
Abstract
Introduction
Obesity in adolescence is a significant ongoing public health problem that has not improved over the past decade.
Objective
This descriptive qualitative study explores the perspective of female adolescents who are overweight or obese regarding their views on health and weight within the clinic setting.
Methods
In-depth interviews were conducted with female adolescents (age 13–19 years old; BMI ≥85th percentile) from the mid-west region of the United States (N = 28). Inductive thematic analysis using Braun & Clarke’s methods was utilized.
Results
The findings from this study revealed that the adolescents’ view of health encompasses physical, mental, and psychosocial health dimensions, and despite being overweight and obese, the participants felt healthy. Participants discussed the need to eat healthier and increase their daily physical activity, but were unable to transform this into action. Within the clinical setting, the adolescents were sensitive to weight discussions.
Conclusion
Results from this study can increase providers’ understanding of the adolescent, increase awareness of adolescent sensitivity, and assist researchers in developing age-appropriate interventions for effective treatment and prevention of childhood obesity.
Introduction
Obesity in American youth has reached epidemic proportions and is a significant public health problem (Ogden et al., 2018). The prevalence of adolescents who are obese (age 12–19 years, 20.5%) is greater than school-aged children (age 6–11 years, 17.5%) and preschool-aged children (age 2–5 years, 8.9%) who are obese (Ogden et al., 2015). Despite health care and clinical research efforts, adolescent obesity rates have not decreased over the past decade (Ogden et al., 2018).
Review of Literature
The increased incidence of adolescents with obesity reinforces the ongoing need for effective health care services to alleviate the short- and long-term health risks associated with obesity. Obesity significantly affects female adolescents’ physical, social, and psychological health (Morinder et al., 2011; Muhlig et al., 2016). Youth who are obese face increased morbidity and mortality in adulthood (Caprio et al., 2017; Rajjo et al., 2012) and report increased levels of depression, anxiety, bullying, and stigmatization (Buttitta et al., 2014; Levy & Pilver, 2012; Puhl et al., 2011).
Over the past decade health care efforts have been unsuccessful in decreasing obesity rates amongst youth (Al-Khudairy et al., 2017; Skinner & Skelton, 2014). As many of the pediatric weight management programs have been developed by adults in health care and research, questions have arisen about if the programs are meeting the adolescents’ needs and wants. Oftentimes, health care providers (HCPs) do not hold the same perspectives on health and illness as their patients (Menez et al., 2013). HCPs may not have the same health goals or similar measures of what constitutes weight management success as their patients (Teixeira et al., 2012). Developmental differences in weight loss goals, motivations, and behaviors could potentially impact the effectiveness of weight loss outcomes.
Gender is well established as a category of analysis in health care, and is an emerging area of research (Baggio et al., 2013) that influences the way obesity is experienced and how it effects health management (Garaigordobil et al., 2009; Patton et al., 2016). Past research demonstrates that adolescent health programs with a focus on individual behavior change have had limited success (McGovern et al., 2013). Lack of success in behavior change may be due to not incorporating the adolescent gendered perspective on health and weight. Many programs only addressed the physical components of health and did not ask the adolescents about how they felt about their health or weight.
The adolescent perspective on obesity and treatment has recently emerged. Adolescents with obesity hold diverse perceptions of causation for their obesity. In a systematic review, adolescents’ perceptions of obesity, the causes of obesity, and the clinical setting indicated insufficient understanding of the adolescent’s interpretation of their health and weight (Lachal et al., 2013). The divergence between the adolescent’s and a health care provider (HCP) perception of health and weight has the potential to undermine their healthcare relationship (Lachal et al, 2013; Øen et al., 2018).
The purpose of this study was to explore the perspective of female adolescents with overweight or obesity regarding their views on health and weight, and also how these concepts impact their experience within the clinical setting. This approach is consistent with child development principles (Erikson, 1963; Hamilton et al., 2004) and viewed within the socio-ecological model where youth are situated in families and societies (Brofenbrenner, 1979). Results from this study can assist providers and researchers to create effective weight management programs that match treatment plans to adolescent expectations and needs.
Methods
Design
Qualitative methodology permits researchers to describe and interpret participant experiences of specific phenomena in certain contexts. Individual interviews were utilized to gather female adolescents with obesity perspectives on health, weight, and weight management in the clinical setting. To identify and analyze patterns in the data Braun and Clarke's (2006) method of thematic analysis was used.
Study Setting, Participants, and Recruitment
The study was conducted in the Midwestern United States, representing moderate-sized urban cities, surrounding suburban areas, and rural communities. Recruitment of participants occurred in pediatric and adolescent specialty clinics that provided care for youth with overweight and obesity. Participants included female adolescents, aged 13–19 years old, English speaking, and who had a BMI ≥85th percentile for gender and age (Centers for Disease Control and Prevention (CDC), 2018). They all had at least one outpatient clinical encounter in the previous year. Participants with a history of an eating disorder were excluded from the study.
Recruitment flyers were also posted in public spaces such as libraries and cafes. Potential participants could call a phone number if interested in the study and the first author would follow up and discuss the study with them. Recruitment also occurred in the clinical setting, within clinics that provide care for children and adolescents with obesity. Nurses at the clinics provided informational handouts to prospective participants that described the study. Since the terms overweight and obesity have been found offensive to adolescents, these terms were omitted from the recruitment materials (St. George et al., 2013; Puhl et al., 2012). If the adolescent/parent indicated interest in learning more about the study and possible participation, the nurses in the clinic collected the adolescent’s name and phone number so the study investigators could contact them. If the adolescent was 13–17 years old, a parent/guardian’s signature was required. The first author then made telephone contact with the adolescent and/or guardian and provided detailed information to all parties.
A time and date for an interview was scheduled with the potential participants at a location of their choice, such as in their home or a public café. For participants aged 13–17 years old a parent/guardian was required to be present at the beginning of each meeting. Snowball sampling did occur for one participant.
Ethical Considerations
The University of Wisconsin - Milwaukee Institutional Review Board reviewed and approved this study. Upon meeting with adolescents aged 18–19 years old, written informed consent was obtained. When meeting with adolescents aged 13–17 years old, written informed consent was obtained by the parent or legal guardian and verbal informed assent was obtained by the adolescent and.
Interviews
The first author met with all potential participants and parents to discuss and obtain informed assent and consent. The parent was then asked to leave the room, providing privacy for the interview. The interviewer was a female nurse experienced in health promoting conversations and health care of adolescents with overweight and obesity. Interviews were undertaken with an empathetic and kind demeanor and began with general questions about the participant to allow for rapport to develop. Interviews used client-centered conversation and open-ended questions regarding the meaning of health, the meaning of weight, and the participant’s experiences within the clinical setting. Interviews lasted 40–65 minutes and were recorded. Adolescents were offered a $25 gift card in acknowledgement of their time. Immediately following each interview, the first author transcribed the recordings verbatim, including utterances and pauses. When codes and emerging themes became saturated, and no new data had emerged in the final three interviews (as determined by two authors), recruitment was halted.
Data Analysis
There were 28 total participants. Immediately after all interviews, as part of the self-reflexivity process, the first author began writing down her reflections on the interviews and analysis process. This continued throughout the entire analysis. Braun and Clarke’s (2006) six phase thematic analysis process was used to analyze the data. Phase 1: Familiarizing yourself with the data. The first author continued to familiarize herself with the data by reading and re-reading the entire data multiple times. Initial thoughts and possible codes were written down, and relevant passages of text were noted. Phase 2: Generating initial codes. The first two authors independently open-coded all interview transcripts. Codes were discussed, adjusted, and renamed until consensus was reached. Phase 3: Searching for themes. Codes were merged into category systems. The first two authors noted preliminary themes that were representative of the data. Emerging themes were compared to strengthen the credibility of the analysis. Phase 4: Reviewing themes. Themes were continually checked across single transcripts and the entire data set. Ongoing conversations between the first two authors occurred regularly throughout the analysis process to. Phase 5: Defining and naming themes. Themes began to be refined and defined until the final themes were given names that reflected their general meaning. Theme names were extracted from participant’s words, to honor and elevate the participant voice. Phase 6: Producing your report. Results were written that included chosen text extracts that best represented the various themes.
Results
Demographics (see Table 1)
Participants had the option to provide demographic data, and one participant elected not to share her height and weight. Participants’ ages ranged from 13 to 19 years (mean =15.8, SD = 1.86) and were enrolled in 7th grade through freshman in college (median = 10th grade). The adolescents self-reported weight ranged from 135 to 361 pounds (mean = 204.8 pounds, SD = 10.5 pounds), and ranged from the 85th to >99th percentile (mean = 94th percentile, SD = 0.8). Based upon CDC criteria a majority of participants (64%) were categorically “obese” and the remaining 36% categorically “overweight.” The participants reported they had been living with increased weight for an average of 5–6 years (with answers ranging from “1–2 years” through “all my life”).
Demographic Characteristics of Participants (n = 27).a
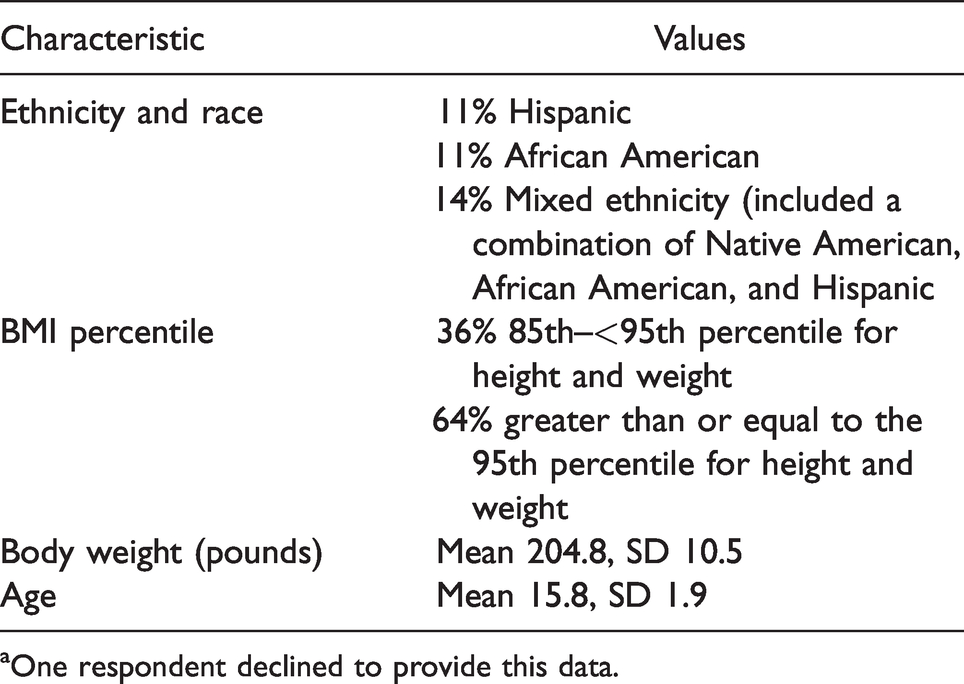
aOne respondent declined to provide this data.
Though efforts were made to recruit a diverse sample of adolescents, a majority of the participants (64%) were Caucasian, with the remaining 36% comprised of a variety of ethnicities and cultural groups: Mixed ethnicity (14%) African-American (11%), and Hispanic (11%). The area where recruitment occurred has a similar ethnic compilation. All participants reported attending at least one clinical encounter in the previous year.
Interviews
Four themes emerged from the data demonstrating the participant’s perspectives on health and weight: Health is like a physical, mental, and social balance; Food and physical activity ideals; Weight is more than a number; and I can be healthy but bigger (see Table 2)
Four Themes.
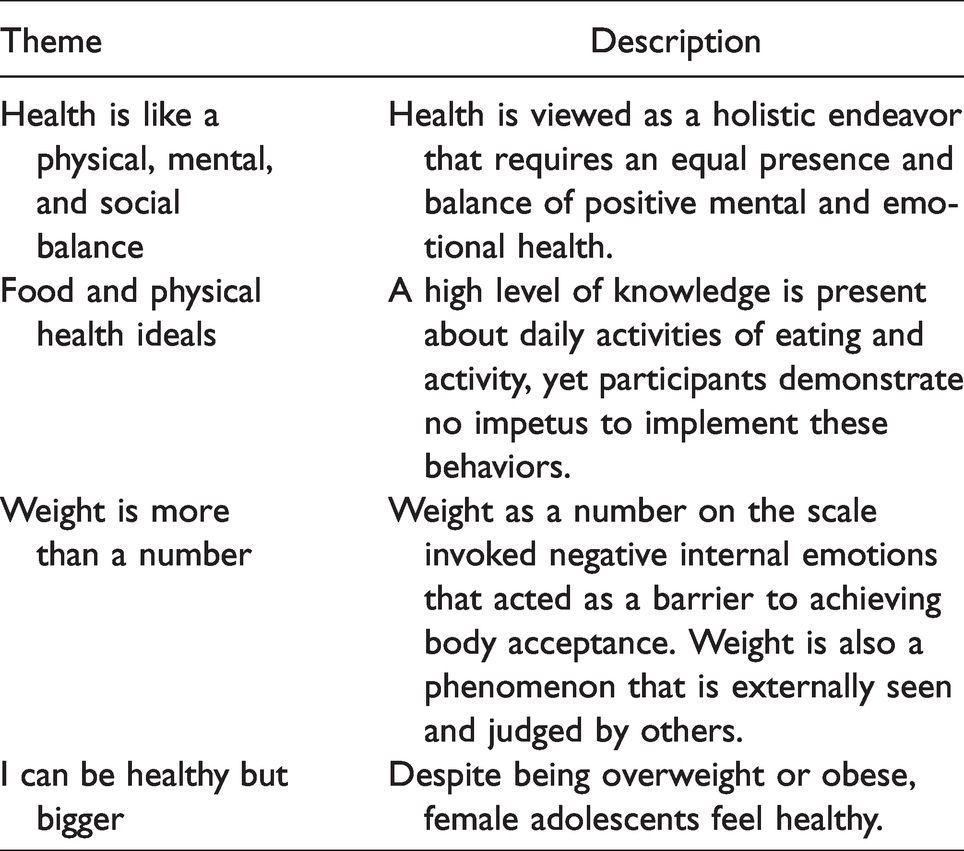
Theme 1: Health is like a physical, mental, and social balance.
The majority of the participants illustrated a holistic view of health that included aspects of physical, mental, social, and emotional health. A participant shared, “There’s like physical health and then there is mental/emotional health. There’s one more health, um … (pause) social health! I think [health is] a good balance of all three of them. So you can’t just be like really good at one of them and horrible at the other two (Participant #13, age 15).” Mental health was especially prevalent in the transcripts and a strong focus of conversations. Participants described how taking care of themselves involved actions they could take to improve their physical health, and also required coping with the stresses of daily life, staying positive, and maintaining relationships with others.
This perspective also influenced the way participants viewed health care. Health care was not just about physical complaints, infectious disease, or medical prescriptions; it included things that could affect one’s thinking, mood, or behavior such as anxiety or depression. This is reflected in the statement, “A lot of people I think consider health care primarily in like, physical. So like, they think about diseases, stuff, and medications. But um, I don’t know, at least for me it’s really important – mental health care. Because I mean like anything that affects a person’s like day-to-day life I think could fall under health care, whether it is physical or mentally” (Participant #21, age 17). Participants expressed the desire for HCPs to assess and discuss their psychological well-being during weight-related clinic visit in addition to physical behaviors and actions. Theme 2: Food and physical activity ideals Theme 3: Weight is more than a number.
The number on the scale was not only felt inside themselves, but also seen by others. The participants indicated that weight, as the size of their body, was seen and judged. For example, a participant declared, “And people only judge you by you like how you look. I mean that’s the first thing people see is how you look and I, I sometimes feel like because of my size, people didn’t want to be friends with me. Because why would they want to be friends with a fat girl?” (Participant #9, age 19). To avoid this judgment, the teens avoided various social situations, such as clothes shopping or eating out with friends. The study participants talked about school as a difficult place to live with increased weight, especially in their younger adolescence and middle school years, due to stigmatizing and bullying by peers. Theme 4: I can be healthy but bigger.
Discussion
Our study aimed to understand how female adolescents living with overweight and obesity perceive the concepts of health and weight, and how they experience the clinical encounter when talking about health and weight. Four themes emerged from the data analysis. The first theme, Health is like a physical, mental, and social balance, illustrate how health is seen through a holistic lens that encompasses physical, mental, and emotional aspects of life. The participants overwhelmingly discussed the importance of addressing an individual’s mental health during clinic visits. The past decade has demonstrated an increase in mental and emotional health disorders among female adolescents (Collishaw, 2015; Mojtabai et al., 2016). Psychosocial processes and disorders maintain a formidable influence on the general health of adolescents (Elgar et al., 2016), thus, increasing health care’s emphasis on mental health and holistic care may be warranted.
Growth and development is a time of rapid change and adolescents face increasing autonomy in eating behaviors, food choices, and physical activity options. This makes adolescence an important time to address nutrition and activity related to increased weight. In the second theme, Food and physical health ideals, when asked to describe” health” participants would focus on general actions a person can take to be healthy, such as “healthy eating” or “exercising more.” The participants demonstrated basic knowledge about defining healthy and unhealthy foods, and the need for 30 minutes of sustained physical activity, yet were unable to verbalize their own food and physical activity goals. This aligns with Smith et al. (2014) who reported that adolescents struggled to articulate their desires in weight management care. The adolescents also highlighted the barriers they faced in achieving these goals and did not identify ways they could successfully integrate healthy behaviros into their daily lives. Stevenson et al. (2007) also demonstrated that adolescents often focus on the barriers to healthy eating and the need to lose weight, versus actualizing the knowledge and ideals (Stevenson et al., 2007). HCPs need to be skilled in assessing an individual’s interpretations of their condition and resources; this can help adolescents explore their ambivalence and realize their ideals into pragmatic and achievable goals. Adolescent-friendly care assists adolescents to assume an increasingly independent role in their health and health care.
Our findings illustrate that identifying, labeling, and discussing weight-related topics within the clinical setting was not simple or straightforward. In the third theme, Weight is more than a number, participants explained that they faced a myriad of emotions when discussing their own weight. While they could rationalize that a number on the scale was simply a number, they would then describe how that number simultaneously evoked negative emotions and could be seen by others and judged negatively. It became a lived experience within themselves and impacted their perceptions of how others viewed them. Having the number (weight) further categorized as “overweight” or “obese” by a health care member brought further struggle. The label of overweight or obesity can impact an adolescent’s health. Hunger and Tomiyama (2018) found that girls (aged 14 years old) who were weight-labeled by their family demonstrated a stronger association with disordered, unhealthy eating, than girls who were not weight-labeled. This association was independent of race, parental income, parental education, and initial BMI (Hunger & Tomiyama, 2018).
While negative associations with weight were brought up in our study, the participants also expressed a desire for body acceptance. This finding is consistent with a growing trend of research towards body image (Ali et al., 2013; Halliwell, 2013; Webb et al., 2014). When combined with the participants’ holistic view of health, it’s not surprising that the participants explained that they “felt” healthy. In the final theme, I can be healthy but bigger, results demonstrated that female adolescents with overweight and obesity view their health separately from their body weight. Their body size did not dictate their interpretation of self-health. Feeling healthy while living with overweight and obese has not been recently explored in adolescence, but these data are consistent with research on adult females, where women with obesity felt healthy (Buxton & Snethen, 2013). The adolescent brain is not fully mature or developed (Steinberg, 2005) and it may be difficult for adolescents to conceptualize poor health in the absence of a tangible and definable condition that makes a person feel ill.
As our findings suggest, “health” and “weight” are felt phenomenon for the adolescents and can impact mental and emotional health (Juvonen et al., 2017). Results suggest that HCPs should focus on developing their skills in assessing individual interpretations of an adolescent’s understanding. Insight into a patient’s perspective of health and weight may have significant implications in effectively promoting behavior change and long-term weight control (Teixeira et al., 2012).
Strengths & Limitations
A strength of this study is that participants in this study ranged from 13 – 19 years old, encompassing a wide range of experiences across the adolescence stage. Yet, this range could also be limiting. Differences between the younger and older participant’s experiences could exist. Variability in the data may have been hindered if participant’s perceptions differentiated across early and late adolescence.
Of the sample, 2/3 of the participants were Caucasian. Racial and/or cultural differences may exist in perceptions of weight. Adult African American women have demonstrated various perceptions on obesity and weight as compared to Caucasian women (Thomas et al., 2008). In a narrative review of the literature significant cultural differences on the perceptions of health were found in Mexican youth and may be exacerbating the development of obesity (Aceves-Martins et al., 2016). It is unknown if similar differences exist amongst American adolescents of diverse ethnic backgrounds.
Implications for Practice
Our findings demonstrate the need to develop non-stigmatizing approaches for HCPs and parents to facilitate positive weight-related communication for female adolescents. The use of stigmatizing language and attitudes in health care and general society has been well documented (Tomiyama et al., 2015; van Geel et al., 2014) and adversely affects health (Puhl et al., 2020). Youth are especially vulnerable to the negative effects of weight stigma such as disordered eating and body dissatisfaction (Eisenberg et al., 2017; Puhl et al., 2017). Words and the number on the scale are powerful and impact the lived experience of the adolescent female. Practitioners must carefully navigate the complex perceptions and feelings these youth face regarding their weight. Health care efforts for individualized weight management may be enhanced with consideration of this crucial feature of one’s lived experience and could be a targeted aspect of treatment efforts.
Conclusion
The perceptions of female adolescents living with obesity and overweight provide valuable insight regarding health and weight within the context of the HCE. Our findings highlight the central role mental health plays in the conceptualization of adolescent health, and provides critical insight into the values related to health and health care held by overweight and obese female adolescents. Understanding how adolescents interpret weight within the HCE may assist practitioners in establishing positive therapeutic relationships, fostering effective communication, and guiding health education. Weight stigma in health care cannot be tolerated and efforts to educated and eliminate weight bias should be supported. These insights regarding female adolescent perspectives on health and weight can offer important information for weight management and intervention development.
Appendix: Semi-Structured Interview Guide
What does health mean to you?
How do you view your own health?
How is health important/not-important in your daily life?
What does weight mean to you?
Discuss what weight means to you in your day-to-day life.
How do you view your own weight?
Please describe clinic appointments with doctors, nurses, or dieticians
What occurs?
How does this make you feel?
What else would you like to share with me regarding your health care experiences?
Footnotes
Acknowledgments
The authors would like to acknowledge Judy Hilgers and Jen Rehm for their assistance. We also would like to thank the participants for their time, honesty, and trust.
Ethics
Research was conducted under review of an Institutional Review Board; all participants were interviewed after proper informed consent and assent (of minors) was obtained. This study was conducted in accordance with the 1964 Declaration of Helsinki and its subsequent amendments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.