
Abstract
Introduction
Iron deficiency anemia during pregnancy is a significant public health problem in low- and middle-income countries. The World Health Organization recommended a daily oral dose of iron and folic acid supplements throughout pregnancy. Poor adherence to iron and folic acid supplementation arises in pregnant women associated with serious adverse health outcomes.
Objective
This study aimed to assess iron–folate adherence and associated factors among pregnant women in public health facilities of Durame town, Southern Ethiopia, in 2022.
Methods
An institution-based cross-sectional study was conducted from March 1–30, 2022. A structured interviewer-administered questionnaire was used to interview a total sample size of 317 participants. Logistic regression analysis was computed, and variables with a p-value of less than 0.25 in the bivariate logistic regression analysis were selected for multivariable logistic regression analysis. Finally, significance was declared at p < .05 with 95%CI.
Results
The findings of this study showed that adherence to iron–folate among pregnant women was 180 (60%) (95%CI: 54–65.7). The odds of iron–folate adherence among women who had not had anemia in their current pregnancy were 63% (AOR = 0.37, 95%CI: 0.14–0.99) less likely to have adherence, and the odds of iron–folate adherence among women who had not heard about the disease anemia were 58% (AOR = 0.42, 95%CI: 0.22–0.81) less likely to have adherence.
Conclusion
Iron–folate adherence in Durame public health facilities was better compared to other studies even if it was not high enough to prevent anemia and folate deficiency. Women who had not had anemia in their current pregnancy and women who had not heard about the disease anemia were significantly associated with adherence to iron–folate. Thus, healthcare providers should provide health education on the enhancement of adherence to iron–folate utilization and the means how to prevent iron–folate deficiency during their clients’ pregnancy.
Background
Anemia is a prevalent public health issue linked to a higher risk of morbidity and mortality among young children and pregnant women (WHO, 2012). The World Health Organization (WHO) defines anemia among pregnant women as having hemoglobin levels of less than 11.0 g/dl (WHO, 2016). Physiological changes in women during pregnancy, fetal growth, and fetal development increase the requirement for iron and folic acid (IFA). The probability of presenting iron and folate deficiency is high if the diet is not supplemented with IFA tablets during pregnancy (Martí-Carvajal et al., 2002).
IFA adherence measures how closely clients fulfill the dosage and timing of IFA supplements as advised by their healthcare providers (WHO, 2015). If a woman takes 65% or more of the IFA supplement, which equates to taking the supplement at least 4 days a week, she is considered adherent to the supplement (Marcewicz et al., 2018).
Iron deficiency anemia is a disorder where the body produces a smaller amount of red blood cells due to a lack of iron (WHO, 2015). Anemia occurs when the blood's hemoglobin concentration is less than usual due to a lack of one or more crucial nutrients (WHO, 2016).
Antenatal mothers are among the risk groups for anemia due to low iron stores in their bodies. This is supported by reports from the WHO, indicating that anemia affected 38.2% of pregnant women globally and 46.3% in Africa (Elysium, 2011). Concerning the prevalence of anemia among Ethiopian reproductive-age women, it is estimated that 24% of them are anemic (Zerfu, 2016). To reduce the risk of maternal iron deficiency anemia, the WHO recommended a daily oral dose of 60 mg of iron and 400 μg folic acid supplements throughout pregnancy, to begin as early as possible as a routine part of antenatal care (ANC) (WHO, 2016). Several studies have reported that the utilization of IFA supplementation during pregnancy reduces the risk of fetal, neonatal, and childhood mortality by preventing maternal anemia, low birth weight, and premature and preterm delivery (Malek et al., 2016). Despite this fact, WHO recommends providing all pregnant women with a standard dose of 60 mg of iron and 400 μg of folic acid supplementation for 6 months daily to prevent maternal anemia and neonatal neural tube defects (WHO, 2016). Adherence to IFA supplement during pregnancy is poor and has not improved significantly in the last decades among low- and middle-income countries. The study conducted in South Australia showed that 23% of pregnant mothers adhered to IFA supplementation (Titilayo et al., 2010). In Malawi, 37% of pregnant mothers consumed the ideal minimum of 180 IFA tablets (WHO, 2012), (Birhanu et al., 2018). Another study done at the University of Gondar, in Northwest, Ethiopia, reported that 55% of pregnant women adhered to the recommended IFA supplementation (WHO, 2016).
Pregnant mothers who had poor adherence to IFA supplementation could develop anemia during the antenatal period. Maternal anemia might cause low weight gain, preterm labor, congestive heart failure, lower resistance to infection, bleeding, and poor cognitive development. Similarly, folic acid deficiency during pregnancy is also associated with an increased risk of neural tube defect, preeclampsia, fetal malformations, and preterm delivery (FMOH, 2020). According to a national survey report, Ethiopia in 2004 adopted the global IFA supplementation strategy targeting to reduce the prevalence of iron deficiency anemia in women of reproductive age and children under five by one-third, which is expected to be achieved through distributing IFA supplements during ANC visits (Office, 2017). Increases were observed in the prevalence of anemia from 17% to 24% in the last 5 years among pregnant women, and the coverage of IFA supplementation during pregnancy has improved from 1% to 5%, but remains at the substandard level as only 5% of pregnant women were taking IFA tablets for 90 days or more during their most recent pregnancy in Ethiopia (SSAE, 2017; Zerfu, 2016).
The reasons for poor adherence to IFA supplementation arise from pregnant women's behavior such as misunderstanding of instructions, side effects, frustration about the frequency and number of pills taken, nausea, and constipation, which might make the intervention inadequate to reduce anemia among pregnant women (WHO, 2016). Taking into account the existing problem under study, which is a public health problem in Ethiopia, this work provided up-to-date information concerning the magnitude and associated factors of IFA adherence among the study population. Thus, this study aimed to assess the proportion of adherence and associated factors of IFA supplementation among pregnant women attending ANC in public health facilities of Durame town, Southern Ethiopia.
Literature Review
Proportion of Iron–Folate
Daily IFA supplementation is currently recommended by WHO as part of ANC, to reduce the risk of low birth weight, maternal anemia, and iron deficiency (WHO, 2021). Iron deficiency anemia during pregnancy is a significant public health problem in Sub-Saharan Africa and is associated with serious adverse health outcomes (Ba et al., 2019). A systematic review and meta-analysis conducted in Sub-Saharan Africa showed that the overall prevalence of IFA supplementation in pregnancy was 39.2% (Fite et al., 2021). A similar study conducted in Sub-Saharan Africa revealed that the overall prevalence of adherence to ≥90 days of iron supplementation during pregnancy was 28.7%, ranging from 1.4% in Burundi to 73.0% in Senegal (Ba et al., 2019). A cross-sectional study conducted in Tanzania showed that 20.3% of respondents have adhered to IFA supplementation (Lyoba et al., 2020). A similar study conducted at public hospitals in Jigjiga Town, Somali Region, in 2020 revealed that 54.9% of pregnant women were adherent to IFA supplementation (Ridwan & Shafi, 2021b). Another similar study conducted in Ethiopian public health facilities during the COVID-19 pandemic showed that 56.5% of pregnant women have adhered to IFA supplementation (Tefera et al., 2023). A study conducted in Adwa town, Tigray, showed that 40.9% of participants were adherent (took four or more tablets per week) to IFA supplementation (Gebremichael & Welesamuel, 2020). A similar study conducted in Armachiho Health Centers, Northwest, Ethiopia, showed that adherence to IFA was 28.7% (Agegnehu et al., 2019). A study conducted in public health facilities in Northwest Ethiopia showed that about 52.8% of pregnant women attending ANC clinics were adherent to IFA supplementation (Demisse et al., 2021). A study conducted in Aykel town, Northwest Ethiopia, showed that the rate of adherence to IFA supplementation among pregnant women was 47.6% (Assefa et al., 2019). A study conducted in Northwest Ethiopia showed that 163 (51.4%) of the respondents were adherent to IFA supplementation (Boti et al., 2018). A study conducted at Debre Tabor General Hospital showed that 39% received IFA supplementation counseling, and 52% had some knowledge of IFA supplementation (Gebremariam et al., 2019).
Factors Associated With Iron–Folate Adherence
A systematic review and meta-analysis conducted in Sub-Saharan Africa showed that women who were counseled on IFAS during their courses of pregnancy, women who knew IFAS, women who knew about anemia, and women who had received a fourth visit for ANC (Fite et al., 2021). A similar study conducted in Sub-Saharan Africa revealed that those receiving ≥4 ANC visits, had secondary or higher education, and older women aged 35–49 years were significant factors for iron–folate adherence (Ba et al., 2019). A study conducted in Jigjiga Town showed that the time to start ANC, knowledge of anemia, counseling on the importance of the iron–folic acid, IFAS given during clinical visits, number of meals consumed, number of children, and distance to health facility were independernt predictors of adherence to IFA supplementation (Lyoba et al., 2020). A study conducted in Ethiopia's public health facilities during the COVID-19 pandemic showed that mothers with primary education, urban resident mothers, mothers who had four or more ANC visits, mothers who had registered for their first ANC at early gestational age, and mothers who had good awareness about birth defects were independent predictors of adherence to IFA supplementation (Tefera et al., 2023). A study conducted in Jigjiga Town showed that secondary and above-educated women, women who had more than four ANC visits, and knowledgeable women about IFA supplements were significant factors for iron–folate adherence (Ridwan & Shafi, 2021b). A study conducted in Adwa town, Tigray, Ethiopia, showed that women in the age group of 25–29 years, women who received nutrition counseling, women who had satisfactory knowledge, and women currently having anemia had statistically significant associations with adherence to IFA supplementation (Demisse et al., 2021). A study conducted in Aykel town, Northwest Ethiopia, showed that pregnant women who had a history of abortion, had knowledge of anemia, and received health education were more likely to be adherent with IFA supplementation. Furthermore, knowledge about the benefits of the supplement and not facing any problems in the health facilities during IFA tablet collection were the factors associated with IFA supplementation adherence (Assefa et al., 2019). In a study conducted in Burji Districts, Segen Area People's Zone, Southern Ethiopia, the maternal educational status, history of anemia during the current pregnancy, and knowledge about IFA were significant factors for IFA adherence (Boti et al., 2018). A study conducted in Debre Tabor General Hospital in Ethiopia showed that gravidity, gestational age at the first ANC visit, pregnant women who got advice about IFAS, current anemia, and had knowledge about IFAS were statistically associated with adherence to IFA supplementation among pregnant women (Alemayehu et al., 2019).
Methods
Study Setting
This study was conducted in Durame town public health institutions, Kembata Tembaro Zone, Southern Ethiopia. Durame town is surrounded by Damboya woreda. It is located at a distance of 116 km to the north of Hawassa, the capital city of the South Nation Nationality People Region (SNNPR), and 350 km south of Addis Ababa, the capital city of Ethiopia. The town administrative has three kebeles. Based on the 2007 Census conducted by the CSA, this Woreda has a total population of 24,472 of which 12,173 are men and 12,299 are women (Gebremedhin et al., 2014). The town administrative has one general hospital and two health centers, and those facilities have been providing ANC, delivery, and postnatal care services.
Study Design and Period
An institution-based cross-sectional study design was conducted from March 1–30, 2022.
Operational Definition
Pregnant women who had taken the IFA tablet at least 4 days a week were classified as adhering to IFA supplementation, and pregnant women who had taken less than 4 days a week were classified as not adhering to IFA supplementation (WHO, 2021).
Research Questions
What is the prevalence of adherence to IFA supplementation among pregnant women?
What are the factors associated with adherence to IFA supplementation among pregnant women?
Population
All randomly selected pregnant mothers who were attending the ANC clinic at Durame town general hospital and health centers were the source of population. Pregnant mothers who had at least a second ANC visit for the present pregnancy and received IFA tablets for at least 1 month were included in the study. Pregnant mothers who came for the first ANC visit and were critically ill during the data collection period were excluded.
Sample Size Determination
The single population proportion sample size calculation formula was used to estimate the required sample size with assumptions of 95%CI, 5% margin of error, (p = 74.9%) established prevalence from previous studies on utilization of iron supplementation during pregnancy in eight rural districts of Ethiopia (Gebremedhin et al., 2014), adding a 10% non-response rate. Based on the above assumption consideration, the final sample size became (n = 317).
Sampling Techniques
After the proportional allocation of pregnant women from one general hospital and two health facilities, a systematic random sampling technique was employed to include a sample of 317 participants. The sampling fraction (K) was; N/n = 930/317 = 3. Then, the lottery method was employed to identify the first pregnant women to be interviewed, and three were drawn as the first pregnant women to be interviewed. Consequently, women were identified, and an interview was held every three intervals.
Variables and Data Measurement
The dependent variable was adherence to IFA supplementations. The independent variables were as follows: socio-demographic characteristics (age, marital status, economic status, family size, residence, and level of education); obstetric characteristics (gravid, parity, ANC visit, abortion, stillbirth, and ANC follow-up started time); and women awareness: healthcare system-related characteristics (the problem faced in the facility, shortage of supplementation within the facility, health education, and collected tablet per visit).
Data Collection Instrument and Procedure
The data collection tool was prepared in English after reviewing related literature and then translated into the Amharic language. The questionnaire consisted of socio-demographic characteristics, obstetric characteristics, women's awareness, physical attribute-related characteristics, and healthcare system-related characteristics.
Data were collected using a pre-tested structured interviewer-administered questionnaire from the study participants. To assure the quality of data, two experienced BSc midwives were trained for data collection, and two BSc nurses were assigned as a supervisor under the supervision of the principal investigator. Filled questionnaires were daily checked for completeness and consistency. The reliability of the questionnaire was checked by Cronbach's alpha value, which was 0.82.
Data Quality Control
Data quality management was started during questionnaire development by translating the questionnaires prepared in the English language into the Amharic language. Before data collection, training was given to data collectors regarding the objective of the study and the inclusion and exclusion criteria of the study. Data quality was assured in pre-analytic stages, during analytic stages, and in postanalytic stages; data was checked for documentation and completeness.
Statistical Analysis
Data entry, cleaning, and screening were done exclusively by the principal investigator and co-investigators. The edited and cleaned data were entered into Epi Data version 3.1 and exported to SPSS version 26 for analysis. Descriptive statistics were performed using frequency tables and graphs; percentages and the presence of associations were determined by using the X2-test. Logistic regression analysis was computed to identify those adhered to IFA supplementation from the independent variables. Variables with a p-value of less than 0.25 in the bivariate logistic regression analysis were selected for multivariable logistic regression analysis. Finally, significance was declared at p < .05 with 95%CI.
Result
Socio-Demographic Characteristics
In this study, a total of 317 participants were involved; from them, 300 participants were included with a response rate of 94.64%. About half of the participants’ age range was between 26 and 35. In addition to this, almost all of the participants were married (296, 98.7%) (Table 1).
Socio-Demographic Characteristics of the Study Participants in Durame, Southern Ethiopia, 2022 (N = 300).

Obstetrics-Related Characteristics
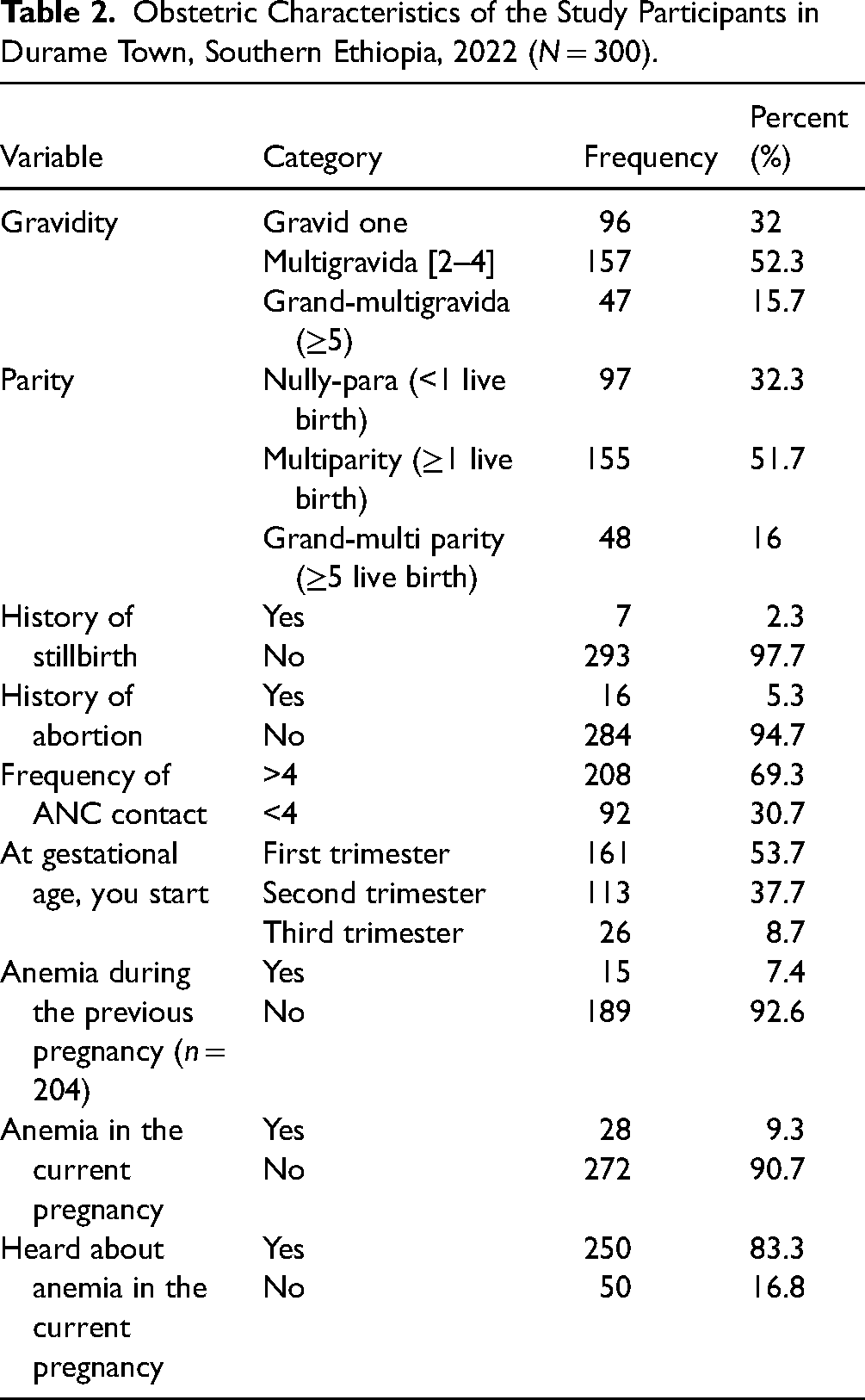
About half of the participants (157, 52.3%) were multigravida, and two-thirds of the participants (208, 69.3%) had ANC contact more than four times. Most of the participants (293, 97.7%) had no history of stillbirth (Table 2).
Obstetric Characteristics of the Study Participants in Durame Town, Southern Ethiopia, 2022 (N = 300).
Iron–Folate-Related Characteristics
This study comes up with IFA adherence of 180 (60%) (95%CI: 54–65.7) in Durame public health facilities (Figure 1). Of the total participants, about 236 (78.7%) had heard about IFA (Figure 1).

Iron–folate supplementation in Durame town public health facility, 2022 (N = 300).
Factors Influencing Iron–Folate Adherence
In bivariate analysis, the place of residence, educational status of the pregnant mother, anemia status in the current pregnancy, and hearing about anemia were candidates for multivariate analysis. In the final model, only anemia status in the current pregnancy and hearing about anemia were found to be statistically significant (Table 3).
Bivariate Analysis of Adherence of Iron and Folic Acid in Durame Town, Southern Ethiopia, 2022 (N = 300).

*p-value <.05, **p-value <.01.
The odds of IFA adherence among women who had not had anemia in their current pregnancy were 63% (AOR = 0.37, 95%CI: 0.14–0.99) less likely to have adherence compared to those who had anemia in their current pregnancy. Similarly, the odds of IFA adherence among women who had not heard about the disease anemia were 57% (AOR = 0.43, 95%CI: 0.22–0.81) less likely to have adherence compared to those who had heard about the disease anemia.
Discussion
IFA supplementation is a routine task of clinicians working in maternal and child health units in Ethiopia. Even if there were routine offerings, it is not known whether the clients are using them appropriately or not. With this idea in mind, this study was conducted in Durame public health facilities, and it brings the following magnitude and factors that may influence the adherence to IFA supplementation.
This study comes up with IFA adherence of 80 (60%) (95%CI: 54–65.7) in Durame public health facilities. Contrary to this study, a study conducted in Burji Districts, Segen Area People's Zone, revealed that adherence to IFA supplementation was 51.4% (Boti et al., 2018). Similarly, other studies reported that adherence to IFA supplementation was 44% in Debre Tabor General Hospital (Gebremariam et al., 2019), 47.6% in Aykel town (Assefa et al., 2019), and 52.8% in public health facilities in Northwest Ethiopia (Demisse et al., 2021).
IFA supplementation adherence was better in the current study; this difference might be due to the current increased information-delivering mechanisms of the health system. This study also shows that information was key to IFA supplementation adherence. Moreover, those delivery mechanisms might bring up a higher understanding of the community about anemia and folate deficiency.
In this study, the odds of IFA adherence among women who hadn't anemia in their current pregnancy were less likely to have adherence compared to those who had anemia in their current pregnancy. Consistently other studies state that IFA supplementation adherence was more likely among participants who had anemia during the current pregnancy in Southern Ethiopia (Boti et al., 2018), in Debre Tabor General Hospital (Gebremariam et al., 2019), and public health facilities in Northwest Ethiopia (Demisse et al., 2021).
This might be due to the right information delivered by health professionals when they treat their clients. In addition to this, when clients already had the disease, professionals might give due emphasis to counseling them to have a good prognosis. On the other hand, it might be due to when clients know that they have the disease, they may have a better follow-up to care for themselves.
This study showed that the odds of IFA adherence among women who had not heard about the disease anemia were less likely to have adherence compared to those who had heard about the disease anemia. In the same manner, other studies conducted among pregnant women state that women who have good knowledge of anemia were more likely to have IFA supplementation adherence (Boti et al., 2018; Demisse et al., 2021; Gebremariam et al., 2019; Getachew et al., 2018; Ridwan & Shafi, 2021a).
This might be because when people know about the disease, they may react accordingly. If they had already known about how harmful anemia and folate deficiency is, they may stick with the prescription orders given to them to prevent the disease.
Strengths and Limitations
This study includes pregnant women who had at least a second ANC visit for the present pregnancy and received IFA tablets for at least 1 month to assess adherence to IFA and associated factors, and compares results with other related studies. This study is limited to the population in Southern Ethiopia and does not have results that can be applied to the broader population of pregnant women. The limitation of this study related to the study types and nature of the cross-sectional study, which did not draw inferences and show cause-and-effect relations among dependent variables and independent variables. The study is to some extent limited because it is based on retrospective information provided by the respondents, which may be subject to recall bias. Nevertheless, such bias was minimized to some extent by restricting the study to mothers who gave birth within 1 year of the survey.
Implications for Practice
The reasons for poor adherence to IFA supplementation arise from pregnant women's behavior such as misunderstanding of instructions, side effects, frustration about the frequency and number of pills taken, nausea, and constipation, which might make the intervention inadequate to reduce anemia among pregnant women. The findings of this study have several impacts to prevent iron deficiency anemia and folate deficiency during pregnancy. This study revealed the factors associated with IFA adherence among pregnant women that give clues to improving service provision for pregnant women during the antenatal period. All stakeholders like the Minister of Health (MOH), NGOs, zonal health offices, and hospital and health center managers should improve the availability and accessibility of IFA supplementation to improve poor adherence to IFA utilization among pregnant women. Pregnant women are responsible for implementing IFA utilization protocols and positive coping strategies to prevent iron deficiency anemia and infants suffering from folic acid deficiency (neural tubal defects).
Conclusion and Recommendation
The overall proportion of adherence to IFA among pregnant women in this study was 180 (60%). This implies that many mothers continue to practice in contravention of WHO guidelines, and more work is needed to promote adherence to IFA usage during the antenatal period in healthcare institutions and in the community. The place of residence, educational status of the pregnant mother, anemia status in the current pregnancy, and hearing about anemia had a statistically significant association with adherence to IFA in bivariate logistic regression analysis. Women who had not had anemia in the current pregnancy and women who had not heard about the disease anemia were significantly associated with adherence to IFA in multivariate logistic regression analysis. Thus, healthcare providers should provide health education on the enhancement of adherence to IFA utilization and the means how to prevent IFA deficiency during their clients’ pregnancy.
Footnotes
Acknowledgment
The author(s) would like to acknowledge the Wolkite University College of Medicine and Health Science, Durame town health institution leaders, and data collectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This research is done in compliance with the Declaration of Helsinki's ethical principles for medical research involving human subjects. Ethical approval was obtained from the Institutional Ethical Review Board (IERB) of the School of Midwifery, Wolkite University with reference number CMHS/IRB's 0025/2021. A letter of permission was obtained from the Durame Zone Health Bureau and respective hospitals. The purpose of the study was informed to mothers/caregivers. Furthermore, it is affirmed to mothers or caregivers as they have the right to decline to participate in the study or not to respond to any item, which they do not want in the interview, and their participation in the study or refusal to participate has no any influence on the care provided in the hospital. Informed written consent was obtained from the mother by the granted ethical approval letter from the Wolkite University Department of Midwifery.