
Abstract
Introduction
The spread of microorganisms is caused by direct or indirect contact, respiratory droplets, and airborne transmission. Knowledge and compliance with standard precautions are crucial in preventing infection in the hospital.
Objectives
To assess the level of knowledge and compliance with standard precautions among registered nurses who work in military hospitals and the factors affecting compliance with standard precautions.
Methods
A descriptive cross-sectional study was conducted. Four hundred and eight registered nurses at three Jordanian Royal Medical Services hospitals completed an online self-report questionnaire using a convenience sampling technique. The statistical package for social sciences (SPSS) version 25 was used to analyze the data.
Results
The level of knowledge of standard precautions among nurses was excellent, with an overall mean score of 15.59 ± 2.22 out of 20; around half (54%) of them had an excellent level. Nurses’ compliance with standard precautions was intermediate, with an overall mean score of 59.65 ± 14.57 out of 80. Forty-seven percent of nurses had a high degree of compliance. Compliance with standard precautions was correlated positively with age, working experience in years, total knowledge score, training in standard precautions, and availability of personal protective equipment, and negatively with exposure to sharp injuries.
Conclusion
Nurses play a key role in preventing and managing hospital infections through their responsibility for a large proportion of patient treatment and care. Therefore, efforts should be made to improve nurses’ perceptions of the basic elements of standard precautions. Even so, results showed that compliance with standard precautions was intermediate. This highlights the need to take the necessary measures to raise the level of compliance. Even so, results showed that compliance with standard precautions was intermediate. This highlights the need to take the necessary measures to raise the level of compliance.
Introduction/Background
Standard precautions (SPs) are designed by the Centers for Disease Control and Prevention (CDC) to minimize all pathogens’ transmission risks, including blood-borne pathogens in healthcare units (Paul et al., 2014). There was confusion concerning body substance isolation and universal precautions (UPs), and the two practices encouraged the creation of SPs. According to Bouchoucha (2014), the CDC expanded the isolation precaution concepts in 1996 to form the SPs. The SPs included and expanded the UP elements to encompass all body fluids and blood except sweat (Garner, 1996).
The CDC documented SPs elements in 2007, including hand hygiene, personal protective equipment (PPE), cough etiquette or respiratory hygiene, sharp safety, safe injection practice, sterile instruments and devices, and clean and disinfected environmental surfaces (Badran et al., 2021). PPE refers to equipment that nurses wear to protect themselves from contact with or exposure to infectious pathogens, such as face masks, gloves, coats, and gowns (Lee et al., 2021). It protects nurses from multiple patient interactions, covering the clothing and skin likely to come into contact with saliva, blood, and infectious materials (Lee et al., 2021).
Another element of SPs is environmental infection prevention and control policies, indicating that ecological surfaces are also part of the strategy. Cleaning eliminates important microorganisms from environmental surfaces and must be followed by disinfection to destroy pathogens (Mirza et al., 2015).
Review of Literature
Knowledge and compliance with SPs will protect and reduce rates of infection (Zeb & Ali, 2021). Therefore, many researchers conducted studies about these issues in different countries. In Jordan, the most recent study was conducted by Al-Faouri et al. (2021) on 300 registered nurses; the mean knowledge score was 16.72 out of 20 (81%), and the compliance score was 49.15 out of 80 (61%). Although the participants’ compliance was intermediate, they did have a high degree of knowledge; compliance was positively connected with age, experience, and knowledge. The nurses in all health sectors were not represented in the prior survey.
Knowledge and compliance with SPs are crucial in ensuring the prevention of infection across the hospital. These prevention steps are put in place to ensure the safety of patients and staff from contracting infections (Jones, 2019). The knowledge and compliance of SPs are essential for minimizing and preventing hospital-acquired diseases (Zeb & Ali, 2021). Numerous studies conducted in different countries agreed that knowledge and compliance correlated positively (Al-Faouri et al., 2021; Luo et al., 2010).
The Royal Medical Services (RMS)—the military health sector—is one component of the public medical sector in Jordan. It provides comprehensive healthcare services, including primary healthcare services, in-field clinics, and eight comprehensive medical centers distributed across all regions of the Kingdom. It plays a key role in providing secondary and tertiary healthcare services, owning 16 hospitals (10 main hospitals and six specialized medical centers) spread across all regions of the Kingdom. The RMS also provides free health services to approximately 38% of individuals in Jordan with health insurance. The RMS started and developed in a different way from the other sectors. The period during which military nurses provided medical attention and preventive health care to members of the armed forces, they had different qualifications, salaries, promotions, certifications, practices, and knowledge (Jebreel et al., 2018).
In Jordan, limited studies have been conducted during the last decade regarding SPs, targeting nursing students and registered nurses who work in private, government, and university hospitals. However, only one study conducted by Al-Rawajfah et al. (2013) targeted the nurses who work at the RMS. These nurses have some characteristics that distinguish them from others. There is a high proportion of nurses in Jordan, working under military rules and having a specialization system. Therefore, this study has assessed the level of knowledge and compliance with SPs among registered nurses who work in military hospitals and the factors affecting their compliance.
Therefore, nurses’ compliance and knowledge regarding the appropriate use of the PPEs as one element of SPs enables them to minimize the risks of infection while ensuring that the association between the healthcare givers and the clients remains the most significant concern in the organization. There is little known about SP's level of knowledge and compliance in RMS hospitals. This study's findings could provide baseline data to assist nursing managers and decision-makers in setting priorities for developing educational programs and strategies to enhance knowledge and compliance with SPs among military nurses.
Purpose of the Study
This study aims to assess the level of knowledge and compliance with SPs among registered nurses who work in military hospitals and the factors affecting compliance with SPs.
Methods
Design
A descriptive cross-sectional design was conducted during February and March 2022.
Sample
The study was conducted for RMS hospitals after grouping them into strata based on the country's three locations (northern, central, and southern regions); then, a simple random technique was used for selecting one hospital from each stratum. The sample size was estimated using the Thompson formula: n = [N × (1 − p)]/[N − 1 × (d2/Z2)] + (1 − p)], where N is the population size (4,258), n is the sample size, Z is the confidence level at 95%, p is the probability (50%), and d is the error proportion (0.05). Based on this formula, the minimum sample size is 353 nurses (Thompson, 2012). This formula was used to calculate the appropriate number of participants from each region based on the proportion of nurses in that region: for the northern region, 0.21 × 353 = 74; for the central region, 0.62 × 353 = 219; and for the southern region, 0.17 × 353 = 60. To overcome the problems of a low response rate and missing and incomplete questionnaires, the sample was increased to 408 registered nurses who had at least one year of experience.
Inclusion/Exclusion Criteria
Inclusion criteria include registered nurses who worked in the selected hospitals and had at least a bachelor's degree and at least one year of experience. While the exclusion criteria included: novice nurses enrolled in a newcomers’ course that extended for one year.
Instruments for Data Collection
An online self-report questionnaire with a consent form was used to collect the data. The questionnaire consists of two parts: (a) sociodemographic and clinical information, which was developed by the researcher based on previous studies, consists of age, marital status, educational level, experience in years, working region, working department, and technical classification. Clinical information includes the history of exposure to polluted sharp injuries, impaired skin exposure to blood or body fluids, training status on SPs, desirability to train on SPs, having the sharp container in the working department, having the PPE in the working department, the vaccination status against hepatitis B virus (HBV), whether the participants know the serum level of anti-hepatitis B (anti-HB), and whether they perform needle recapping. The knowledge and compliance scale of SPs was first developed by Askarian et al. (2007) and modified by Luo et al. (2010). The scale has a high content validity index of 0.98, and the reliability coefficient is 0.86 (Luo et al., 2010). The knowledge of SPs subscale consists of 20 items. The response to each item is ranged from “correct” = 1 to “incorrect” or “don’t know” = 0. The range of the total score is (0–20). Total knowledge scores were categorized into three levels: I. Poor: <50th percentile (range: 0–9); II. Satisfactory: 50th–75th percentile (range: 10–15), III. Excellent: >75th percentile (range: 16–20; AL-Rawajfah & Tubaishat, 2015; Sarani et al., 2016). The compliance with SPs scale consists of 20 items on a 5-point Likert scale. The response to each item ranges from never = 0, seldom = 1, sometimes = 2, usually = 3, to always = 4. The range of the total score is (0–80). Low (scores: <50%), intermediate (scores: 50%–75%), and high (scores: >75%; AL-Rawajfah & Tubaishat, 2015; Sarani et al., 2016).
Pilot
After the first draft of the questionnaire was completed, it was distributed to other research team members for feedback, and then it was edited to apply to a pilot study. Before beginning the main research, the authors undertook a pilot study on a convenience sample of 22 nurses. The purpose is to identify any problems or challenges in the data gathering and the suitability of the questionable items. From the standpoint of the participants, the step evaluates and ensures the clarity and familiarity of the questionnaire's words and phrases. According to their feedback, the items were clear, comprehensive, appropriate, and simple to complete.
Ethical Considerations
Ethical approval was obtained from the Committee of Scientific Research and Ethics of Research at the Faculty of Nursing, Al al-Bayt University (AABU/No. 141/2021, 22.1.2021), as well as RMS Institutional Review Board of the selected hospitals. Ethical considerations were protected, such as voluntary and anonymity to participate and confidentiality of the data. Full information about the study was provided by the consent form, such as study purpose, significance, and right to withdraw from the study at any time without any penalties. Data were collected via an online self-reporting questionnaire after getting access to the registered nurse by email. In addition, permission to use the instruments was obtained from the original authors, Askarian et al. (2007) and Luo et al. (2010).
Statistical Analysis
Statistical Package for Social Sciences (SPSS) platform version 25 was used to analyze the data after screening and cleaning, and then descriptive and inferential statistical tests were used to analyze nurses’ knowledge and compliance with SPs.
Results
Sample Characteristics
A total of 700 nurses working in RMS hospitals were invited to participate in this study; 408 agreed, with a response rate of 58%. Concerning sociodemographic data, the mean age of participants was 32.52 years (SD ±5.20), and the mean experience years in nursing was 11.22 years (SD ±5.22). Table 1 presents more information about the participants’ characteristics.
Sample Characteristics of the Study Sample.

Regarding the clinical information about participants, the history of exposure to sharp injury and impaired skin and mucosa from patients’ body fluids was 21.57% and 34.07%, respectively. Although 78.68% of participants had enrolled in SP training sessions, 87.01% desired further SP training. Eighty-six percent of nurses had a special sharps box and PPE in their departments. Although a high percentage of nurses (89.22%) disclosed that they were vaccinated against HBV, more than half (52%) did not know their serum level of anti-HBs, 38% knew their level was negative, and 10% knew it was positive. Finally, 47.06% of nurses were still performing needle recapping.
Nurses’ mean knowledge score of 15.59 out of 20 ± 2.22, representing a score of 77.95% ([15.59/20] × 100%). The quartiles for total nurses’ knowledge scores were 25th = 14, 50th = 16, and 75th = 17. Table 2 indicates the frequency and percentage of correct and incorrect answers for each knowledge item.
Items of Knowledge of Standard Precautions Scale.

Nurses’ compliance scores are allocated between 19 and 80, with a mean total compliance score of 59.65 ± 14.57 out of 80, representing a score of 74.56% ([59.65/80] × 100%). Of the 408 nurses, 31 (7.60%) scored 80, the most frequent score. The quartiles for total compliance scores were 25th = 50, 50th = 60, and 75th = 72 (see Table 3). Based on Table 4, hand washing has the highest compliance within the SPs domain, followed by wearing a facemask; a protective suit is the least compliant.
Items of Compliance With Standard Precautions Scale.

Compliance With Standard Precaution (SP) Domains.

A one-way between-groups analysis of variance was conducted to identify the geographic region's impact on SP knowledge levels. Nurses were divided into three groups: Group 1: central region; Group 2: northern region; Group 3: southern region.
Despite reaching statistical significance, the difference in mean scores between the groups was relatively small. The Tukey honestly significant difference test indicated that the mean score for the central region (M = 59.64, SD = 14.23) was significantly different from the southern region (M = 54.59, SD = 14.57). Table 5 illustrates the participants’ compliance with SPs by region.
Comparing Participants’ Knowledge and Compliance With Standard Precautions (SPs) by Geographic Region.

Note. Standard deviation (SD), the mean difference is significant at the 0.05 level.
In the current analysis, the total compliance score was the dependent variable, and other predictors were independent variables. Age, experience, and knowledge were considered continuous variables, and the other predictors were dichotomous variables. The independent variables were entered simultaneously in the regression model. A standard multiple regression was calculated to predict compliance with SPs based on independent variables. A significant regression equation was found F(10,397) = 9.25, p < .001, with an R2 of 0.19. This stated that the model as a whole explained 19.0% of the variance in compliance score. The findings show age (β = 0.37, p < .001), working experience in years (β = 0.29, p < .001), total knowledge score (β = 0.19, p < .001), exposure to sharp injury (β = −0.15, p < .001), training in SPs (β = 0.18, p < .001), and availability of PPE (β = 0.17, p < .001). Compliance with SPs was correlated positively with age, working experience in years, total knowledge score, training in SPs, and availability of PPE, and correlated negatively with exposure to sharp injuries. Gender, having a sharps disposal box, exposure of impaired skin to blood or body fluids, and performing needle recapping were not statistically significant predictors (Table 6).
Predictors of Compliance With SPs.
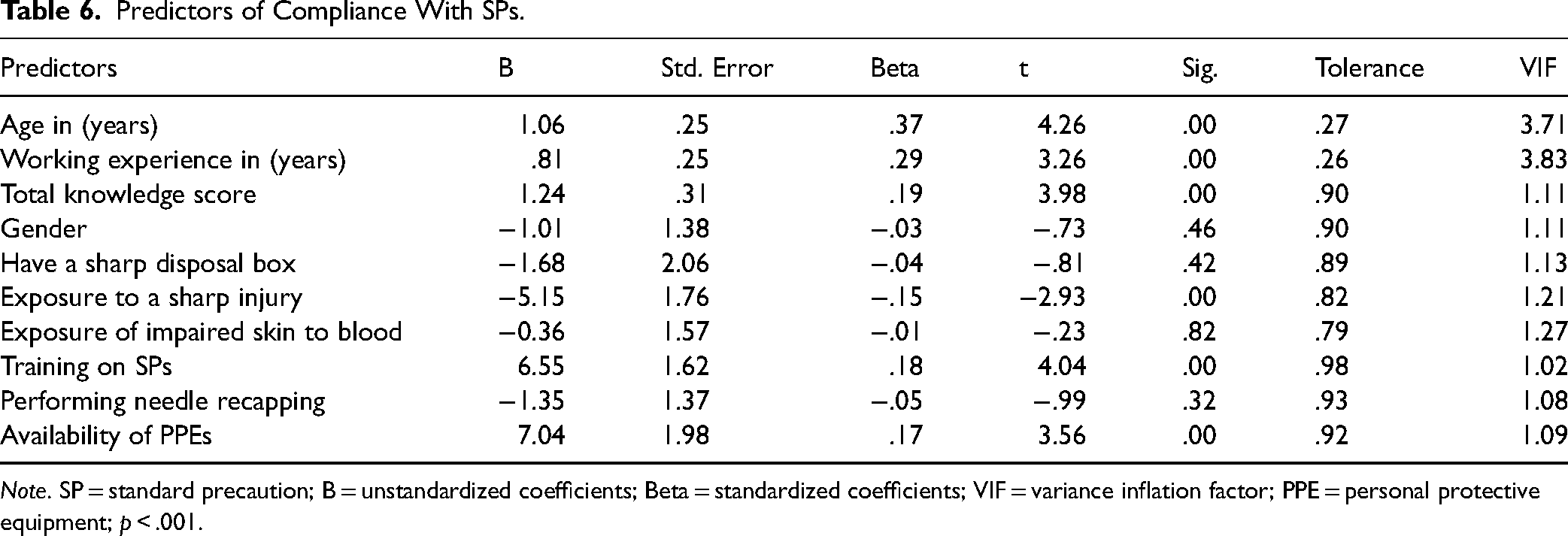
Note. SP = standard precaution; B = unstandardized coefficients; Beta = standardized coefficients; VIF = variance inflation factor; PPE = personal protective equipment; p < .001.
Discussion
The findings of this study revealed that over a fifth (21.57%) of the nurses were exposed to a polluted sharp injury; this result is similar to other studies (Abalkhail et al., 2022; Dilie et al., 2017; Kasatpibal et al., 2016; Luo et al., 2010). On the other hand, this was lower than similar studies among nurses and healthcare workers (HCWs) in different countries: China, Iran, Jordan, and Egypt, respectively (Almhammd et al., 2020; Ghanei Gheshlagh et al., 2018; Saadeh et al., 2020; Sabaa et al., 2021). The history of sharp injuries in this study was below average compared to other studies. Action should be taken to eliminate this issue by introducing a policy to motivate nurses to apply the recommended safe injection practice because most blood-borne pathogens are acquired from sharp injuries.
More than two-thirds of participants had received training in SPs, as in two studies conducted in Jordan by Al-Rawajfah et al. (2013) and in Pakistan by Shah (2017). In addition, this study showed a higher proportion of SP-trained participants than several studies conducted in different regions (Aung et al., 2017; Beyamo et al., 2019; Haile et al., 2017; Kasa et al., 2020; Luo et al., 2010; Ogoina et al., 2015). Most of these studies showed a positive correlation between training and knowledge of SPs, so training is considered essential to gaining knowledge about SPs. The reason for the high proportion of trained nurses in the current study may be that the newcomer nurses must be engaged in the newcomer's course, whereas the training on SP is a part of this course based on RMS policy, and the training on SPs was increased during the COVID-19 pandemic.
This study's findings that the majority of participants had received an HBV vaccination (89.22%) are in line with findings from other studies (Al-Rawajfah et al., 2013; Almhammd et al., 2020). Because HCWs have a significant risk of contracting bloodborne viruses, a high number of HBV vaccinations are the result of following the CDC's recommendations. Additionally, in nursing programs, this immunization is typically administered prior to the commencement of clinical courses. However, 48% of the nurses in this study did not know the level of anti-HBs in their serum, which may be a sign that they were not getting regular checkups.
The overall knowledge score about SP was 15.59 ± 2.22 out of 20, indicating an excellent level of knowledge. Around half of the participants (59.6%) obtained scores between 14 and 17 out of 20. These findings are consistent with the findings of several studies, such as that conducted in North Jordan by Al-Faouri et al. (2021; mean score 16.27 ± 3.15 out of 20); in China by Almhammd et al. (2020; overall score 17.3 ± 1.8 out of 20), and in South Korea by Oh and Choi (2019; mean score of 88.8 ± 7.5 out of 100). In this study, the nurses have poor knowledge of three items of the knowledge scale, which may be due to the fact that the training course materials did not cover them. First, the lowest scoring item was the question about the main goal of SPs, which was answered by around one-quarter of the participants; this result is consistent with those of Almhammd et al. (2020) but inconsistent with those of Al-Faouri et al. (2021). Secondly, only around one-quarter of participants answered correctly regarding the care of patients with syphilis needing extra precaution; this agrees with Almhammd et al. (2020). Thirdly, around half of the participants answered incorrectly regarding wearing gloves during oral procedures; this result is consistent with those of Almhammd et al. (2020) but contradicts those of Al-Faouri et al. (2021). The highest knowledge scores were for the use of gloves followed by applied hand washing; this result agrees with the results of several others (Al-Faouri et al., 2021; Almhammd et al., 2020; Luo et al., 2010).
Moreover, the results showed that the majority of nurses knew what SPs are, although around half did not know that SPs should be applied when dealing with all patients, regardless of their diagnosis. Above 90% of nurses answered correctly that gloves should be changed when coming into contact with different patients, and the majority knew that they should wash their hands immediately after contacting the patient's fluids. Although nurses’ knowledge level was high, 74.02% answered incorrectly that the main objective of SPs is to protect both HCWs and patients and to ensure a safe environment. In addition, nurses should know that the SPs alone are insufficient when dealing with infectious diseases such as hepatitis C and syphilis. In this study, the results revealed that more than 80% of the participants knew that dealing with patients with tuberculosis or infectious skin diseases needs additional care, such as contact and airborne precautions, while more than half of the participants in another study did not realize this (Al-Faouri et al., 2021). These results highlight the necessity to focus on the basic elements of SPs when introducing lectures, workshops, training programs, and orientation. The higher results in the current study may be because experience and training play a significant role in gaining knowledge, or this study was conducted during the COVID-19 pandemic.
Concerning compliance with SPs, the mean score was (59.65 ± 14.57 out of 80, 74.56%), indicating an intermediate degree of compliance. Around half of the participants (52.0%) obtained scores of 50–72 out of 80. The reason may be that strict measures taken during the COVID-19 pandemic increased nurses’ commitment to applying SPs, especially wearing masks. Several similar studies in different regions around the world showed a discrepancy in mean scores: Al-Faouri et al. (2021), in North Jordan, found that 266 nurses working in three hospitals had a mean score of (49.15 out of 80, 61.43%); a Jordanian national population-based study conducted by Al-Rawajfah et al. (2013) on 889 nurses working in different health sectors revealed a mean compliance score of 82.69%; a study in Saudi Arabia by Almoghrabi et al. (2018) on 416 nurses working in 45 primary health centers found a mean compliance score of 85.92%; and Luo et al. (2010) with 1,444 nurses working in 18 Chinese hospitals indicated a mean score of 60.36%. The discrepancy in the mean compliance scores between these studies may be due to the different working environments and departments.
Wearing gloves during the disposal of stool and urine is the highest compliance item, but wearing gloves during intramuscular or hypodermic injection is the lowest. Hand washing, using a facemask, and wearing gloves had the highest compliance mean scores, followed by disposing of sharps. Protective clothing for eyes, hair, shoes, and suits had the lowest compliance scores, probably due to the unavailability of some PPEs such as head covers, shoe covers, goggles, and aprons in all hospital departments. In addition, around half of the nurses fully complied with hand-washing when contacting different patients, taking off their gloves, and contacting patients’ body fluids. More than 50% of nurses fully complied with wearing gloves when dealing with stool and urine, contacting the patient's mucosa, obtaining a saliva culture, changing the dressing, and cleaning blood traces. On the other hand, only 26% of nurses always wore gloves for intramuscular or hypodermic injections and 31% for venous puncture. Finally, only 34% of nurses were fully compliant with disposing of sharps. These results are higher than those of Al-Faouri et al. (2021), perhaps because the head nurses and managers in military hospitals had more authority in endorsing the commitment to SPs than head nurses and managers in other health sectors.
Regarding predictors of compliance with SPs, this study revealed that knowledge is positively correlated with compliance, indicating that the higher the knowledge scores, the better the compliance; this result agrees with other studies (Al-Faouri et al., 2021; Luo et al., 2010). In addition, a very weak positive correlation was found by Al-Rawajfah and Tubaishat (2015). However, other researchers (Almhammd et al., 2020; Aung et al., 2017; Ogoina et al., 2015; Oh & Choi, 2019; Sarani et al., 2016), found that knowledge was not correlated with compliance. Also, in the current study, age is positively correlated with compliance, agreeing with Beyamo et al. (2019); it may be that the years of working experience increase with age, and the nurses may have had a high perception regarding the risks of infectious diseases. In addition, in the current study, training on SPs is positively correlated with compliance, agreeing with some (Al-Rawajfah et al., 2013; Beyamo et al., 2019; Haile et al., 2017; Luo et al., 2010), but not all (Aung et al., 2017) studies. Moreover, the availability of PPE is positively correlated with compliance, supporting other findings (Beyamo et al., 2019; Haile et al., 2017; Luo et al., 2010).
In the current study, gender is not correlated with compliance, supporting other findings (Al-Faouri et al., 2021; Al-Rawajfah & Tubaishat, 2015; Aung et al., 2017). However, Haile et al. (2017) showed that female nurses were 2.18 times more compliant than male nurses. Also, having a sharps disposal box was not correlated with compliance, although Luo et al. (2010) found a positive correlation with compliance. The exposure of impaired skin to a patient's body fluids was not correlated with compliance, although Aung et al. (2017) found a positive correlation between them. The current study agreed with Aung et al. (2017) in finding no correlation between needle recapping and compliance with SPs.
Strengths and Limitations
This study is one of the first to look into knowledge and compliance with SPs among nurses working in military hospitals. It also provides baseline data to help nursing managers and decision-makers identify priorities for developing educational programs to improve military nurses’ knowledge and compliance with SPs. However, the current study has some limitations, including the use of a cross-sectional design and the fact that it was limited to RMS hospitals.
Implications for Practice
This study produced baseline data and an appropriate assessment of the level of knowledge and compliance with SPs among Jordanian nurses and identified the factors preventing nurses from complying with SPs. It may be necessary for nursing managers and policymakers to prioritize developing educational programs and strategies to improve knowledge and enhance compliance with SPs among nurses. Such strategies include organizational support by enhancing the infection control committee's role, nursing empowerment to reduce the exceeded workload, supply management to provide adequate and appropriate equipment and resources, and health promotion activities through lectures and workshops about SPs. This study suggests the necessity of cooperation between the health sectors in Jordan to formulate policies that reduce the transmission of infection between healthcare staff and patients and, thus, the community. Through nursing motivation, these policies should include enhancing knowledge and complying with SPs to limit the spread of infectious diseases, especially in the southern region.
Conclusions
It is critical to ensure that high-quality medical treatment and security are provided by preventing and controlling hospital infections. Nurses play a key role in preventing and managing hospital infections. Adherence to SPs is an essential part of preventing hospital infections.
According to the findings of this study, the level of knowledge regarding SPs is excellent, but the nurses have the lowest score in the main goal of implementing the SPs. Therefore, efforts should be made to improve their perception of the basic elements of SPs. Even so, results showed that compliance with SPs was at an intermediate level. This highlights the need to take the necessary measures to raise the level of compliance. Compliance with SPs was correlated positively with age, working experience in years, total knowledge score, training in SPs, and availability of PPEs, and correlated negatively with exposure to sharp injuries.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Institution Review Board Approval
The present research was conducted in accordance with the general ethical guidelines and the ethical approval was obtained from the IRB of Al al-Bayt University. Written informed consent was obtained from all participants prior to the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.