
Abstract
Background
Many countries need to accelerate their progress to achieve the sustainable development goal target of neonatal death. It is still high in Ethiopia. Thus, this study aimed to assess the mortality predictors and length of hospital stay among Neonates admitted to the Neonatal Intensive Care Unit of Gurage zone public Hospitals.
Method
In this study, a facility-based retrospective follow-up study was applied among 375 neonates admitted to the NICU of selected public hospitals in the Gurage zone from June 1, 2019 to June 30, 2021. The researchers used Epi-Data entry 3.1 for the data entry and then exported it to STATA version 14 for analysis. The Kaplan–Meier survival curve and log-rank test were used to estimate and compare the survival time of categorical variables, respectively.
Result
The researchers observed about 85 (22.7% with 95%CI: 18.7, 27.2) deaths from the 2305 person-days follow-up. The median survival time was 14 days. The overall incidence density rate was 36.9 per 1000 person-days observed (95%CI: 29.8, 45.6). Perinatal asphyxia (AHR: 2.9[CI: 1.8; 4.8]), cesarean section as a mode of delivery (AHR: 1.1[CI; 1.01; 1.15]), maternal age of greater or equal to 35 years (AHR: 1.1[95% CI: 1.01, 1.15]), and twin pregnancy (AHR: 2.3[95% CI: 1.2, 4.3]) were predictors of neonatal mortality.
Conclusion
The survival rate of neonates was higher compared to other studies. So, to reduce the burden of neonatal mortality, health care providers should give special attention to twin pregnancies, neonates delivered via cesarean section, and neonates with a problem of perinatal asphyxia.
Introduction
More than half (62%) of neonatal deaths occur during the first three days of life (Sankar et al., 2016). A decrement in neonatal death from 39 to 29 was observed between the 2005 and 2016 Ethiopian demographic health survey (EDHS), but it has remained stable since 2016 (EPHIEE, 2019). West and Central Africa and South Asia had the highest neonatal mortality rate (NMR) in 2017. However, most regions reported accelerated progress in reducing neonatal death from 2000 to 2017, and more than 60 countries need to accelerate their progress to achieve the sustainable development goal target of neonatal death by 2030 (Hug et al., 2019). In India, neonatal death decreased from 38 to 23,·five deaths per 1,000 live births (Dandona et al., 2020). The pooled mortality rate of preterm neonates in East Africa is 19.2%, and the odds of mortality among preterm neonates with respiratory distress syndrome and neonates with birth asphyxia were higher (Chanie et al., 2021). The incidence density rate (IDR) of neonatal mortality in Sub-Saharan Africa was high. The IDRs of neonatal mortalities in neonatal intensive care units and the community of these countries were 24.53 and 1.21 per 1000 person-days, respectively. Asphyxia and respiratory distress syndrome were independent predictors of time to neonatal mortality in neonatal intensive care units (Bitew et al., 2020). There is a wide variation in neonatal mortality in sub-Saharan Africa, ranging from 8 to 50 per 1000 live births and an average of 30.1 deaths per 1000 live births (Kayode et al., 2017). Despite the potential factors that could influence the survival status of newborns, these factors are not well known in the study area. Thus, this study aimed to assess the mortality predictors and length of hospital stay among neonates admitted to the Neonatal Intensive Care Unit of Gurage zone public Hospitals. The finding of this study will help the researchers to uncover the various domains of factors by doing further based on the outcomes identified in this study and improve the survival status of neonates by acting on the modifiable factors.
Literature Review
The Magnitude of Neonatal Mortality
A hospital-based prospective and retrospective study in India revealed an overall NMR of 10.4% (Ravikumar et al., 2018). In Africa, the NMR was 22% in rural Ugandans (Hedstrom et al., 2014) s(9) and 14.2% in Nigeria Enugu State University Teaching Hospital (Ekwochi et al., 2014). A study done in Mauritania revealed that 34.7% of neonates died, and among those deaths, 71.3% were during the first six days of life (Weddih et al., 2019).
A decrement in neonatal death from 39 to 29 was observed between the 2005 and 2016 EDHS but has remained stable since 2016 (7). A study conducted in the Neonatal Intensive Care Unit (NICU) at Arba Minch General Hospital discovered that the IDR of neonatal mortality was 31.6/1,000 neonate days. The first day of survival probability was 96.1%. The study also showed that survival probability on the 7th day, 14th day, and 21st day was 75%, 69.9%, and 66.2%, respectively, with an overall median survival time of six days (Dessu et al., 2018). A study at Jimma University Medical center showed that the incidence of nonatal mortality was 30 deaths per 1,000 institutional live births (10) and 27 per 1000 neonates-day (Orsido et al., 2019). A study done at the University of Gondar Comprehensive Specialized Hospital revealed that 14% of neonatal death was in the first 24 hours, 60% in the first three days, and almost 84% in the first week of life. Also, the failure probability was 13.79%, 59.77%, 83.91%, and 97.70% in the 1st day, 3rd day, 7th day, and 14th day of hospital stay on the incidence rate of 23.81, 33.92, 31.48, and 28.90 deaths per 1000 neonate-days observation, respectively (Gudayu et al., 2020). Another study in Mekelle general and Ayder comprehensive specialized hospitals revealed the neonatal mortality incidence of 126.5 per 1000 live births (Kahsay et al., 2019). Similarly, studies done in the NICU of Arba Minch General Hospital and Debre Markos Referral Hospital discovered 20.8% and 21.3% deaths, respectively (Alebel et al., 2020; Dessu et al., 2018). The failure probability on the 1st day, 3rd day, and 7th day of hospital stay was 19.4%, 58.2%, and 91%, respectively, and there was no failure after 16 days (Dessu et al., 2018).
Predictors of Mortality in Neonates
Socio-demographic Factors
A study in the Democratic Republic of Congo revealed that neonates born to mothers aged <18 and more than 35 years had a high risk of death (Mashako et al., 2019). A meta-analysis study showed that nulliparous age <18 years (AOR: 2.07) (Kozuki et al., 2013). In Ethiopia, newborns from mothers less than or equal to18 years old account for most neonatal deaths compared to babies born from mothers aged 35 years or above (AHR: 12.6) (Dessu et al., 2018). A study showed that neonates born to mothers of advanced age were at a higher risk of death (AHR = 2.60) (Mengistu et al., 2020). In another study, the risk of death in preterm (before 34) was 4.5% higher than in babies born after 34 weeks, and the risk becomes higher at 32 weeks (10.17 times) (p < .0001) (Ravikumar et al., 2018). In another study, the deaths of preterm babies were higher (24.5%) than the deaths of term babies (7.1%) (Sabzehei et al., 2018).
Obstetrics Factors
A study in Northwestern rural China on predictors of neonatal death revealed that neonatal death was higher among multiparous women (OR = 2.77) (Li et al., 2015). In Sub-Saharan Africa, multiple births (twins or triplets or more) were independent predictors of time to neonatal death (Bitew et al., 2020). In Ethiopia, multiple pregnancies increase neonatal death risk (Mengistu et al., 2020; Orsido et al., 2019). NMR was also greater among mothers who did not receive antenatal care throughout the first trimester of pregnancy (OR = 2.49) (Li et al., 2015). A study done in Afar Region Public Hospitals found high neonatal mortality among those delivered by cesarean section (Woday Tadesse et al., 2021). In Southern Ethiopia, the cesarean section had a 66% protective effect on neonatal death compared with SVD (Orsido et al., 2019).
Neonatal Medical Conditions
Studies in India and Bangladesh also revealed that rspiratory distress (33.6%) (24), prinatal asphaxia (25.3% and 24.3%), and sepsis (25.3% and 21.9%) were predictors of neonatal death, respectively (Ravikumar et al., 2018; Shahidullah et al., 2017). A study at Arba Minch General Hospital revealed that five-minute APGAR scores ≤5 had a higher risk of neonatal death (Dessu et al., 2018). Thus, this study aimed to assess the mortality predictors and length of hospital stay among Neonates admitted to the Neonatal Intensive Care Unit of Gurage zone public Hospitals.
Methods
Study Design and Setting
In this study, a retrospective cohort study was applied to assess the survival status and predictors of death among neonates admitted to the Neonatal Intensive Care Unit of Gurage zone public Hospitals. The researchers calculated follow-up time for each patient from the date of admission to the file closure (due to death, transfer out, default, and the last date of discharge). The study was conducted in the Gurage zone from June 1, 2019 to June 30, 2021.
Study Participants and Eligibility
All neonates admitted to the NICU in the selected hospitals of the Gurage zone were the source populations. All neonates aged 28 days and less admitted to the NICU in the selected hospitals of the Gurage Zone from June 1, 2019 to June 30, 2021 were included in this study. All patients with incomplete baseline information (at least the infant's socio-demographics, admission date, and exit date from the cohort) were excluded.
Sample Size and Sampling Procedure
The sample size was determined using double population proportion from factors in different studies using Epi info version 7 by considering a 95% confidence interval, power of 80%. The total sample size for this study was 397, considering the presence of perinatal asphyxia as an explanatory variable for neonatal death in previous literature (Orsido et al., 2019).
Sampling Technique and Procedure
Simple random sampling technique was applied to select hospitals. The researchers constructed a sampling frame at the selected hospitals. The participants who fulfilled the inclusion criteria were selected using excel (computer-generated random sample). The study subjects were allocated to each health facility based on the proportion of the number of medical records of the neonates (Figure 1).

Schematic presentation of sampling technique to assess the mortality predictors and length of hospital stay among neonates admitted to the Neonatal Intensive Care Unit of Gurage zone public Hospitals.
Data Collection Tools and Procedures
In the checklist of socio-demographic characteristics, we included the maternal-related and neonatal-related information. Data were extracted through chart review using a structured tool. Before the actual data collection, we orient the data collectors and the supervisor on the objectives and contents of the checklist. Four trained nurses as data collectors and one MSc nurse as a supervisor reviewed all medical records of neonates that fulfilled the inclusion criteria.
Data Quality Assurance
The data quality was assured by designing proper data abstraction tools. After the evaluation by experienced researchers, we conducted a pretest on 5% of the sample size. Training regarding the data abstraction checklist and data collection process for both data collectors and supervisors was given. Close supervision and monitoring during data collection was carried out.
Data Processing and Analysis
All filled checklists were entered into Epi-Data 3.1 and checked for completeness and consistency before being exported to STATA version 14. The data were processed by STATA version 14 to estimate the survival time of neonates. We calculated the incidence of death concerning person-time at risk.
Cox proportional hazard model assumptions were checked using log–log, Kaplan–Meier versus predicted survival plot and ran a global test using the Schoenfeld residual test. Bivariate Cox proportional hazards (PH) model was employed, and we considered variables with a p-value <.2 in the bivariate analysis as a candidate for the multi-variable Cox-PH regression model. Variables with a p-value ≤.05 level in the multivariate analysis were considered significant predictors of neonatal mortality in the final Cox regression analysis.
Results
Socio-demographic Characteristics of Mothers of Neonates
Among 397 neonatal charts reviewed, 375 (94.5%) records met the criteria and have undergone the final analysis. The majority were 247(65.9%) were male, and the majority (71.2%) of the neonates were from rural areas (Table 1).
Socio-demographic Characteristics of Mother at Gunchire Primary Hospital and Wolkite University Specialized Hospital, Gurage Zone, South Ethiopia, August 2021 (n = 375).

Maternal Obstetrics History
More than half of the mothers (201[53.6%]) were multiparous. About 239 (63.7%) of the neonate's mothers attend antenatal care follow-up. Two third of neonates (251 [66.9%]) were born in the hospital (Table 2).
Obstetrics History of the Mothers of Neonates at Gunchire Primary Hospital and Wolkite University Specialized Hospital, Gurage Zone, South Ethiopia, August 2021(n = 375).

Neonatal-Related Characteristics
Among the neonates included in the study, 85(22.7%) of them died (Table 3).
Neonatal-Related Characteristics of Gunchire Primary Hospital and Wolkite University Specialized Hospital, Gurage Zone, South Ethiopia, August 2021(n = 375).

Length of Hospital Stay for Neonates Admitted to NICU
The neonates were followed for a minimum of one day and a maximum of 20 days of hospital stay. The mean and median length of hospital stay for the neonates was six days (Figure 2).
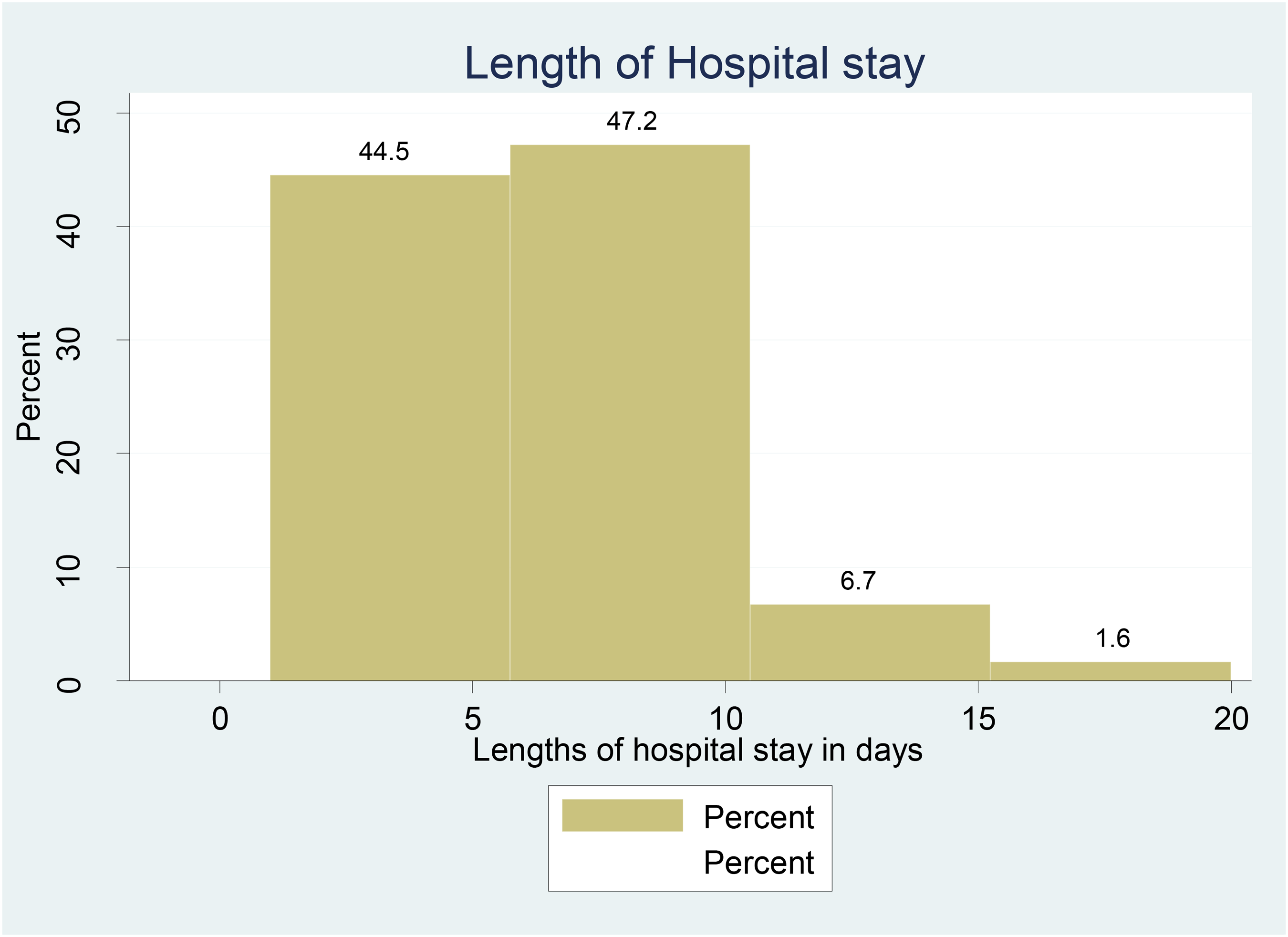
Length of hospitals of neonates admitted to the Neonatal Intensive Care Unit at Gurage zone public hospitals, 2021.
Incidence of Death Among Neonates
Three hundred and seventy-five neonates admitted to NICU were followed and given 2305 person-days observation. Eighty-five infants (22.7%) passed away throughout the observation period. We calculated the death incidence rate using person-days of follow-up. The overall IDR was 36.9 per 1,000 person-days observation (95%CI: 29.8, 45.6). After the first day, third day, and seventh day of admission, the cumulative probability of survival was, respectively, 0.984, 0.93.7, and 0.824% (Figure 3).
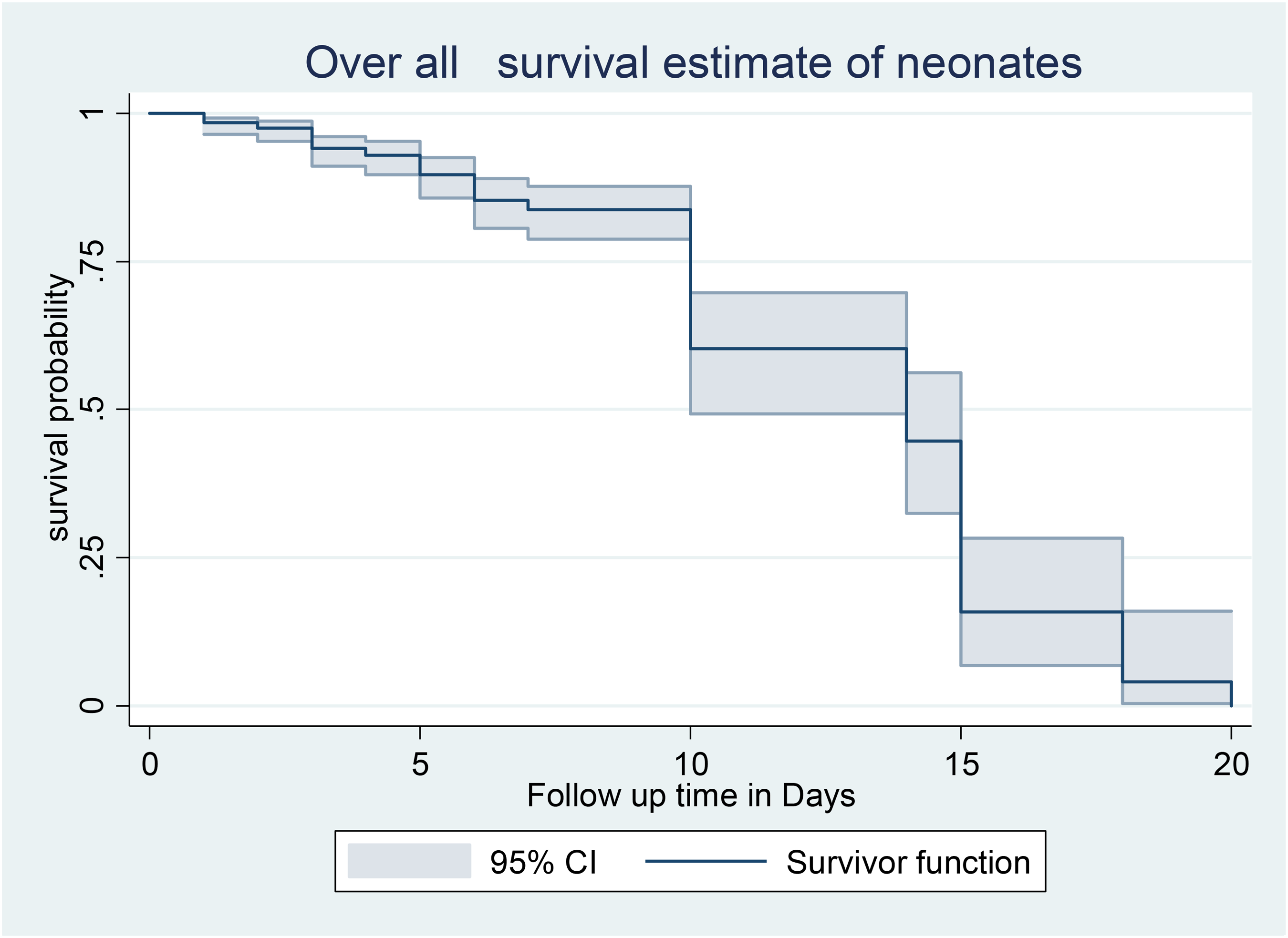
Overall Kaplan–Meier survival curve with 95% confidence intervals of neonates admitted to the Neonatal Intensive Care Unit at Gurage zone public hospitals, 2021.
Predictors of Neonatal Mortality
The Cox-PH adjusted model allowed us to isolate four significant factors (Table 4). The hazard of mortality in neonates with perinatal asphyxia was 2.91 times higher as compared to their counterparts (AHR: 2.9; [CI: 1.8; 4.8]). The hazard of mortality in neonates delivered via cesarean section was 1.08 times higher as compared to those delivered via spontaneous vaginal delivery (AHR: 1.1; [CI; 1.01;1.15]). The hazard of neonatal mortality was 1.08 times higher among neonates with maternal age of greater or equal to 35 years as compared to those with maternal age of <35 years (AHR: 1.1; [95% CI: 1.01, 1.15]). The hazard of neonatal mortality was 2.3 times higher among twins compared to singleton neonates (AHR: 2.3; [95% CI: 1.2, 4.3]).
Bivariable and Multi-variable Cox Regression Among Neonates Attending NICU of Gunchire Primary Hospital and Wolkite University Specialized Hospital, Gurage Zone, South Ethiopia, August 2021 (n = 375).

Note. CHR = crude hazard ratio; AHR = adjusted hazard ratio; CI = confidence interval; NICU = neonatal intensive care unit.
* Significant (p-value <.05).
Discussion
The cumulative incidence of death was 22.7% (95%CI: 18.7, 27.2). The cumulative incidence finding was consistent with the study conducted in Debre Markos Referral Hospital (21.3%) (13), Hosana, which was 25 deaths per 1000 neonate days (Moges et al., 2021). This finding is lower than the study findings from Mekelle, Ethiopia (Kahsay et al., 2019). This difference may be due to the difference in the study design.
This study indicated that the overall incidence of death was 36.9 (95%CI: 29.8, 45.6) per 1000 neonate-days observations. This finding is lower than the studies conducted in Mizan Tepi, Ethiopia (62.15 deaths per 1000 neonate-day observations (Bereka et al., 2021). The possible reason may be the difference in the study population (they consider only Preterm Neonates). But, it is higher than the studies conducted in the Wolaita zone, Ethiopia, which was 20.8 per 1000 neonate days (Berhanu et al., 2021), Debre Markos, Ethiopia (25.8 deaths per 1000 neonate days) (Alebel et al., 2020), and Hosanna, Ethiopia (18.8%) (Moges et al., 2021).
After the first day and seventh day of admission, the cumulative survival probability was 85.3% (80.7, 88.9) and 70.5% (62.9, 76.8), respectively. The seventh-day survival probability was consistent with a study conducted in Arba Minch, Southern Ethiopia (75%) (Dessu et al., 2018). But, the first-day survival probability was lower than the finding from Arba Minch, Ethiopia (Dessu et al., 2018). The median survival time of the neonates was 14 days. It is consistent with the findings from Mizan Tepi University Teaching Hospital, South West Ethiopia, and 15 days (8).
In this study, the hazard of death was higher among neonates who delivered via cesarian section than those delivered via spontaneous vaginal delivery. The supporting evidence for this is from Kenya and Tanzania (Ochieng Arunda et al., 2020) and Africa (Bishop et al., 2019). The possible pathologic cause may be the hypothesis that cesarean delivery could result in the prolonged immunologic immaturity linked to the less native intestinal flora, which may increase the risk of infections and other diseases, as well as neonatal respiratory problems like birth asphyxia and neonatal respiratory distress syndrome (Bager, 2011; Liston et al., 2008). But, cesarean delivery was protective in other studies in Wolaita zone, Southern Ethiopia (decreased the risk of neonatal death by 91.6%) (Berhanu et al., 2021), and Mizan Tepi, South West Ethiopia, in which vaginal mode of delivery increased the risk of preterm (Bereka et al., 2021).
The hazard of neonatal death from mothers with age ≥35 years was higher compared to mothers aged 20–34 years. But, a study from rural Tanzania reveals neonatal deaths from young mothers (aged 13–19 years) were higher compared to age 20–34 years (Selemani et al., 2014). The possible pathophysiologic explanation may be due to older mothers’ susceptibility to deterioration of most physiological functions, such as inadequate uteroplacental circulation and placental hypo perfusion caused by the aging uterus and vasculature, which may lead to fetal growth restriction (Cohen, 2014). Evidence from 45 low and middle-income countries suggests the importance of reducing adolescent births among the youngest age group as a strategy for addressing the problems of neonatal mortality (Neal et al., 2018). But, none of the maternal-related conditions were significantly associated with neonatal mortality in Asmara, Eretria (Andegiorgish et al., 2020).
The hazard of neonatal mortality among twins was higher. This may be because twin pregnancies born moderately and late preterm encounter higher rates of neonatal morbidities (Refuerzo et al., 2010). Twin pregnancies are more likely to be affected by fetal growth restriction and preterm birth (24). Sixty low- and middle-income countries provide evidence for this (Bellizzi et al., 2018); Gambia (Miyahara et al., 2016) and sub-Saharan Africa twins account for an increasing share of neonatal death (15.1%) (Monden & Smits, 2017). It may be due to increased rates of obstetric and perinatal complications and several innate characteristics such as premature separation of the placenta (Glinianaia et al., 2011). In addition, multiple-born neonates are at increased risk of prematurity and low birth weight, which may make them susceptible to infection. The hazard of mortality was higher among neonates with perinatal asphyxia. There is much supporting evidence for this in southeast Nigeria (Uleanya et al., 2019) and Hosanna, Ethiopia (Moges et al., 2021; Townsend & Khalil, 2018). The possible scientific justification could be that asphyxia contributes to the deprivation of oxygen in the body, leading to hypoxia, hypercarbia, and acidosis formation, which may damage vital organs leading to death.
Limitations of the Study
Since the data were collected from medical records, socioeconomic factors were not possible to obtain for the whole cohort, as they might be associated with mortality; therefore, these variables in analyses were not included. So, the researchers recommend that future researchers incorporate these variables by applying the prospective study design.
Conclusion and Recommendation
The survival rate of neonates was higher compared to other studies. The risk of death increased if the neonates were from mothers aged ≥35, with perinatal asphyxia, were twins, and with cesarean section as the mode of delivery. To reduce the burden of neonatal death, health care providers should give special attention to twin pregnancies and neonates delivered via cesarean section neonate with a problem of perinatal asphyxia.
Footnotes
Acknowledgment
We would like to thank Wolkite University, Department of Nursing for facilitation. Our gratitude goes to supervisors, the data collectors, and the staff of Wolkite University specialized hospital and Gunchire primary hospital for their cordial collaboration.
Author’ Contributions
B.C. prepared the proposal, provided training for data collectors, supervised data collection, analyzed and interpreted the data, and wrote the main manuscript; T.F. prepared the proposal and reviewed the manuscript; B.T., F.A., A.K., and B.G. reviewed the manuscript; S.G. supervised and evaluated the overall research process and reviewed the whole manuscript; H.A., S.T., A.A., Y.M., B.T.,, M.A., and F.T. reviewed the manuscript.
Availability of Materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request and will be attached to the editorial office when requested.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Research, Ethical Clearance Committee of Wolkite University with a protocol number of 019/2021. Following the approval, the official letter was obtained from the College of Medicine and Health Sciences of Wolkite University and given to the hospital managers, medical directors, and neonatal intensive unit coordinators. Permission was obtained from the hospital's administration before data collection.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was not sought from the legally authorized representatives of the patients directly since we used a medical record.