
Abstract
Background
Adequate eHealth literacy and health promotion behavior (HPB) are important to achieve good health-related quality of life. There is limited information on the influence of eHealth literacy and HPB on body mass index (BMI) in our setting and among public service workers.
Objectives
This study assessed the eHealth literacy, HPB, and BMI of public service workers and determined the influence of eHealth literacy and HPB on BMI.
Design
A descriptive cross-sectional design was adopted.
Methods
A simple random sampling technique was used to select 440 public service workers from civil service of redacted. A structured questionnaire was used to collect data on socio-demographics, eHealth literacy, and HPB. Weight and height were measured and BMI was calculated. Data were analyzed using frequency, percentage, mean, standard deviation, and logistic regression analysis. The significant level was set at 0.05.
Results
More than one quarter (28.2%) of respondents had low eHealth literacy, and more than one third (42.5%) had inadequate (30.0% fair and 12.5% poor) HPB. An average (50.5%) had a level of obesity that ranged from preobesity to type 2 obesity. There was a significant association between eHealth literacy and HPB with the BMI of respondents at p < .05.
Conclusion
There was inadequate eHealth literacy and HPB among public service workers. An average of the workers had a level of obesity that ranged from pre-obesity to type 2 obesity. There was a significant association between eHealth literacy and BMI and also between HPB and BMI of respondents. Community health professionals should assist public service workers to develop competencies and skills useful in evaluating health information on the Internet and applying such information to make informed decisions.
Introduction
Public service workers occupy a high percentage of the nation's workforce, and their quality of life is crucial to their productivity and the nation's economy. However, previous studies have reported poor Health Promotion Behaviors (HPB), high prevalence of obesity (Aladeniyi et al., 2017), and noncommunicable diseases among public service workers (Aladeniyi et al., 2021; Babatunde et al., 2020). According to Aladeniyi et al. (2017), public service workers engage more in sedentary behavior, lack physical activities, and engage in unhealthy eating behavior. Sedentary and poor dietary behaviors are major factors that may predispose public service workers to overweight and obesity with increased risk of lifestyle diseases (Aladeniyi et al., 2021). Lack of HPB can endanger the health of public service workers. Therefore, encouraging public service workers to engage in HPB will improve their quality of life and in turn improve their productivity and the nation's economy (Babatunde et al., 2020).
Health-promotion behaviors refer to self-directed habits, they consist of activities that include taking responsibility for personal health, engaging in physical activities, and engaging in healthy nutritional habits and stress management (Fashafsheh et al., 2022; Ross et al., 2017). Studies have reported a correlation between HPB and good health (Gurusamy et al., 2022; Nari et al., 2021). Health promotion behavior promotes fitness and plays an important role in the prevention of overweight and obesity (Fruh et al., 2021). It also plays a significant role in the prevention of non-communicable diseases like cancers, cardiovascular diseases, and diabetes. The ability of people to actively gain access to health information that is valuable to them has a major influence on their HPB (Xie et al., 2022). Adequate eHealth literacy has been reported as an influencer of HPB (Wang et al., 2022).
eHealth literacy and health promotion are interrelated concepts that contribute to individual and population health (Ghazi et al., 2023). eHealth literacy is an electronic health literacy that requires an individual to be able to seek, identify, and appraise health-related information from electronic resources for the purpose of solving health challenges (Liu & Xiao, 2021; Paige et al., 2019). According to Norma and Skinner (Norman & Skinner, 2006), eHealth literacy encompasses the skills and knowledge required to navigate, evaluate, and utilize digital health resources such as websites, search engines, online databases, or mobile apps effectively. eHealth literacy simply put, is an individual's ability to search for desired health-related information on the Internet, understand and rate the worth of such information, and use the health information to meet personal health needs or solve personal health problems.
People who are interested in their health often form positive attitudes toward looking for health-related information and searching online for information on preventive behavior; this may enhance their interest to take action in engaging in HPBs (Merati-Fahi et al., 2022). According to Kim et al. (2023) eHealth literacy can indirectly cause health-related information to influence health-promoting behaviors. Previous studies have provided evidence that people with adequate eHealth literacy have a high tendency to engage in healthy behaviors. Such studies include those among college students (Gürkan & Ayar, 2020); nurses (Kim & Oh, 2021), and older adults (Li et al., 2020; Wang et al., 2022). However, these studies are from other countries and among people who are not public service workers. There is limited information in the literature on the influence of eHealth literacy on BMI in our setting and also among public service workers. Previous studies emphasized improving HPB to prevent overweight and obesity and increased risk of lifestyle diseases (Aladeniyi et al., 2021; Babatunde et al., 2020).
Improving eHealth literacy competencies and HPB of public service workers are essential and may enhance the correct use of health information for improved health-related quality of life and control of overweight and obesity. This study assessed the eHealth literacy, HPB, and BMI of public service workers and determined the influence of eHealth literacy and HPB on BMI.
Review of Literature
Being overweight and obese are linked with many health challenges including hypertension, cardiovascular disease, type 2 diabetes, and breathing problems (Aladeniyi et al., 2021). Despite the understanding of the harmful effects of obesity, there are limited achievable and sustainable activities highlighted in the literature that can be used to tackle the problem of obesity (Fruh et al., 2021). Many programs have been suggested to tackle inappropriate weight gain. Part of the government's plan included promoting healthy nutrition, compulsory nutrition labeling, increased physical activities, and sugary drinks tax (Chukwuonye et al., 2022; Food and Agriculture Organization of United Nations Global Forum on Food Security and Nutrition • FSN Forum Discussion 14.06.2016–07.07.2016). However, much has not been achieved through these programs. Improving eHealth literacy and engaging in healthy habits may yield positive results. Poor eHealth literacy skills were reported as a barrier to the utilization of the enormous eHealth resources (Brørs et al., 2020; Schreiweis et al., 2019). There is limited study on eHealth literacy and health promotion behavior of public service workers including the influence of these variables on the control of body weight and maintenance of normal body mass index (BMI) among public service workers in our setting. This information is significant for planning workplace intervention strategies to address overweight and obesity among public service workers. This study assessed the influence of eHealth literacy and health promotion behaviors on the BMI of public service workers.
Methods
Research Design and Setting
A descriptive cross-sectional survey was adopted. This study collected data from many different individuals who are public service workers at once to describe the distribution of the variables of interest. The research questions included: what is the eHealth literacy level, health promotion behavior, and body mass index of public service workers, and last, what is the association between eHealth literacy, health promotion behavior, and the body mass index of public service workers. The setting for this study was the Civil/Public Service Commission in Ondo state, Nigeria. The study population was the public service workers in Ondo-state. The state public service was composed of the Ministries, Departments, and Agencies (MDAs) that were in charge of the government workers and all their official activities in the state. It is located in the capital city of the state. In total, there were 47 MDAs and 25,000 public service workers at the time of this study.
Research Questions
What is the eHealth literacy level of public service workers?
What is the health promotion behavior of public service workers?
What is the body mass index of public service workers?
Is there an association between eHealth literacy, health promotion behavior, and body mass index?
Sample and Sampling Technique
Sample size was calculated using the Taro Yamane formula (n = N1 + N(e)2), where n represents the desired sample size. N represents the population size, which is 25,000, and e stands for sampling error (0.05 as acceptable error). Calculation yielded 394 respondents; with the addition of a nonresponse rate, the total was 440. A total of 17 MDAs were selected out of the 47 MDAs using a simple random sampling technique, and this represented more than one third of the total MDAs.
Inclusion and Exclusion Criteria
To select respondents, a purposive sampling technique was used, inclusion criteria were public service workers who were on grade level 7 to 17 and were willing to participate in the study. Grade level in public service refers to the position of government workers while in office. It indicates the level of education and remuneration. The higher the grade level, the higher the position, level of education, and remuneration. The workers on grade level 7 to 17 were the senior cadre of public service workers. This category of public service workers was included in this study because we assumed that these categories of workers have the ability to read and write; as being literate is an important eHealth literacy skill. The exclusion criterion was the public service workers whose grade level was below 7 because a low-grade level is associated with a low educational level.
Instrumentation
Three instruments were used for data collection, these included structured a self-administered paper questionnaire, a HANA Model weighing scale, and a calibrated meter rule. The questionnaire was divided into sections. The first section obtained questions on the socio-demographic characteristics of respondents which included gender, age, marital status, level of education, grade level, ethnicity, and religion. The second section of the questionnaire contained the eHEALS questions which assessed the eHealth literacy of respondents. The eHEALS was adopted from a previous study (Sudbury-Riley, 2018). It is an 8-item scale, scored on a 5-point Likert scale. The eHEALS has been validated in different countries and in different settings and populations (Chung et al., 2018; Shiferaw et al., 2020), including the study in low-income countries (Shiferaw et al., 2020) and it was concluded that eHEALS has significant validity and reliability. This attests to its reliability among samples with different demographics which includes low-resource nations. The third section of the questionnaire contained 25 items that obtained information on the health promotion behavior of respondents, it was arranged in five subscales, which included nutrition, health responsibility, physical activity, social engagement, and relaxation. It was adapted from a previous study (Ejechi, 2016) that assessed health promotion behavior in early old age in Nigeria. The reliability test of this scale was Cronbach's alpha, 0.72. Respondents were requested to indicate the frequency of the habits/lifestyle listed in the domains as it applies to them.
Respondent's body weight was measured with a HANA Model weighing scale that was placed on a hard and flat ground. The pointer of the scale was on zero while each respondent was positioned on the scale with light clothing and shoes removed. The respondent's weight was approximated to the nearest 0.5 kg when the pointer of the scale became stable. The respondent's height was measured using a calibrated meter rule. Each respondent was asked to stand against the wall with their head straight looking ahead without shoes and with closed feet. Height was measured to the nearest 0.5 cm. Face, content validity, and cultural appropriateness of the questionnaire were achieved through scrutiny of items on the questionnaire by three experts in the fields of community health, public health, and health literacy. This was meant to determine the extent to which items on the questionnaire measured the objectives of the study. Experts were also asked to determine the cultural appropriateness of eHEALS items. All items were considered relevant and appropriate by experts. To determine the reliability of the instrument, a test-retest was conducted using public service workers from MDAs that were not included in our study. The questionnaire was applied on two different occasions with intervals of 2 weeks and both scores were correlated. The result yielded a Cronbach's alpha reliability coefficient of 0.92 for eHealth literacy items while for HPLS was 0.86. The test-retest was also used as a pilot test. The pilot test was used to assess the understanding of public service workers of the questionnaire and if items on the questionnaire captured their experiences. The workers were asked to fill out the questionnaire at the same time. They were told to ask questions where an item seemed unclear and they needed clarification. The public service workers considered the questionnaire clear with meanings that they understood.
Data Collection
Data were collected by the second author and two research assistants who were final-year nursing students. Research assistants were taken through the questionnaire, including the use of the weighing scale and the calibrated meter rule and calculation of the BMI. Data were collected within 3 months, between February and April 2022. Respondents were contacted during the working hours while data were collected in their offices. The purpose of the study was first explained, and completed questionnaires were retrieved immediately and coded.
Ethical Consideration
Ethical approval was obtained from the Health Research and Ethical Committee with Protocol Number: OSHREC 30/11/2021/404. Permission to collect data was obtained from the head of each MDA. The purpose of the study and what respondents were required to do were explained in detail, and both verbal and written informed consent were obtained from respondents. Confidentiality and anonymity were maintained.
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 20. Health literacy, HPB, and BMI were analyzed using frequency, percentage, mean, and standard deviation. eHealth literacy was measured using a 5-point Likert scale (strongly agree = 5, agree = 4, undecided = 3, disagree = 2, and strongly disagree = 1). A higher score indicated higher eHealth literacy. Overall eHealth literacy was classified as adequate, marginal, and inadequate eHealth literacy. Health Promotion behavior was measured using a 4-point scale (never = 1, sometimes = 2, often = 3, always = 4). Negatively worded items were reverse scored. The maximum available score for the entire scale was 100. Respondents who scored above the overall mean value of 22.39 were classified as exhibiting good HPB, those who scored at the mean were categorized as fair HPB, and those who scored below the mean were classified as poor HPB. Body mass index (BMI) was calculated as weight (kg) divided by height in square meters (m2). BMI was categorized in accordance with WHO criteria as <18.5 =underweight, 18.5–24.9 = normal weight, 25.0–29.9 = preobesity, >30.0–34.9 = obesity type 1, and 35.0–39.9 = obesity type 2. The association between these variables was analyzed using logistic regression analysis. The p-value was said to be significant at less than .05 at a 95% confidence interval.
Results
Sample Characteristics
Table 1 shows the distribution of the socio-demographic variables of the respondents. The mean age of respondents was 41.3 ± 2.7 years. More than half (57.3%) were females. Most (90.2%) had tertiary education, and more than one third (35.5%) of respondents were senior-level officers (on grade 14–17 cadre).
Distribution of the Sociodemographic Characteristics of the Respondents.

Research Question Results
eHealth literacy of respondents
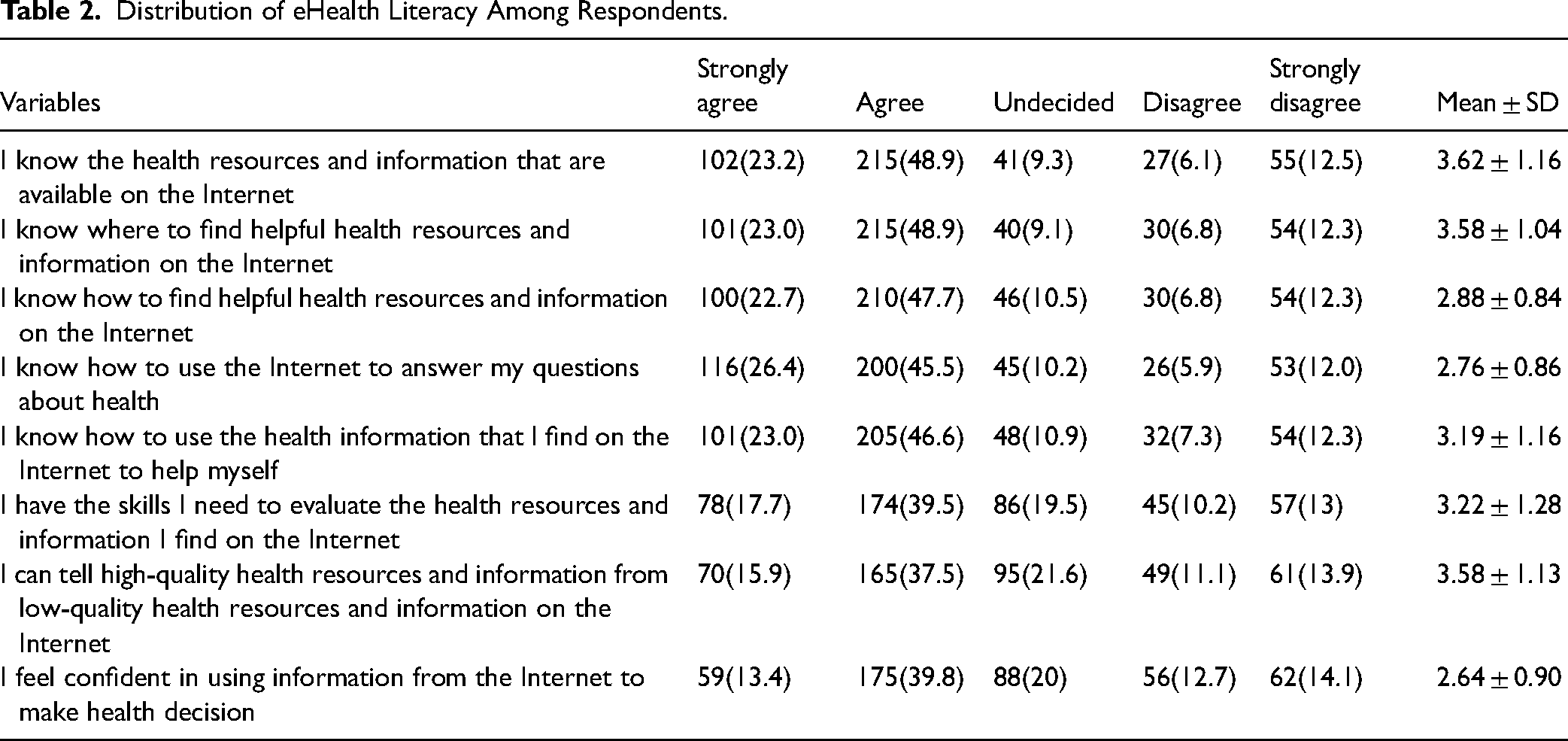
Table 2 shows the distribution of eHealth literacy of the respondents. The majority (72.1%) of the respondents agreed that they knew the health resources and information that were available on the Internet. However, more than one of four disagreed on having the skills to evaluate health resources and information on the Internet (23.2%) and disagreed with feeling confident in using information from the Internet to make health decisions (26.8%). A larger proportion of the respondents (70.4%) agreed that they knew how to find helpful health resources on the Internet. However, about one of four (24.9%) disagreed while more than one of five (21.6%) were undecided on their ability to distinguish high-quality health resources from low-quality health resources on the Internet. Overall, more than a quarter (28.2%) had a low eHealth literacy while a few (14.5%) had fair eHealth literacy.
Distribution of eHealth Literacy Among Respondents.
Health Promotion Behavior of Respondents
The findings from the distribution of health promotion behaviors are shown in Table 3. More than one of four respondents consumed oil and fatty food often (25.9%) and (21.4%) always. In the same vein, more than one of four consumed sugary food and drinks often (26.6%) and always (22.0%); consumed alcohol (23.0%) always, and had no enough sleep (24.3%) sometimes. Also, only half (50.0%) sometimes go for medical checkups, more than one third (46.8%) never engaged in cycling, and almost one third (32.0%) never engaged in any outdoor sports. More than one of four (38.4%) were sometimes exposed to electricity generator smoke. A few (14.8%) had safe sex sometimes. Further findings based on the domains of health promotion behaviors as shown in Supplementary Table 1 showed that respondents’ mean scores were lowest in nutrition (8.32 ± 2.00), physical exercise (6.88 ± 1.94), and engagement in social activities (9.67 ± 2.59). The overall HPB result showed that more than one third (42.5%) of the respondents had inadequate health promotion behavior (fair = 30.0%, poor = 12.5%).
Distribution of Health Promotion Behaviors Among Respondents.

Reverse scored.
Body Mass Index Categorization Among Respondents
Figure 1 presented the BMI categorization which represented the level of obesity of the respondents. Less than half (45.9%) had normal BMI. An average (50.5%) had a level of obesity. More than one third (36.4) were preobese, and a few (10.9%) had obesity class 1 while very few (3.2%) had obesity class 2.

Percentage distribution of BMI respondents (N = 440).
Association of eHealth Literacy and Health Promotion Behavior With BMI
Table 4 presented the association of eHealth literacy and health promotion behavior with the Body Mass Index (BMI) of respondents, as determined through logistic regression analysis. The model indicated that health promotion behavior and eHealth literacy collectively contributed to 11% of the variance in respondents’ BMI. Respondents with good health promotion behavior were twice as likely to have a normal BMI compared to those without (p < .01, Odds ratio: 1.53, 95% confidence interval (CI): 0.80–2.78). Similarly, respondents with fair health promotion behavior were one time more likely to have a normal BMI (p < .01, Odds ratio: 0.22, 95% CI: 0.82–2.61). Moreover, respondents with marginal eHealth literacy were one time more likely to exhibit a normal BMI (p < .01, odds ratio: 1.02, 95% CI: 0.63–2.23). These findings indicated a significant association of both health promotion behavior and eHealth literacy with the BMI of respondents.
Relationship Between eHealth Literacy, Health Promotion Behavior and BMI of Respondents.

0a = reference variable.
Discussion
The aim of this study was to assess the level of eHealth literacy skills and health promotion behavior and further determine their association with the BMI of public service workers. To the best knowledge of the authors, this study is the first study on the influence of eHealth literacy and health promotion behavior on the BMI of public service workers in this setting. The mean age of respondents was 43.22 ± 11.27 years, while about 1/3rd was within 45–54 years. Most of the respondents were married and had a tertiary level of education. This is dissimilar to previous studies that were conducted among high school students (Gürkan & Ayar, 2020) and older adult patients whose ages were 14–18 years and above 60 years respectively. Also, this is dissimilar to other studies in which the majority had secondary school-level education (Li et al., 2020; Soleimaninejad et al., 2021; Wang et al., 2022).
eHealth Literacy of Respondents
More than one third of respondents had inadequate eHealth literacy, this is similar to findings in previous studies among health care workers in which about one third had inadequate eHealth literacy (Shiferaw & Mehari, 2019). The study among patients with chronic diseases reported that the majority of respondents had inadequate eHealth literacy (Shiferaw et al., 2020). The difference in findings may be attributed to the educational background of respondents, and the majority in this study had a tertiary level of education. This study reported that the majority of respondents knew health resources and information available on the Internet. However, a significant number of respondents reported their lack of confidence in using information from the Internet to make health decisions. This is consistent with findings in previous studies (Park & Lee, 2015; Shiferaw & Mehari, 2019). A study explained that knowledge is not enough to influence behavior change (Wang et al., 2022). According to Knowledge Attitude Behavior (KAB) theory, the role of belief and self-efficacy is important in using health information from the Internet to make health decisions. Having confidence in using health information to make health decisions is a demonstration of the skill of self-efficacy. Therefore, self-efficacy of people is required to translate known information into useful decisions about one's own health. Furthermore, more than one third of respondents had no skill required to evaluate health resources and information on the Internet and could not differentiate high from low-quality health resources and information on the Internet. This is consistent with findings in a previous study (Park & Lee, 2015). Pew Internet and American Life Project commented that health information on the Internet is so numerous that it can be cumbersome to decipher for consumers. Moreover, having the skills to search the Internet differs from understanding the quality of the health information on the Internet. The inability to estimate the worth or quality of health information on the Internet may serve as a barrier to the effective utilization of such information for one's health.
Health Promotion Behaviors of Respondents
The result of this study showed that respondents scored lowest in nutrition, physical exercise, and engagement in social activities and highest scores in relaxation and health responsibility. This is similar to the study among nursing students (Kim & Oh, 2021), who also reported the lowest scores in physical exercise and the highest score in stress management. This is contrary to the study among university workers that reported that more than half of their respondents engaged in HPB and the majority engaged in nutrition and social activities; however, only a few engaged in physical activities (Joseph-Shehu et al., 2019). Also, a study among employees reported lower scores in physical activities (Ghorabi et al., 2021). Workers could benefit from increased awareness and education.
Association of Health Promotion Behavior and BMI of Respondents
This study reported an association between HPB and BMI. A similar study among nursing students also reported an association of health promotion lifestyle with student's BMI (Al-Kandari et al., 2008). Another study among male nurses showed that participants with normal BMI had a higher health promotion lifestyle mean score compared with those who were obese (Abbasi & Aghaamri, 2020). Also, in a study of weight management through improved HPB (Behr et al., 2022), participants experienced weight loss at 6 months and 12 months with improved HPB. There was a gradual reduction in weight from initial weight at 6 and 12 months. A longitudinal study reported a positive correlation of HPB with health-related quality of life (Li et al., 2022). Health challenges of overweight and obesity in developing and developed countries have been linked to people's daily habits and lifestyles (Borroso et al., 2018; Li et al., 2021). This indicates that improving HPB may help to reduce excess weight and maintain normal weight.
Association of eHealth Literacy and BMI of Respondents
This study reported that half of our respondents had a level of obesity, from pre-obese to type 2 obesity and this was significantly associated with eHealth literacy. A systematic review (Myers-Ingram et al., 2023) to determine the effectiveness of an eHealth literacy weight management intervention among adults who were overweight and obese reported that eHealth literacy had a short-term effect on weight loss. Another review (Kupila et al., 2023) among similar populations reported a positive effect of eHealth interventions on weight loss and concluded that eHealth literacy may be a very important and economical tool that can be useful for managing weight loss among people who are obese. Improving eHealth literacy and enhancing health promotion behaviors may yield good outcomes in managing people's weight and may curb conditions like overweight and obesity.
Taking advantage of the digital age and the enormous information available on the Internet, enhancing eHealth literacy can be targeted for improved health promotion behaviors and improved health outcomes of the general population. The health and quality of life of public service workers are very crucial as this has direct implications for their productivity and the nation's economy. Enhancing knowledge and skills of eHealth literacy and HPB can be achieved through the development of health education programs and access to health information. The government has an important role which includes the development and implementation of eHealth literacy enhancement policies through funding of projects. For example, the provision of free Wi-Fi in the workplace may improve access to health information for health promotion and improved health-related quality of life.
Strengths and Limitations of the Study
Collection of primary and original data from a randomly selected subpopulation of senior public service workers is the strength of this study. The study was limited by the utilization of a cross-sectional design and hence the causal relationship between eHealth literacy, HPB, and BMI cannot be established.
Implication for Practice
Community health professionals should consider it their responsibility to conduct interventions to improve public service workers' knowledge, skills, and competencies to obtain, judge, and utilize health information on the Internet and also apply such information to make informed decisions on improving their lifestyle and maintaining healthy weights.
Conclusion
This study concluded that more than one third of public service workers had inadequate eHealth literacy and poor health promotion behaviors. Respondents lacked the skill to evaluate health resources and information on the Internet and could not confidently use obtained information to make decisions that concerned their health. Physical exercise and nutrition were the least HPBs engaged in. An average of respondents had a level of obesity that ranged from preobesity to type 2 obesity. Adequate eHealth literacy and good HPB were associated with the BMI of respondents. The findings of this study proposed that the problem of overweight and obesity among public service workers can be improved through improved eHealth literacy and HPB.
Supplemental Material
sj-docx-1-son-10.1177_23779608241274253 - Supplemental material for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector
Supplemental material, sj-docx-1-son-10.1177_23779608241274253 for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector by Cecilia Bukola Bello and Mary Omolara Balogun, Laofe Ogundipe, Simeon Kayode Olubiyi, Theresa Olaitan Bamigboye, Deborah Tolulope Esan in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241274253 - Supplemental material for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector
Supplemental material, sj-docx-2-son-10.1177_23779608241274253 for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector by Cecilia Bukola Bello and Mary Omolara Balogun, Laofe Ogundipe, Simeon Kayode Olubiyi, Theresa Olaitan Bamigboye, Deborah Tolulope Esan in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608241274253 - Supplemental material for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector
Supplemental material, sj-docx-3-son-10.1177_23779608241274253 for Influence of eHealth Literacy and Health Promotion Behavior on Body Mass Index of Workers in the Public Sector by Cecilia Bukola Bello and Mary Omolara Balogun, Laofe Ogundipe, Simeon Kayode Olubiyi, Theresa Olaitan Bamigboye, Deborah Tolulope Esan in SAGE Open Nursing
Footnotes
Acknowledgments
We thank all those who were involved in this study.
Author Contributions
CBB conceptualized the study, supervised the research process, and prepared the original draft of the manuscript. MOB collected data and was involved in data analysis and interpretation. LO conducted the literature search and edited the draft. SKO was involved in data analysis and interpretation. TOB was involved in the preparation of the original draft of the manuscript. DTE was involved in literature search and data interpretation and revised the draft critically. All authors read and approved the final draft of the manuscript.
Data Availability
The data for the findings of this study are with the corresponding author and will be made available on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical approval was obtained from the Ministry of Health Ethical Committee with Protocol Number: OSHREC 30/11/2021/404. Both verbal and written informed consents were obtained from respondents before data collection. Anonymity and confidentiality were maintained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.