
Abstract
Introduction
Diabetes mellitus (DM) is a main, highly prevalent, and challenging public health issue. Suboptimal self-care for type II diabetes can lead to poor glycemic control, complications, and even death.
Objective
This study investigated the incidence of distress and its link with self-care habits of patients with diabetes type II.
Methods
A correlational, cross-sectional design with a convenient sample of 200 patients was used to conduct this study. Three questionnaires were administered: (A) the demographic and medical data questionnaire; (B) diabetes self-care activities in brief; and (C) the diabetes distress scale in Arabic language.
Results
The patients’ mean age was 51.78 ± 11.34; 80% of patients practiced lower levels of diabetes self-care, and 37% of them had a high level of diabetes distress. Self-care is associated with diabetes distress (R = −0.152, p-value = .032).
Conclusion
Self-care activities can help in the early detection and management of diabetes distress. Sustained self-care education is promising to minimize diabetes distress. The potential advantages of association between diabetes distress and self-care can offer self-care programs that enhance diabetes distress management.
Introduction/Background
Diabetes mellitus (DM) represents a main prevalent challenging disease in the 21st century (Yari et al., 2023). According to the International Diabetes Federation (IDF, 2021), 537 million adults are living with diabetes globally. The prevalence of diabetes has reached 10.5%, with almost half (44.7%) of adults undiagnosed. IDF projections show that by 2045, 783 million adults will be living with diabetes—or one in eight adults. A rise of 16% (74 million) since the previous IDF estimates in 2019 (Saeedi et al., 2019).
Diabetes represents a chronic illness that affects people on a socioeconomic, mental, and physical level (The daily burden of managing a condition significantly influences patients’ emotional health. A significant psychosocial issue for persons with diabetes is diabetes distress (Arditi et al., 2019; Quinn et al., 2017).
Review of Literature
A previous meta-analysis demonstrated that the overall prevalence of diabetes distress was 36% globally (Perrin et al., 2017a, 2017b). Diabetes distress primarily refers to the negative emotional or affective experiences brought by the challenges of living with diabetes resulting from social and financial effects (Pintaudi et al., 2015).
Foot ulceration is a main complication of DM and is associated with high levels of morbidity and mortality, as well as significant financial costs. In developing countries, foot ulcers and amputations are unfortunately very common (Hirpha et al., 2020). In the course of their lives, nearly one-third of patients with diabetes may develop a diabetic foot ulcer (DFU) (Lane et al., 2021).
Patients with diabetes often experience emotional distress because they must make significant lifestyle changes. The instructions from healthcare professionals can be complex and difficult to understand, especially for those without a medical background, which adds to their emotional burden (Todalabagi et al., 2020). Additionally, diabetes distress was found to be a predictor of foot care (Yari et al., 2023).
DM needs comprehensive, lifetime self-management on the part of the patient (Centers for Disease Control and Prevention (CDC), 2020). Patients or families manage most day-to-day diabetes treatment; hence, there is a critical need for reliable and effective diabetic self-management tools (Todalabagi et al., 2020).
Diabetes self-care necessitates extensive diet and lifestyle changes from the patient, together with the assistance of the healthcare team, to maintain a higher degree of self-confidence and successfully modify behavior. Chronic diabetes often requires regular follow-ups from healthcare providers to maintain metabolic control and avoid long-term complications (Yari etal., 2023). Hence, the nursing role is essential to patients’ understanding of their demands and needs with appropriate self-care activities (Schmitt et al., 2021).
Several studies have discussed that inadequate self-care in diabetes accounts for the fear of diabetes complications (as a major stressor) and reduces the quality of life (Berry et al., 2018; Perrin et al., 2017a, 2017b; Sharif-nia et al., 2022). Therefore, self-care becomes an essential component of health maintenance to prevent and delay any diabetes-related problems (Summers-Gibson, 2021).
Significance of Study
Diabetes control is still diminished and the economic impact of this disease is extensive (Shelbaya et al., 2020). A recent study concluded that only 5% of the patients had good glycemic control. Suboptimal levels of diabetes self-care activities had been detected in the study (Mohamed et al., 2023).
Patients with diabetes have a higher likelihood of experiencing diabetes distress, which can lead to macrovascular and microvascular complications and a higher risk of mortality within a certain time frame after developing a foot ulcer (Polikandrioti et al., 2020; Yari et al., 2023).
Recently, numerous studies that engaged in self-care-oriented behavior to help promote better stress management had been proposed (Rose et al., 2022; Xu, 2020; Yu et al., 2020). Despite the recommendation, the relationship between self-care and diabetes distress has not been addressed well.
Additionally, to guide interventions toward improving self-care and health outcomes, it is crucial to identify factors linked to problematic diabetes self-care. Discovering how self-care with less stress is helpful for nurses as clinicians and researchers in developing and refining methods to treat and measure diabetes distress is an urgent issue. Therefore, this research
Theoretical Framework
Orem's theory of self-care directed this study. The theory is based on the concept that self-care is a human regulatory function, and the person deliberately achieves defined elements to adjust his or her own functioning (Patrcia et al., 2021). The human regulatory function includes prerequisites that are required for continuing life and growth such as air, water, and food. It incorporates additionally purposeful actions toward maintaining internal and external conditions needed to promote health (Summers-Gibson, 2021). This study examined the influence of internal conditioning factors (diabetes distress) on self-care among adult patients with diabetes type II.
The application of Orem's theory of self-care to the study variables is illustrated in Figure 1. As can be seen, the figure begins with the baseline self-care requisites that every person must possess and then move to health-deviated self-care requisites when a person is diagnosed with diabetes type II as well as will acquire therapeutic self-care requisites, whereas the internal condition factor of diabetes distress is illustrated as the main influencing factor on self-care activities.
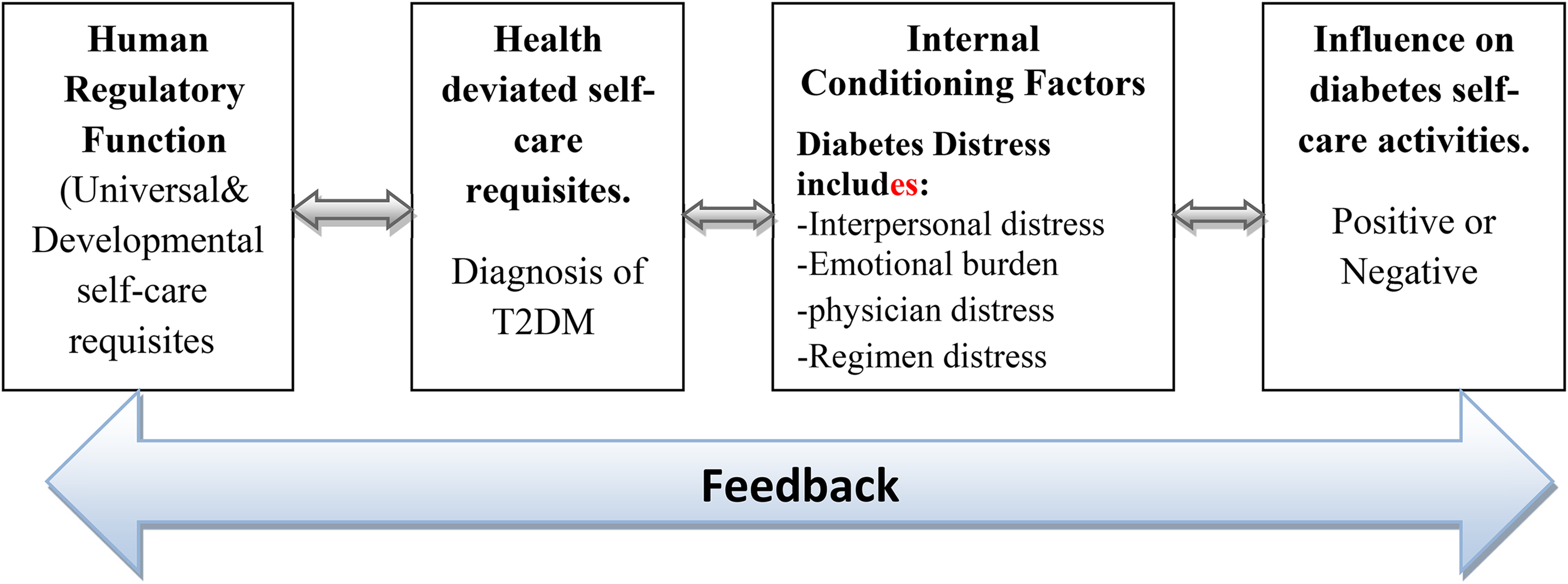
Application of Orem's theory of self-care concepts in the current study.
Methods
Research Design
A correlation and cross-sectional design were employed to achieve the research aim. This study aimed to describe variables and explore the association between variables in one or more populations.
Research Question
To what extent is there a relationship between diabetes distress and self-care activities?
Sample
A convenient sample of 200 patients with diabetes type II who met the inclusion criteria participated in the study.
Sample Size Calculation
The number of participants was 200 patients based on the following equation with (95% significance level):

Inclusion/Exclusion Criteria
Subjects who met the inclusion criteria for this study will be included as follows: (1) patients who are literate and could communicate; (2) had diabetes type II, diagnosed by a physician; (3) patients who are older than 18 years; (4) patients with mental disorders or refused to participate were excluded.
Settings
The current study was conducted at inpatients and outpatients’ clinics in certain Cairo University hospitals. These hospitals serve patients with chronic illnesses from different governorates. Data was collected from both inpatient (providing medical management, health services, and monitoring for patients with diabetes) and outpatient clinics (diagnosis, follow-up, laboratory, radiology, dressing, and medication services for DM).
Data Collection Measures
Data were collected using the following three tools:
The demographic and medical data questionnaire: It was designed by the researchers to collect variables such as marital status, gender, education, age, occupation, and time since the diagnosis of diabetes. Summary of diabetes self-care activities (SDSCA): It consisted of 12 short self-report items that assessed the following components of diabetes self-care over the previous seven days: foot care (four items), exercise (two items), nutrition (four items), and blood-glucose testing (two items) (Toobert et al., 2000).
Scoring System
The subjects were required to rate how many days during the previous 7 days they had engaged in a particular form of self-care. The scale was between 0 and 7, with higher scores indicating higher diabetes management activities. For each domain, a mean score was generated, and scores were labeled as “good” or “bad,” depending on whether they were above or below the mean value. The mean score was determined by adding the average scores for each exercise, blood glucose testing, foot care, and diet and dividing those results by four (Gebre et al., 2019). The patient was categorized as having “bad self-care practice” if it was <3 or having “good self-care practice” if their overall mean score was ≥ 3.
Reliability
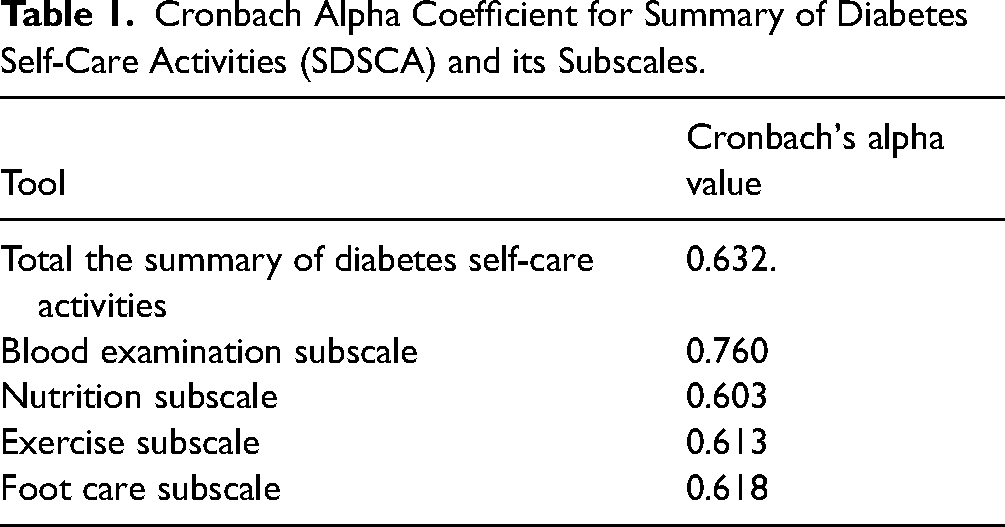
The test–retest reliability for the Arabic version of the summary of diabetes self-care activities was 0.912 (p < .001). The split-half reliability was 0.9, and Cronbach's alpha (α) was 0.76. The alpha scores for the subscales were as follows: foot care (0.77), exercise (0.83), blood-glucose testing (0.92), and diet (0.89) (AlJohani et al., 2016). In the current study, the internal consistency of the tool was tested for its reliability by using the Cronbach alpha coefficient as presented in Table 1.
The Arabic version of the diabetes distress scale (DDS-17). It included 17 items in four subscales as follows: interpersonal distress (three items), physician distress (four items), regimen distress (five items), and emotional distress (five items) (Polonsky et al., 2005).
Cronbach Alpha Coefficient for Summary of Diabetes Self-Care Activities (SDSCA) and its Subscales.
Scoring System
The subjects were required to answer each question on a scale from 0 to 6 according to the following: (6) a severe problem, (5) a serious problem, (4) a somewhat serious problem, (3) a moderate problem, (2) a slight problem, and (1) not a problem. Thus, higher values indicated more significant distress with a total score of 17–102 points. The sum of the entire score divided into 17 was used to determine the overall mean score. Three groups were created from the data: high distress (mean score of ≥ 3), moderate distress (mean score of 2–2.9), and no distress (mean score of < 2).
Reliability
The Cronbach's alpha value of the Arabic version of the DDS was 0.848 for the total scale. The test–retest reliability value was 0.78 (Batais et al., 2021). Cronbach's alpha value in the current study is presented in Table 2:
Cronbach Alpha Coefficient for Diabetes Distress Scale (DDS) and its Subscales.

Tools Validity
The study tools were submitted to a panel of experts in the fields of medical-surgical nursing and community health nursing in order to assure content validity. Experts were asked to examine the instrument for content, clarity wording, length, format, and overall appearance. Modifications were carried out accordingly.
Data Collection Procedure
Upon receiving formal approval from the research ethics committee from Faculty of Nursing Cairo University, to conduct the study, official permission was obtained before initiation of data collection. Data were collected from June 2022 to January 2023 three times per week. The researchers explained the aim of the current study to the eligible participants who agreed to participate, then distributed the study questionnaires. First, participants were asked to sign in the informed consent, followed by filling in the self-administered questionnaires. If needed, the questionnaire items were read out and explained to the participants by the researchers. This meeting takes about 30–45 min for each participan. The researchers were present with the patients during filling the questionnaire to ensure individualized response.
Data Analysis
SPSS V22 was used in the data analysis. The participants’ socio-demographic characteristics and key research variables were described using descriptive statistics. Additionally, a t-test assured the normality and homogeneity of the variance. The correlations between the different variables were examined using Pearson's correlations. The significance threshold for each two-tailed statistical test was 0.05.
Results
Table 3 shows that 81% of the participants were females in the age group 51–70 years with a mean age of 51.78 ± 11.34, 47% could not read or write, and 86.5% were married, with the highest proportion (77.5%) not working and 68% living in an urban area. Regarding smoking habits, Table 4 demonstrates that 86% of the participants were not smokers. Half of the participants were diagnosed with diabetes 10 years ago or less. Additionally, 20% had no medical history, followed by 17% of the study participants who complained of hypertension, neurological problems, and foot problems.
Frequency and Percentage Distribution of Participants’ Demographics (n = 200).

Frequency and Percentage Distribution of Medical Characteristics among the Participants (n = 200).

Figure 2 illustrates that 80% of the participants practiced lower levels of diabetes self-care. Moreover, Table 5 demonstrates that 81.5%, 77%, 62%, and 33% had poor self-care activity regarding nutrition, follow-up blood-glucose level, practicing exercise, and showing foot care, with a mean of 1.42 ± 1.56, 1.41 ± 2.07, 2.01 ± 2.38, and 2.56 ± 2.05, respectively.

Distribution of the studied participant's diabetes self-care activity (n = 200).
Distribution of Diabetes Self-Care Activity Among the Participants (n = 200).
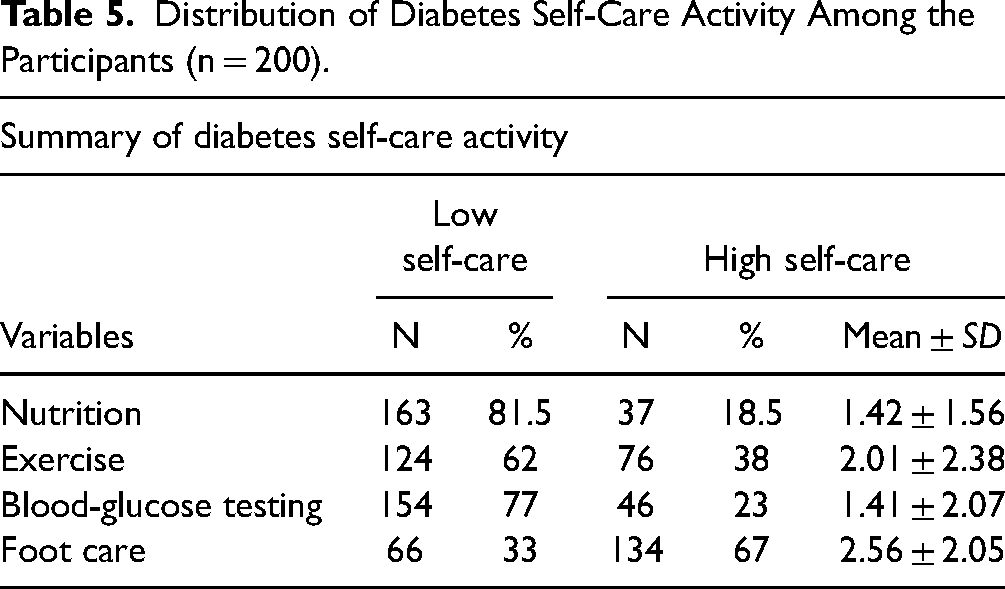
Figure 3 demonstrates that slightly more than one-third of the participants (37%, 36%, and 27%) had high, none, and low levels of diabetes distress, respectively. Besides, Table 6 reveals that 57.5% of the individuals felt a high level of emotional distress, and 54% of them represented a high level of regimen distress. Table 7 shows a correlation between patients with diabetes’ self-care behavior and distress.
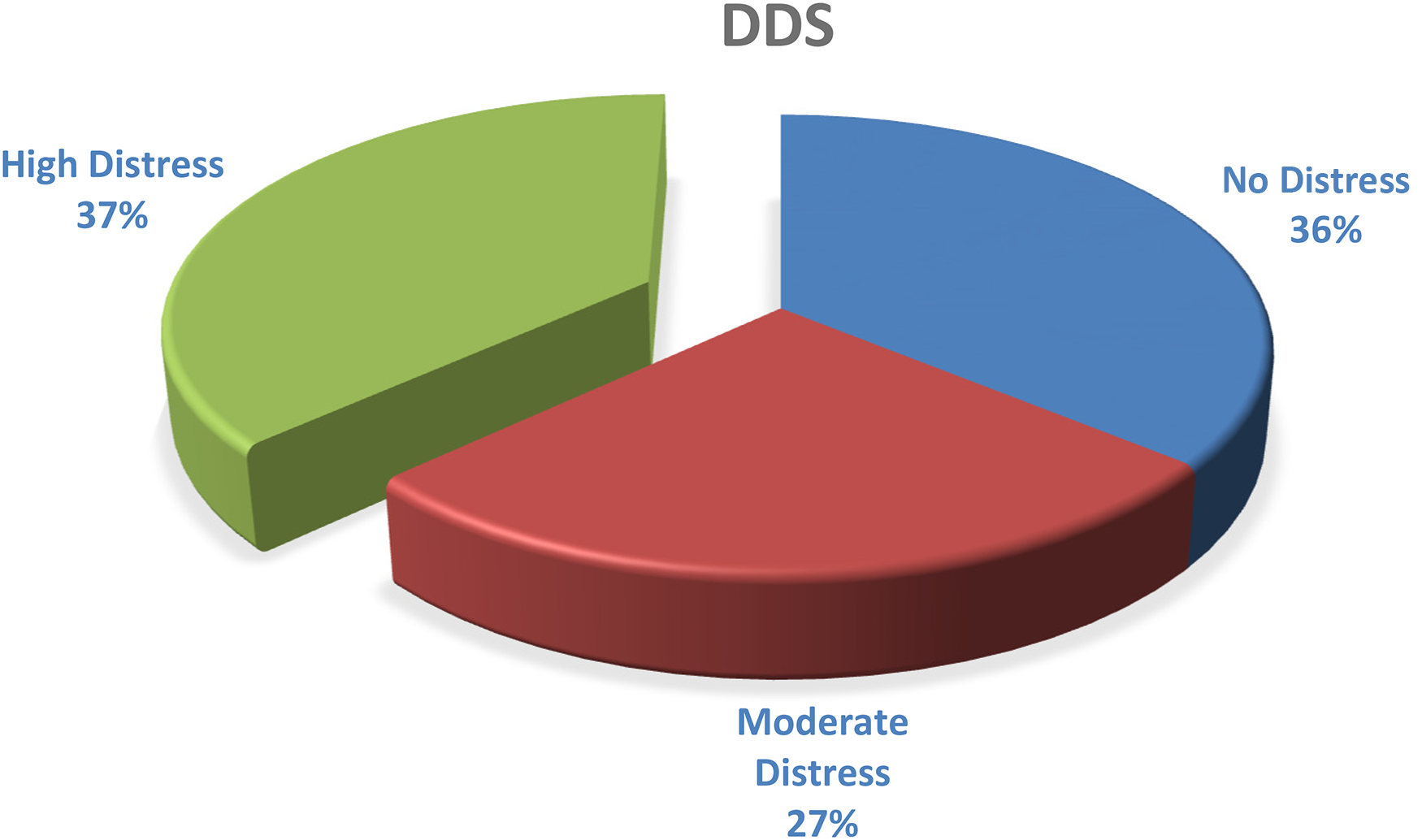
Distribution of the studied participant's diabetes distress (n = 200).
Distribution of Diabetes Distress Score Among the Participants (n = 200).

The Association Between Diabetes Distress Score and Diabetes Self-Care Activity Among the Participants (n = 200).

**Significant at .05 level.
Table 8 shows a significant association between marital status, place of residence, duration of diabetes, and diabetes distress score at r = .314 at a p-value of .000, r = −.328 at a p-value of .000, and r = .289 at a p-value of .000, respectively. In addition, there is a significant relationship among gender, level of education, place of residence, and diabetes self-care activity (r = −.164 at a p-value of .021, r = .288 at a p-value of .001, and r = .359 at a p-value of .000).
The Association Between Diabetes Self-Care Activity, Demographics, Medical Data, and Diabetes Distress Scores Among the Participants (n = 200).
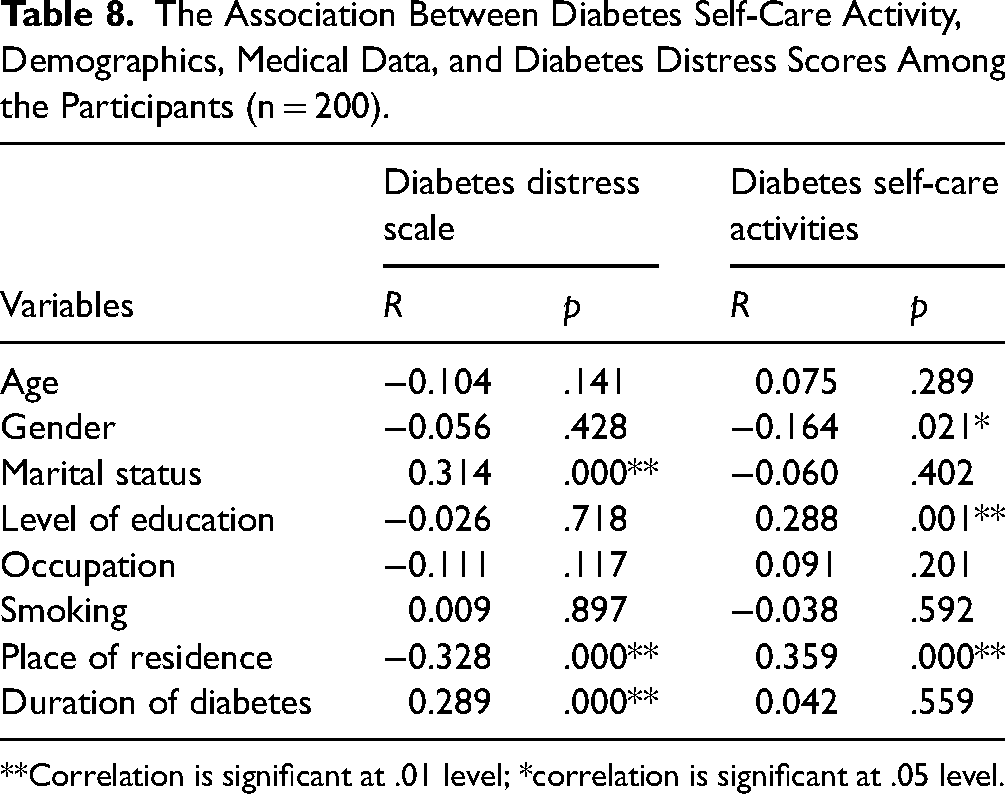
**Correlation is significant at .01 level; *correlation is significant at .05 level.
Section I: Demographic and Medical-Related Data (Tables 3 and 4)
Section II: Diabetes Self-Care Activity and Diabetes Distress Score (Tables 3, 4 and Figures 2, 3)
Discussion
The study results clarified that most participants were homemakers, married, nonsmoking females, aged 51–70, and two-thirds were living in urban areas. These findings are similar to those of a study conducted by Azzam et al. (2021), who conducted a study on factors influencing the glycemic control of Egyptians with diabetes visiting Mansoura district primary care facilities.
These results could be interpreted based on the fact that obesity is the most frequent risk factor among patients with diabetes type II (Klein et al., 2022). Moreover, obesity is common in female patients; therefore, most study participants were female. Furthermore, about half of the participants could not read or write. This result could be related to the fact that most of the attendees at a government hospital are patients with lower education levels and economic status since the services are free) Azzam et al., 2021).
Concerning past medical history, about half of the study participants had diabetes at 10 years old, besides hypertension, neurological, and foot problems. This result is in line with Gabal et al. (2018), Jia and Sowers (2021), and Kassem et al. (2022), who reported that patients with metabolic disorders, including insulin resistance and diabetes, have a high prevalence of hypertension.
The present study's findings clarified that most of the research participants practiced poor levels of diabetes self-care. This result agrees with Molalign et al. (2021), who found that more than half of the participants demonstrated poor diabetes self-care practices. In addition, most of them lacked self-care concerning diabetic nutrition. These findings agree with that of Metwally et al. (2021), who described that more than 75% of the subjects had poorly managed or uncontrolled diabetes.
Intriguingly, about two-thirds of the participants practiced high foot care. This result disagrees with previous research by Hassan (2020), who studied the protection motivation theory applied to diabetic foot care practices in Egypt and showed that the study subjects demonstrated a low level of foot self-care. These results could be explained based on the fact that women have a high level of knowledge about foot care, as reported by Abo-Eata et al. (2022).
Concerning diabetes distress, the outcome of the present study indicated that about a third of participants were suffering from high diabetes distress, with the most affected domains being emotional distress and regimen distress. These findings match the results of Hassan et al. (2022), who studied diabetes distress in a sample of Egyptian diabetic elderly patients. This study demonstrated that one of the elements influencing patients with diabetes’ distress is self-care. This result is inconsistent with previous research by Prihatiningsih and Rahmawati (2021), demonstrating that diabetes distress does not correspond to self-care.
The most important findings in the current study were the significant relationships among marital status, place of residence, duration of diabetes, and diabetes distress. Being married increases the risk of developing diabetes distress. This is consistent with that of Aljuaid et al. (2018) but, inconsistent with Hassan et al. (2022).
In this research, the higher the incidence of developing diabetes distress was in participants with disease duration < 10 years. This result agrees with Kamrul et al. (2022); however, it disagrees with. The shorter the duration of DM, the less the disease management skills and awareness regarding diabetes medications, complications, and a proper diet, resulting in a higher level of distress.
In addition, there is a significant relationship between gender and diabetes self-care activity. This finding is in alignment with Aseeri (2020). The factor that probably contributed to this result is that most of the current study subjects were urban females. The self-care activity is a best practice among urban females rather than males.
Moreover, current research has revealed that self-care directly correlates with education levels. These findings support previous studies by Afaya et al. (2020) and Mahdilouy and Ziaeirad (2021). The plausible factor attributed to this expectation is that higher education levels have better judgment, more awareness among participants regarding complications of diabetes, and better decision-making capability for adhering to diabetes self-care activities.
Study Strengths and Limitations
The study reveals additional information about the association between diabetes distress and diabetes self-care activities, which enriches the understanding of the role of SDSCA among patients with diabetes type II. The study had some limitations, and the interpretation of results should thus be done within the context of our methods. First, the cross-sectional design of the study does not allow for drawing definite conclusions about the causal association between diabetes distress and self-care activities. However, the results of this study provide some evidence for a future intervention study to confirm the causality of the concepts.
Second, self-report measures may be subjective to response bias and the over-estimation of behavior performance. Lastly, the convenience non-probability sampling method may lead to bias in the results of the study, as it may not be representative of all patients. We evaluate the possibility of bias as not substantial as the selected study setting from both inpatient and outpatient clinics serving all Egyptian patients with diabetes from different geographical locations were involved in the study.
Implications for Practice
This study revealed important information about patients with diabetes type II regarding their self-care behaviors and diabetes distress. Nurses play a significant role in providing comprehensive care including health education on the proper diabetes self-care activities for those specific groups of the population. Nursing management for patients with diabetes should focus on improving self-care behaviors, particularly in measuring blood sugar, exercise, and foot care. Educational guidelines regarding diabetes self-care activities should be conducted, discussed, and taught to patients with diabetes using the booklet and illustrated pamphlets for each one to improve their knowledge and practices. The replication of the current study with a larger sample of new mothers in different settings is required for generalizing the results.
Conclusion
In conclusion, the study demonstrated that most participants were females aged 51–70, urban residents, those without formal education, nonsmokers, and homemakers. Furthermore, they demonstrated poor levels of diabetes self-care practice and high levels of emotional distress and regimen distress. In addition, the study found that self-care is correlated with diabetes distress. Moreover, there are significant relationships among marital status, place of residence, duration of diabetes, and diabetes distress score. Additionally, there are significant relationships between diabetes self-care activity, gender, place of residence, and level of education.
Footnotes
Acknowledgments
The authors gratefully acknowledge all diabetic patients from medical wards and outpatient clinics for diabetes at Cairo University Hospitals, Cairo, Egypt who volunteered to participate in the current study. A manuscript submitted to the journal signifies that it has not been published previously, has not been copyrighted, and has not been submitted elsewhere. The authors declare no conflict of interest and all authors have read the final manuscript, have approved the submission to the journal, and have accepted full responsibilities pertaining to the manuscript's delivery and contents and we omitting to pay an Article Processing Charge (APC).
Ethical Considerations
This study was approved by an institutional review board from the Faculty of Nursing at Cairo University (approval # RHDIRB201901701). and conducted in accordance with accepted national and international standards. Moreover, permission to conduct the study was obtained from the administrators of Cairo University Hospitals where the study was conducted. In addition, before the phase of data collection, the researchers obtained written informed consent from each subject who agreed to participate in this study. All subjects were informed about the aim of the study and clearly mentioned that participation in the study is voluntary and that they have the right to withdraw at any time without any negative consequences. Anonymity and confidentiality were assured through coding the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.