHO guidelines), and not good (if the respondents did not comply) (WHO, 2010).
Data Collections
Data collection was carried out over from June to August 2022. The research team (members of three) and two enumerators were involved in the data collection process. The enumerators have completed their bachelor’s in nursing education. The questionnaire packet, which consists of six sections, required approximately 60 min to be completed. It was distributed door to door by the researcher and enumerators, accompanied by local health volunteers with a level of education of senior high school graduates at minimum. Before the data collection process, the researcher conducted a briefing to ensure the similarity of perceptions. Each respondent was visited once without further assessment.
Data Analysis
The data obtained were then analyzed statistically. Descriptive analyses used were frequency and percentage. The inferential analysis used is a variance-based or component-based structural model called Partial Least Square (PLS) Regression using SmartPLS software. This analysis is used to predict the dependency variable (nutritional behavior to prevent childhood stunting) based on a variation of several independent variables (child factors, mother factors, father factors, household factors, and the dimension of maternal caregiving capabilities).
The first step in evaluating PLS-SEM results involves examining the measurement models. The relevant criteria differ for reflective and formative constructs. Researchers assess the structural model if the measurement models meet all the required criteria. Hypothesis testing is done by statistical test t. If the test results obtained a value of >1.96 (alpha 5%) it means significant testing, and if the value t < 1.96 means the test is not significant.
Ethical Consideration
Participation in this study was voluntary. The information regarding this study was provided, and written informed consent was sought from all respondents before participation. To maintain confidentiality, respondent names were not recorded, but we changed it into code. The respondents also had the right to discontinue participation during the data collection. There were no negative consequences or repercussions regarding their refusal. The Health Research Ethics Committee of the Faculty of Nursing, XXX, granted ethics approval for this study.
Results
The samples were collected from seven different healthcare centers (puskesmas) in Surabaya City, including Mulyorejo (100 people; 16.67%), Klampis Ngasem (100 people; 16.67%), Tenggilis (100 people; 16.67%), Pacar Keling (100 people; 16.67%), Ketabang (50 people; 8.325%), Dupak (50 people; 8.325%), and Kalijudan (100 people; 16.67%). Data collection was carried out from August to October 2022.
Table 1 shows the child factors, which can be described that respondent’s children are 12–17 months old (37.7%), were female (51.0%), had a term on delivery (83, 3%), had normal birth weight (93.7%) and birth length (84.7%) and were a second child in their family (39.3%). The average child’s birth weight is 3,057 g, and the birth length is 49.34 cm. Most were not exclusively breastfed (71.8%). Most (91.0%) got the first complementary food at the appropriate time. Only 22.2% of children reported by their mothers never suffered from an infectious disease (such as cough, influenza, fever, or diarrhea) in the last three months. The tendency for children to suffer from infection is relatively high. On average, children have had an infection 1.51 times in the last three months.
Frequency and Percentage Distribution of the Child Factors (n = 600).

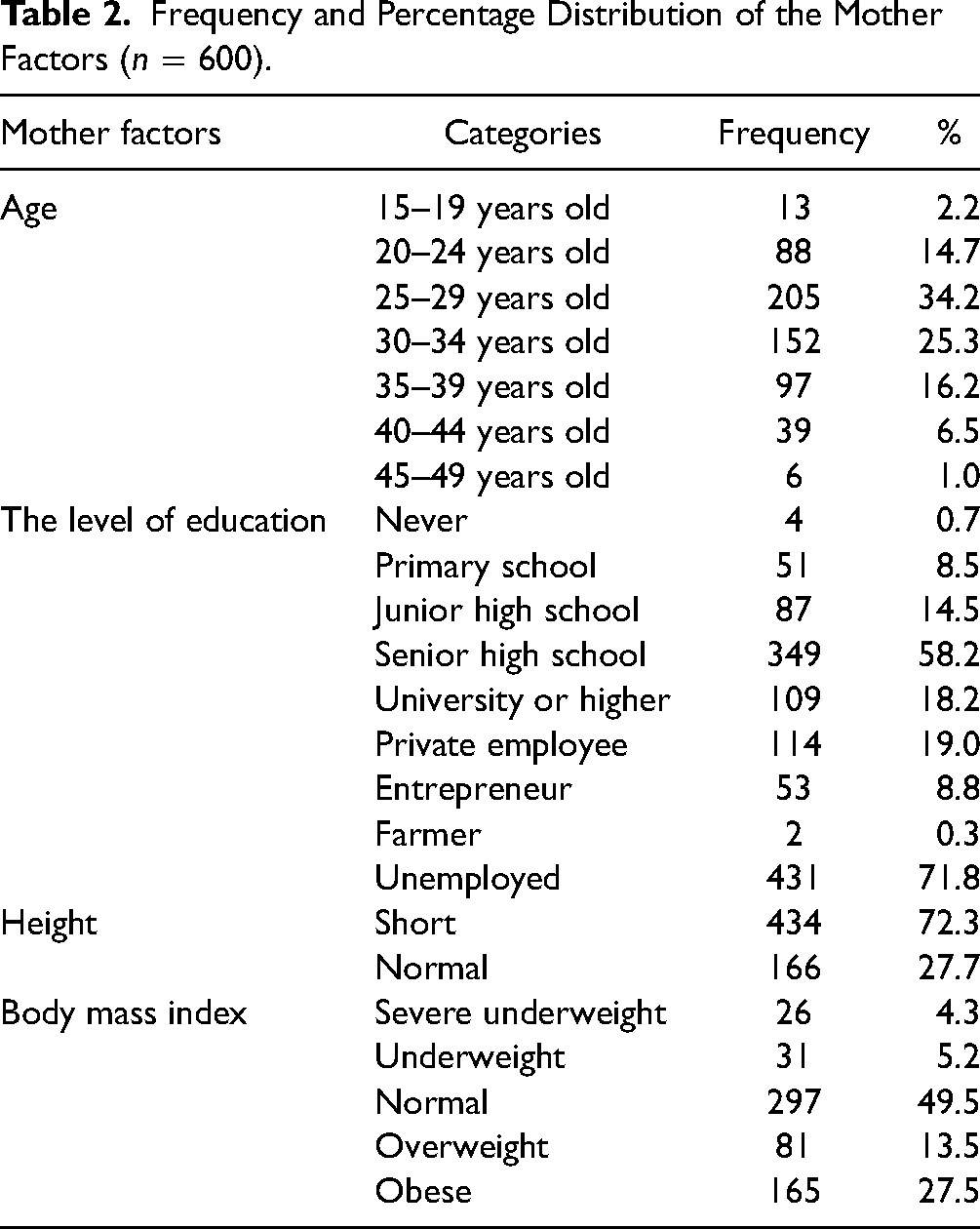
Many mothers were aged 25–29 years old (34.2%), junior/high school graduates (72.6%), and unemployed (71.8%). Most (72.3%) mothers have a short height (<159 cm). The average height of the mothers was 155.5 cm. More than 50% of mothers were in the high Body Mass Index (BMI) category (40.0%), with an average BMI of 24.49 and a body weight of 59.038 kg. See Table 2 for mother factors.
Frequency and Percentage Distribution of the Mother Factors (n = 600).
According to Table 3, the highest proportion were fathers aged 30–34 years old (27.7%), junior/high school graduates (77.7%), and worked as private employees (66.0%). More than 50% (51.7%) of fathers have a short height (<168 cm). The average height of the father was 166.68 cm. Many fathers were in the high BMI category (40.5%), with an average BMI of 24.20 and a body weight of 67.25 kg. While Table 4 shows that most respondents only have one under-5-year-old child at home (88.5%), with low economic levels (62.7%) and live in urban areas (74.8%). More than half of respondents have poor house sanitation (58.2%) and live in food-insecure families (64.3%).
Frequency and Percentage Distribution of the Father Factors (n = 600).

Frequency and Percentage Distribution of the Household Factors (n = 600).

Table 5 informs that many mothers still perceived their physical health as unhealthy (49.2%) and had weak social support (48.5%). Although decision-making autonomy is more than 50% in the strong category, 49.2% of mothers still have weak decision-making autonomy. There are still 47.5% of mothers who have a low level of empowerment. While Table 6 shows most respondents (73.0%) provide meals for their children that meet the MDD recommended by WHO, only half of the respondents meet the child’s MMF (55.0%). Moreover, less than half of respondents meet their child’s MAD (36.2%).
Frequency and Percentage Distribution of Maternal Caregiving Capabilities (n = 600).

Frequency and Percentage Distribution of Nutritional Behavior to Prevent Childhood Stunting (n = 600).

For the measurement of the outer model, a face validity assessment was conducted by observing the correlation between indicators and latent variables in the previous studies, which proved significant and robust. Several indicators had insignificant outer weight values <0.20 (P > 0.05). Deletion was performed on insignificant outer weight indicators. The composite reliability score of each indicator is >0.6, and the AVE value is >0.5, which means that all indicators are reliable and valid in measuring the model’s variables. The value of cross-loadings indicated that each indicator obtained a lower correlation value with other latent variables than the latent variable itself.
The inner model’s measurement obtained the average R-square of 0.060, which meant that the exogenous variable could explain endogenous variables. The average variance extracted is 0.670. Then the goodness of fit index (GoF) score is 0.273. It means that the model obtained a good fit. The inner and outer measurement results show that the model can explain the correlation between exogenous and endogenous constructs.
The PLS analysis results demonstrated a significant effect of child factors on maternal caregiving capabilities (path coefficient = 0.100, t = 2.605 (>1.96)). The first age of complementary feeding was the indicator that significantly affected child factors to maternal caregiving capabilities. Mother factors also significantly influenced maternal caregiving capabilities (path coefficient = 0.171, t = 3.800 (>1.96)). The indicator that contributed a significant effect on mother factors on maternal caregiving capabilities is the mother’s level of education. Father factors did not contribute a significant effect on maternal caregiving capabilities (path coefficient = −0.036, t = 0.736 (>1.96)). Household factors have a significant effect on maternal caregiving capabilities (path coefficient = 0.396, t = 10.338 (>1.96)). Indicators that contributed a significant effect on household factors on maternal caregiving capabilities are economic level and food security. The analysis results indicated maternal caregiving capabilities’ effect on nutrition behavior in preventing childhood stunting (path coefficient = 0.111, t = 2.493 (>1.96)). Indicators that significantly affected maternal caregiving capabilities on nutritional behavior in preventing childhood stunting are perceived physical health, psychological well-being, and decision-making autonomy, while the indicators that construct nutritional behavior in preventing childhood stunting are dietary diversity, meal frequency, and acceptable diet (See Figure 1 and Table 7).

Path of model to enhance maternal caregiving capabilities in preventing childhood stunting among 6–23-month-old children based on the UNICEF model of care.
Hypothesis Testing Result.
Discussion
Child, mother, and household factors influenced maternal caregiving capabilities. Child factors contributing to maternal caregiving capabilities are the age of first complementary feeding. Most children in this study start their complementary feeding at six months old. A previous study stated that complementary feeding, recommended by WHO to be given to their children when they reach six months old, not only benefits for children but also the mother. As many variables affect complementary feeding, a mother must hardly decide when and how it begins (Amalia et al., 2022; Wahed et al., 2022). Although mothers have quite a lot of power over child-feeding decisions on the household level, the older generation and fathers also influence feeding choices (Purwaningtyas et al., 2019). Fathers decided how money was spent in the household, and grandmothers tried to maintain the traditional ways of child care (Nousiainen, 2014). This allows the mother to elaborate on her knowledge and skill regarding complementary feeding and experience negotiation with her spouse or older generation until she finally decides when she first introduces the complementary food to their children. Directly, it also can increase their maternal caregiving capabilities.
The study found that the mother factor contributing to maternal caregiving capabilities is education. Most mothers in this study finished their secondary high school level, either junior or senior high school. Educated mothers are more capable of accessing available health facilities and have enough knowledge about child nutrition. Better-educated women also have more say in family decisions (Rahman et al., 2015). Previous studies revealed that higher levels of maternal education were associated with various health-related parenting behaviors and more advantageous health investment behaviors during early childhood (Mauludyani & Khomsan (2022); Prickett & Augustine, 2016). It also leads to better care practices which contribute to child well-being (Sarkar et al., 2023). As a primary caregiver for their children, a mother needs sufficient capabilities to manage resources to perform adequate care practices, including better education.
Household factors indicators that significantly contribute to maternal caregiving capabilities are economic level and food security status. Most respondents in this study were living in a low economic level family with a monthly income less than Surabaya City minimum wage. More than half of respondents live in food-insecure families. These two indicators were related to each other. Poverty and household food insecurity make mothers unable to provide adequate dietary intake and to provide and sustain adequate care (Jonah et al., 2018). A previous study found that poverty influences mothers’ cognitive performance and critical thinking, especially in decision-making. It also influences the mother’s key behavioral pattern, such as whether one is likely to act in line with the goals and what kinds of risks will be taken to achieve them. Mothers living in poverty tend to have negative self-appraisal, which bothers their ability to navigate life challenges, including caregiving for their children (Sheehy-Skeffington & Rea, 2017). Household food insecurity also forced mothers to maintain their child’s food supply by creatively changing their daily habits in nutrition, such as decreasing protein foods (e.g., meat, eggs, beans), fruits, and vegetables and increasing grain and starches consumption (Burke et al., 2017; Drucker et al., 2019).
Maternal caregiving capabilities strongly affect mothers’ nutritional behavior to prevent childhood stunting among 6–23-month-old children. Indicators contributing to it are perceived physical health, psychological well-being, and decision-making autonomy. A previous study found that self-perceived health concerns correlate with one’s dietary patterns, which means health concerns can be an essential predictor of dietary behavior, especially for women (Jezewska-Zychowicz et al., 2017). In Indonesia, mothers are the primary nutrition providers and care for young children. This demanding task needs good physical and mental health. Vice versa, poor mental health in mothers might cause them to be less able to provide appropriate care to their children, which later has adverse consequences on their children’s health (Ickes et al., 2018; Rahman et al., 2008). Women with greater control in deciding how household resources are to be used are more capable of maintaining and improving the nutrition and health of themselves and their children (Rahman et al., 2015; Synthesa & Hartono, 2023). These three things are needed to boost the mother’s ability to provide appropriate infant and young child-feeding practices to prevent childhood stunting in early life.
Strengths and Limitations
This study has a limitation which must be considered when interpreting the result. The cross-sectional design limits our ability to draw causal inferences and to establish temporality. However, the study has strengths which include: (1) the number of respondents involved in this study is high; (2) the instrument used was internationally standardized with high validity and reliability; and (3) studies examining maternal caregiving capabilities in South-East Asia setting are still lacking.
Implications for Practice
The highlighted novelty aspect of this study is the model to improve mothers’ maternal caregiving capabilities to increase nutritional behavior to prevent childhood stunting, based on the UNICEF model of care. The model’s development should pay attention to child factors, mother factors, and household factors that can influence maternal caregiving capabilities. Then maternal caregiving capabilities will shape the mother’s expected nutritional behavior in preventing childhood stunting. This model also can be used by nurses as the nursing intervention of Family Nursing Care for families with children under 5 years old, as an effort to prevent stunting.
Conclusions
Child factors, mother factors, and household factors influence maternal caregiving capabilities. Maternal caregiving capabilities have a single and strong effect on proper nutritional behavior to prevent childhood stunting among 6–23-month-old children. Nursing interventions to increase maternal caregiving capabilities can consider its components, especially perceived physical health, psychological well-being, and decision-making autonomy. The improvement of mothers’ maternal caregiving capabilities is expected to increase their ability to implement appropriate nutrition behavior to prevent childhood stunting as early as possible.
Footnotes
Acknowledgments
The authors gratefully acknowledges staff and local health volunteers of Puskesmas Mulyorejo, Klampis Ngasem, Tenggilis, Pacar Keling, Ketabang, Dupak, and Kalijudan, East Java Province, Indonesia, who assisted the researcher in data collection. The author also wishes to thank all respondents involved in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Participation in this study was voluntary. The information regarding this study was provided, and written informed consent was sought from all respondents before participation. To maintain confidentiality, respondent names were not recorded, but we changed it into code. The respondents also had the right to discontinue participation during the data collection. There were no negative consequences or repercussions regarding their refusal. The Health Research Ethics Committee of the Faculty of Nursing, Universitas Airlangga, granted ethics approval for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Research and Technology/National Research and Innovation Agency (Indonesia) through Higher Education Basic Research Scheme (PDUPT), (grant number 964/UN3.15/PT/2022).