
Abstract
Background
Obesity management in young women necessitates interventions that include dietary modification and physical exercise. High-intensity lifestyle modification is effective in managing obesity in young women.
Objectives
The study determined the effectiveness of a nurse-led lifestyle modification intervention (NLLMI) on obesity among young women in India.
Methods
The study adopted a quasi-experimental pre- and post-interventional control group research design. The study was conducted among obese young women in the communities of Jabalpur, Madhya Pradesh, India. The participants were selected using convenient sampling technique. The sample included 150 women in the study group and 150 in the control group. The NLLMI comprising of exercises and dietary modifications were taught to the participants for 30 min three times a week for 24 weeks. Thereafter, they were encouraged to follow the diet and perform the exercises on their own for the next 12 weeks. Practice diary was maintained by the participants and they were encouraged to continue the intervention through the phone. The participants in the control group did not engage in the NLLMI until the post-test. However, they did receive the same NLLMI after the trial was over.
Results
There was a high statistically significant difference (p = 0.001) between the study group and the control group the after 12th and 24th weeks of NLLMI. The study group had a significant reduction in BMI after the intervention.
Conclusions
Young obese women may benefit from a NLLMI if they regularly follow the healthy eating habits and physical exercise.
Introduction
Overweight (BMI ≥ to 25.0 kg/m2) and obesity (BMI ≥ to 30 kg/m2) increase the risk of numerous diseases such as diabetes, cardiovascular disease (CVD) and cancer (Status, 1995). Overweight and obesity are increasing in number in the past decade as an epidemic and pandemic (Swinburn et al., 2011) and are considered as one of the major public health challenges (WHO, 2014a). In 2016, WHO identified more than 1.9 billion adults who are 18 years and older as overweight and over 650 million as obese. In India, more than 135 million people are obese. The prevalence of obesity varies from 11.8% to 36.3% due to the differences in age, gender, socio-economic status and geographic nature of the environment (Ahirwar & Mondal, 2019). With a steady increase in the number of overweight and obese people, there is a growing public health concern on the body size and lifestyle diseases (Sand et al., 2015).
Obesity occurs due to underlying energy imbalance between consumed and expended calories. In recent days, obesity epidemic is increasing due to increased energy from greater availability of energy-dense food. Additionally, economic, social and environmental factors related to food supply play a significant role on the individual's ability to achieve the balance (Yoo, 2018). A 13-year follow-up study identified that the waist circumference of young people who consumed fatty food was higher than those who consumed the lowest fast food. Likewise, higher incidences of elevated triglycerides were found in these people (Lopez-Lopez et al., 2021). Overweight and obesity poses various negative health consequences including type 2 diabetes, sleep apnoea, cancer, sexual and reproductive health issues, cervical and breast cancer, mental health disorders and metabolic disturbances (WHO, 2017).
Young adult women are considered as a vulnerable group for overweight and obesity considering their appearance and weight balance (Sand et al., 2015). In general, women have a greater proportion of body fat than men (Wu & O'Sullivan, 2011). Women maintain a greater percentage of body fat mass (FM) than men from the onset of puberty to menopause despite smaller energy intake per kg lean mass (Kant & Graubard, 2006) and preferential use of fat as a fuel during exercise compared to men (Tarnopolsky, 2008). A possible reason for these findings is that the greater FM in women relates to more effective fat storage during non-exercising periods, especially during postprandial periods. In addition, the reproductive years and gestation are characterised by elevated levels of ovarian hormones. The oestrogens contribute to the gender differences in FM and the gestational changes in body composition (O'Sullivan, 2009).
Obesity negatively affects fertility in young women due to metabolic and hormonal alterations including hyperinsulinemia and hyperleptinemia, hyperandrogenism and insulin resistance (Kulie et al., 2011; Lash & Armstrong, 2009). Maternal health has been reported to decline as a result of overweight and obesity (Canto-Cetina et al., 2018; Lindsay et al., 2018; White et al., 2017). Additionally, obesity causes early loss of pregnancy, high risk for obstetrical conditions, higher caesarean rates, increased maternal and neonatal mortality rates and congenital malformations (Harper, 2015; Poston et al., 2016).
Lifestyle modification interventions including nurse-led lifestyle modification interventions (NLLMI) have been beneficial in reducing cardiovascular risk scores in different populations (Li et al., 2022; Saffi et al., 2014; Zheng et al., 2020; Zhu et al., 2013). In particular, the outcomes of nurse-led interventions of diet and exercise have extensively been examined in lifestyle intervention research (Bennett & Sothern, 2009; Castro et al., 2020; Lloyd et al., 2012; Psouni et al., 2016; Samdal et al., 2017). A systematic review of 18 studies that evaluated the effectiveness of nurse-led interventions in diverse settings found that diet and exercise interventions were more effective in preventing childhood and adolescent overweight and obesity (Whitehead et al., 2021). Additionally, a 16-week intervention with exercise significantly reduced the BMI and improved the components of metabolic syndrome (Ismail, 2022).
In most the Asian countries, reduced physical activity due to mechanisation, improved motorised transport and viewing television for a longer duration have resulted in overweight and obesity (Mazidi et al., 2018; Venkatrao et al., 2020). India in particular has more than 30 million obese people and the number is increasing alarmingly (Hadaye et al., 2020). Despite much effort has been taken to prevent childhood and adolescent obesity (Hennessy et al., 2019), high-quality evidence is limited related to obesity-related outcomes in India. A systematic review of 16 interventional studies concluded that physical activity, dietary modification, education and behavioural therapy significantly reduce body mass index (BMI), triglycerides and systolic and diastolic blood pressure (Rajjo et al., 2017). The role of nurses in the obesity prevention in the young women has been under-researched despite nurses play a vast role in the healthcare workforce worldwide (World Health Organization, 2016). Thus, we designed this study to determine the effectiveness of NLLMI on obesity among young women in India with an intention that nurses apply lifestyle interventions in routine care for young women with obesity.
Materials and Methods
Research Approach
A quantitative research approach was adopted in the study.
Research Design
The study adopted a quasi-experimental pre and post-test control group research design.
Setting
The study was conducted in the rural communities named Panagar block and Shahpura block in Jabalpur, Madhya Pradesh, India. Panagar has 80-g panchayat with a population of 236,848 and 113,614 females and Shahpura has 84-g panchayat with a population of 191,710 and 92,557 females. After the initial survey, the study and control groups were randomly allocated. Based on the survey report, there were 113,614 females and 92,557 young women residing in the two villages who were potentially eligible to participate in the study.
Population
The population for this study included all obese young women whose BMI was more than 24.9.
Sample Size
The sample size was calculated and was also computed by power analysis. The estimated sample size was 287. Considering an attrition rate of 10%, the sample size was rounded to 300, consisting of 150 in each group.
Sampling Technique
A non-probability convenient sampling technique was used to select young obese women for the study. In the first stage, ten villages including five from Panagar and five from Shahpura were selected using the lottery method. During the second stage of sampling, a list of addresses of all women aged 20–40 years was obtained from the Primary Health Centre (PHC). All the young women were requested to gather at the primary health center. Then, the weight and height were taken and young women having BMI more than 24.9 were taken for the study. In the third stage, women who fulfilled the inclusion criteria were selected. Approximately 20–25 young obese women from each village participated in the study. Panagar block was chosen as the study group and the Shahpura block as the control group.
Inclusion Criteria
The study included obese young women who had a BMI of more than 24.9; in the age group of 20 to 40 years; available during data collection and who were able to understand and speak Hindi, an Indian language.
Exclusion Criteria
The study excluded young women with Gynaecological problems such as uterine fibroids, dysfunctional uterine bleeding, prolapsed uterus and having any surgical incision; pregnant women or women up to 6 weeks’ postpartum period.
Ethical Considerations
Formal ethical approval was obtained from NIMS University review board and ethics committee. (Ref No: NIMSUNI/IEC/2019 dated 29 July 2019). Both written and verbal information about the study’s purpose was given in the Hindi language to all women who participated in the study. Women were asked to participate voluntarily. The study objectives, benefits and period involved in practicing the lifestyle modification intervention were explained in the consent form. Women who agreed to participate had the right to withdraw at any time during the study. None of the identifying information of the participants was collected. The data collection sheets were coded and only the investigators of the study had access to the collected data. The research was conducted according to the Helsinki ethical recommendations.
Pilot Study
The pilot study was conducted with 10% of the total sample of the main study. No significant modifications were made in the tool after the pilot study. Inter-rater/inter-observer method was used to test the reliability of the tool and the reliability was r = 0.87
Data Collection Instruments
Socio-demographic information, clinical profile and WHO Asian Pacific BMI scale were the tools used in the study. The following BMI classification was used to determine the BMI of the study participants.

Description of NLLMI
Diet modification and physical exercise were the main constituents of this program. It consisted of a structured exercise program developed with the help of a physiotherapist. The following floor exercises were used to reduce the total body fat:
Leg raise exercise = 5 set 10–15 repetition, Plank = 30 s × 5set
Side plank = 30 s × 5 set, holding leg at 45 degrees = 5 set 20–30 s
Knee chest exercise = 5 set × 10–15 repetition.
Sit-Ups = 3 set 10–15 repetition
Walking: Brisk walking for 10 min every day and gradually increasing the time from 10 to 30 min. Exercises were monitored by the investigator for 30 min/day thrice a week for the duration of 24 weeks. Thereafter for the next 12 weeks, they were reinforced to practice these exercises on their own.
Diet: The structured NLLMI consisted of an approximate caloric intake as per the caloric requirement proposed by ICMR 2010 (Energy required for BMR, i.e., 25 kcal/kg/day + energy for daily physical activity + energy for SDA) (7). It was suggested as per their pre-study weight and BMI. Diet chart (typically 1200–1500 kcal/) was advised for obese young women. This included cereals/day, pulses/day, meat including egg, vegetables including green leafy and skimmed milk, sprouts and salads a 4 pm snacks including fruit/sugar-free biscuits. Also, a restriction of oil intake to 20 gms/ day and consumption of sugar to a minimum was suggested. The vegetarian diet included pulses and legumes. And recommended an intake of a minimum of 2000 mL of drinking water per day. A practice diary was maintained to confirm the regular practice of NLLMI. Subjects were followed up telephonically every 7 days.
Data Collection Procedure
Prior permission was taken from the chief medical officer and block medical officer and consent was taken from the participants. The baseline characteristics of the participants were recorded before starting the intervention. After the assessment of Pre interventional BMI, 300 obese young women were selected for the study. Among them, 150 were taken up in the study and 150 in the control group. The BMI of the young woman was calculated by finding the height and weight of the young woman. Height was measured by a Stadiometer capable of measuring up to the accuracy of 0.1 cm. Height was measured by making the young woman stand without footwear, with feet parallel; heels, buttocks and occiput touching the measuring rod; hands hung by the sides and head held comfortably upright. Weight was calculated with a portable balance device with an accuracy of 100 g. Young Women were instructed to stand on the balance with feet apart without footwear and look straight.
After the pre-test, the obese young women in the study group were taught about the NLLMI. The exercise was demonstrated to the study group by the investigator. The exercise session was conducted in a public hall. The investigator remained with the young women while they completed the questionnaire and answered the questions. It took 30–35 min to collect the pre-test data from each sample. After the pre-test, no specific attention was given to the participants of the control group. The participants of the study group received NLLMI. However, the participants of control group received the NLLMI after the post-test was conducted for both the study and control group considering the principle of beneficence.
Data Analysis
Statistical Package for the Social Sciences version 16 software (SPSS Inc., 2012) was used for the data analysis. The student's independent t-test was used to compare values between the study and control groups. The chi-square test was used for determining the association between the variables. A p-value less than 0.05 was considered to be statistically significant.
Results
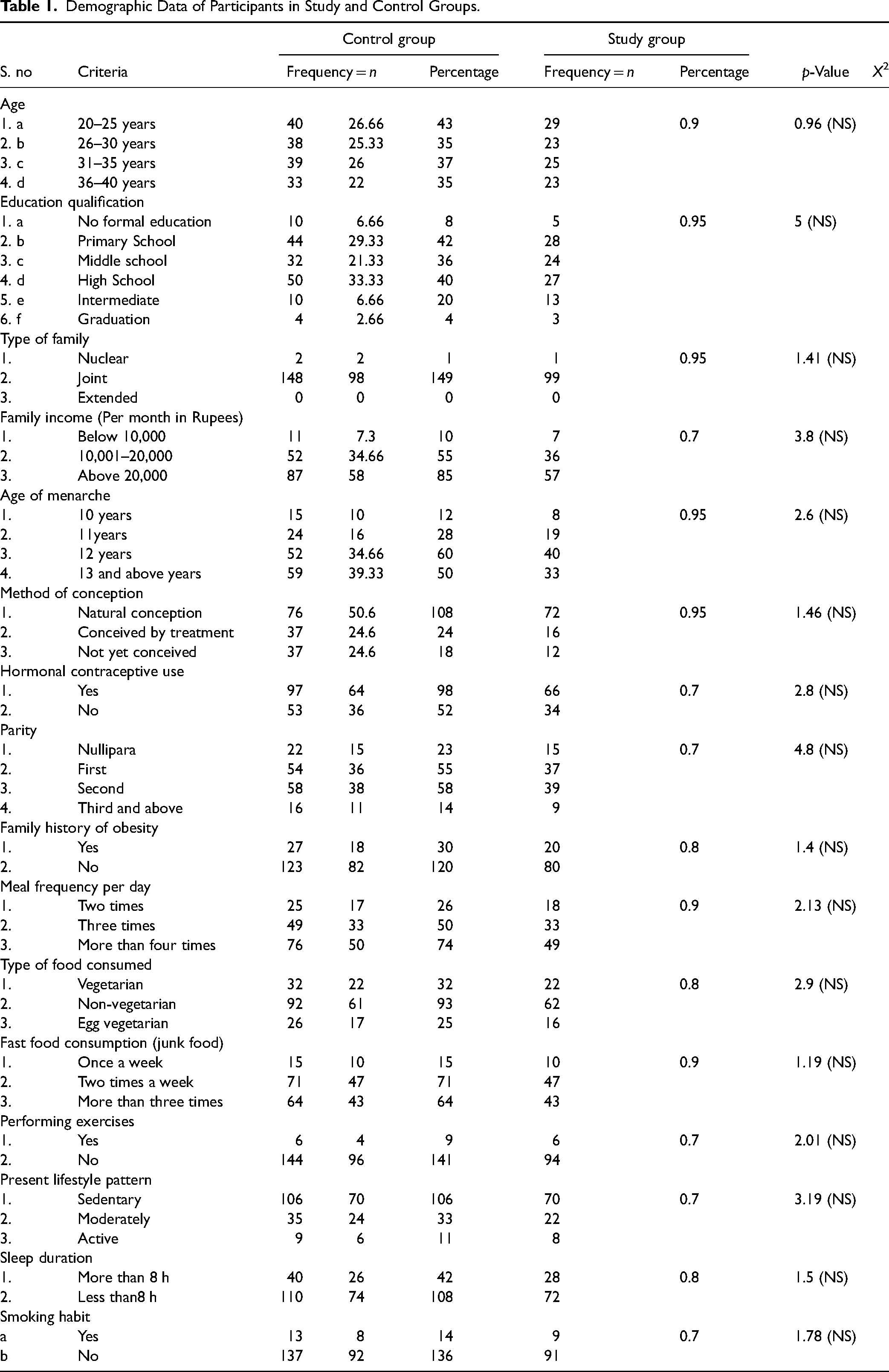
The baseline values were not significantly different between the study and control groups for any of the demographic variables, including age (p = 0.96), educational qualification (p = 5), type of family (p = 1.41), family income (p = 3.8), age of menarche (p = 2.6), method of conceiving (p = 1.46), hormonal contraceptive use (p = 2.8), parity (p = 4.8), family history of obesity (p = 1.4), meal frequency per day (p = 2.13), types of food consumed (p = 2.9), fast food consumption (p = 1.19), performing exercises (p = 2.01), present lifestyle pattern (p = 3.19), sleep duration (p = 1.5) and smoking habits (p = 1.78; Table 1).
Demographic Data of Participants in Study and Control Groups.
Figures 1 and 2 show the BMI of the study participants in the study. The maximum reading for study group was in Grade I (66%), 34% were in Grade II, whereas none were in overweight and normal weight in the pre-intervention. The result showed that in the 12th week, the maximum reading was in Grade I (62%), followed by 36% in Grade II and overweight was 2% and the least reading was in normal weight (0), respectively. Furthermore, in the 24th week, the maximum reading in Grade I was 67%, 33% in Grade II and overweight and normal weight readings were 0, respectively.

Distribution of participants according to the body mass index (study group).

Distribution of participants according to the body mass index (control group).
BMI in the control group showed the reading in Grade I as 66%, 34% in Grade II and none in overweight and normal weight (0), respectively, in the pre-intervention. In the 12th week, the maximum reading was 62% in Grade I, 36% in Grade II, 2% in overweight and the least reading was 0 in normal weight. During 24th week, the maximum reading from Grade I was 67%, 33% in Grade II and overweight and normal weight was 0, respectively.
Comparison Between Pre and Post-Test Body Mass Index Scores in Control Group at 12 Weeks.

Note. NS = non-significant.
The pre-test and post-test BMI in the control group at 12 weeks were statistically tested by applying the t-test method @ 0.05%. With the calculated value of t (0.16), which was less than the table value (1.98), the difference between the pre and post-test was non-significant. The pre-test and post-test BMI in the control group at 24 weeks were statistically tested by applying the t-test method @ 0.05%. With the calculated value of t (0.2), which was less than the table value (1.98), the difference between the pre and post-test was non-significant.
Comparison Between Pre and Post-Test Body Mass Index Scores in Control Group at 24 Weeks.

Note. NS = non-significant.
Comparison Between Pre and Post-Test Body Mass Index Scores in Study Group at 12 Weeks.

Note. HS = highly significant.
The pre-test and post-test BMI in the study group at 12 weeks were statistically tested by applying the t-test @ 0.05%. Having the calculated value of t (4.84), which was more than the table value (1.98), the difference between the two conditions was highly significant, showing the effectiveness of the NLLMI on the BMI scores. Similarly, the pre-test and post-test BMI in the study group at 24 weeks were statistically tested by applying the t-test method @ 0.05%. With the calculated value of t (11.61), which was more than the table value (1.98), the difference between the pre and post-test was highly significant, showing the effectiveness of the NLLMI on the BMI scores.
Comparison Between Pre and Post-Test Body Mass Index Scores in Study Group at 24 Weeks.
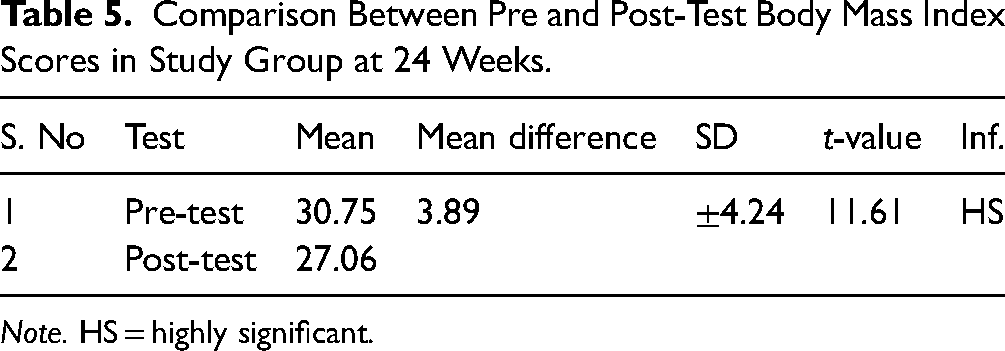
Note. HS = highly significant.
Discussion
Obesity is a national healthcare crisis. People who are obese are at increased risk of medical, emotional, psychological and behavioural complications (Williams, 2022). In particular, young women who are overweight and obese are unaware of their biological risks to be passed on to ther unborn children (Freer, 2016). Furthermore, the burden of obesity has traditionally been associated with rich, living in urban areas in developing countries (Martorell et al., 2000; Neuman et al., 2013). However, the obesity risk has moved to rural areas in the last three decades. In particular, rural areas account for 55% of global rise in mean BMI between 1985 and 2017 (Brenner et al., 2019). It has been observed that with increased life expectancy, rural women spend most of their time in household activity and the upbringing of the children and less likely to take care of their physical health, which in turn increases the risk associated with obesity (Yoosefi Lebni et al., 2020).
Earlier studies reported that people who are poor and less educated have more health problems than richer and educated (Marmot et al., 2008; Mikkonen, 2010). It shows that there are disparities existing in the access and availability to health care (Van Lerberghe, 2008). Moreover, as the number of female-headed households increased dramatically in the recent centuries, especially in developing countries (Rafii et al., 2013) due to addiction or disability of husband, divorce, death of spouse, migration, increased life expectancy among women and being abandoned by husband (Horrell & Krishnan, 2007). Female-headed households are forced to play multiple, and conflicting roles and lack of access to high-paying jobs. Thus, these women are unable to maintain their health due to problems such as poor socio-economic status, poverty and multiple responsibilities (Connell et al., 2012). Therefore, in order to improve the equity and patient-centred care, it is necessary to better understand and address the underlying causes of poor health. The WHO in 2009 itself identified that women and girls have specific health needs around the world and the health systems fail to identify them. Therefore, WHO calls for action to address the health issues surrounding women to improve their health status. Considering the status of rural women and WHO's recommendations, the authors of the study decided to deliver NLLMI to obese young women in the rural villages of India to prevent them developing obesity-related complications and to improve their overall health status.
In our study, both the participants of the study and the control group had Grade I and II obesity in the pre-intervention. Similarly, many studies reported obesity in young women across the world (Fryar et al., 2018; Nglazi & Ataguba, 2022; Sand et al., 2015; Vahratian, 2009). The increasing prevalence of overweight and obesity is a critical public health problem for young women of childbearing age. Moreover, obesity in young women is linked to both short- and long-term health problems in the women and their children. Furthermore, chronic diseases such as diabetes, cancer and CVDs are linked to obesity later in life (Nglazi & Ataguba, 2022). Considering the increasing trend in overweight and obesity, it demands public health attention and increased public awareness is needed about obesity and the health consequences of obesity.
Wadden et al. (2011) found that 10% of participants achieved weight loss at the first year, whereas 42.2% of participants lost weight at the end of 4th year. He further found that the young people who has favourable physical activity and dietary control maintained weight loss compared to those who did not. This long-term study provides a critical evidence that a comprehensive lifestyle modification program can promote clinically significant weight loss in overweight and obese participants. Similarly, Donnelly et al. (2016) identified that a 12-week weight loss intervention resulted in weight reduction in young women. More recently, Webb and Wadden, (2017) referring to the Guidelines for the management of overweight and obesity in adults recommends that a minimum of 6 months high-intensity comprehensive lifestyle intervention consisting of a reduced calorie intake, increased physical activity and behaviour modification might result in typically loosing approximately 8 kg. This approach not only reduces the body weight; it also improves the quality of life of people who are obese. Likewise, the results of our study showed the NLLMI in young women significantly reduced BMI by practicing NLLMI for 24 weeks in comparison to the control group.
In consistent to our study findings, Wilson (2020) suggests and recommends that lifestyle modifications are the first-line therapy for people with overweight and obesity. Furthermore, moderately reduced calorie intake, increased physical activity and behavioural modifications including motivational interviewing and cognitive behaviour therapy are recommended for modest weight loss that can be maintained long-term. Moreover, other strategies including self-distraction to help with cravings and boredom eating, removal of environmental triggering foods and planning ahead are suggested. In addition to this finding, Digenio et al. (2009) reported that a high-frequency face-face lifestyle modification counselling showed significant improvements in high-density lipoprotein cholesterol and triglyceride levels, waist circumference, measures of quality of life and weight-related symptoms. Likewise, a six-month high-intensity interval aerobic exercise that was conducted for 30 min three times daily with a caloric restriction and the Mediterranean diet significantly reduced the BMI and blood pressure (Ismail et al., 2023).
Furthermore, Thiabpho et al. (2018) informed that a tailored lifestyle modification having the components of health education, nutritional counselling and exercise training for 16 weeks resulted in healthy weight loss and reduced the metabolic syndrome risk in young obese women. The authors recommended that these strategies to be integrated into the conventional practice in health centres. Additionally, interventions that encompass behavioural modifications of dietary and physical activity are essential for the management of obesity from childhood, which in turn will prevent obesity in young age (Mohd Shariff et al., 2018). More recently, Chopra et al. (2020) stated that weight management in a step-wise intensification of interventions including dietary and physical activity through lifestyle counselling would be beneficial in minimising the prevalence and consequences of overweight and obesity. Lastly, another study reported that a continuous aerobic exercise three times a week for two months significantly reduced the BMI, waist circumference, systolic blood pressure, high-density lipoprotein, diastolic blood pressure and triglycerides (Ismail & Abdelghany, 2022). Thus, the researchers recommend that healthcare providers and health systems to promote healthy lifestyle changes for people who are overweight and obese. The strength of the study is that the BMI has significantly reduced following NLLMI. This is an intervention which can be easily integrated in every clinical and community practice setting, which in turn will minimise the healthcare burden of the county and improve the quality of life of young women.
Conclusion
The authors conclude by stating that the NLLMI on obesity has shown remarkable reduction of BMI among young women in India. Therefore, the authors recommend combination of exercise and healthy diet as a great tool for assisting women in achieving positive energy, both physically and emotionally. Such lifestyle modification initiatives can have a big influence on young obese women and assist to curb the rising obesity epidemic. Women who exercise frequently and adhere to a healthy diet and exercise plan can enjoy and experience the freedom, emancipation and energy that it provides. This research demonstrates that NLLMI can be used as a complementary therapy to help young obese women improve their lifestyles.
Limitations
The study limits the generalisation as the study was conducted in two settings with a limited sample.
Recommendations
The authors recommend conducting the same study on a larger sample and in an urban setting to see the difference in the effectiveness of NLLMI on obesity among young rural and urban women. Likewise, future studies can be conducted to determine the efficacy of NLLMI on the reproductive outcome of young women.
Implications for Practice
Evidence-based research findings can be used by healthcare practitioners to identify and provide resources for obese young women to improve and promote their overall health and well-being. Nurses in the community play an important role in distributing evidence-based complementary therapy to help young obese women overcome their issues. Moreover, evidence-based practice can help young obese women improve their health. Preliminarily, a lifestyle change package could be advised as an extra intervention for women suffering from physical and psychological symptoms related to obesity.
Footnotes
Acknowledgements
The authors extend their sincere thanks to all young obese women who volunteered to participate in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Formal ethical approval was obtained from NIMS University review board and ethics committee (Ref No: NIMSUNI/IEC/2019 dated 29th July, 2019). Both written and verbal information about the study purpose were given in Hindi language to all women who participated in the study. Women were asked to participate voluntarily. The study objectives, benefits, and period involved in practicing the lifestyle modification intervention were explained in the consent form. Women who agreed to participate had the right to withdraw at any time during the study. None of the identifying information of the participants were collected. The data collection sheets were coded and only the investigators of the study had access to the collected data. The research was conducted according to Helsinki ethical recommendations.