
Abstract
Introduction
Globally, neonatal mortality remains a significant challenge, with Sub-Saharan Africa bearing the highest burden. Ethiopia ranks among countries with the highest neonatal mortality rates, but limited data exist on timing and predictors of neonatal deaths in the study setting.
Objective(s)
To assess neonatal survival and identify predictors of mortality among neonates admitted to the neonatal intensive care unit (NICU).
Methods
A prospective cohort study was conducted on 504 neonates admitted to NICU. Adjusted hazard ratios (AHRs) with 95% confidence intervals (CIs) were calculated to evaluate associations between potential predictors and mortality.
Results
At study end, 23.6% (95% CI: 19.8, 27.4) of neonates died, with a mortality rate of 35.5 per 1,000 neonate-days. Neonatal survival declined from 90% on day 1 to 66% by day 28. Significant predictors of mortality included lack of antenatal care (ANC) (AHR = 3.09), failure to cry immediately at birth (AHR = 2.61), respiratory distress syndrome (AHR = 6.96), and meconium aspiration syndrome (AHR = 9.16).
Conclusion
Neonatal mortality remains high in the study setting. Strengthening maternal and neonatal care, especially ANC and institutional delivery, is vital to improve neonatal survival.
Introduction
Globally, approximately 2.3 million newborns died within the first 28 days of life in 2022, representing nearly half of all under-5 child deaths (World Health Organization, 2024). While substantial progress has been made since 1990, neonatal mortality rates remain disproportionately high in sub-Saharan Africa and South Asia, with rates of 27 and 21 deaths per 1,000 live births, respectively, compared to much lower rates in high-income regions (Mohamed et al., 2022; World Health Organization, 2024). Ethiopia's neonatal mortality rate remains above the Sustainable Development Goal target, with recent estimates around 23 deaths per 1,000 live births, highlighting ongoing challenges specific to the country (Kebede, 2025). The Sustainable Development Goals aim to reduce neonatal mortality to at least 12 per 1,000 live births by 2030 (Tolossa et al., 2022). Ethiopia's neonatal mortality rate decreased from 39 per 1,000 live births in 2005 to 29 per 1,000 in 2016 but increased to 33 per 1,000 in 2019 (Tekeba, Tamir et al., 2024).
Review of Literature
Major causes of neonatal mortality include preterm birth, perinatal asphyxia, infections, and congenital abnormalities. Contributing factors encompass poor maternal health, inadequate obstetric and neonatal care, and societal factors such as women's status, nutritional status, and traditional practices (Mengesha et al., 2016; Tolossa et al., 2022; Wondwossen et al., 2015; World Health Organization, 2017). Understanding the predictors and survival patterns of neonates in Ethiopia is critical to inform targeted interventions and accelerate progress toward national and global neonatal health goals (Kebede, 2025).
While Ethiopia has achieved notable reductions in neonatal mortality over the past decades, rates remain high due to multiple persistent challenges. System-level barriers such as inadequate health facility readiness, poor infrastructure including difficult geographic access and transportation, and shortages of skilled health personnel significantly limit effective neonatal care. Socio-economic inequities and cultural factors further hinder equitable access to timely, evidence-based interventions. Additionally, gaps in the implementation and utilization of proven maternal and neonatal health services, including antenatal care (ANC), skilled birth attendance, and postnatal follow-up, continue to impede progress. Addressing these multifaceted barriers is crucial to reduce neonatal deaths and achieve national and global health targets (Ethiopia Ministry of Health Fact Sheets, 2024; Kebede, 2025; Tebeje et al., 2025).
In Ethiopia, few studies have comprehensively examined neonatal mortality and its predictors. Existing research has largely been retrospective, omitting critical predictors and focusing only on survival status during neonatal intensive care unit (NICU) admission without follow-up post-discharge (Dessu et al., 2019; Enawgaw et al., 2025; Mengesha et al., 2016). To generate robust evidence for reducing neonatal mortality in Ethiopia, prospective studies with extended follow-up are essential. Addressing this knowledge gap, this study aimed to assess the survival status and identify predictors of neonatal mortality among neonates admitted to the NICU.
Methods and Materials
Study Design, Setting, and Period
A facility-based prospective cohort study was conducted from November 25, 2022, to February 25, 2023, at the NICU. The hospital has 15 departments and thirty units, with the NICU providing care to approximately 24,000 neonates annually. The NICU is equipped with essential supportive technologies including radiant warmers, continuous positive airway pressure (CPAP) machines, phototherapy units, and oxygen concentrators. Skilled staff, including pediatricians, neonatologists, and trained nurses, provide round-the-clock neonatal care in this facility.
Variables of the Study
Dependent variable: Neonatal mortality during the 28-day follow-up period.
Independent variables: Maternal sociodemographic factors (age, residence, marital status, education, ethnicity, religion, employment), maternal obstetric and medical factors (ANC, gestational age, pregnancy type, parity, birth interval, labor onset and duration, maternal medical diseases, obstetric complications), service delivery characteristics (mode and place of delivery, delivery attendant, iron-folic acid supplementation, postnatal care), and neonatal factors (sex, age at admission, birth weight, temperature, breastfeeding initiation, crying immediately after birth, respiratory distress syndrome (RDS), sepsis, perinatal asphyxia, meconium aspiration syndrome (MAS), congenital abnormalities, jaundice, resuscitation with bag and mask, CPAP intervention).
Sample Size Determination and Sampling Procedure
The sample size (n = 504) was calculated using Epi Info version 7 based on the cohort formula, with assumptions of 95% confidence interval (CI), 80% power, and a 1:1 ratio of exposed to non-exposed groups while considering different significant variables from previous studies (Berhanu et al., 2021; Eshete et al., 2021; Limaso et al., 2020). Predictor variables considered included fifth-minute APGAR score, birth weight, breastfeeding initiation time, and neonatal complications. Birth weight was identified as the primary predictor (Gebremariam et al., 2021; Park et al., 2018), yielding the largest sample size estimate of 480. An additional 5% was added to account for non-response and loss to follow-up, resulting in a final sample size of 504. Consecutive sampling was used to enroll eligible neonates until the sample size was reached.
Source and Study Population
The source population comprised all neonates admitted to the NICU during the study period. The study included neonates admitted between November 25, 2022, and February 25, 2023, whose mothers or caregivers were available to provide data during collection.
Data Collection Tools, Procedures, and Follow-Up
Data collection tools were adapted from the World Health Organization (WHO) standard verbal autopsy questionnaire (Mosley & Chen, 2003) and relevant literature, with modifications to fit the local context (Alebel et al., 2020; Eshete et al., 2021; Limaso et al., 2020). The questionnaire was initially prepared in English and translated into Afan Oromo and Amharic to ensure comprehensibility and consistency. Data were collected prospectively by five trained Bachelor of Science health professionals (two nurses, two midwives, and one supervisor) through interviews with mothers or caregivers and clinical assessments of neonates. Information collected included sociodemographic characteristics, maternal and neonatal clinical data, and service delivery factors. During hospitalization, neonates were followed daily in the NICU. Post-discharge follow-up was conducted via daily telephone calls to mothers and weekly home visits by health extension workers until the end of the neonatal period (28 days). Neonatal outcomes, including survival status and dates of any events (death or censoring), were recorded based on WHO verbal autopsy guidelines (Mosley & Chen, 2003). Cases where mothers or caregivers could not be reached despite home visits were recorded as lost to follow-up.
Data Quality Control
A pre-test was conducted on 5% of the sample at similar but another setting to assess the clarity and relevance of the questionnaire. Based on the pre-test results, some variables were amended for clarity, completeness, and contextual relevance. These amendments included refining definitions of key clinical predictors, improving the wording and sequence of questionnaire items to reduce ambiguity. Data collectors and supervisors received training on study protocols and data collection methods prior to fieldwork. The principal investigator and supervisor reviewed all completed questionnaires daily for completeness and accuracy, providing feedback as needed.
Regarding data cleaning, the researchers conducted a comprehensive process including range and consistency checks, identification and management of outliers, duplicate record detection, and correction of typographical and logical errors. Missing data were assessed and handled to minimize bias. Regarding subjects lost to follow-up in the survival analysis, these neonates were treated as censored observations at their last known follow-up time. Double data entry was performed to minimize entry errors prior to analysis.
Statistical Assumptions and Analysis
Multicollinearity among predictor variables was assessed using the variance inflation factor; values exceeding 10 indicated multicollinearity. Due to multicollinearity between attendant of delivery and postnatal care, attendant of delivery was excluded from the multivariable analysis. The proportional hazards assumption was checked graphically using log-minus-log survival plots for categorical variables; no violations were found, validating the use of the Cox proportional hazards model.
Data Processing and Analysis
Data were entered into EpiData version 3.1 and exported to SPSS version 20 for analysis. Descriptive statistics were calculated, including frequencies, percentages, means, medians, and standard deviations. Survival time was estimated using Kaplan–Meier (Kaplan & Meier, 1958; Shreffler & Huecker, 2020) survival curves, with comparisons performed via the log-rank test. Bivariable Cox proportional hazards regression was conducted to identify candidate predictors (p < 0.20) for multivariable analysis. Multivariable Cox regression models were used to estimate adjusted hazard ratios (AHRs) and 95% CIs for variables associated with neonatal mortality, with statistical significance set at p < 0.05.
Operational Definitions
Censored: Neonates who did not experience death during the follow-up period (including those who recovered, self-discharged, lost to follow-up, transferred, or still admitted beyond 28 days) (Mengistu et al., 2020). Event: Confirmed neonatal death during the follow-up period (Alebel et al., 2020). Survival status: The recorded outcome of each neonate (death or censored) at the end of follow-up. It was coded as a binary event indicator, where 1 represented death of the neonate and 0 represented censoring. Survival time: Duration in days from NICU admission until death or censoring (Tolossa et al., 2022).
Results
Maternal Sociodemographic Characteristics
A total of 504 neonates and their mothers participated in the study. The mean maternal age was 26.3 ± 5.3 years, with 48.4% aged under 25 years. Most mothers (75.2%) resided in urban areas. The Oromo ethnic group constituted 71.2% of participants. Housewives accounted for 73.2%, and 26.4% of mothers had completed secondary education (Table 1).
Maternal Sociodemographic Characteristics of Neonates Admitted to NICU from November 2022 to February 2023.

Indicates Sulte, Tigre, Gurage and Walaita; bIndicates Wakefata.
Maternal Obstetric and Medical Characteristics
Nearly all (97.2%) mothers attended at least one ANC visit, with 67.5% completing four or more visits. Two-thirds (66.9%) of mothers had one child, and 87.9% had singleton pregnancies. Medical conditions were present in 14.7% of mothers, with anemia affecting 9.3%. Obstetric complications during the current pregnancy were reported by 27.4% of mothers (Table 2).
Maternal Obstetric and Medical-Related Characteristics of Neonates Admitted to NICU from November 2022 to February 2023.

Indicates hepatitis, human immunodeficiency virus, heart failure, gastritis, bIndicates oligohydramnios, polyhydramnios.
APH = Antepartum hemorrhage; DM = Diabetes-mellitus; PROM = Prolonged rupture of membrane; ANC=antenatal care.
Service Delivery-Related Characteristics
Most mothers (80.6%) received iron-folic acid supplementation during pregnancy. Deliveries occurred predominantly in health facilities (94%), including hospitals (67.9%) and health centers (16.3%), while 6% occurred at home. Spontaneous vaginal delivery accounted for 54.8% of births. Postnatal care utilization was high at 94.4% (Table 3).
Service Delivery-Related Characteristics of Neonates Admitted to NICU from November 2022 to February 2023.
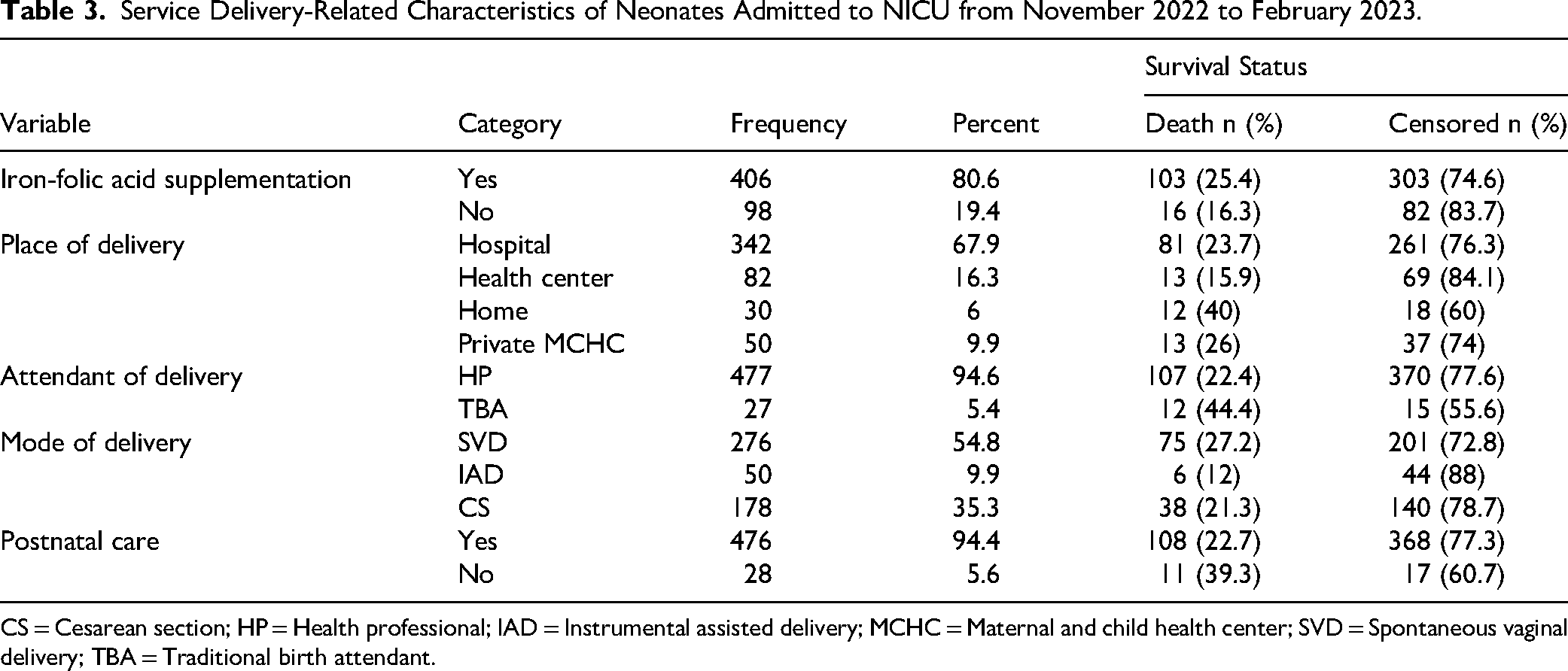
CS = Cesarean section; HP = Health professional; IAD = Instrumental assisted delivery; MCHC = Maternal and child health center; SVD = Spontaneous vaginal delivery; TBA = Traditional birth attendant.
Neonatal Characteristics
Among neonates admitted to the NICU, 60.1% were male. Most (70.8%) were admitted within 24 h of birth. Approximately 30.2% did not cry immediately after birth, and 70.8% did not initiate breastfeeding within the first hour. Normal birth weight (2,500–4,000 g) was observed in 54%, and a normal admission temperature (36.5–37.5 °C) in 31.3%. One-fourth (25.8%) of neonates were admitted with sepsis. Resuscitation with bag and mask and CPAP intervention were provided to 10.3% and 20% of neonates, respectively (Table 4).
Neonatal Characteristics of Neonates Admitted to NICU from November 2022 to February 2023.

CPAP = Continuous positive airway pressure; MAS = Meconium aspiration syndrome.
Neonatal Survival Status
During the 28-day follow-up, 119 neonates (23.6%; 95% CI: 19.8, 27.4) died, resulting in a mortality rate of 35.5 deaths per 1,000 neonate-days based on 3,349 neonate-days of observation. Notably, 41% of deaths occurred within the first 24 h, and 90% within the first seven days. Among the 385 censored neonates, the majority recovered, with smaller proportions self-discharging, remaining under follow-up, transferring to other facilities, or lost to follow-up (Figure 1).
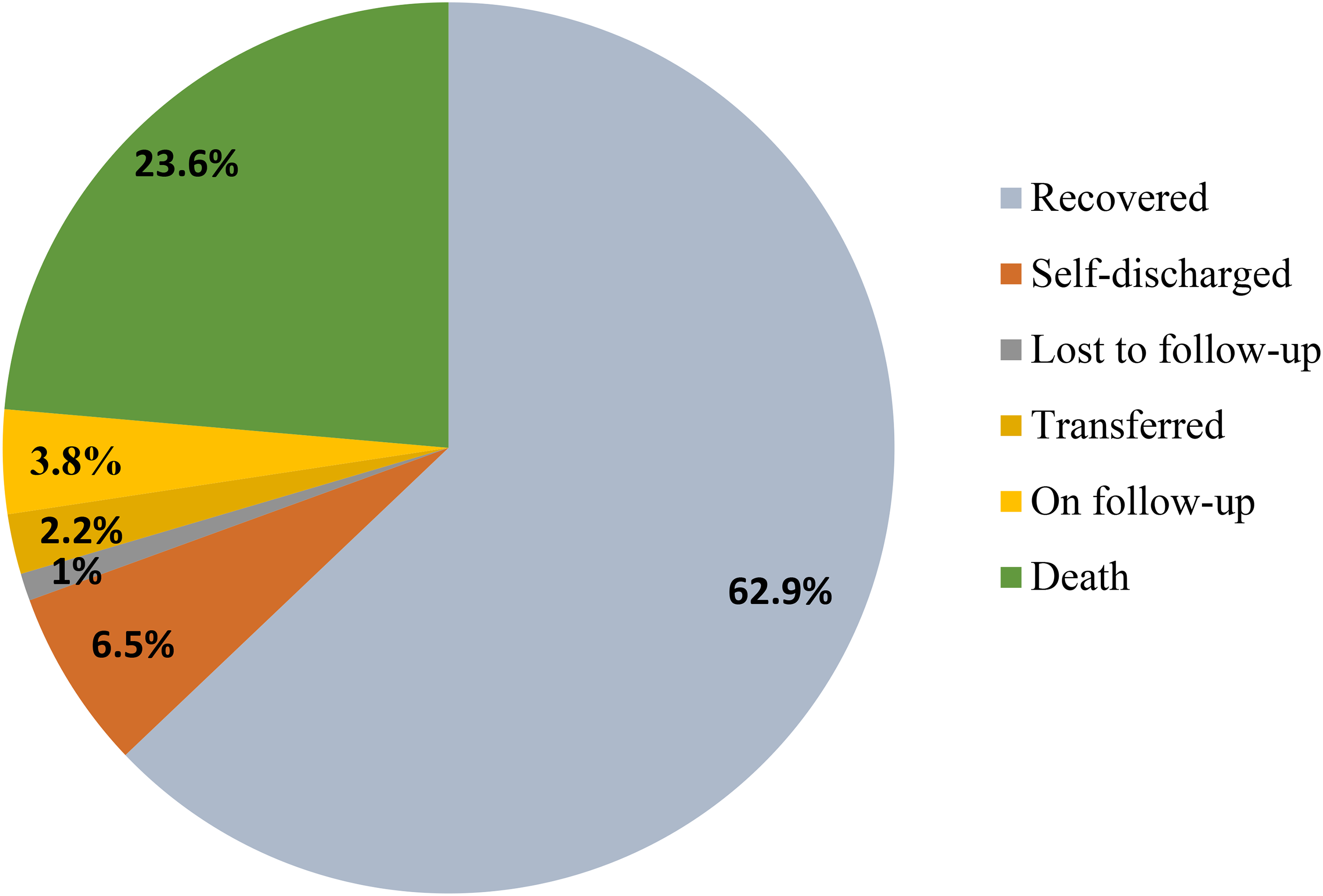
Outcomes of neonates admitted to NICU from November 2022 to February 2023. NICU=neonatal intensive care unit
Kaplan–Meier Survival Analysis
The Kaplan–Meier survival estimates indicated cumulative survival probabilities of 90.1%, 75.3%, 67.5%, and 66.1% at days 1, 7, 14, and 28, respectively. The overall mean survival time was 20 days (95% CI: 18.9–21.5). The Kaplan–Meier survival estimate represents the probability of survival accounting for censoring and time-at-risk, while crude mortality is a simple observed proportion. Both metrics provide complementary insights but should be interpreted in the context of censoring and follow-up patterns (Figure 2).

Overall Kaplan-Meier survival curve among neonates admitted to NICU from November 2022 to February 2023.
Neonates who did not cry immediately at birth had significantly lower survival probabilities (38.1%) compared to those who cried immediately (80.2%) (p = 0.001). The median survival time for neonates who did not cry at birth was 10 days (95% CI: 6.49–13.51). This difference was statistically significant with p-value <0.001. The x-axis is labeled clearly as “Time (days)” spanning from 0 to 28 days to represent neonatal follow-up time. The y-axis is labeled as “Estimated Survival Probability,” ranging from 0 to 1, corresponding to 0% to 100% survival.
Two survival curves compare neonates who cried immediately at birth (higher survival) versus those who did not (lower survival). Small tick/censor marks appear on curves at times when neonates were censored (lost to follow-up or study end without death). Below the curves, risk tables display the number of neonates still at risk at key time points (e.g., 0, 7, 14, 21, 28 days), contextualizing reliability of survival estimates. This presentation visually clarifies the significant survival difference between groups, with median survival around 10 days for neonates who did not cry immediately (Figure 3).

Comparison of the survival function of neonates who cried versus did not cry immediately at birth admitted to NICU from November 2022 to February 2023.
Predictors of Neonatal Mortality
After controlling for confounding variables, multivariable Cox proportional hazards regression analysis identified seven significant predictors of neonatal mortality:
Age of mother: Neonates born to mothers aged >30 years had twice the hazard of mortality compared to those born to mothers <25 years ([AHR] = 2.10, 95% CI: 1.26–3.50).
ANC follow-up: Neonates born to mothers without ANC follow-up had three times the hazard compared to those whose mothers had ANC (AHR = 3.09, 95% CI: 1.32–7.22).
Place of delivery: Neonates delivered at health centers showed lower mortality hazard vs. hospitals (AHR = 0.51, 95% CI: 0.26–0.98), likely due to referral bias—low-risk cases remain at health centers, while high-risk transfers to hospitals incur delays.
Crying immediately at birth: Neonates who did not cry immediately had nearly three times higher hazard compared to those who cried (AHR = 2.61, 95% CI: 1.70–4.01).
RDS: Neonates with RDS had almost seven times higher hazard (AHR = 6.96, 95% CI: 3.60–13.43).
MAS: Neonates with this syndrome had nine times higher hazard (AHR = 9.16, 95% CI: 3.58–23.4).
Perinatal asphyxia: Those with perinatal asphyxia had four times higher hazard (AHR = 4.34, 95% CI: 2.01–9.35) (Table 5).
Bivariable and Multivariable Cox Regression Analysis of Neonates Admitted to NICU from November 2022 to February 2023.

AHR = Adjusted Hazard Ratio; CHR = Crude Hazard Ratio; IAD = Instrumental Assisted Delivery; MCHC = Maternal and child health center; SVD = Spontaneous Vaginal Delivery; 1.00 = Reference Category; CI=confidence interval.
Discussion
This prospective cohort study evaluated the survival status and predictors of neonatal mortality among neonates admitted to the NICU. The neonatal mortality rate observed was 35.5 per 1,000 neonate-days, with an overall mortality proportion of 23.6% (95% CI: 19.8, 27.4). This finding aligns with studies conducted in Eastern Ethiopia (20%) and Debre Markos (21.3%) (Alebel et al., 2020; Desalew et al., 2020). However, it was higher than reports from Dire Dawa (11.4%) (Thomas et al., 2021), Hawassa (14.2%) (Taye et al., 2024), Nekemte town (15.3%) (Tolossa et al., 2022), Southern Ethiopia (16.5%) (Orsido et al., 2019), and Hadiya zone (18.8%) (Moges et al., 2021), possibly reflecting differences in sample sizes, socio-economic factors, health service utilization, and retrospective versus prospective study designs (Orsido et al., 2019; Thomas et al., 2021). These differences may reflect variations in sample sizes, socio-economic factors, healthcare utilization, institutional settings, economic disparities, and study designs, with retrospective cohorts potentially underestimating mortality due to incomplete records (Taye et al., 2024).
The cumulative neonatal survival proportion at 28 days in this study was 66.1%, which is lower than the 71.11% reported in Amhara regional referral hospitals and 93.96% in Tigray, Northern Ethiopia (Mengesha et al., 2016; Mengistu et al., 2020). This discrepancy likely arises because this study focused on admitted neonates, representing a high-risk group, whereas the other studies included all live births, which generally have better outcomes. Conversely, the survival proportion in this study exceeds the 57.14% reported in a study at the University of Gondar, which exclusively investigated preterm neonates—a particularly vulnerable subgroup (Yismaw et al., 2019). This suggests that risk of death among premature neonates is higher and they frequently succumb shortly after birth due to adjustment difficulties outside the uterus (Huka et al., 2023; Toma et al., 2021).
Survival at the end of the first day was 90.1%, comparable to Amhara regional referral hospitals (89.15%) (Mengistu et al., 2020), but lower than findings in Southern Ethiopia's Bombe Primary Hospital (97.2%) (Berhanu et al., 2021) and the University of Gondar (96.71%) (Yismaw et al., 2019). Differences may reflect study design variability, as retrospective studies risk underestimating early mortality due to incomplete data.
Maternal age over 30 years was associated with a twofold increased risk of neonatal death compared to mothers under 25 years. This is consistent with findings from Sudan, Southern Ethiopia, and Amhara regional referral hospitals (Bashir et al., 2013; Eshete et al., 2021; Mengistu et al., 2020). Advanced maternal age (AMA) influences mortality through a complex interplay of biological, health system, socio-cultural, and nursing-related factors. AMA is associated with the increased risk of adverse neonatal outcomes including preterm birth, low birth weight, congenital anomalies, and perinatal asphyxia. Biologically, AMA increases maternal comorbidities such as hypertension and diabetes, and contributes to placental insufficiency, which compromise fetal development and neonatal health. Studies in Ethiopia and globally document that neonates born to AMA mothers have higher mortality, partly due to increased perinatal complications and lower Apgar scores. Socio-economic factors, such as lower access to quality maternal health services and delayed care-seeking, exacerbate risks. Older maternal age is linked to higher incidence of complications and prematurity, which may explain this increased risk (Kim et al., 2021; Mutz-Dehbalaie et al., 2014; Tekeba, Techane et al., 2024).
Lack of ANC follow-up tripled the hazard of neonatal mortality, aligning with previous studies from Nigeria, Western Ethiopia, Wolaita, Debre Markos, Hadiya, Gedeo, and Asella (Adetola et al., 2011; Alebel et al., 2020; Aredo et al., 2024; Eshete et al., 2021; Moges et al., 2021; Orsido et al., 2019; Tolossa et al., 2022). ANC offers critical opportunities to detect and manage pregnancy complications early and impart birth preparedness education, ultimately reducing neonatal morbidity and mortality (Tolossa et al., 2022). Socio-economic factors, such as lower access to quality maternal health services and delayed care-seeking, exacerbate risks. Inadequate ANC compounds this risk by missing opportunities for early detection and management of pregnancy complications, vaccination, and birth preparedness education. Health system gaps like shortages of skilled providers, limited infrastructure, and poor continuity of care reduce ANC effectiveness, especially in rural and underserved areas (Asaye et al., 2025; Ethiopian Public Health Institute, 2022). From a nursing perspective, failure to provide comprehensive ANC including counseling and timely intervention increases vulnerability to adverse outcomes. Nurses and midwives play a pivotal role in identifying high-risk pregnancies and facilitating referrals, but may face challenges such as heavy workloads and limited resources. Socio-cultural barriers including traditional beliefs, gender norms, and financial constraints also reduce ANC attendance and skilled birth attendance, further threatening neonatal survival (Alemu et al., 2025; Awoke et al., 2024; Gebrekirstos et al., 2025; Ministry of Health Ethiopia, 2024). AMA and lack of ANC influence neonatal mortality through biological vulnerabilities compounded by systemic inadequacies and socio-cultural barriers. Addressing these factors requires integrated interventions targeting health system strengthening, community engagement, and capacity-building for maternal and neonatal care providers to improve outcomes (Tekeba, Tamir et al., 2024).
Interestingly, neonates delivered at health centers had a lower mortality hazard than those at hospitals (adjusted HR 0.51, 95% CI: 0.26–0.98). This counterintuitive finding likely stems from referral bias: low-risk cases are typically managed at health centers, whereas high-risk mothers are transferred to hospitals, where delays may contribute to adverse outcomes. Lack of timely transportation, financial constraints, and hospital capacity issues may exacerbate this risk. As no prior studies have reported this association, further research is needed to understand the impact of delivery setting on neonatal survival.
Neonates who did not cry immediately after birth had nearly a threefold increased mortality risk, consistent with studies from the University of Gondar and Nekemte Referral Hospital (Gudayu et al., 2020; Roro et al., 2019). Not crying signifies ineffective lung inflation and cardiopulmonary instability, serving as a simple clinical indicator of increased mortality risk (Kc et al., 2020).
RDS increased mortality risk nearly sevenfold, corroborating studies from Mexico, Afar, Debre Markos, Hadiya, and Addis Ababa (Alebel et al., 2020; Menalu et al., 2022; Moges et al., 2021; Reyes et al., 2018; Zekarias et al., 2024). The vulnerability of premature neonates, who represent over one-third (37.3%) of admissions, likely explains this high association as RDS is a leading cause of death among this group (Basiri et al., 2015; Dev et al., 2022; Mbawala et al., 2014; Taye et al., 2024).
MAS increased the risk of death ninefold. MAS, resulting from inhalation of meconium-stained amniotic fluid, is a significant cause of respiratory distress and a major contributor to neonatal morbidity and mortality, frequently necessitating NICU admission (Adugna et al., 2025; Dini et al., 2024; Louis et al., 2014).
Perinatal asphyxia quadrupled neonatal mortality risk, supporting findings from Ghana (Apanga et al., 2024) and various Ethiopian regions, including East Wollega, Wolaita, Hadiya, Hawassa, and Addis Ababa (Abera et al., 2021; Menalu et al., 2022; Moges et al., 2021; Orsido et al., 2019; Taye et al., 2024). Asphyxia impairs neonatal respiratory function at birth and is a critical determinant of survival (Woday et al., 2019).
Neonatal nurses play a pivotal role in the early identification and management of common life-threatening conditions such as respiratory distress, perinatal asphyxia, and MAS. Through continuous monitoring of vital signs, assessment of respiratory effort, and timely initiation of supportive therapies such as oxygen administration, CPAP, and suctioning nurses can stabilize neonates and reduce morbidity and mortality. Their expertise in neonatal resuscitation and adherence to protocols improves outcomes for infants experiencing birth asphyxia (Alemu et al., 2025; Mathai et al., 2007). Furthermore, nurses and midwives are essential in providing antenatal education and counseling, emphasizing birth preparedness, danger sign recognition, and the importance of facility-based deliveries. Community-based follow-up programs, often led by nurses, facilitate early postnatal visits and monitor growth and development, ensuring prompt referral of at-risk neonates (Alemu et al., 2025). Training and capacity-building interventions led by experienced neonatal nurses enhance the skills of less experienced staff and birth attendants, strengthening emergency newborn care across facilities. Such programs focus on evidence-based practices, newborn resuscitation, and supportive care techniques, which have proven effective in reducing neonatal mortality in resource-limited settings (Awoke et al., 2024).
Strengths and Limitations
The study's strengths include its prospective cohort design with 28-day follow-up, enabling timely and comprehensive assessment of neonatal survival during hospitalization and post-discharge, which reduces biases typical in retrospective studies. Inclusion of consecutive NICU admissions with daily clinical monitoring and systematic follow-up captured data from a high-risk population, allowing robust evaluation of mortality predictors.
Limitations involve being single-center in a referral hospital NICU with many severely ill cases, limiting generalizability and possibly overestimating mortality. Referral delays and inborn versus outborn status were not modeled, potentially confounding delivery place associations. Lack of clustering adjustment for twins and variable post-discharge follow-up response may affect precision and outcome completeness. Analytical limitations include potential overfitting, omitted variable bias, lack of model validation, and unmeasured confounders like socio-economic status and staffing ratios. Counterintuitive findings, such as lower mortality at health centers, likely reflect unmeasured referral severity bias; these warrant cautious interpretation and further research. No recommendations are intended for preferring health centers over hospitals—multi-site studies are needed.
Implications for Practice
Enhancing Antenatal Care Coverage
The finding of this study that lack of ANC triples neonatal mortality risk (AHR 3.09, 95% CI 1.32–7.22) underscores ANC's role in early detection of risks like preterm birth and maternal complications (e.g., anemia in 9.3% of cases). High-quality ANC—defined per WHO as ≥8 contacts—enables screening, iron-folic acid supplementation (received by 80.6% here), and birth preparedness, reducing hazards by addressing modifiable factors. Nurses should lead community outreach to boost uptake from 97.2% ever-attendance to ≥4 visits (currently 69.4%), targeting rural mothers (24.8% of sample) via home visits and education on danger signs. Policy-wise, integrate ANC with health extension programs to achieve Ethiopia's Health Sector Transformation Plan II goals.
Optimizing Institutional Deliveries with Referral Awareness
Neonates delivered at health centers showed 49% lower mortality hazard than hospitals (AHR 0.51, 95% CI 0.26–0.98), likely due to referral bias: low-risk cases (e.g., spontaneous vaginal deliveries, 54.8%) stay local, while high-risk transfers delay care. This counterintuitive result cautions against preferring health centers outright; instead, strengthen first-line facilities with basic resuscitation tools. Midwives/nurses should promote ≥94.6% health professional-attended births (current rate) but ensure seamless referrals via ambulance networks, reducing home deliveries (6%). Conceptualize as a tiered system: equip health centers for stable cases, reserving hospitals for complications like RDS (14.3% prevalence).
Immediate Neonatal Resuscitation and Supportive Care
Failure to cry at birth nearly tripled mortality (AHR 2.61, 95% CI 1.70–4.01), signaling cardiopulmonary instability in 30.2% of admissions. Nurses must prioritize Helping Babies Breathe protocols: dry, stimulate, and bag-mask ventilate (used in 10.3%) within the Golden Minute. For RDS (AHR 6.96, 95% CI 3.60–13.43; 14.3% cases), MAS (AHR 9.16, 95% CI 3.58–23.4), and asphyxia (AHR 4.34, 95% CI 2.01–9.35), scale CPAP (20% usage) and oxygen in all NICUs, targeting preterm neonates (37.3%). Train staff on kangaroo care and early breastfeeding (only 29.2% within 1 h), conceptually bridging intrapartum stability to postnatal survival.
System-Level Strengthening: Referrals, Transport, and Follow-Up
With 41% deaths in first 24 h and survival dropping to 66.1% by day 28, post-discharge monitoring (94.4% postnatal care) is vital. Implement daily phone/home visits by nurses/health extensions for high-risk neonates (e.g., low birth weight, 43.5%). Address transport gaps exacerbating referral risks via subsidized ambulances and community financing.
Empowering Nursing Workforce
Nurses/midwives (key in 94.6% deliveries) should drive identification (e.g., hypothermia in 59.5%), resuscitation, ANC counseling, and follow-up. Provide simulation-based training on NICU protocols, empowering them as change agents in Ethiopia's 23.6% NICU mortality context.
Health System and Community Integration
Bolster infrastructure (e.g., CPAP units, staffing), training, and awareness campaigns are to increase ANC/institutional uptake. Partner with Ethiopia's Ministry of Health for scalable interventions, conceptually aligning predictors with Sustainable Development Goal 3.2 (≤12 deaths/1,000 live births by 2030). These evidence-based steps can halve hazards from top predictors, improving survival from 66.1% to national targets.
Recommendations to Improve Neonatal Mortality Rates
To improve neonatal mortality rates, focus on expanding high-quality ANC and promoting institutional deliveries, especially at health centers with lower mortality risk. Prioritize maternal health for women aged 30 and above. Implement immediate neonatal care, including resuscitation, and manage respiratory distress, meconium aspiration, and perinatal asphyxia. Equip NICUs with respiratory support like CPAP and bag-mask ventilation. Strengthen referral systems with timely transport and post-discharge follow-up. Promote community awareness on ANC and institutional deliveries, train healthcare workers in neonatal care, and ensure skilled staff and essential equipment in facilities. These actions collectively reduce neonatal deaths effectively.
Conclusion
Neonatal mortality remains high among NICU admissions in the study area, with significant predictors including maternal age over 30, lack of ANC, place of delivery, failure to cry at birth, RDS, MAS, and perinatal asphyxia. These findings emphasize the need to strengthen maternal and neonatal healthcare through improved ANC coverage, institutional deliveries with referral systems, and enhanced neonatal resuscitation and respiratory support. While the study's design and observation offer valuable insights, methodological limitations affect generalizability. Future research should enhance analytic rigor and population representativeness. Policy efforts must focus on expanding access to quality care, building workforce capacity—particularly among nurses and midwives—and integrating community education and follow-up. Investment in infection control, infrastructure, and data monitoring aligns with national programs such as the Quality Equity and Dignity initiative and the 10 Million Safer Births Initiative, supporting Ethiopia's progress toward SDGs. The active role of neonatal nurses and midwives in early complication management and multidisciplinary collaboration is vital, consistent with Ethiopia's Health Sector Transformation Plan II priorities.
Supplemental Material
sj-docx-1-son-10.1177_23779608261437595 - Supplemental material for Neonatal Survival and Predictors of Mortality Among Neonates Admitted at Neonatal Intensive Care Unit in Ethiopia: A Prospective Cohort Study
Supplemental material, sj-docx-1-son-10.1177_23779608261437595 for Neonatal Survival and Predictors of Mortality Among Neonates Admitted at Neonatal Intensive Care Unit in Ethiopia: A Prospective Cohort Study by Gemechu Dereje Feyissa, Daniel G/tsadik, Tilaye Workneh, Endashaw Mandefro Kidane and Mokonnen Dereje in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261437595 - Supplemental material for Neonatal Survival and Predictors of Mortality Among Neonates Admitted at Neonatal Intensive Care Unit in Ethiopia: A Prospective Cohort Study
Supplemental material, sj-docx-2-son-10.1177_23779608261437595 for Neonatal Survival and Predictors of Mortality Among Neonates Admitted at Neonatal Intensive Care Unit in Ethiopia: A Prospective Cohort Study by Gemechu Dereje Feyissa, Daniel G/tsadik, Tilaye Workneh, Endashaw Mandefro Kidane and Mokonnen Dereje in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgment
The authors would like to thank the data collectors, the NICU staff of AHMC for their cooperation, and the mothers of neonates who voluntarily participated and provided the required information to complete this research.
Ethical Statement
The study protocol conformed to the Declaration of Helsinki and was approved by the Institutional Review Committee of Rift Valley University (Ref/No: 18817/28/22). Administrative permission was obtained from AHMC and the NICU. Verbal informed consent was obtained from mothers or legal guardians after providing clear explanations of the study's purpose. The ethics committee waived written informed consent given the minimal risk involved, with assurances of confidentiality and secure data management. Only the principal investigator accessed identifiable data.
Authors Contributions
GDF contributed to study conception, design, and acquisition of data, software, analysis and interpretation, a critical review of the document and development of the manuscript. DG and TW participated in reviewing the study design, data analysis, interpretation, and revision of the manuscript. EMK and MD involved in reviewing the study design, data analysis, and interpretation. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing and Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.