
Abstract
Introduction
Ventilator-associated pneumonia (VAP) is a significant nosocomial infection in intensive care units (ICUs), contributing to increased morbidity and mortality. Nurses in ICUs play a critical role in implementing prevention strategies.
Aim
The aim of this study was to evaluate ICU nurses’ knowledge of and compliance with VAP prevention strategies in Hebron hospitals, and to examine associations with demographic variables.
Methods
A descriptive cross-sectional study was conducted among 160 ICU nurses from six hospitals in Hebron, Palestine. Data were collected using a validated, self-administered questionnaire assessing knowledge (15 items) and compliance (17 Likert-scale items). Descriptive statistics, Mann–Whitney U tests, Kruskal–Wallis tests, and Spearman's correlation were used for analysis.
Results
Nurses demonstrated a moderate level of knowledge regarding VAP prevention (mean correct responses = 50.96%). Significant differences in knowledge were observed based on gender (P = .044), hospital type (P = .011), and education level (P = .001). Overall compliance was high (mean score = 2.55 out of 3), with the highest adherence reported in hand hygiene and patient positioning practices. Nurses from private hospitals reported significantly higher compliance (P = .003). However, no significant correlation was found between knowledge and compliance (P = .062).
Conclusion
Despite moderate knowledge, ICU nurses demonstrated high compliance with VAP prevention strategies. However, inconsistencies in certain practices and the lack of a strong correlation between knowledge and compliance suggest that experience alone may not ensure adherence. Targeted educational interventions, standardization of protocols, and institutional support are essential to improving VAP prevention in ICUs.
Keywords
Introduction
Ventilator-associated pneumonia (VAP) is a well-known nosocomial infection among patients receiving mechanical ventilation (Centers for Disease Control and Prevention [CDC], 2018). According to the National Healthcare Safety Network, the incidence of VAP in various hospitals ranges from 0.0 to 4.40 per 1,000 ventilator-days. Depending on the diagnostic criteria used, the overall incidence ranges from 5% to 65% (Hickey & Giwa, 2023; Guillamet & Kollef, 2024). VAP prolongs hospital stays, increases morbidity and mortality, and places a significant financial burden on healthcare systems due to extensive resource utilization. Between 15% and 50% of patients with VAP may die as a result of the infection.
One key factor contributing to the development of VAP is the introduction of bacterial organisms into the lower respiratory tract via an endotracheal tube, increasing the risk of pulmonary infections (Mohammad et al., 2024). VAP is defined as an infection that occurs in patients who are intubated and on mechanical ventilation for more than 48 hr. Clinical signs in affected patients include fever, respiratory distress, and purulent tracheal secretions (Kohbodi et al., 2023, Zubedeh, 2016).
VAP affects approximately 5% to 40% of patients who have been mechanically ventilated for more than 2 days. The incidence in North America is estimated at 1–2.5 cases per 1,000 ventilator-days, while in Europe, it is approximately 18.3 cases per 1,000 ventilator-days (Papazian et al., 2020). A multinational, prospective cohort study involving 70,115 patients from the Middle East, including 4,809 patients with VAP, reported an overall VAP incidence of 13% in the region (Rosenthal et al., 2023).
The latest guidelines on VAP prevention recommend six key strategies for patients on mechanical ventilation: (1) avoid intubation when possible, (2) minimize the duration of mechanical ventilation, (3) provide regular oral care, (4) elevate the head of the bed, (5) maintain ventilator circuits, and (6) properly select and manage endotracheal tubes (Klompas et al., 2022).
The literature evaluating nurses’ knowledge and practices regarding VAP reveals inconsistencies in classification and measurement of their adherence to prevention strategies (Rosenthal et al., 2023). In a U.S.-based study assessing the knowledge of evidence-based guidelines for VAP prevention among nurses, physicians, and respiratory therapists, all groups demonstrated high knowledge, with no significant differences between them (Stoesser et al., 2013). However, this finding contrasts with results from studies conducted in Egypt (Ali et al., 2013) and Ethiopia (Wami et al., 2018), which reported lower levels of knowledge and inconsistent practices among intensive care unit (ICU) nurses.
The significance of this research lies in understanding the current knowledge and practices of ICU nurses regarding VAP prevention strategies in Hebron hospitals. Such understanding may inform targeted interventions, educational programs, and policy improvements. Ultimately, this study aims to enhance ICU nurses’ knowledge and compliance, reduce the incidence of VAP, improve patient outcomes, and optimize the quality of care in Hebron hospitals.
The aim of this study was to evaluate ICU nurses’ knowledge of and compliance with VAP prevention strategies in Hebron hospitals and to identify differences based on gender, hospital type, and education level.
Review of the Literature
The guidelines for preventing VAP have the potential to influence nurses’ clinical practices. Their level of knowledge appears to be shaped by prior exposure to information, underscoring the need for ongoing in-service education and training programs to enhance understanding and adherence to these guidelines (Alkubati et al., 2023). The primary objectives of mechanical ventilation are to improve gas exchange (reverse hypoxemia and relieve acute respiratory acidosis), alleviate respiratory distress, enhance pulmonary mechanics (prevent and reverse atelectasis, improve compliance, prevent lung injury), promote lung and airway healing, and avoid complications (protect the lung and airway, prevent disuse respiratory muscle dystrophy) (Keyt et al., 2014).
VAP is one of the most common hospital-acquired infections in mechanically ventilated patients. It is associated with higher mortality rates, prolonged ICU stays, and increased healthcare costs. The prevalence of VAP is strongly linked to intubation and the presence of an endotracheal tube. Therefore, effective prevention strategies are critical and remain a serious concern for mechanically ventilated patients (Miller & Copplestone, 2018).
VAP is highly prevalent among critical care patients and accounts for more than half of the antibiotics administered in ICUs. According to the International Nosocomial Infection Control Consortium, the overall rate of VAP is 13.6 per 1,000 ventilator-days. However, this rate varies depending on patient demographics, risk factors, and hospital settings. VAP typically develops within 5 to 7 days after the initiation of mechanical ventilation, with a reported mortality rate ranging from 24% to 76% (Miller & Copplestone, 2018). Prolonged endotracheal intubation is the primary risk factor for VAP development (Forel et al., 2017). Immune compromised individuals, older adults, and patients with chronic conditions such as lung disease, malnutrition, or obesity are at increased risk (Bankanie et al., 2021).
In the context of Arab countries, several studies have examined ICU nurses’ knowledge of and adherence to VAP prevention strategies. For example, a study conducted in Yemen by Alkubati et al. (2023) reported that, despite moderate levels of knowledge, compliance with evidence-based guidelines was limited due to resource constraints and inconsistent protocol implementation. Similarly, a study in Jordan by Aloush and Alsaraireh (2018) found limited adherence to VAP prevention bundles among ICU nurses, largely due to the lack of structured training programs. In Egypt, Khalfallah et al. (2025) identified a substantial gap between nurses’ knowledge and actual clinical practice in VAP prevention. These findings underscore the need for standardized training initiatives and reinforced institutional policies across healthcare settings in Arabic countries to promote consistent and effective VAP prevention. Including these regional insights adds cultural and contextual relevance to the current study.
Aim of the study
This study aimed to evaluate ICU nurses’ knowledge of and compliance with VAP prevention strategies in Hebron hospitals. Additionally, the study sought to identify differences in knowledge and compliance based on gender, hospital type, and education level.
Methods
Study Design
This study employed a quantitative approach using a descriptive cross-sectional design.
Research Question
What is the level of knowledge and self-reported compliance of ICU nurses in Hebron hospitals with ventilator-associated pneumonia (VAP) prevention strategies, and what factors influence these outcomes?
Population, Sample, and Setting
The target population consisted of nurses working in adult ICUs in Hebron Governorate, Palestine. The expected sample size was 165 nurses, based on the total number of ICU nurses across six hospitals in the region. A consecutive sampling method was used, wherein all nurses working in adult ICUs at the following hospitals were invited to participate:
Halhul Governmental (President Mahmoud Abbas) Hospital (n = 11) Al-Mezan Specialized Hospital (n = 22) Al-Ahli Hospital (n = 80) Hebron Governmental Hospital (n = 36) Dura Governmental Hospital (n = 10) Abu Al-Hassan Al-Qasim Hospital (n = 6)
The rationale for using consecutive sampling was the limited number of ICU nurses in Hebron hospitals, totaling only 165.
Inclusion and Exclusion Criteria
Inclusion criteria
Currently working in an ICU
Minimum of 1 year of ICU experience
Experience caring for patients on mechanical ventilation
Exclusion criteria
Nurses temporarily assigned to the ICU during emergency staff shuffling
Nursing students completing ICU internships
Three nurses were excluded for not meeting the inclusion criteria, and two declined participation. Therefore, the final sample consisted of 160 ICU nurses. This breakdown reflects the staffing capacity and distribution across adult ICUs in the Hebron Governorate.
Ethical Considerations
Ethical approval for the study was obtained from the Palestine Polytechnic University ethics review committee (Approval No. EA.2024.25). Informed consent was obtained from all participants, with assurances of confidentiality and anonymity.
Data Collection
Data were collected using a self-administered questionnaire distributed to ICU nurses at the participating hospitals. Approval was first obtained from the university and then from each hospital. The researchers visited the ICU departments, explained the purpose of the study to the head nurses, and distributed the questionnaires to eligible participants.
Participants were informed about the study's objectives and assured that their participation was voluntary. Written consent was obtained prior to participation. Data collection occurred over a 3 week period in each hospital, primarily between the morning and evening shifts—when nurses were generally available. Nurses were asked to complete the questionnaire independently and honestly. Completion time was approximately 15 to 20 min. Researchers reviewed the completed questionnaires for completeness before submission.
The questionnaire was designed to assess ICU nurses’ knowledge and compliance with VAP prevention strategies and to explore potential differences related to demographic variables.
Instrument
Data were collected from ICU nurses using a structured questionnaire designed to assess nurses’ knowledge and evaluate their practices related to VAP prevention. The tool was used with permission from Meawed et al. (2021) after obtaining formal approval.
The questionnaire consisted of three sections:
Demographic information: This section collected data on participants’ age, gender, educational level, hospital type, number of years working in the ICU, and total years of professional nursing experience. Knowledge assessment: This section included 15 multiple-choice questions designed to measure nurses’ knowledge of VAP prevention strategies. Based on the scoring criteria established by Aziz et al. (2020), knowledge levels were categorized as follows:
Excellent: 81%–100% Good: 61%–80% Average: 41%–60% Poor: ≤40% Compliance assessment: This section comprised of 17 items measured using a 3-point Likert scale (1 = Never, 2 = Sometimes, 3 = Always). Compliance scores were interpreted using the following scale:
High compliance: 2.34–3.00 Moderate compliance: 1.67–2.33 Low compliance: 1.00–1.66
Pilot Study
Pilot testing was conducted with 30 ICU nurses from Al-Ahli Hospital to ensure the reliability and clarity of the questionnaire. The instrument demonstrated strong internal consistency, with a Cronbach's alpha coefficient of .85. Responses indicated that participants clearly understood the questions, and no modifications were required.
Study Period
The study was conducted from February to April 20.
Statistical Analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS), version 26. Descriptive and inferential statistics were employed to analyze the data.
Descriptive statistics included frequencies and percentages for categorical variables (e.g., gender, education level, hospital type) and means with standard deviations for continuous variables (e.g., age, years of ICU experience, total work experience). Inferential statistics included the following tests:
Spearman's correlation was used to assess relationships between continuous variables. Chi-square test was employed to examine associations between categorical variables. Mann–Whitney U test was used to compare differences between two independent groups based on continuous variables. Kruskal–Wallis test was used to examine differences in knowledge and compliance scores across multiple groups.
A significance level of P < .05 was used throughout the analysis. The results indicated statistically significant internal consistency among the 17 compliance items, confirming that they effectively measured the intended constructs.
Results
Sample Characteristics
The final sample consisted of 160 ICU nurses from six hospitals in Hebron, Palestine. Table 1 presents the demographic and professional characteristics of the participants. The majority of participants were male (68.1%), with a mean age of 28 years (SD = 5.17). Most nurses held a bachelor's degree (80.6%), and a majority worked in private hospitals (62.5%). The average ICU work experience was 4 years (SD = 3.92), and the total mean years of professional experience was 6 years (SD = 4.99).
Demographic and Professional Characteristics of ICU Nurses (N = 160).

Note. ICU = intensive care unit; VAP = ventilator-associated pneumonia.
Approximately half of the nurses (49.4%) reported receiving prior training in VAP prevention. Furthermore, 73.1% reported the existence of a VAP prevention protocol in their unit.
Strategies
Nurses’ knowledge of VAP prevention strategies was assessed using 15 multiple-choice questions shown in Table 2. The question with the highest percentage of correct responses was Question 10: “A nurse who is caring for a ventilated patient should wash hands?"—with 71.9% correctly identifying the answer: “before and after oral/endotracheal tube suctioning.”
Means and Standard Deviations of Compliance with VAP Prevention Guidelines.

Note. VAP = ventilator-associated pneumonia.
Conversely, Question 9 had the highest proportion of incorrect answers. Only 26.3% correctly selected the guideline-recommended frequency for changing ventilator circuits (“every new patient”), while 73.8% responded incorrectly, indicating a critical knowledge gap regarding equipment handling practices.
The total average of correct responses across all items was 50.96%, while incorrect responses totaled 49.04%, suggesting an overall moderate level of knowledge among ICU nurses.
Differences in Nurses’ Knowledge of Ventilator Care Bundle
The results revealed statistically significant differences in ICU nurses’ knowledge of the ventilator care bundle (VCB) based on gender, type of hospital, and educational level. Specifically, male nurses demonstrated significantly different knowledge levels compared to female nurses (P = .004). Similarly, nurses working in private hospitals had significantly different knowledge scores compared to those in governmental hospitals (P = .011). Furthermore, educational level was a strong predictor of knowledge, with those holding higher academic qualifications performing better (P = .001) as shown in Table 3.
Differences of Nurse's Knowledge of Ventilator Care Bundle According to Demographic Variables.

Kruskal–Wallis test (level of education)/Mann–Whitney test (gender, hospital type).
These P-values are all below the threshold of statistical significance (P < .05), indicating that gender, hospital type, and educational background are important variables influencing nurses’ knowledge of VCB guidelines.
From Table 4, the results revealed that there was a positive significant relationship between (age, total years of working experience) and nurses’ knowledge of VCB with r = .164, r = .163, respectively, with P = .038, .039. But there was no a significant correlation between years of experience at ICU and nurse's knowledge of VCB, with P = .159.
Spearman Correlation Between Nurse's Knowledge of and (Age, Duration of Experience).
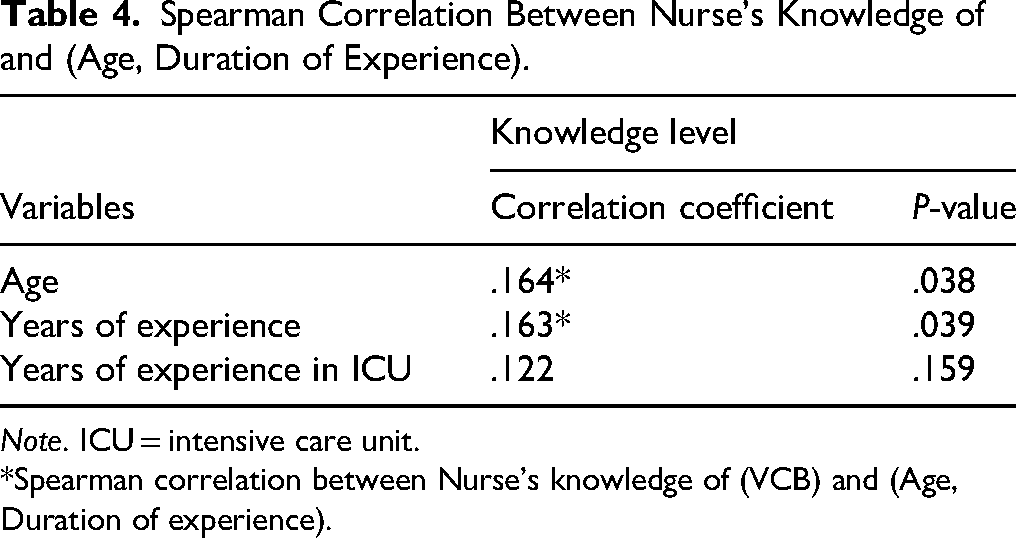
Note. ICU = intensive care unit.
*Spearman correlation between Nurse's knowledge of (VCB) and (Age, Duration of experience).
In Table 4, nurses’ self-reported compliance with VAP prevention strategies was assessed using a 17-item Likert scale. The overall mean compliance score was 2.55 (SD = 0.28), indicating a high level of adherence. Highest scoring practices included hand hygiene before (M = 2.83) and after patient contact (M = 2.80), use of gloves (M = 2.76), and patient positioning (semi-Fowler, M = 2.66). However, some practices showed only moderate compliance, such as the use of closed-circuit suction systems (M = 2.31) and changing ventilator circuits only when soiled (M = 2.32). These results highlight both strengths and gaps in current ICU nursing practice.
The Kruskal–Wallis test and Mann–Whitney test were conducted to check the differences of nurse's level of compliance to the VAP prevention strategies based on demographic variables. Table 5 displays the results.
Means VAP Prevention Guidelines.

Note. VAP = ventilator-associated pneumonia.
Evaluation key: 1–1.66 = low, 1.67–2.33 = moderate, 2.34–3 = high.
A Spearman correlation analysis was conducted to examine the relationship between nurses’ level of compliance with VAP prevention strategies and the variables age and duration of experience as shown in Table 6.
Differences of Level of Compliance to the VAP Prevention Strategies According to Demographic Variables.

Note. VAP = ventilator-associated pneumonia.
Kruskal–Wallis test (level of education)/Mann–Whitney test (gender, hospital type).
A Spearman correlation analysis was conducted to examine the association between the level of knowledge of VCB and the level of compliance to VAP prevention strategies. The results are presented in Table 7.
Spearman Correlation Between Nurse's Level of Compliance to VAP Prevention Strategies and (Age, Total Years of Working Experience, Years of Experience at ICU).

Note. VAP = ventilator-associated pneumonia; ICU = intensive care unit.
*Spearman correlation between Nurse's level of compliance to VAP prevention strategies and (Age, Total years of working experience, Years of experience at ICU).
In Table 8, the analysis showed that there was no significant relationship between the level of knowledge of VCB and the level of compliance to VAP prevention strategies, with P = .062.
Relationship Between Nurses’ Level of Knowledge of VCB and their Level of Compliance.

Note. VCB = ventilator care bundle.
Discussion
This study investigated the knowledge and self-reported compliance of ICU nurses in Hebron hospitals with VAP prevention strategies. The findings provide a comprehensive overview of knowledge gaps, adherence levels, and factors influencing compliance, reflecting broader challenges in implementing evidence-based infection control practices in clinical settings.
Knowledge of VAP Prevention Strategies
The study revealed that ICU nurses demonstrated moderate knowledge, with an overall correct response rate of 50.96%. The highest correct response (71.9%) was related to hand hygiene, which aligns with existing literature emphasizing its central role in infection prevention (Klompas et al., 2022). Conversely, a significant proportion (73.8%) answered incorrectly regarding the frequency of ventilator circuit changes, reflecting a critical knowledge gap. This finding is consistent with Grap et al. (2021), who reported inconsistencies among nurses in applying updated clinical guidelines regarding ventilator equipment maintenance.
The analysis showed significant differences in knowledge levels based on gender, hospital type, and educational level, with male nurses, those in private hospitals, and those holding higher degrees exhibiting greater knowledge. This could reflect differential access to training, continuing education, and institutional emphasis on evidence-based protocols (Bankanie & Outwater, 2021). Nurses with master's degrees had the highest knowledge scores (median = 0.7333), supporting prior studies indicating that advanced education enhances awareness of infection prevention protocols (Chakraborty et al., 2022).
Interestingly, age and total years of professional experience showed a modest positive correlation with knowledge (r = .164, P = .038; r = .163, P = .039), while ICU-specific experience did not (P = .159). This suggests that while general clinical exposure may contribute to knowledge acquisition, ICU-specific tasks require targeted, continuous training. This observation echoes findings by Piquilloud et al. (2021), who emphasized that experience alone is insufficient without structured education on updated guidelines.
Compliance with VAP Prevention Strategies
Despite moderate knowledge levels, nurses reported a high level of compliance (M = 2.55, SD = 0.28), particularly in hand hygiene (M = 2.83 before and M = 2.80 after patient contact) and maintaining a semi-Fowler position (M = 2.66). These practices are cornerstone elements of VAP prevention, reflecting effective implementation of basic control measures (Muscedere et al., 2019).
However, moderate compliance was observed in more technical practices such as the use of closed-circuit suction systems (M = 2.31) and ventilator circuit changes only when visibly soiled (M = 2.32). These findings mirror those of Al-Sayaghi (2020), who noted that nurses often struggle with the consistent application of protocol-driven tasks, often due to unclear guidelines, lack of training, or resource constraints.
Nurses from private hospitals reported significantly higher compliance levels (M = 2.64) compared to those in governmental hospitals (M = 2.47, P = .003). This could be attributed to institutional support, better staffing ratios, and more frequent in-service training in private settings (Abdelhamid & Khan, 2021). These disparities call for standardized policy enforcement across sectors to ensure uniform quality of care.
Interestingly, gender and education level did not significantly influence compliance scores, suggesting that adherence is more influenced by institutional practices than individual characteristics. This is supported by Meddings et al. (2020), who found that environmental and systemic support often outweigh personal attributes in promoting infection control behaviors.
Correlation Between Knowledge and Compliance
A key finding was the absence of a significant correlation between knowledge and compliance (r = .148, P = .062). This is consistent with Chang et al. (2021), who argue that knowledge alone does not ensure behavioral adherence due to barriers such as time constraints, institutional workload, and lack of reinforcement. Nurses may possess a theoretical understanding but fail to translate it into practice without conducive work environments.
This disconnect emphasizes the importance of multifaceted interventions that go beyond knowledge dissemination. For instance, simulation-based training, audit-feedback mechanisms, and leadership support have shown effectiveness in translating guidelines into clinical action (Al-Mugheed & Bani-Issa, 2022; Qtait, 2023).
Impact of Experience and Age on Compliance
Unlike knowledge, compliance was negatively correlated with age (r = −.202, P = .010) and total years of experience (r = −.156, P = .050), suggesting that younger nurses may be more responsive to protocols and updated evidence-based practices. This trend is supported by Meddings et al. (2020), who reported that newly trained staff often show higher adherence due to recent education and greater adaptability to change.
Surprisingly, ICU-specific experience had a positive correlation with compliance (r = .165, P = .037), indicating that those accustomed to ICU dynamics are more likely to follow structured practices. This supports the notion that targeted, role-specific experience, rather than general tenure, fosters the practical application of prevention strategies (Qtait & Sayej, 2016).
Limitations and Future Directions
One notable limitation is that the assessment of “practice” was based solely on self-reported compliance, without observational validation. This raises concerns about response bias and limits the generalizability of the results. Future studies should incorporate direct observation, performance audits, or clinical simulations for a more accurate assessment of actual behavior (Klompas et al., 2022).
Moreover, qualitative investigations could explore the barriers and motivators behind adherence or nonadherence to VAP prevention strategies, providing deeper insights into institutional and behavioral challenges.
Nursing Implications
The findings of this study underscore the importance of continuous education and training programs to enhance ICU nurses’ knowledge and compliance with VAP prevention strategies. Hospitals should implement standardized protocols, ensure adherence to the VCB, and conduct regular competency assessments to maintain high standards of practice.
The significant differences observed based on hospital type and education level suggest the need for targeted interventions, particularly in private hospitals and among nurses with diploma-level education. Additionally, infection control teams should prioritize strengthening hand hygiene practices and advocate for the use of observational methods to enforce guidelines.
Future research should explore the barriers to compliance and effective educational strategies to improve VAP prevention. Addressing these challenges will ultimately enhance patient outcomes and reduce healthcare-associated infections.
Implications and Recommendations
The findings of this study have practical implications for clinical education, hospital policy, and infection control.
Structured and continuous training: Regular in-service training programs tailored to ICU protocols are essential. These should focus on evidence-based guidelines and hands-on applications (Alkubati et al., 2023).
Standardization across institutions: Policy harmonization between governmental and private hospitals could address disparities in knowledge and compliance. Hospital leadership must invest in institutional support to enforce guideline adherence (Abdelhamid & Khan, 2021).
Audit and feedback mechanisms: Incorporating real-time feedback and routine audits can help bridge the gap between knowledge and practice (Chakraborty et al., 2022).
Resource provision: Ensuring the availability of necessary supplies (e.g., chlorhexidine, closed-circuit suction systems) is crucial for enabling compliance.
Conclusion
The study reveals a moderate level of knowledge (50.96%) among ICU nurses regarding VAP prevention strategies, with significant differences based on gender, hospital type, and educational level. However, despite these knowledge gaps, overall self-reported compliance was high (M = 2.55), particularly for basic infection control practices like hand hygiene and patient positioning.
There was no significant correlation between knowledge and compliance (P = .062), suggesting that higher knowledge does not necessarily translate into better practice. Notably, compliance was higher in private hospitals (P = .003), while age and general work experience negatively correlated with compliance, indicating that younger and less experienced nurses reported higher adherence to VAP protocols.
These findings emphasize the need for standardized training and institutional reinforcement, particularly in public healthcare settings, to ensure consistent and evidence-based application of VAP prevention practices across ICU settings.
Supplemental Material
sj-docx-1-son-10.1177_23779608251349956 - Supplemental material for Knowledge and Practices of Intensive Care Unit Nurses Related to Prevention of Ventilator-Associated Pneumonia Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251349956 for Knowledge and Practices of Intensive Care Unit Nurses Related to Prevention of Ventilator-Associated Pneumonia Cross-Sectional Study by Nesreen Alqaissi and Mohammad Qtait in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608251349956 - Supplemental material for Knowledge and Practices of Intensive Care Unit Nurses Related to Prevention of Ventilator-Associated Pneumonia Cross-Sectional Study
Supplemental material, sj-doc-2-son-10.1177_23779608251349956 for Knowledge and Practices of Intensive Care Unit Nurses Related to Prevention of Ventilator-Associated Pneumonia Cross-Sectional Study by Nesreen Alqaissi and Mohammad Qtait in SAGE Open Nursing
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all individuals who have contributed to this research. We are grateful to the participants for their cooperation.
Ethics Approval
This study was conducted in accordance with ethical principles outlined by Palestine Polytechnic University ethical board. Ethical approval was obtained from Palestine Polytechnic, and informed consent was secured from all participants number (Rec,112.2024).
Informed Consent
Written informed consent was obtained from each participant. Participation remained anonymous and data were treated with confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study would be available upon reasonable request from the principal investigator.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.