
Abstract
Introduction
Co-morbid depression in hypertension leads to non-adherence to anti-hypertensive treatment.
Objective
To assess the magnitude and severity of depression and associated factors among hypertensive patients attending follow-up treatment at public hospitals of Hadiya zone, Ethiopia, 2022.
Methods
Hospital-based cross-sectional study was conducted from January 1, to January 31, 2022. The total sample size was 315 and used a systematic random sampling technique. Data were collected through a face-to-face interview. Data were entered using Epi-data Version 4.6 and exported to SPSS Version 25 for analysis. The goodness-of-fit test was done. Binary logistic regression was done, and variables with a p-value of < .25 in the bivariable analysis were taken into the multivariable analysis. Statistically significant was declared at a p-value of < .05 with an adjusted odds ratio and 95% confidence interval.
Result
The magnitude of depression among hypertensive patients was 37.1% (95% CI 31.7–43.9). Regarding the severity, 56.1% had no depression, 6.7% had mild, 17.3% had moderate, 14.7% had moderately severe, and 5.1% had severe depression. Body mass index: 19.12–24.9 kg/m2 [AOR 0.06, 95% CI: 0.02–0.23], body mass index: 25–29.9 kg/m2 [AOR 0.08, 95% CI: 0.02–0.35], absence of family history hypertension [AOR 0.39, 95% CI: 0.18–0.85], presence of co-morbidity [AOR 2.43, 95% CI: 1.34–4.42), low perceived stress scale [AOR 0.07, 95% CI: 0.01–0.56], low medication adherence [AOR 2.70, 95% CI: 1.17–6.24], and moderate medication adherence [AOR 0.29, 95% CI: 0.09–0.88] were significantly associated.
Conclusion
About four in 10 hypertensive patients attending follow-up treatment were depressed. The mean score of severity of depression was mild. Body mass index, family history of hypertension, co-morbidity, perceived stress scale, and medication adherence were significantly associated with depression. Therefore, maintaining body mass index, screening and treating co-morbid illness, accommodating stress, and educating about medication adherence might minimize the risk of depression.
Introduction
Depression and hypertension are known chronic illnesses causing huge burdens worldwide (Jung & Rn, 2016; Kulkarni & Lingappa, 2019; Mandolikar et al., 2017). The burdens include: increased risk for suicide, psychological stress, and physiological restriction (Ginty et al., 2012). The overall global prevalence of depression in hypertensive patients is 27%. Despite this prevalence, depression and its severity among hypertensive patients did not get more attention as a result of feeling of low self-worth, poor concentration, problem of thinking and making decision, depressed mood, loss of pleasure, and decreased energy (Marcus et al., 2012; Sharma & Agrawal, 2017). The statistical association between depression and hypertension is bi-directional (Ma, 2018; Prathibha et al., 2017; Sharma & Agrawal, 2017). Co-morbid depression in hypertension leads to non-adherence to anti-hypertensive treatment and poor compliance with lifestyle modification (Moon et al., 2018; Sharma & Agrawal, 2017).
Review of Literature
Literature indicates that depression and its severity can predict the later incidence of hypertension (Ginty et al., 2012; Kretchy et al., 2014; Mermerelis et al., 2018; Nkporbu et al., 2015). Literature indicates that depression in hypertension is related to uncontrolled blood pressure (Almas et al., 2014; Nkporbu et al., 2015), poor quality of life, and further complications of hypertension (Almas et al., 2014; Mermerelis et al., 2018; Nkporbu et al., 2015; Sharma & Agrawal, 2017). The presence of co-morbid depression in hypertension increases the risk of having poor sleep quality, which predisposes to other health problems (European Society of Cardiology, 2016).
The prevalence of depression in overall medically ill patients in both outpatient and inpatient settings in Ethiopia was 24.5% and 59.7%, respectively (Tilahun et al., 2018), but little is known about the mental health status of hypertensive patients specifically. Studies reported the magnitude of psychological distress rather than specific mental illness. Therefore, this study focused on assessing the magnitude, severity of depression, and associated factors among hypertensive patients attending follow-up treatment at public hospitals in the Hadiya zone, Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted in the public hospitals of the Hadiya zone. Hadiya zone is located 232 km southwest of Addis Ababa, the capital of Ethiopia. The estimated total population of the zone is 1,506,733 among whom, 745,381 (49.47%) are males and 761, 352 (50.53%) are females. The zone has four public hospitals. Namely, Wachemo University Nigist Eleni Mohammed, Memorial Comprehensive Specialized Hospital (WCUNEMMCSH), Gimbichu primary hospital, Hommacho Primary Hospital, and Shone primary hospital. The hospitals give service to more than three million populations in the catchment area. Currently, on average, 800 hypertensive patients attend their treatment at public hospitals in the zone per month. The study was conducted from January 1, to January 31, 2022.
Study Design
Hospital-based cross-sectional study was employed.
Source Population
Source population included all hypertensive patients attending follow-up treatment at public hospitals of Hadiya zone.
Study Population
Study population included all selected hypertensive patients attending follow-up treatment at public hospitals in the Hadiya zone during the study period.
Eligibility Criteria
All hypertensive patients aged 18 and above were included, however, patients severely ill and during the study period were excluded from the study.
Sample Size Determination
The sample size was calculated by using the single population proportion formula. The assumptions of a 5% margin of error, 95% confidence level, and 24.7% proportion of depression in hypertensive patients taken from a previous study (Gebre et al., 2020) are as follows.

By using a 10% non-response rate, the final sample size was 315.
Sampling Techniques
All hospitals in the zone were included in the study. The preceding 3-month report of hypertensive patients who visit the follow-up treatment at the public hospitals of the zone before data collection was obtained from each hospital. Then, the preceding 3-month report was averaged to 1 month, which was WCUNEMMCSH (310), Gimbichu primary hospital (180), Hommacho primary hospital (150), and Shone primary hospital (160). Next, the proportional allocation was used to select the required number of patients from each hospital. Finally, systematic random sampling was used to include patients with a calculated constant value that was (800/315) = 2. The first patient was selected by using the lottery method and then, every second hypertensive patient was interviewed (Figure 1).
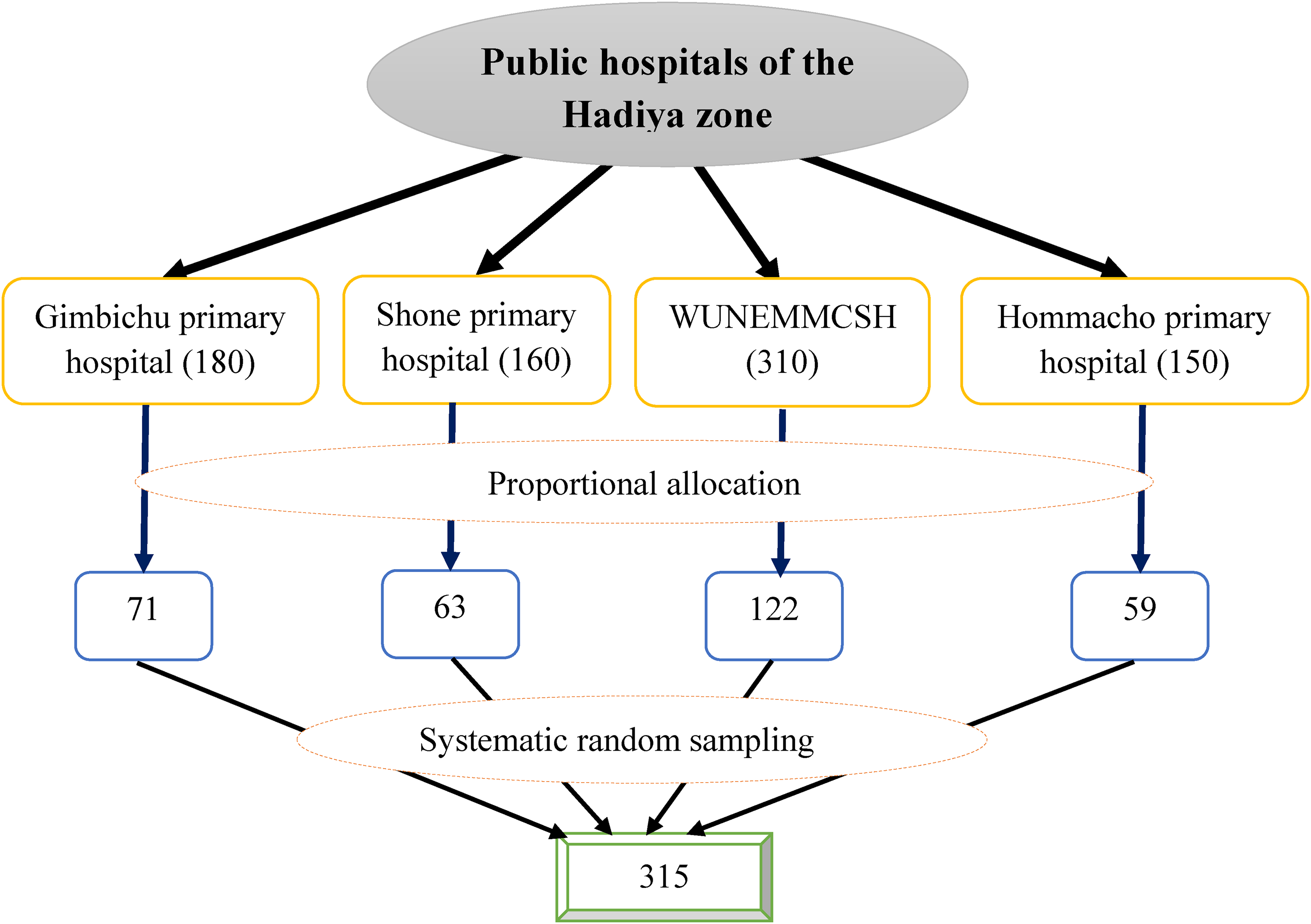
Diagrammatic presentation for sampling procedure of depression among patients with hypertension attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022.
Study Variables
Dependent Variable
Depression.
Independent Variables
Sociodemographic factors
Age, sex, religion, marital status, ethnicity, residence, educational status, and occupation.
Clinical factors
Current blood pressure status, body mass index, family history of hypertension, family history of mental illness, history of admission, and co-morbid chronic illness.
Medical-related factors
Number of antihypertensive medications, duration of treatment, and medication adherence.
Psychological and behavioral factors
Current alcohol use, current chat chew, current tobacco use, perceived stress level, and social support status.
Operational Definition
Depression
Depression is assessed and measured by using pre-tested patient health questionnaires-9 (PHQ-9) that have nine validated items designed to evaluate the presence of depressive symptoms (Gilbody et al., 2007). The items are directly based on the nine diagnostic criteria for major depressive disorder in the Diagnostic and statistical manual fourth edition (DSM-IV) (Sadock & Sadock, 2007). Each item was rated on a three-point scale (i.e., 0 not at all, 1 several days, 2 more than half the days, and 3 nearly every day). The total PHQ-9 score ranged from 0 (absence of depression symptoms) to 27 (most severe depression symptoms). Then, the response was categorized as
Social support status
Social support status is assessed and measured by using Oslo-3 social support scale (OSS-3). It has three items that assess social support. The sum score scale ranged from 3 to 14 and was categorized as
Medication adherence
Medication adherence is measured by using Morisky medical adherence scale-8 (MMAS-8). It consists of eight items with a scoring scheme of yes for 1 and no for 0 for the first seven items and a five-point scale (i.e., 1 never, 2 once in a while, 3 sometimes, 5 usually, and 5 all the time) for the eighth item. Then, the score was categorized as
Perceived stress level
Perceived stress level is measured by using the perceived stress scale (PSS) which is a validated tool used in chronically, ill patients (Lee et al., 2015). The PSS has 10 items and each has a five-point scale (i.e., 0 never, 1 almost never, 2 sometimes, 3 fairly often, and 4 very often). The sum score of PSS ranged from 0 to 40 and was categorized as
Current substance user
A patient who used all or either alcohol, cigarette, or chat at least once in the past one before the study period.
Controlled blood pressure
Controlled blood pressure refers to an average blood pressure less than or equal to 140 mmHg and diastolic blood pressure less than or equal to 90 mmHg (European Society of Cardiology, 2016).
Data Collection Tool
Sociodemographic information was collected by using structured and pre-tested questionnaires. Depression and its severity were assessed by using pre-tested PHQ-9 that have nine validated items designed to evaluate the presence of depressive symptoms (Gilbody et al., 2007; Kroenke et al., 2001). The items are directly based on the nine diagnostic criteria for major depressive disorder in the DSM-IV. The PHQ-9 is a validated tool in Ethiopia and its Cronbach’s alpha was 0.81, reliability was 0.92 with sensitivity of 86% and specificity of 67%. Medication adherence information was gathered by using MMAS-8. The sensitivity and specificity of MMAS-8 items were 93% and 53%, respectively, and the Cronbach’s alpha was 0.83 (Morisky et al., 2008). Social support status information was gathered by using OSS-3. The OSS-3 confirmed the feasibility and predictive validity concerning psychological distress (Zeb et al., 2018). The stress status information was collected by using PSS which is a validated tool used in chronically, ill patients (Lee et al., 2015). PSS assesses stress and coping strategies for the stress (Lee, 2012). The patient's medical record was reviewed to assess co-morbidity and behavioral-related information.
Data Collection Procedure
Data were collected through face-to-face interviews with hypertensive patients. Four diploma nurses and four experienced epidemiologists were recruited for data collection supervision respectively.
Data Quality Assurance
The questionnaire was prepared in English, translated to Amharic (the local language of Ethiopia) for data collection, and retranslated back to English after data collection by language experts to maintain consistency. A two-day training was given for data collectors and supervisors. A pre-test was conducted on 5% (16 hypertensive patients) of the sample size at Durame general hospital a week before the initiation of the main study. Based on the pre-test result, the necessary corrections were made. The Cronbach's alpha reliability test was done and it was 0.82. Continued close follow-up and supervision were performed by supervisors and researchers throughout data collection. All filled questionnaires were reviewed for completeness before data entry.
Statistical Analysis
Data were entered using Epi-data software Version 4.6 and exported to SPSS Version 25 for analysis. Descriptive analysis was performed and the results were presented using tables, figures, frequencies, and percentages. Multicollinearity was considered by using a variance inflation factor (VIF > 10). The goodness-of-fit test was done using the Hosmer-Lemeshow model. Binary logistic regression was done, and variables with a p-value of less than .25 in the bivariable analysis were taken into the multivariable analysis. Statistically significant was declared at a p-value of less than .05 with an adjusted odds ratio and 95% confidence interval.
Result
Sociodemographic Characteristics of Hypertensive Patients
A total of 312 hypertensive patients responded to the interview which yields an overall response rate of 99%. The age group of 141(45.2%) was 40–60 years old and the sex of 159(51.0%) was female. More than half, 201(64.4%) of the participants, were followers of the protestant religion and similarly, 213(68.3%) were married. The ethnicity of 203(65.0%) was Hadiya and the residence of more than half, 182(58.3%) was rural. Regarding educational status, 132(42.3%) had no formal education and the occupation of 107(34.3%) was farmer (Supplemental Table 1).
Clinical Characteristics of Hypertensive Patients
The blood pressure of more than half, 167 (53.5%) of the study participants was controlled. The body mass index of 220(70.5%) was 19.12–24.9 kg/m2. Majority of the study participants 219(65.1%) had no family history of hypertension and more than half, 205(65.7%) have no diagnosed co-morbid chronic medical illness (Supplemental Table 2).
Medical-Related Characteristics of Hypertensive Patients
More than half, 180(57.7%) receive a combination of two or more antihypertensive medications, but, the rest 132(42.3%) receive single antihypertensive medications. The duration of treatment for the majority of the study participants, 259(83.0%) was less than 10 years, however, for 53(17.0%) was less than 10 years.
Medication Adherence of Hypertensive Patients
Out of the total of 312 study participants, the medication adherence of 121(38.8%) was low, 82(26.3%) was moderate, and 109(34.9%) was severe (Figure 2).

Medication adherence of hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
Psychological and Behavioral Characteristics of Hypertensive Patients
Out of the total 312 study participants, 36(11.5%) were current alcohol users, but 276(88.5%) were not current alcohol users. Similarly, 58(18.6%) were current chat chewers, however, 254(81.4%) were not current chat chewers. Regarding tobacco, 27(8.7%) were current users, on the other hand, 285(91.3%) were not current tobacco users.
The Perceived Stress Level of Hypertension Patients
Out of the total of 312 study participants, the perceived stress level of 206(66.0%) was low, 77(24.7%) was moderate, and 29(9.3%) was severe (Figure 3).

Perceived stress level of hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
Social Support Status of Hypertensive Patients
Out of the total of 312 study participants, the social support status of 156(50.0%) was low, 45(14.4%) was moderate, and 111(35.6%) was severe (Figure 4).
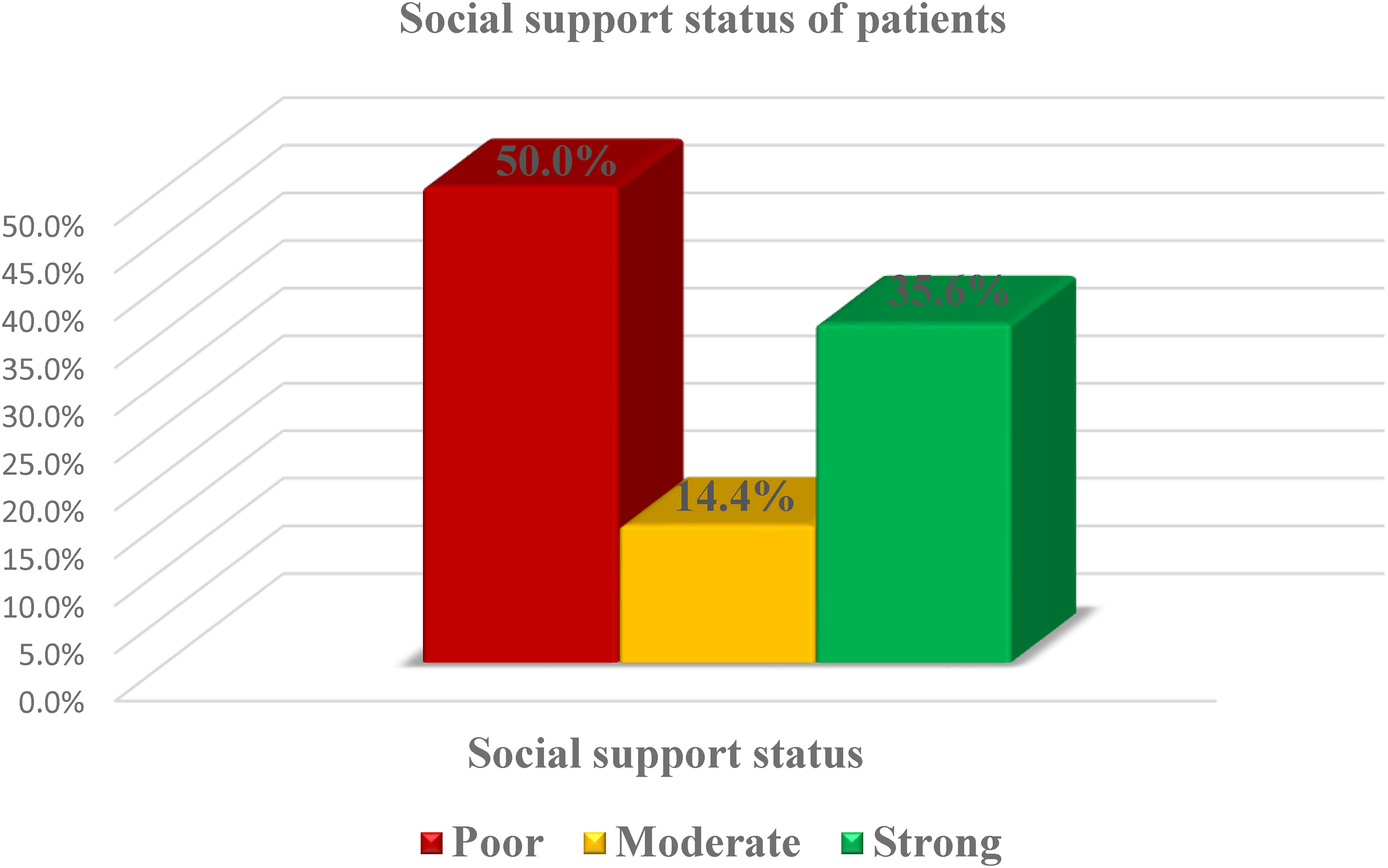
Social support status of hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
The Magnitude of Depression Among Hypertensive Patients
Out of the total 312 hypertensive patients, 116(37.2%) were depressed, however, 196(62.8%) were not depressed (Figure 5).

Magnitude of depression among hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
Depression Regarding the Sex of Hypertensive Patients
Out of the 312 hypertensive patients, 44(37.9%) of males and 72(62.1%) of females were depressed. However, 109(55.6%) of male and 87(44.4%) of female were not depressed (Figure 6).
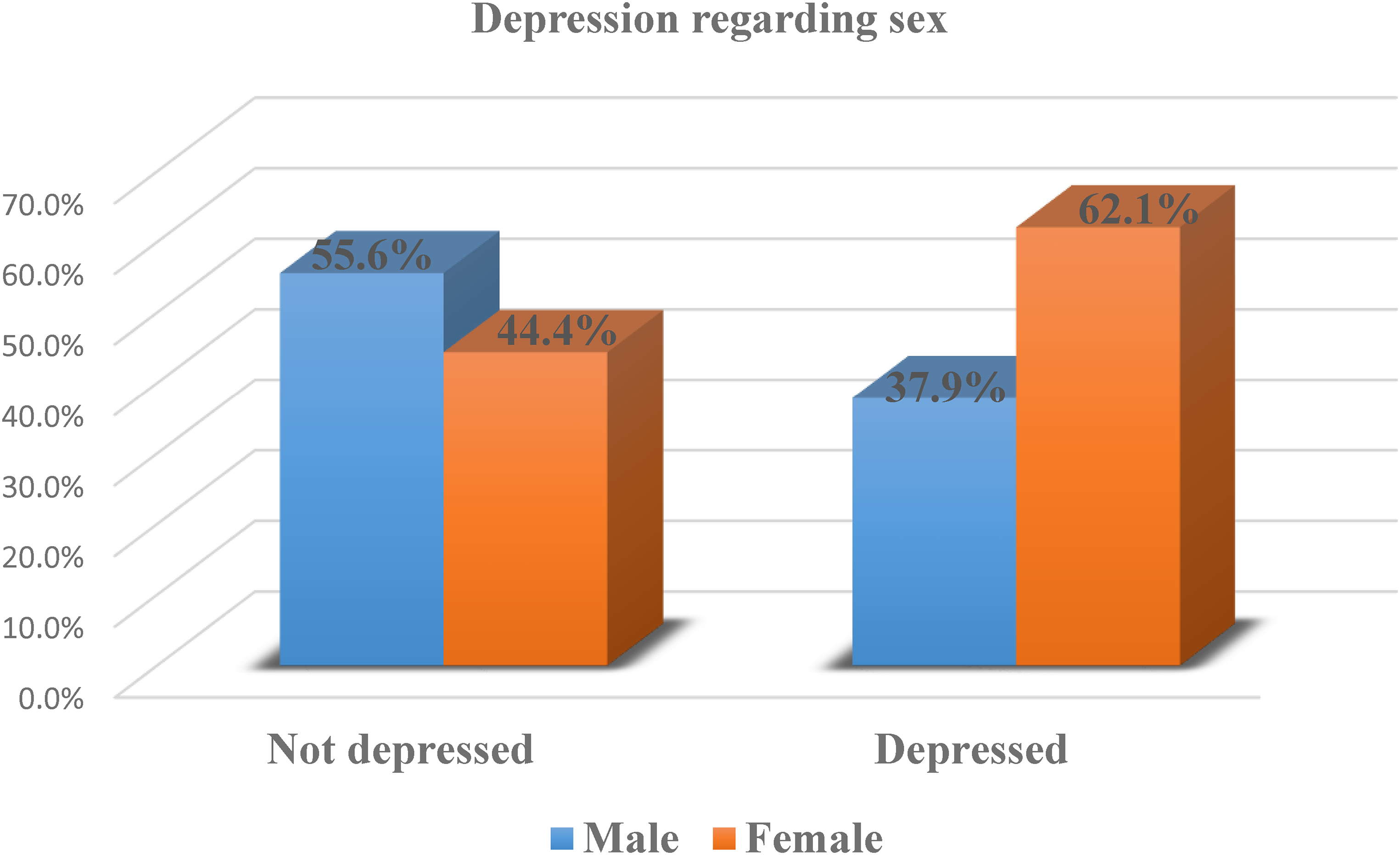
Depression regarding the sex of hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
The Severity of Depression Among Hypertensive Patients
Regarding the severity of depression, 175(56.1%) had no depression, 21(6.7%) had mild depression, 54(17.3%) had moderate depression, 46(14.7%) had moderately severe depression, and 16(5.1%) had severe depression (Figure 7).
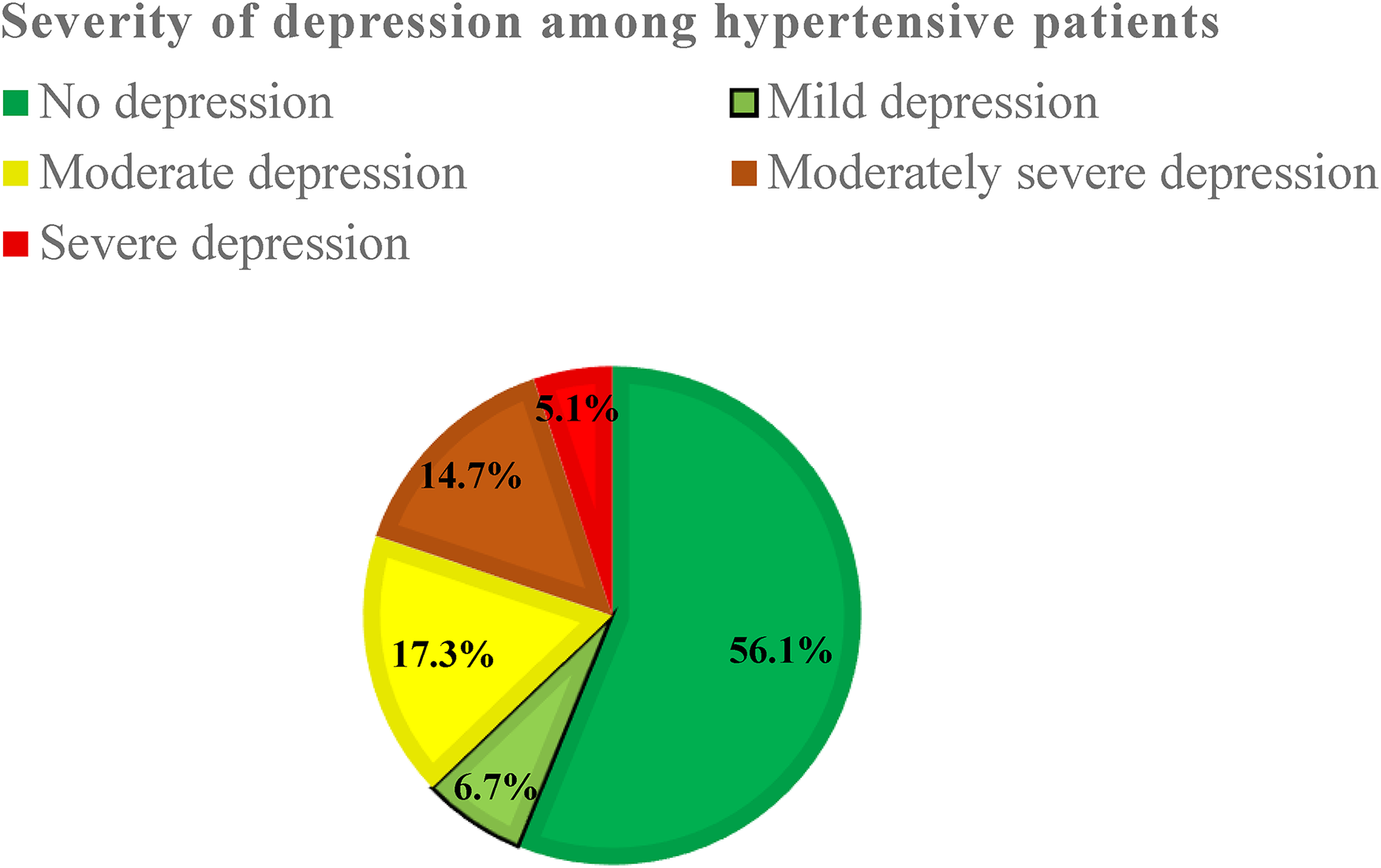
Severity of depression among hypertensive patients attending follow-up treatment at public hospitals of Hadiya Zone, Ethiopia, 2022 (n = 312).
Factors Associated With Depression Among Hypertensive Patients
In bivariable analysis, sex, the number of antihypertensive medications, blood pressure status, body mass index, co-morbidity, family history of hypertension, PSS, social support, and medication adherence were significantly associated with depression among hypertensive patients. (Supplemental Table 3). Whereas in multivariable logistic regression analysis, body mass index: 19.12–24.9 kg/m2 [AOR 0.06, 95% CI: 0.02–0.23], body mass index: 25–29.9 kg/m2 [AOR 0.08, 95% CI: 0.02–0.35], absence of family history hypertension [AOR 0.39, 95% CI: 0.18–0.85], presence of co-morbidity [AOR 2.43, 95% CI: 1.34–4.42], low PSS [AOR 0.07, 95% CI: 0.01–0.56], low medication adherence [AOR 2.70, 95% CI: 1.17–6.24], and moderate medication adherence [AOR 0.29, 95% CI: 0.09–0.88] were significantly associated with depression among hypertensive patients (Supplemental Table 3).
Discussion
The magnitude of depression in this study was 37.2% (95% CI: 31.7–42.9). It was in line with previous studies done in India 41% (Ashok & Ghosh, 2020) and Pakistan 40.1% (Mahmood et al., 2017). However, it was lower than studies reported from Bosnia 46% (Stanetic et al., 2017) and Afghanistan 58.1% (Hamrah et al., 2018). On the other hand, it is much higher than studies reported from South Africa 6.2% (Oshodi et al., 2012), Nigeria 29.4% (Nkporbu et al., 2015), Spain 15.5% (Mejia-lancheros et al., 2014), Saudi Arabia 20.7% (Alhamidah et al., 2017), and Eastern Ethiopia 27.2% (Abdisa et al., 2022). This difference might be due to reasons related to using different depression assessment tools validated for different countries. Regarding this, a study done in Bosnia used Beck Depression Inventory, a study done in South Africa and Nigeria used General Health Questionnaire, and a study done in Spain used DSM-IV, and PHQ-9 was used in this study. In addition, the tools have different cut points to have depression for specific countries based on their socio-cultural depression.
In this study, the severity of depression was assessed. The mean score of the severity of depression among hypertensive patients was 7.13, which is in the range of mild depression. This might be due to the socio-cultural and religious coping mechanisms.
In this study, body mass index was significantly associated with depression. Hypertensive patients who had a body mass index of 19.12–24.9 kg/m2 were 94% less likely to be depressed compared to hypertensive patients who had a body mass index ≥ 30 kg/m2. And also, hypertensive patients who had a body mass index of 25–29.9 kg/m2 were 92% less likely to be depressed compared to hypertensive patients who had a body mass index ≥ 30 kg/m2. This was supported by a study done in Eastern Ethiopia (Abdisa et al., 2022).
This study revealed that a family history of hypertension was significantly associated with depression. Hypertensive patients who had no family history of hypertension were 61% less likely to be depressed compared to hypertensive patients who had a family history of hypertension. This might be due to the absence of genetic interaction between depression and hypertension run in the family (Asres et al., 2016). It was supported by a previous study reported from Pakistan (Mahmood et al., 2017).
The finding of this study indicated that the odds of having co-morbidity with chronic medical illness among hypertensive patients were associated with depression. Hypertensive patients who had a co-morbid chronic medical illness were 2.43 times more likely to be depressed compared to hypertensive patients who had no co-morbidity. This might be the fact that physiological change, symptom burden, and functional impairment from multiple illnesses play a vital role in depression (European Society of Cardiology, 2016; Katon, 2011; Moon et al., 2018). It is consistent with studies by Abdisa et al. (2022) and Hamrah et al. (2018).
The PSS showed a significant association in this study. Hypertensive patients who had a low PSS were 93% less likely to be depressed compared to hypertensive patients who had a high PSS. The increased PSS from different stressors interferes with the physical status and disturbs the mental status which leads to depression.
This study revealed that adherence to anti-hypertensive medication was significantly associated with depression. Hypertensive patients who had low adherence to anti-hypertensive medication were 2.70 times more likely to be depressed compared to hypertensive patients who had high adherence to anti-hypertensive medication. However, hypertensive patients who had moderate adherence to anti-hypertensive medication were 71% less likely to be depressed compared to hypertensive patients who had high adherence to anti-hypertensive medication. This shows that non-adherence to anti-hypertensive medication, which leads to prolonged duration of illness and complications of the illness might increase the risk of being depressed. In another way, the early manifestation of depression leads to a lack of interest and initiation for giving values regularly. This finding was supported by other studies (Ashok & Ghosh, 2020; European Society of Cardiology, 2016; Jung & Rn, 2016; Moon et al., 2018). This less likely association with moderate adherence suggests that the odds of depression decrease as drug adherence increases.
Strengths and Limitations
Strengths and limitations can be noted within this study. Including hypertensive patients from different hospitals and using the validated tool can contribute to the strength of the study. Ignoring hypertensive patients from private hospitals can be limitation of the study. In addition, it may be susceptible for socio-cultural desirability bias and unable to include qualitative design could be mentioned as the potential limitation of the study.
Implications for Practice
Identifying the independent risk factors of depression for hypertensive patients is imperative in aiding policy makers to important strategies at policy level and it gives clue for health workers in managing psychosocial, behavioral, and socio-cultural status of the patients. The health management strategies of developing countries should include the preventive measures of depression. Managing the hypertensive patients’ inconsideration of body mass index, familial history of hypertension, co-morbid chronic physical illness, PSS, and medication adherence can imply the effective prevention strategy for these patients. Stake holders of the health care system can have better and effective improvement on depression and related mental causes if they implement their strategic plan in consideration with the implied independent risk factors.
Conclusion
About four in 10 hypertensive patients attending follow-up treatment in public hospitals of Hadiya zone were depressed. The mean score of severity of depression was mild. Body mass index, family history of hypertension, co-morbid chronic physical illness, PSS, and medication adherence were significantly associated with depression among hypertensive patients. Therefore, maintaining body mass index, early diagnosing and treating co-morbid chronic medical illness early, accommodating stress, and giving health education about medication adherence might minimize the risk of depression among hypertensive patients.
Supplemental Material
sj-docx-1-son-10.1177_23779608231193744 - Supplemental material for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia
Supplemental material, sj-docx-1-son-10.1177_23779608231193744 for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia by Elias Nigusu, Ruhama Ermias, Selamu Abose, Elias Ezo, Solomon Gebre and Taye Mezgebu in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608231193744 - Supplemental material for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia
Supplemental material, sj-docx-2-son-10.1177_23779608231193744 for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia by Elias Nigusu, Ruhama Ermias, Selamu Abose, Elias Ezo, Solomon Gebre and Taye Mezgebu in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608231193744 - Supplemental material for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia
Supplemental material, sj-docx-3-son-10.1177_23779608231193744 for Magnitude and Severity of Depression and Associated Factors Among Hypertensive Patients Attending Follow-up Treatment at Public Hospitals of Hadiya Zone, Ethiopia by Elias Nigusu, Ruhama Ermias, Selamu Abose, Elias Ezo, Solomon Gebre and Taye Mezgebu in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgement
We would like to thank the study participants for the scarification of their valuable time and Wachemo University for funding.
Author Contributions
All authors have made substantial contributions to the work. Participated in the conception, design, and acquisition, conducted the data analysis and interpretation; took part in drafting, revising, and critically reviewing the article. All authors gave final approval of the version to be published and all authors have agreed on the journal to which the article has been submitted; agreed to be personally accountable for all aspects of the work.
Availability of Data
The data used for this study are available from corresponding authors on secured and reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The fund for this study was covered by Wachemo University.
Ethical Consideration
Ethical clearance was obtained from Wachemo University College of Medicine and Health Science, Institutional Review Board (IRB/906/14) and a formal letter of cooperation was written to hospitals.
Informed Consent
Written informed consent was obtained from each participant, and the information obtained from them would not have been disclosed. Coding was used to eliminate names and other personal identification of respondents to ensure anonymity, privacy, and confidentiality. Thoroughly, our research passed required the principles of the Declaration of the Helsinki General Assembly, Seoul, Korea, and October 2008.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.